Embed Size (px)
DESCRIPTION
Pharm notes
Citation preview

PHARMACOLOGY UNIT ONE
Warde

Drug Development and Nomenclature
• Sources of drugs• Plants • Animals• Synthetic chemicals• Genetically engineered chemicals

Drug Development and Nomenclature
Plants • Date to primitive times • Classified according to their physical and chemical
properties • Alkaloids • Glycosides • Gums • Oils • Resins

Drug Development and Nomenclature
• Animals• Traditionally, drugs from animal sources
• eg.insulin
• Today, genetically engineered hormones are rapidly replacing animal-based drugs

Drug Development and Nomenclature
• What is the advantage of genetically engineered drugs over those made from animals?
Drug Development and Nomenclature
• What is the advantage of genetically engineered drugs over those made from animals? • Genetically engineered drugs are considered purer,
causing less adverse drug reactions

Drug Development and Nomenclature
• Synthetic Chemicals• Most drugs today are synthetic chemical compounds
• partial or total• Partially synthetic agent
• derivative of a natural substance + a pure chemical.
• An advantage of totally synthetic drugs• pure chemicals
Drug Development and Nomenclature
• Genetically engineered Chemicals• Developed using DNA technologies
• Insulin Recombinant DNA technology • Genomics
• Study & identification of genes & gene function • Enabled researchers to manipulate chemical
formulas to produce more specifically targeted drugs with fewer adverse effects
• Proteomics • Study of protein structure and function • Technology essential in biomarker discovery

Drug Development and Nomenclature
• Genetically engineered Chemicals (cont.)
• Transcriptomics• Study of the transcriptome• Aids in understanding the development and
differentiation of a cell
• Metabonomics • Study of metabolic responses to drugs, environmental
changes, and diseases • Can possibly predict an individual patient’s response to
drug treatment
Drug Development and Nomenclature
• Drug development process• First step: discovery of a potential new drug
molecule. • Preclinical trials
• Designed to provide basic safety, bioavailability, pharmacokinetic, and initial efficacy data about the drug
• Clinical trials • Performed on humans in several phases.
• Only about 10% of new drugs that begin clinical trials are approved.

Question
In this phase of clinical trials, the majority of the risks associated with the new drug therapy are identified. A. Phase I
B. Phase II
C. Phase III
D. Phase IV

Answer and Rationale
In this phase of clinical trials, the majority of the risks associated with the new drug therapy are identified.
C. Phase III
In phase III of drug trials, 1,000 to 3,000 patient volunteers are enrolled in double-blind studies and crossover design studies. These studies are monitored closely to evaluate the safety and effectiveness of the drug.

