Embed Size (px)
Citation preview
Updates in Gastrointestinal Cancer Staging in AJCC8
Andrew M Bellizzi, M.D. Department of Pathology
University of Iowa Hospitals and Clinics [email protected]

Background• Residency in Anatomic/Clinical Pathology at UVA:
04-08 • Fellowship in GI/Liver Pathology at OSU: 08-09 • Faculty at BWH/DFCI/HMS: 09-11 • At Iowa since November 2011
• Director of GI Pathology for HCCC • Co-Director of Immunopathology Laboratory • CAP Immunohistochemistry Committee, Vice Chair
• Teaching: Dx and Reporting of GI/Neuroendocrine/ Hereditary Tumors; Judicious Use of Diagnostic IHC
• Research: Applications of Diagnostic IHC
Outline
• AJCC8 • Everything else • GI – Upper GI – Lower GI – Hepatobiliary – Pancreas
• Tumor Deposits

AJCC8
• AJCC7: 6 editors credited • AJCC8: 18 editors and expert subspecialty
panel leaders • AJCC8: 420 physicians were involved in
analyzing large published data sets (e.g., esophagus cancer staging based on 23K resected cancers)
• Editor-in-chief, Mahul Amin, is a pathologist!

GI Pathologists who Co-Authored AJCC8
John Goldblum Upper GI
Robert Odze Upper GI
Deepa Patil Upper GI
Laura Tang Upper GI, Neuroendocrine
Mary Kay Washington Upper GI
Stan Hamilton Lower GI
Sanjay Kakar Lower GI
Shuji Ogino Lower GI
Alyssa Krasinskas Hepatobiliary
Mari Mino-Kenudson Hepatobiliary
Guido Rindi Neuroendocrine
David Klimstra Neuroendocrine

Analysis of Large Data Sets
Organ N
Esophagus 22654Stomach (pTNM) >25000 (IGCA)Stomach (ypTNM)
700
Small intestine 3141 duodenum, 3807 non-duodenum (NCD)
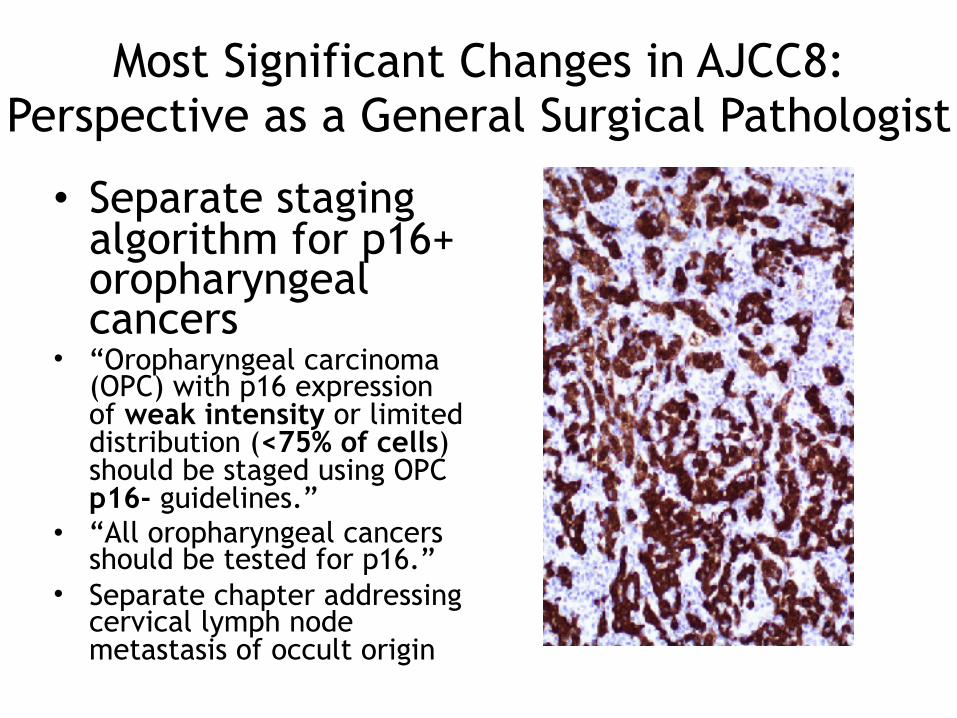
Most Significant Changes in AJCC8: Perspective as a General Surgical Pathologist
• Separate staging algorithm for p16+ oropharyngeal cancers
• “Oropharyngeal carcinoma (OPC) with p16 expression of weak intensity or limited distribution (<75% of cells) should be staged using OPC p16- guidelines.”
• “All oropharyngeal cancers should be tested for p16.”
• Separate chapter addressing cervical lymph node metastasis of occult origin

