Embed Size (px)
Citation preview

1474
DIAGNOSTIC TECHNIQUES
JACC Vol. 5. No.6June 1985:1474-7
Unusual Distribution of Left Ventricular Hypertrophy in ObstructiveHypertrophic Cardiomyopathy: Localized Posterobasal Free WallThickening in Two Patients
BARRY J. MARON, MD, FACC, PAOLO SPIRITO, MD, FRANCESCO CHIARELLA, MD,
CARLO VECCHIO, MD
Bethesda, Maryland and Genoa, Italy
Two patients with hypertrophic cardiomyopathy and apreviously unreported distribution ofteft ventricular hypertrophy are described. Each patient showed substantial wall thickening that was confinedto the posternbasal segment of the left ventricular free wall, as wellas evidence of dynamic subaortic obstruction. This observation emphasizes the fact that hypertrophic cardio-
Two-dimensional echocardiography has been used to identify a variety of patterns of left ventricular hypertrophy inpatients with hypertrophic cardiomyopathy (1-4). Ventricular wall thickening is most commonly present in substantialportions of both ventricular septum and anterolateral freewall (2,5). However, hypertrophy may often be localizedto relatively small areas of the left ventricular wall, usuallythe anterior basal septum (2). This report describes twopatients with hypertrophic cardiomyopathy and evidence ofsubaortic obstruction in whom a previously undescribed pattern of ventricular wall thickening was identified. In thesepatients, hypertrophy was confined to the posterobasal freewall, that portion of the left ventricle least frequently hypertrophied in patients with hypertrophic cardiomyopathy(2).
Case ReportsClinical findings. Clinical and echocardiographic find
ings in the two patients are summarized in Table I. The
From the Cardiology Branch, Echocardiography Laboratory, NationalHeart, Lung, and Blood Institute, National Institutes of Health, Bethesda,Maryland and Divisione di Cardiologia, Ente Ospedaliero Ospedali Galliera, Genoa, Italy. Manuscript received October 9, 1984; revised manuscript received December 26, 1984, accepted January 11, 1985.
Address for reprints: Barry J. Maron, MD, National Heart, Lung, andBlood Institute, National Institutes of Health. Building 10. Room 7B-15.Bethesda, Maryland 20205.
© 1985 by the American College of Cardiology
myopathy is characterized by a broad morphologicspectrum. Furthermore, it demonstrates a uniquecircumstance in which left ventricular outflow tract obstruction may occur in the absence of anterior and basalseptal hypertrophy.
(J Am Coli CardioI1985;5:1474-7)
patients differed with regard to symptomatic state, PatientI being virtually asymptomatic and Patient 2 demonstratingmarked functional limitation with dyspnea on exertion andfatigue, angina pectoris, lightheadedness, palpitation andsyncope. Electrocardiograms showed only a deep S wavein lead VI in Patient I and absence of an R wave in leadsVI and V2 in Patient 2.
Each patient had an ejection murmur (grade 4/6 in PatientI and grade 2/6 in Patient 2) at the lower left sternal borderand apex, which increased with standing and decreased withsquatting. Systemic blood pressure recordings were normalin each patient; Patient 2 had normal coronary artery anatomy as demonstrated by coronary arteriography.
Echocardiographic findings. The echocardiographicfindings were quite similar in the two patients. Each patientshowed hypertrophy confined to only a small region of theleft ventricular wall, that is, the posterobasal free wall justbehind the posterior mitral leaflet (Fig. I to 3). The thicknessof this region was marked (19 mm in Patient I and 18 mmin Patient 2), but was limited to only about a 2 em segmentof the wall, resulting in the morphologic appearance of adiscrete mass. In each patient, all visualized portions of theventricular septum appeared to be of normal thickness. Inaddition, both patients showed reduced end-diastolic crosssectional area of the left ventricular outflow tract as assessedby two-dimensional echocardiography (Table 1).
Both patients also showed systolic anterior motion of themitral valve on echocardiography under basal conditions
0735-1097/85/$3.30

JACC Vol. 5. No.6June 1985:1474-7
MARON ET AL.POSTEROBASAL HYPERTROPHY IN CARDIOMYOPATHY
1475
Table 1. Clinical and Morphologic Data in Two Patients With Hypertrophic Cardiomyopathy and Isolated Posterobasal LeftVentricular Free Wall Hypertrophy
Echocardiographic Dimensions
LYID (mm) LYOTAge (yr) vs- PBLV* LA Areat
Case &Sex FC (mm) (mm) d (mm) (cnr')
1 36M I 9 19 47 27 41 3.82 33F 3 10 18 36 22 31 4.5
*Measurements made by convention at end-diastole (peak of the R wave on the electrocardiogram); [ cross-sectional area of the left ventricular outflowtract at end-diastole as determined by two-dimensional echocardiography (I I); the normal range is 9.0 to 12.6 em! and the range for patients withhypertrophic cardiomyopathy and basal subaortic pressure gradient is 1.5 to 5.0 ern", d = diastole; F = female; FC = functional class (New YorkHeart Association); LA = left atrium; LYID = left ventricular internal dimension; LYOT = left ventricular outflow tract; M = male; PBLV =posterobasal left ventricle; s = systole; VS = ventricular septum.