Drug Development
• Critical Thinking Scenario• Page 23
Drug Development and Nomenclature
• Nomenclature• Chemical name
• Precisely describes the drug’s atomic and molecular structure
• Generic name • Nonproprietary name; identifies the drug’s active ingredient
• Trade name• Brand or proprietary name
Legislation • Legislation to Promote Truth In Advertising
• 1912• 1938 first labeling requirements• Federal Trade Commission regulates the advertisement of
medications aimed at the general public
• Standards for Drug Purity and Content• Pure Food and Drug Acts • Federal Food, Drug, and Cosmetics Act of 1938 • Kefauver-Harris Amendment
Controlled Substances Legistation• Harrison Narcotic Law of 1914
• Regulation of manufacture and distribution of certain drugs
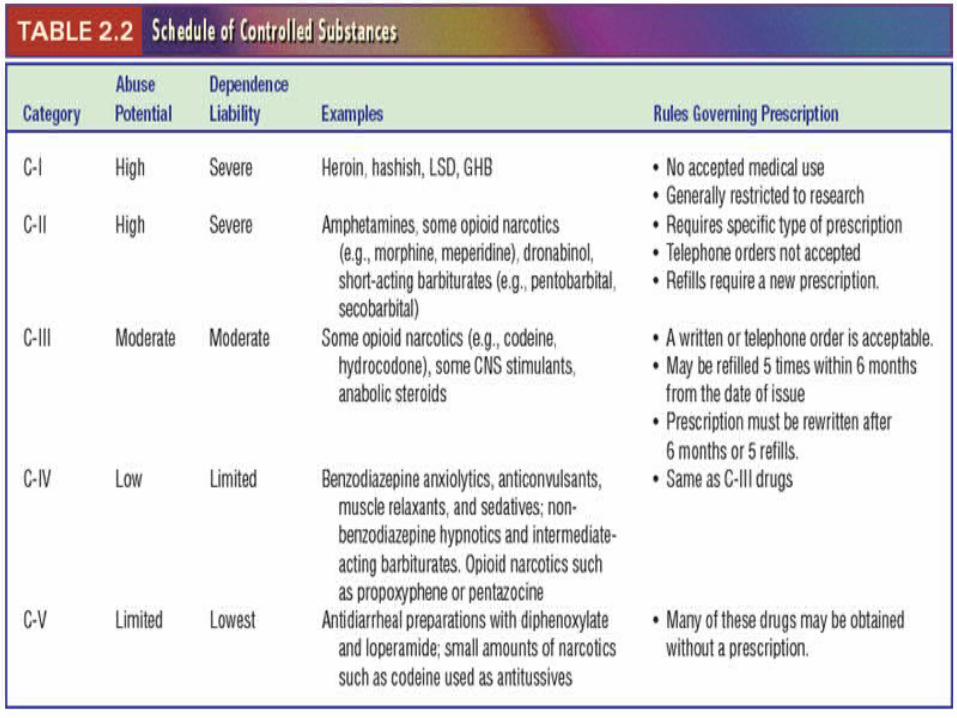
• The 1970 Comprehensive Drug Abuse Prevention and Control Act • Established Drug Enforcement Agency (DEA)• Five categories, known as schedules, were established
• Scale of I – V; I has greatest potential for abuse and no accepted medical use
• Designed to alleviate problem of drug abuse• Drugs categorized & controlled based on abuse potential & medical
usefulness
• Special rules for prescribing, dispensing & storing
Nursing Management of Controlled Substances
• Prescribing, dispensing, & storing of controlled substances is subject to governmental control
• Procedures are precisely defined by law for every step, from manufacture to administration to wasting or discarding
• Many hospitals use an automated system to electronically track the use of stock drugs.
Legislation Regarding Drug Distribution
• The Durham-Humphrey amendments (1952) • Nonprescription drugs (over-the-counter drugs [OTC])• Legend (prescription) drugs
• Labeled properly• Procedures for the distribution of legend drugs
Patient Education – A Safety Net
• Patient learning needs• Teaching
• Focus• Content
• Evaluation & Documentation educational outcomes• Consumer info

Patient Education – A Safety Net • Consumer info
• Online Pharmacies • Increased usage • Average saving of 24% • Not all are regulated• The Ryan Haight Internet Pharmacy Consumer Protection Act of
2005
• Nongovernmental Institutional Controls• Individual institutions & accrediting agencies
• Safeguards in Drug Development, Manufacture, & Distribution in Canada• Similar to US
Importance of Nursing Management of Drug Therapy
• Nurses• Legally responsible for the drugs they administer • Safe drug administration
• Requires a thorough understanding of therapeutic drug actions and adverse drug reactions.
• Some clinical settings allow nurses to modify drug regimens
• Application of the nursing process to the pharmacologic aspects of patient care is especially important d/t long-term use of drug therapy • Necessary to control chronic disease processes
• Nursing management of drug therapy • An applied science

UNIT 2
Pharmacotherapeutics, Pharmacokinetics, and
Pharmacodynamics
Pharmacotherapeutics Key role in nursing drug management The study of desired therapeutic goal/effect from drug therapy The clinical purpose/indication—for giving a drug
• Can be to induce a cure or prevent a problem• Symptom relief• Cure• Prevention• Misc.

Pharmacotherapeutics (cont.)
• Nurses role in pharmacotherapeutics?• Need to question all orders
• Does the intended pharmacotherapeutics of a drug correlate with the patient’s reason for receiving drug therapy?

Pharmacokinetics
• Movement of the drug particles inside the body.
• Phases• Absorption• Distribution• Metabolism• Excretion

Pharmacokinetics: Process By Which Drugs Move Through The Body
• Drug molecules move during all phases of pharmacokinetics. • Drugs cross cell membranes in one of three ways:
1.Can pass between the spaces or channels between the molecules in the membrane
2. Can pass through the membrane with the help of a transport system (If Hydrophilic, helper proteins and enzymes, water soluble more steps involved, more time)
3. Can penetrate the membrane directly
(If lipophilic, no helpers needed, lipid soluble, less time)
• The chemistry of the drug particles also affects the movement of particles throughout the body
Principles of Absorption• Movement of drug from site of administration into
bloodstream• Rate of absorption depends on:
• Route of administration• Oral vs. Parenterally vs. IM vs SQ• Food or other drugs may interfere
• Speed of dissolving• Enteric coating

