Embed Size (px)
DESCRIPTION
The NUJS MUN Conference '15 UNGA Background Guide
Citation preview

United Nations General Assembly
Agenda:
Improving and Ensuring Access to Life-saving Drugs
for LDCs and Developing nations.

NOTE FROM THE EXECUTIVE BOARD
Greetings Delegates!
Welcome to the General Assembly at the NUJS Model United Nations 2015. I,
Mimansa Ambastha, will serve as your Chairperson with Kirti Misra as your Vice-
Chair.
This background guide is merely a glimpse at the agenda at hand, and serves the
purpose of sketching out the key aspects that should be covered within the committee
during the conference. Your real research lies beyond this guide and we hope to see
some strong content and debate come our way.
An agenda relating to access to essential drugs has very rarely been discussed on
student platforms, much less Model UNs. However, the opportunity to discuss the
same will give us a chance to move beyond the realm of comfortable agenda-setting
and instead learn about new ones. This agenda particularly caught my eye as it so
greatly affects each one of us. It is not about a conflict in a far off place of the world or
about some financial hurricane toppling over Wall Street, but about something as
basic and essential as medicines which we consume on a regular basis. Thus,
increasing barriers to their access leads to a great cause for worry.
The agenda at hand is both vast and complex, and a successful discussion on it would
entail the collective participation of all of you. It shall be your prerogative to decide the
direction in which you want to take this committee. We hope to see a great level of
effort and enthusiasm from you all, so that we all can take back a great experience.
Happy researching!

INTRODUCTION
Over the last three decades, medical technologies have transformed many previously
untreatable diseases such as HIV/AIDS into manageable long-term conditions.
However, as the global disease burden evolves there is a continuing need to develop new
and more effective medicines. The challenge for policymakers is to establish an
environment that stimulates health innovation while ensuring widespread access to new,
more effective products to address unmet global health needs.
Target 6A of the Millennium
Development Goals1 acknowledges the
dire need to improve the availability of
Several countries have made considerable
strides towards increasing access to
necessary medicines and treatments to fight HIV/AIDS, malaria and tuberculosis,
however, the current stage of access to essential medicines in developing countries is not
nearly enough.
In countries for which there is information, the availability of medicines in the public
sector is only one third, while private sector availability is about two thirds, and the prices
people pay for lowest-priced generic medicines vary from 2.5 times to 6.5 times
international reference prices (IRPs) in these two sectors, respectively.2
Recent progress in a number of countries shows that access to essential medicines can be
improved through stronger partnership among governments, pharmaceutical companies
and civil society, including consumers, working together to ensure universal access to
essential medicines. The role of pharmaceutical companies, ranging from multinationals
to generic manufacturers to national distributors, is critical in this effort.
1 http://www.un.org/millenniumgoals/ 2 http://www.who.int/medicines/mdg/MDG08ChapterEMedsEn.pdf
The issues of innovation and access are inevitably
intertwined, cutting across distinct policy areas, in
particular, public health, intellectual property (IP) and
international trade. Finding the right balance between
health, trade and IP policies to sustain innovation and
ensure widespread access to life-saving technologies is one
of the primary public policy challenges of our time.

The third sustainable development goal (SDG)3
promote w ambitious goal which, like every other
SDG, has been broken down into various sub-goals. From child and maternal mortality to
epidemic diseases being all the way down to road traffic accidents, every area of human
mortality is covered.
sub goals offers us the following encouraging targets:
-care services,
including for family planning, information and education, and the integration of
reproductive health into national strategies and programmes.
3.8 Achieve universal health coverage, including financial risk protection, access to quality
essential health-care services and access to safe, effective, quality and affordable essential
3.c Substantially increase health financing and the recruitment, development, training and
retention of the health workforce in developing countries, especially in least developed
countries and small island developing States
3.d Strengthen the capacity of all countries, in particular developing countries, for early
warning, risk reduction and management of national and glo
The medicines themselves are categorised into many: reproductive, basic health
provision, epidemic resilience, medicament pricing and insurance, all of whom are
covered within the SDG. Although the indicators used to measure progress on these
targets and Goals have not yet been developed there is already a lot of political work to
be done.4
3 http://www.un.org/sustainabledevelopment/sustainable-development-goals/ 4 http://www.wipo.int/wipo_magazine/en/2013/05/article_0002.html