Most Significant Changes in AJCC8: Perspective as a General Surgical Pathologist
• Incorporation of results of ER, PR, and HER2 and in pT1-2 N0 M0 ER+/HER2- Oncotype Dx results into overall prognostic stage groups
• Historical precedent – Prostate: PSA, Gleason – Esophagus: SCC<<AdCA

Other Significant Changes that Will Come Up Often: Head and Neck
• Depth of invasion incorporated into oral cancer T category
• Extranodal extension incorporated into the N category (except nasopharynx and p16+ oropharynx)
• New H&N cutaneous squamous cell carcinoma chapter

Other Significant Changes that Will Come Up Often: Breast
• “Lobular carcinoma in situ (LCIS) is a benign entity and is removed from TNM staging.”
• LCIS ≠ Tis
Clarity on measurement of ITC/Nmi

Other Significant Changes that Will Come Up Often: Thorax
• New lung T stages – T1a/b ! T1mi/a/b/c
• Extensive discussion of how to deal with multiple tumor nodules (e.g., separate primary vs intrapulmonary metastasis
• New thymus chapter

Other Significant Changes that Will Come Up Often: Endometrium
• Tis eliminated • Endometrial intraepithelial carcinoma
(EIC) considered T1 • Introduction of N1mi and N2mi

Other Significant Changes that Will Come Up Often
Prostate: pT2 (organ confined disease)
AJCC7 AJCC8
pT2a: Tumor involves ≤1/2 or 1 lobe pT2: Tumor confined within prostatepT2b: Tumor involves >1/2 of 1 lobe
pT2c: Bilateral disease
Thyroid: pT3
AJCC7 AJCC8
pT3: Tumor >4 cm limited to the thyroid, or any tumor with minimal extrathyroid extension (e.g., extension to sternohyoid muscle or perithyroid soft tissues)
pT3a: Tumor >4 cm limited to the thyroid
pT3b: Gross extrathyroidal extension invading only strap muscles from tumor or any size

Other Significant Changes that Will Come Up Often: Melanoma
pT1
AJCC7 AJCC8
pT1a: Thickness ≤1.0 mm without ulceration and mitosis <1 mm2
pT1a: Thickness ≤0.8 mm without ulceration
pT1b: Thickness ≤1.0 mm with ulceration or mitosis ≥1 mm2
pT1b: Thickness <0.8 cm with ulceration or thickness 0.8-1.0 mm regardless of presence of ulceration

Other Changes (only of interest to Munir and me)
• New retroperitoneal sarcoma staging system • New H&N sarcoma staging system • New visceral sarcoma staging system • These supplement staging system for tumors
of somatic soft tissue
• New parathyroid and pheochromocytoma and paraganglioma chapters
• B symptoms eliminated from staging of NHL

How Many Nodes
Esophagus 12-23
Stomach ≥16 (≥30 is desirable)
Non-ampullary duodenal AdCA ≥5 nodes (optimal staging ≥8)
Non-duodenal small intestinal AdCA
≥9 nodes
Apendix AdCA ≥12
Colon ≥12
Intrahepatic cholangiocarcinoma ≥6
Gallbladder ≥6
Distal cholangiocarcinoma ≥12
Ampulla of Vater ≥12
Pancreas ≥12

Esophagus and GEJ
Carcinomas with epicenter within 2 cm of the GEJ care staged as esophageal cancers if they involve the GEJ (in AJCC7 was 5 cm)
Esophageal
Gastric (AJCC8)
Gastric

Separate pTNM and ypTNM Stage Groupings

Esophagus and GEJ
• After neoadjuvant therapy “histologic assessment of most of the periesophageal soft tissue is helpful to retrieve grossly impalpable lymph nodes”
• “Whenever possible, invasion of lymphatic vessels should be reported separately from vascular invasion , as this may portend a difference in prognosis.”
• Positive radial margin (also applies to stomach) – CAP: tumor on ink – Royal College of Pathologists: tumor within 1 mm
• HER2 testing in advanced incurable adenocarcinoma

Stomach
• N3! N3a/b • New ypTNM • “The specimen should be tested for the
presence of Helicobacter pylori infection.” • “Tumor deposits . . . are considered
regional LN metastases for the purposes of staging”
• AJCC8 definition of TD

Small Intestine
• For pT3/4 extent of penetration into the retroperitoneum omitted
• N category – N1: 1-2 (was 1-3) – N2: 3 or more (was 4 or more)
• AdCA – Duodenum 60% (worse stage-specific survival) – Jejunum 20% – Ileum 15%