Principles of Absorption (cont.)
• Surface area• Blood flow• Lipid solubility• Drug concentration• pH

Principles of Distribution
• Movement of drug through bloodstream, into tissues, and into cells
• Distribution depends on:• Blood flow
• Most drugs do not produce it’s effect while in blood
• Drug’s ability to leave blood• Protein binding• Blood brain barrier• Placental membrane
• Drug’s ability to enter cells
Principles of Distribution and Protein Binding of Drugs
• Affects the distribution of a drug • A drug bound to protein is unable to pass thought the capillary
walls (protein needed to distribute through the blood)• Bonds will dissolve in time• Drug molecules will become free and active
• Dosages are calculated by the drug manufacturer based on the protein-binding characteristics of the drug
• Distribution of the drug is altered in a patient with a lower-than-expected protein level

The Effects of Administering Protein-Bound Drugs
QuestionWhat will be the result of administering a highly protein-
bound drug to a patient with liver failure?A. There will be no significant difference in the distribution of the drug.B. The drug will reach the target cells more quickly and therefore will not be as effective.C. The drug will reach the target cells more quickly, which could result in a toxic effect.D. The drug will take longer to reach the target cells, delaying the onset of action.

Answer and RationaleWhat will be the result of administering a highly protein-
bound drug to a patient with liver failure?
C. The drug will reach the target cells more quickly, which could result in a toxic effect.
• Patients with liver failure have lower levels of protein and albumin in their blood than patients without liver failure; therefore, the drug will reach the target cells more quickly, which could lead to a toxic effect. Remember that all recommended drug dosages are calculated based on a patient with normal protein levels
Blood–Brain Barrier—What & Why is it ?
• The capillary bed that services the brain is different from other capillary beds
• The cells are packed tightly together• Instead of wide spaces between the cells in the capillary walls
• This structure prevents drug molecules, and other foreign substances, from passing through and entering the brain.
• The purpose of the blood–brain barrier • Keep toxins and poisons from reaching the brain• At times, this mechanism will prevent treatment of a problem
Placental Membrane—What & Why is it ?
• Separates the maternal circulation from the fetal circulation
• It is not a barrier like the blood–brain barrier• Any drug that can pass through a membrane can pass through the placenta
• In order to pass through the placenta, a drug must be lipophilic, not ionized, and not protein bound.

Principles of Metabolism
• Conversion of drug into another substance(s)• Generally from substances that are lipophilic to hydrophyllic
• Sites of drug metabolism• Liver—Primary site• GI tract• Lungs• Kidneys• Skin
• Factors affecting metabolism• Liver function• Life span/gender• Lifestyle, diet, habits• Environment

Principles of Metabolism (Pharmacokinetics cont…)
• Biotransformation• Another term for metabolism
• Metabolites• Products of metabolism (the chemical the drug
becomes)• Metabolized drugs are generally changed into an
inactive form (inactive metabolite leaves body)• Prodrugs are drugs that are inactive until metabolized
into an active form• An active metabolite may cause a different and
potentially harmful effect, can cause adverse effects before leaves body
Principles of Metabolism (cont.)
• Rates of metabolism and first pass effect• Occurs at different rates for different drugs • Percentage of drug that is metabolized each time the drug
circulates, or passes, through the liver is the same• The total number of drug molecules that are metabolized
will be different• Drugs that are highly metabolized lose much of their
effectiveness during this first pass through the liver • This loss of effectiveness is called the first-pass effect. • These drugs may need higher oral doses to achieve a therapeutic level of
circulating drug

Principles of Metabolism (cont.)
• P-450 system• Microsomal enzymes are called the cytochrome P-
450 system• Liver metabolism is predominantly achieved by
these specific liver enzymes • The enzyme CYP3A4 is the most common• Some drugs either induce or inhibit the P-450 system• A large quantity of one of these enzymes is present,
more metabolism can occur through this pathway • T his increase in metabolism rapidly decreases
the amount of circulating drug

Principles of Excretion• Excretion
• Most common route for drug excretion through the urine
• Routes of excretion• Urine • Bile• Exhaled from lungs• Breast milk• Sweat• Saliva
Principles of Excretion (cont.)
• Factors affecting renal excretion• Glomerular filtration• Passive tubular reabsorption• Active tubular secretion• Diseases and pathophysiologic changes in the kidney decrease the
effectiveness of the kidney in drug excretion• Can be increased if the pH of the urine encourages the drug to
become an ion• Overuse of the active transport system
• Some of the drug particles will remain in the blood until they can be moved by the transport system
• Two drugs can be given together to slow deliberately the rate of excretion of one or both of the drugs