(Fig . 1, 2 and 4). In Patient I, the systolic anterior motionwas marked . and the distal tip of the anterior mitral leafletclosely approached the ventricul ar septum for a substant ialproportion of echo cardio graphic systole (Fig. 4); mild partial premature closure of the aortic valve was also evident.Patient 2 showed only mild systolic anterior motion . whichproved on two-dimensional echocardiographic study to be
Figure I. Patient I. Stop frame two-dimensional echocardiogramobtained in the apical four chamber view during systole. Thediscrete area of localized hypertrophy in the posterobasal segmentof the left ventricle (LV) is indicated by arrowheads . Note themarkedsystolic anterior motion of the anterior mitral leaflet (AML).Only the tip of the anterior leaflet comes in contact with the ventricular septum (VS). which is of normal thickness. LA = leftatrium.
produced preferentially by the posterior mitral leaflet (6 ,7);also , the anterior leaflet prolapsed during late systole intothe left atrium. Premature aortic valve closure was absent.
Hemodynamic data. At cardiac catheterization, Patient2 had a basal 20 mm Hg peak systolic pressure gradientacross the left ventricular outflow tract ; with isoproterenolinfusion the gradient increased to 105 mm Hg. Left ventricular end-diastolic pressure was 20 mm Hg . Patient I didnot undergo catheterization because there was no clinicalindication.
Figure 2. Patient I. Stop frame two-dimensional echocardiogramobtained in parasternal long-axis viewduringsystole. The localizedregion of posterobasal wall thickening is shown by the dotted line.Note the marked mitral systolic anterior motion in which the anterior leaflet bends acutely, so that only the leaflet tip closelyapproaches the ventricular septum (VS) (arrowheads) . Ao ==aorta; LA = left atrium.

1476 MARON ET AL.POSTEROBASAL HYPERTROPHY IN CARDIOMYOPATHY
JACC Vol. 5. No.6June 1985:1474-7
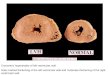
Figure 3. Patient 2. M-mode echocardiogram showing posterobasalleft ventricular waIl(PW)thickening. The ventricular septum(VS) is of normal thickness. The posterobasal free waIl is abouttwice as thick as the septum. Calibration dots are 10 mm apart.MV = mitral valve.
Family studies. Hypertrophic cardiomyopathy was documented by echocardiography in at least one first degreerelative of each study patient. The 34 year old asymptomaticsister of Patient 1 showed a pattern of hypertrophy moretypical of hypertrophic cardiomyopathy (4), involving primarily the anterior and posterior segments of the ventricularseptum (maximal thickness 30 mm). The 67 year old motherof Patient 2 had hypertrophy of the septum and posteriorfree wall, which was most marked in the apical half of theleft ventricle (maximal thicknesses 20 mm), in the absenceof other cardiac disease. Also, the 27 year old asymptomaticbrother of Patient 2 had discrete areas of hypertrophy in theposterior ventricular septum and posterolateral free wall(maximal thickness 22 mm).
DiscussionOur two patients with hypertrophic cardiomyopathy dem
onstrate a unique pattern of left ventricular hypertrophy notpreviously described in two-dimensional echocardiographicstudies of more than 300 patients with this disease (1-4).
Figure 4. Patient 1. M-mode echocardiogram atthe level of the mitralvalve (MV). Systolic anteriormotion of the mitral valve is seen (arrow) as theanterior mitral leaflet comes into near appositionwith the ventricularseptum(VS). This echocardiogram also suggests that mitral systolicanteriormotion is confined to the distal portion of the leaflet(see portion of recording to the left and comparewith that in Fig. 2), but is notproducedby the moreproximal portion of the leaflet (see portion of recording to the right and compare with that in Fig.2). Posterobasal free waIl (PW) hypertrophy is notwelldefinedin thisrecording. RV = rightventricle.
Indeed, these two patients with localized posterobasal wallthickening have hypertrophy in that region of left ventriclewhich is the site least frequently thickened in patients withhypertrophic cardiomyopathy. Therefore, our findings emphasize the diverse morphologic expressions that may occurwithin the clinical spectrum of hypertrophic cardiomyopathy.