Appendix
Grading of “mucinous adenocarcinoma”
G1 LAMN
G2 • Invasive adenocarcinoma without a signet-ring-cell component
• HAMN (rare)
G3 High-grade invasive AdCA, usually with a SRC component
• Tis (LAMN); T1 and T2 do not apply to LAMN
• N category harmonized with colonAJCC7 AJCC8
pT4a: Tumor penetrates visceral peritoneum, including mucinous peritoneal tumor in RLQ
pT4a: Tumor invades visceral peritoneum including acellular mucin or mucinous epithelium involving serosa/mesoappendix
pM1a: Intraperitoneal metastasis beyond RLQ
pM1a: Intraperitoneal acellular mucin
pM1b: Intraperitoneal metastasis containing tumor cells
pM1b: Nonperitoneal metastasis pM1c: Nonperitoneal metastasis

Colon
AJCC7 AJCC8
pM1a: Metastasis to 1 organ or site pM1a: Metastasis to 1 organ or site
pM1b: Metastasis to ≥2 organs or sites OR peritoneum
pM1b: Metastasis to ≥2 organs or sites
pM1c: Metastasis to peritoneum (alone or with other metastases)
• Clarified definition of tumor deposits • Reasserted distinction of lymphatic from
venous invasion • Macroscopic assessment of TME • ITC: up to 20 cells • Micrometastasis: 10-20 cells or ≥0.2 mm

LVI! Small Vessel and Large Vessel Invasion
• “Small vessel invasion is involvement by tumor of thin-walled structures lined by endothelium, without an identifiable smooth muscle layer or elastic lamina.” – Lymphatics (D2-40) – Capillaries – Post-capillary venules
• SVI: LN metastasis • EMVI: Liver metastasis • IMVI: Sig. unclear

D2-40 Elastin

Anus
• New N categories (new stage groupings to incorporate these)

Hepatobiliary• HCC: T categories reconfigured but same features
apply (i.e., size, multiplicity, vascular invasion) • ICC: T1!T1a/b and T2a/b!T2; direct invasion
T3->T4; periductal infiltrating tumor no longer considered T4
• Gallbladder: T2!T2a: peritoneal side, T2b: hepatic side (Shindoh et al. n=252); N category reconfigured
• “50% of gallbladder cancers are discovered at pathological examination after simple cholecystectomy for presumed gallstone disease.”
• Perihilar CC: N category reconfigured (N1 1-3; N2 4+); 50-70% of bile duct cancers

Distal Bile Duct (b/t confluence of cystic duct and CHD and Ampulla)
• “The extrahepatic biliary tree lacks uniform smooth muscle invasion along its length, with scattered or no muscle fibers in the wall of the proximal ducts as compared with the distal bile duct.”
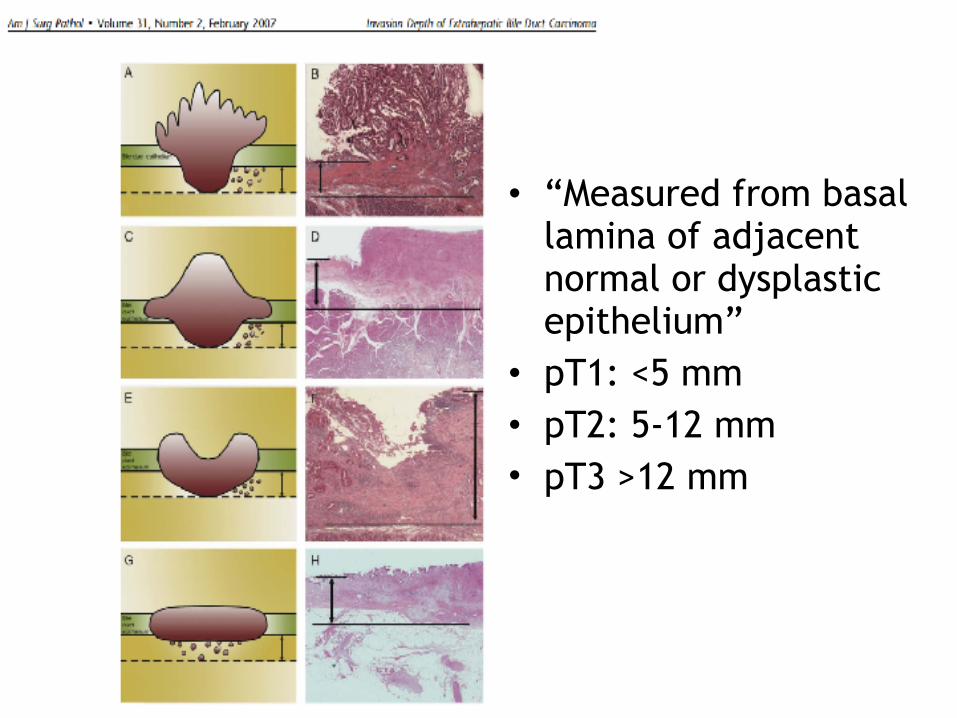
• “Measured from basal lamina of adjacent normal or dysplastic epithelium”
• pT1: <5 mm • pT2: 5-12 mm • pT3 >12 mm