UNDERSTANDING LIFE SAVING DRUGS
What are life saving drugs?
Life Saving Drugs are those that satisfy the priority health care needs of the population.
They are selected with due regard to disease prevalence, evidence on efficacy and
safety, and comparative cost-effectiveness. These medicines are intended to be
available within the context of functioning health systems at all times in adequate
amounts, in the appropriate dosage forms, with assured quality, and at a price the
individual and the community can afford.5
The Model List of medicines6 is a guide for the development of national and
institutional essential medicine lists. It was not designed as a global standard. However,
for the past 30 years the Model List has led to a global acceptance of the concept of
essential medicines as a powerful means to promote health equity. Most countries have
national lists and some have provincial or state lists as well. National lists of essential
medicines usually relate closely to national guidelines for clinical health care practice
which are used for the training and supervision of health workers.7
Significance of Life Saving Drugs
Warming oceans and a changing climate are resulting in extreme weather patterns which
have brought about an increase of infectious diseases both new and re-emerging. These
extreme weather patterns are creating extended rainy seasons in some areas, and
extended periods of drought in others, as well as introducing new climates to different
regions. These extended seasons are creating climates that are able to sustain vectors for
longer periods of time, allowing them to multiply rapidly, and also creating climates that
are allowing the introduction and survival of new vectors. This has increased the urgency
of adequate disease control.
5 http://www.who.int/medicines/services/essmedicines_def/en/# 6 http://www.who.int/medicines/publications/essentialmedicines/en/ 7 http://www.who.int/selection_medicines/en/

The concept of Life Saving Drugs is forward-looking. It
incorporates the need to regularly update medicines
selections to reflect new therapeutic options and changing
therapeutic needs; the need to ensure drug quality; and the
need for continued development of better medicines, medicines for emerging diseases,
and medicines to meet changing resistance patterns.
Lists of such medicines guide the procurement and supply of medicines in the public
sector, schemes that reimburse medicine costs, medicine donations, and local medicine
production. Many international organizations, including UNICEF, UNHCR and UNFPA as
well as nongovernmental organizations and international non-profit supply agencies, have
adopted the essential medicines concept and base their medicine supply system mainly on
the Model List.
Medicines such as antibiotics and antiretroviral have dramatically improved health
outcomes in the same way that technologies such as medical imaging have transformed
diagnosis and treatment. Developing these complex products is an expensive and risky
business. Unlike other areas of technological development, medical innovation is all the
more challenging because of the ethical dimension of medical research, rigorous
regulatory oversight, liability issues, high costs and high failure rate. This helps explain
why IP protection is so important for companies involved in medical research and
development (R&D)8.
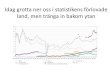
Public sector availability of medicines (given below) is low in all developing country
regions, and is consistently lower than in the private sector. In the 27 developing countries
for which data are available, average public sector availability was only 34.9 per cent.
When medicines are not available in the public sector, patients will have to purchase
medicines from the higher-priced private sector, or forgo treatment altogether. Since
health facilities in the public sector generally provide medicines at low cost or free of
charge, they are especially important for providing access to medicines for the poor. In
8 http://www.wipo.int/wipo_magazine/en/2013/05/article_0002.html
Addressing the root causes of low
public sector availability of medicines
can lead to substantial
improvements.

individual surveys, availability is reported as the percentage of medicine outlets in which
a medicine was found on the day of data collection.
Median
availability is
determined for
the specific list
of medicines in
each survey and
does not account
for alternate
dosage forms of
these products or
therapeutic
alternatives.
Public sector
data may be
limited by the
fact that the list of survey medicines may not correspond to national EMLs where these
exist and some public sector facilities may not be expected to stock all of the survey
medicines. Medicine availability is not guaranteed in private health facilities either. On
average, about one third (36.8 per cent) of private providers in developing countries lacked
availability of essential medicines, but in a sample of six countries in East, South-East and
South Asia the percentage was more than half (55.4 per cent).9
Cost of Manufacturing and Pricing Concerns
The high cost of many life-saving drugs not only keeps
patients from getting treatment, but also discourages
health ministries from improving the quality of patient
9 http://www.who.int/medicines/mdg/
Striking an appropriate balance
between encouraging medical
innovation and enabling access to it
has been a major preoccupation of
policymakers, health activists and the
private sector.

care through the use of newer and better medicines. While the $406 billion-strong drug
industry researches, develops, markets, and prices medicines for the industrialised world,
there is no mechanism to make newer medicines affordable to developing countries.
Newer drugs, which are usually under patent and more expensive than those off-patent,
are expected to become even more expensive with the implementation of the WTO
Agreement on Trade Related Aspects of Intellectual Property Rights (TRIPS) in all
Members, scheduled to be completed by 2006.
MNCs, emerging International Generic Suppliers and national manufacturer and
distributors constitute the normal private sector, profit driven, market competition basis
through which the vast majority of medicines are provided world-wide. Notwithstanding
the recognition that inadequacies in funding and demand side infrastructures are major
impediments to improving access, the organization of the supply side of the market has
been the subject of considerable criticism.
Over several decades, the capabilities of the major R&D based companies have evolved to
fit the business opportunities in the core developed world markets. Their foremost
strengths, therefore, are innovation through high levels of R&D expenditure and highly
functions. These are strongly oriented to
the demands of regulators and rapid
international diffusion of new products
through marketing. The penalties to the
business of falling foul of the exacting
standards of regulators, by squeezing
manufacturing costs, can be severe. Hence, the resources that make up the key
capabilities of primary and secondary manufacture, process maintenance and
development and quality assurance, tend to be of the highest order. The best up-to-date
Think of the businesses where value-based models are common.
Airlines use it to allocate scarce seats on popular flights.
Manufacturers of luxury goods use it to justify prices for goods
that are out of all proportion to the cost of production. As the
healthcare economist Jack Scannell points out, it is a way of
charging more.