Differential diagnosis. The uniqueness of this patternof hypertrophy raises the possibility that our patients had acardiac disease process other than hypertrophic cardiomyopathy (for example, tumor, clot or cardiac manifestationof hypereosinophilia [8]). However, this possibility seemsunlikely for two reasons. First, we were able to confirm byechocardiography a more typical distribution of left ventricular hypertrophy in at least one first degree relative ofeach patient, indicative of the genetic transmission of hypertrophic cardiomyopathy (9) with a variable morphologicexpression (4). Second, each patient showed evidence ofdynamic obstruction to left ventricular outflow (measuredat cardiac catheterization in Patient 2 and estimated by echocardiography in Patient 1) due to systolic anterior motionof the mitral valve (6,7,10,11) and typical of hypertrophiccardiomyopathy. Furthermore, in each patient, clinical evidence of the hypereosinophilic syndrome was lacking; echocardiograms showed no cardiac morphologic changes overa period of about 1 year (Patient l) or 3 years (Patient 2),making the diagnosis of tumor or clot less likely.
Outflow tract morphology. Of note, in hypertrophiccardiomyopathy, subaortic obstruction and systolic anteriormotion of the mitral valve usually occur in the presence ofanterior basal septal hypertrophy and a small left ventricularoutflow tract (II). However, our patients showed a distinctlydifferent left ventricular configuration, in which the left ventricular outflow tract was small even though basal ventricularseptal hypertrophy was absent. This reduction in outflowtract size was probably due, in part, to the posterobasal wallthickening which caused the mitral valve to be positionedabnormally close to the septum, thereby predisposing to theVenturi phenomenon (12) and systolic anterior motion ofthe mitral valve (that is, subaortic obstruction).

JACC Vol. 5, No.6June 1985:1474--7
MARON ET ALPOSTEROBASAL HYPERTROPHY IN CARDIOMYOPATHY
1477
ReferencesI . Maron Bl , Gottdiener IS, Bonow RO, Epstein SE. Hypertrophic car
diomyopathy with unusual locations of left ventricular hypertrophyundetectable by M-mode echocardiography . Circulation 1981;63:409- 18.
2. Maron Bl, Gottdiener JS, Epstein SE . Patterns and significance of thedistribution of left ventricular hypertrophy in hypertrophic cardiomyopathy: a wide-angle, two-dimensional echocardiographic study of125 patients . Am 1 Cardiol 1981;48:418-28 .
3. Shapiro LM, McKenna Wl . Distribution of left ventricular hypertrophy in hypertrophic cardiomyopathy: a two-dimensional echocardiographic study . J Am Coli Cardiol 1983;2:437-44.
4 . Cir6 E, Nichols PF, Maron Bl . Heterogeneous morphologic expression of genetically transmitted hypertrophic cardiomyopathy: two-dimensional echocardiographic analysis . Circulation 1983;67:1227-33.
5 . Martin RP, Rakowski H. French 1, Popp RL. Idiopathic hypertrophicsubaortic stenosis viewed by wide-angle , phased-array echocardiography . Circulation 1979;59: 1206-17.
6. Maron Bl, Harding AM, Spirito P. Roberts WC. Waller BF. Systolicanterior motion of the posterior mitral leaflet: a previously unrecognized cause of dynamic subaortic obstruction in hypertrophic cardiomyopathy . Circulation 1983;68:282-93 .
7 . Spirito P, Maron Bl . Patterns of systolic anterior motion of the mitralvalve in hypertrophic cardiomyopathy: assessment by two-dimensionalechocardiography . Am 1 Cardiol 1984;54:1039-46.
8. Gottdiener IS. Maron BJ, Schooley RT , Harley IB, Roberts WC ,Fauci AS. Two-dimensional echocardiographic assessment of the idiopathic hypereosinophilic syndrome: anatomic basis of mitral regurgitation and peripheral embolization. Circulation 1983;76:572-8.
9. Maron Bl, Nichols PF, Pickle LW, Mulvihill JJ. Patterns of inheritance in hypertrophic cardiomyopathy: assessment by M-mode andtwo-dimensional echocardiography. Am J Cardiel 1984;53:1087 -94.
10. Shah PM, Taylor RD, Wong M. Abnormal mitral valve coaptation inhypertrophic obstructive cardiomyopathy: proposed role in systolicanterior motion of mitral valve . Am 1 Cardiol 1981;48:258-62.
II. Spirito P, Maron BJ. Significance of left ventricular outflow tractcross-sectional area in hypertrophic cardiomyopathy: a two-dimensional echocardiographic assessment. Circulation 1983;67: 1100-8.
12. Wigle ED. Adelman AG. Silver MD. Pathophysiological considerations in muscular subaortic stenosis . In: Wolstenholme GEW, O'Connor M. eds. Hypertrophic Obstructive Cardiomyopathy. London:J & A Churchill, 1971:63-76.