Courtesy of Dr. Sagar Vishal
8 mm
AJCC7: T2, tumor invades beyond bile duct wall AJCC8: T2, tumor invades to a depth 5-12

Ampulla of Vater• Applies to all primary carcinomas that arise in
the ampulla or on the duodenal papilla • Analysis of CK20, CDX2, MUC1, and MUC2 is
conjunction with H&E allows for classification of pancreatobiliary and intestinal subtypes in 92% of cases (clinical sig: PB=gem, IT=FOLFOX)

The Ampullary Problem
• I would call these ampullary cancers “periampullary duodenal” and stage them as small intestinal to avoid pT4

The Ampullary Solution
• pT1a: Tumor limited to ampulla of Vater or sphincter of Oddi
• pT1b: Tumor invades beyond sphincter and/or into duodenal submucosa
• pT2: Tumor invades muscularis propria or duodenum
• pT3a: Tumor invades pancreas (≤0.5 cm) • pT3b: Tumor invades pancreas (>0.5 cm) or
extends into peripancreatic tissue or duodenal serosa
• pT4: Tumor involves celiac axis, SMA, and/or CHA

Pancreas


Pancreas
AJCC7 UIHC (n=188)
AJCC8 UIHC (n=181)
pT1: Limited to pancreas and ≤2 cm
6% (11) pT1a: ≤0.5 cm 0% (0)
pT1b: >0.5 cm and <1 cm 2% (3)
pT1c: 1-2 cm 12% (22)
pT2: Limited to pancreas and >2 cm
20% (38) pT2: >2 and ≤4 cm 64% (115)
pT3: Extrapancreatic spread
73% (138) pT3: >4 cm 22% (40)
pT4: celiac axis or SMA (unresectable)
0.5% (1) pT4: celiac axis, SMA, CHA
0.5% (1)
• Extrapancreatic extension no longer part of T • “Extrapancreatic extension may be difficult
to determine b/c the pancreas does not have a capsule.”
• N1!N1 (1-3) and N2 (≥4)

Neuroendocrine: Jejunoileal NET
• N2: Large mesenteric masses (>2 cm) and/or extensive nodal deposits (≥12), especially those that encase the mesenteric vessels
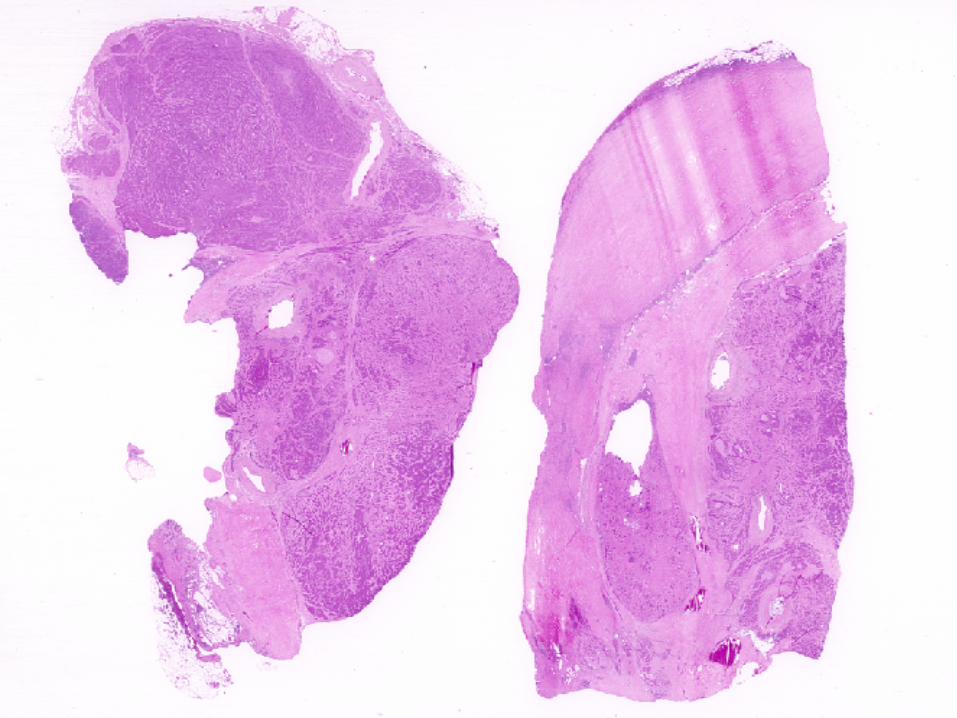