Question
What drug can be given with penicillin to slow the excretion of the drug?A. Birth control pill
B. Rifampin
C. Probenecid
D. Warfarin

Answer and Rationale
What drug can be given with penicillin to slow the excretion of the drug?
C. Probenecid
• Probenecid is a drug used to treat gout. In this situation, the probenecid is used not for its normal pharmacotherapeutic effect but solely to slow the rate of active transport and excretion of the antibiotic

Principles of Excretion (cont.)
• Factors affecting biliary excretion• Enterohepatic recirculation• Drug molecules that are in the bile are reabsorbed• This process lengthens the time the drug is present in the
bloodstream and can produce an effect

Misc Key Concepts • Half-life
• Amount of time required to remove half (50%) of the blood concentration of a drug
• Metabolism + excretion are responsible for elimination of a drug from the body
• Varies w/drug d/t pharmacologic properties• In one half-life, a set percentage of the drug
molecules present in the blood is eliminated

Critical Thinking Scenario• Half-life and Drug Dosing (p. 48)

Misc Key Concepts • Steady state
• The point at which the amount of drug being administered and the amount being eliminated balance off are equal
• Achieved @ four to five half-lives• Increasing the dose has no effect being achieved• Based on the amount of time required for four to five half-lives to
occur• Determines the full pharmacotherapeutic response of a
particular drug dose
Misc Key Concepts
• Clearance• Rate at which drug molecules disappear from the
circulatory system • Major modes of clearance
• Renal excretion • Hepatic metabolism
• Gender of the patient can also alter the clearance of some drugs
Pharmacodynamics
• Biological, chemical, and physiological actions of a particular drug within the body & the study of how those actions occur.• Responsible for therapeutic effects and sometimes
adverse effects• Drugs cannot create new responses in the body• Can only turn on, turn off, promote, or block a response
that the body is inherently capable of producing
Pharmacodynamics (cont.)
• Drug-Receptor Interactions• Most drugs create their effects in the body by attaching to
special sites, called receptors• At the receptor site, the drug is able to stimulate the cell to
act in a way that the cell is designed to act• Each type of receptor is responsible for producing a
particular effect in the cell • An agonist causes the cell to act • An antagonist or blocker prevents something else from
attaching to the cell blocking and action • If the drug is on the receptor, the other chemical cannot
also be on the receptor.

Pharmacodynamics (cont.)
• Occupancy Theory • Single occupancy theory
• The intensity of the body’s response to the drug is directly related to the number of receptors occupied by the drug
• The maximum response occurs when all of the receptors have drug molecules attached
• Modified occupancy theory• Different drugs have different strengths of attractions,
or affinity, for receptor sites. • Once a drug is attached to a receptor, it has different
abilities to stimulate the receptor

Pharmacodynamics (cont.)
• Occupancy Theory (cont.)• Receptor sensitivity changes
• Not static• Continual stimulation from an agonist usually makes the drug
less effective • Continual blockage from an antagonist usually makes the drug
more likely to react
• Nonrecepter responses• Drugs exert their effect by reacting physically or chemically
with other molecules in the body

Factors Influencing Drug Dose
• Potency • Amount of a drug that must be given in order to produce a
particular response
• Efficacy• The level of the drug and how well a drug produces its
desired effect• Minimum effective concentration
Factors Influencing Drug Dose
• Maintenance• Daily dose• Dose that is given consistently over time
• Loading doses• Larger than usual dose to reach an therapeutic effect
quicker• Is computed so that after some of the drug is eliminated,
the drug concentration in the body is still in the therapeutic range

Factors Influencing Drug Dose• Therapeutic index
• Difference between an effective dose and a toxic dose• Relation of ED50 to LD50 • If the amount of a drug required to be the ED50 is similar to the
amount that is the LD50, the mathematical ratio of the two values will equal a number close to one.
• When the ED50 and the LD50 do not differ by much, the drug is considered to have a narrow therapeutic index.
Factors Influencing Drug Dose
• Drug Dosage and Blood Concentration • The higher the drug levels within the body, the s more likely the
patient will experience adverse effects from drug therapy• Monitor blood levels of the drug
• Notify the caregiver if the level indicates that the blood levels are not in the therapeutic range
• The therapeutic range is an average • Varies with patient.





