plant and equipment are used and large numbers of top-class scientists and engineers
10
Anger and cynicism towards big pharmaceutical companies and their opaque pricing
policies with regards to essential medicines have been fuelled by reports like this.
Increasing incidents of price mark ups have come under public scrutiny, with increased
debate on how much life saving drugs should cost. While the pharmaceutical industry has
opted for the value-based approach, meaning maximum profits for them, it is very
questionable whether this is the right model for these companies to employ.
While it may be easy to walk away from other non-essential services, that is not the case
with life-saving remedies, especially when alternatives are non-existent or far less
effective. Aggressive value maximization also sits ill with a patent system that suppresses
competition by awarding a drug company a legal monopoly for a time to sell a drug it has
discovered.
Rationing is the ultimate consequence of high drug prices. Unsurprisingly, this is
unpopular and is causing a backlash. In a number of US states, politicians are seeking to
pass legislation forcing drug companies to disclose more information about the cost of
producing their high-priced remedies. There is even talk of capping prices.11
To understand the urgency of addressing price concerns, one only has to glance through
the statistics once. 99% of maternal deaths happen in developing countries because of
lack of funds and access to healthcare. This shows that economic reasons are one of the
major root causes of lack of medical aid access. Sparse affluence in developing countries
means that it is not profitable for big pharmaceutical corporations to sell life saving
medication there. There is much pressure on developing countries to provide for their
citizens and they (governments and local private organisations on the behalf of patients)
are subsequently forced to buy medicine at exceedingly high prices.
10 http://siteresources.worldbank.org/HEALTHNUTRITIONANDPOPULATION/Resources/281627-1095698140167/AttridgeImprovingAccessFinal.pdf 11 http://www.ft.com/cms/s/0/91b0cc8c-43fd-11e5-b3b2-1672f710807b.html#axzz3snYz25yU

Since lifesaving drugs are in high demand, which is unlikely to change with an increase
prices, big pharmaceutical companies have great incentives to set drug prices high in order
to receive a high return on investment for the research and development of a drug.
However, cases of 5,500%12 mark ups have very little justification.13
So how can a balance with regards to price and access be struck? Well, one way to tackle
the question is to look into Equity Pricing14. Another could be to look into working
around the WTO Intellectual property rights framework (discussed further), which has
enabled big companies to get away with exorbitant pricing practises. Newer innovations
by WHO and countries include suggestions of integrating traditional medicines with
drugs15.
BARRIERS TO ACCESS TO LIFE SAVING DRUGS
Apart from steep prices of medicines playing a role in hindering access to medication in
developing countries and intellectual property rights of pharmaceutical companies
allowing them to mark up prices, other barriers also exist to access to drugs.
1. Regulatory issues: Regulatory authorities are set up to assess the efficacy, quality and
safety of health commodities, provide approval for their distribution and support
authorization for their purchase. However, many low-income countries‟ regulatory
agencies are severely under-resourced, causing delayed registration of life-saving
commodities, a lack of oversight of the quality of products and general inefficiencies that
discourage manufacturers from engaging in the market.
2. Market failures: Another barrier affecting many life-saving commodities is market
failures, where return on investment is not sufficiently high to create incentives for
manufacturers to enter the market or sustain sufficient levels of production.
12 https://www.rt.com/usa/316046-pharma-daraprim-price-hike/ 13 http://globalnews.ca/news/2234578/sticker-shock-how-the-prices-of-life-saving-drugs-skyrocket-overnight/ 14 https://www.wto.org/english/tratop_e/trips_e/hosbjor_presentations_e/15thoen_e.pdf 15 http://apps.who.int/medicinedocs/pdf/whozip16e/whozip16e.pdf