Tumor Deposits• “Tumor deposits are defined as discrete tumor
nodules within the lymph drainage area of the primary carcinoma without identifiable lymph node tissue or identifiable vascular or neural structure.”
• “Shape, contour, and size of the deposit are not considered in these designations.”
• “If the vessel wall or its remnant is identifiable on H&E, elastin, or any other stain, the lesion should be classified as lymphovascular invasion.”
• “The number of tumor deposits is not added to the number of positive lymph nodes.”
• Number of TDs (1-4, 5 or more) should be recorded • Frequency of TDs (Chen et al. SEER. Cancer. 2014.)
– 10% of CRC – 2.5% of all colon and 3.3% of all rectal cancers are N1c

Not a tumor deposit
Still a tumor deposit?

USCAP 2018: Frequency and Significance of Tumor Deposits in
CRC

Research Questions
• What is the frequency of TDs in UIHC in-house-resected CRC?
• How often do patients with a TD have concurrent LN metastasis vs TD in the absence of LN metastasis (i.e., N1c)?
• Does the rate of reporting and frequency of TDs vary between general and GI pathologists?
• What is the prognostic significance of TDs?

Study Design
• Chart review of all UIHC-resected CRC reported from 1/1/2010 to 7/30/2017
• Recorded patient age; gender; tumor site; grade; size; LVI; PNI; presence and number of TDs; number of LNs examined and positive; stage modifier (e.g., y); AJCC 7 T, N, M category; vital status; pathologist; general vs GI
• Fisher’s exact test; p<0.05 considered significant

Results• What is the frequency of TDs in UIHC in-
house-resected CRC? – Total in house cases: 515 – TD not reported: 74 (14%) – TD present: 28% (124/441)
• How often do patients with a TD have concurrent LN metastasis vs TD in the absence of LN metastasis (i.e., N1c)? – TD with concurrent LN met: 93 (75%) – TD without concurrent LN met: 31 (25%) – Among all CRC TD without concurrent LN met in
7% (31/441)

Results
• Does the rate of reporting and frequency of TDs vary between general and GI pathologists? No
TDs Mentioned
TD present p
General 84% (160/190) 27% (43/160) 0.52GI 86% (281/325) 29% (81/281) 0.74

Prognostic Significance of TDsTD present (n=124)
TD absent (n=317)
p
Alive 57% (71) 81% (258) <0.0001
LVI 82% (99) 36% (114) <0.0001
PNI 55% (67) 16% (50) <0.0001T3/4 94% (116) 69% (216) <0.0001N+ 75% (93) 25% (80) <0.0001M+ 15% (19) 3% (8) <0.0001

Prognostic Significance of TDsAlive Dead p
TD present (n=124)
57% (71) 43% (53) <0.0001
TD absent (n=317) 81% (258) 19% (59)
LVI present (n=225)
68% (152) 32% (73) 0.0057
LVI absent (n=232) 79% (184) 21% (48)
PNI present (n=126)
66% (83) 34% (43) 0.024
PNI absent (n=331) 77% (254) 23% (77)
T3/4 (n=345) 71% (245) 29% (100) 0.036
T1/2 (n=112) 81% (91) 19% (21)
N+ (n=186) 65% (120) 35% (66) <0.0001
N0 (n=291) 81% (237) 19% (54)
M+ (n=31) 39% (12) 61% (19) <0.0001
M0 (n=484) 77% (372) 23% (112)

Conclusions
• Tumor deposits are present in 28% of cases • They are ID’d and reported at the same
rate by general and GI pathologists • Concurrent LN mets in 75%; N1c in 25% • TD associated with LVI, PNI, T3/4, N+, M+ • A smaller % of patients with TD are alive
than with LVI, PNI, T3/T4, N+

Outline
• AJCC8 • Everything else • GI – Upper GI – Lower GI – Hepatobiliary – Pancreas
• Tumor Deposits






