3. User supply and demand challenges: The third main barrier affecting many of the
commodities is user supply and demand challenges such as low demand for the product
by end-users, local delivery and distribution breakdowns and incorrect prescription and
use. There has been an insufficient focus on optimizing innovative approaches to product
formulation, packaging and delivery devices.16
Insurance companies17 have also been accused of making it difficult to gain access to
medical aid. This is especially true in the case of families belonging to the relatively higher
socio-economic strata in society, where they can afford insurance, but may not
necessarily be able to pay full price for medicines.
Furthermore, an irregular supply of drugs may lead to interrupted and hence, ineffective
treatment. For example, In Kyrgyzstan, patients had their methadone doses sharply
reduced or were urged to stop treatment in 2005 due to delays in procurement and
distribution18.
Countries also face issues with corruption and wilfully hindered access to medicines by
law enforcement agencies and the bureaucracies. The public system is also plagued with
lack of adequate medical information to the right authorities, resulting in mistaken and
ignorant steps taken against innocent patients. In Indonesia, organizations report that
they are forbidden to make arrests in the clinic area; as a result, some patients report that
they have become targets for the police because they use other drugs in addition to
methadone19.
To further understand barriers to essential drug access in the case of specific medicines,
you can refer to the table given on the next page.
16 Source: https://www.unfpa.org/sites/default/files/pub pdf/Final%20UN%20Commission%20Report_14sept2012.pdf 17 http://www.sacbee.com/opinion/op-ed/soapbox/article16432784.html 18 https://www.opensocietyfoundations.org/sites/default/files/barriersfootnotes040808.pdf 19 STIGMA Foundation, Indonesia. Personal communication, July 16, 2007. On file at IHRD offices.

20
20 Source: https://www.unfpa.org/sites/default/files/pub-pdf/Final%20UN%20Commission%20Report_14sept2012.pdf

THE HUMAN RIGHT TO HEALTH
The right to health has been established as a fundamental human right of economic and
social nature in a number of international human rights treaties. As soon as 1945, the
United Nations (UN) Charter established the role of the UN as, inter alia
international cooperation in solving international problems of an economic, social, cultural or
humanitarian character, and in promoting and encouraging respect for human rights and for
fundamental freedoms for all without distinction as to race, sex, 21.
22 and
health 23. As an
economic and social right, the right to health is to be achieved progressively, according to
24 However, no treaty clearly defines what the right to
health consists in, what its scope is, and how to evaluate whether a state abides by its
obligations.
The international community seems to have become increasingly aware of its obligation
to guarantee the right to health in the context of development - out of the eight
Millennium Development Goals developed by the United Nations Development
Programme (UNDP) in September 2001, four goals are directly related to health, namely:
a) to reduce maternal mortality
b) to reduce under-5 child mortality,
c) to reverse the spread of HIV/AIDS
d) to ensure environmental sustainability by 2015.25
21 Article 13, United Nations Charter 22 Article 55(a) 23 Article 55(b) 24 International Covenant on Economic, Social and Cultural Rights, Art. 2.1 25 United Nations Development Programme (UNDP), Millennium Development Goals. Available at: http://www.undp.org/mdg/ [Accessed on 1st March 2014]

UNDERSTANDING PATENTING
When a pharmaceutical company first develops a new drug to be used for a disease
exclusive right to exploit it under law. Once the patent is acquired by the company it will
for use by patients). The drug is covered under patent protection, which means that only
the pharmaceutical company that holds the patent is allowed to manufacture, market the
drug and eventually make profit from it.
In most cases, the drug patent is awarded for around twenty years. The lifetime of the
patent varies between countries and also between drugs. Since the company applies for a
patent long before the clinic
the effective patent period after the drug has finally received approval is often around
seven to twelve years.
Once the patent has expired, the drug can be manufactured and sold by other companies.
At this point, the drug is referred to as a generic drug. According to guidelines in most
countries, including those from the US FDA, generic drugs have to be identical to the
branded drug. The company holding the initial patent may, however, renew the patent by
forming a new version of the drug that is significantly changed compared to the original
compound.
Compulsory licensing is when a government allows someone else to produce the
patented product or process without the consent of the patent owner, even before the
the TRIPS (Trade-Related Aspects of
Intellectual Property Rights) Agreement. When such a license is granted it means that the
exclusive monopoly of the patent holder is broken and a competitor can produce the
same drug, generally at more affordable prices. Thus, Compulsory licensing occurs when
a government licenses, or permits a third party to license
to use, manufacture, import or sell its patented invention,

consent.26
as poverty or high incidence of disease. However, signatories that undertake compulsory
lic
Article 31 of the TRIPS agreement states that where WTO member states provide in their
patent legislation for grant of compulsory licenses the following things must be kept in
mind by the deciding authority:
each case must be decided on its own merits;
the applicant for the compulsory licence must have initially made efforts to take a
licence from the patentee on reasonable commercial terms, but the patentee did
not agree;
the scope and duration of the compulsory licence must be limited to the purpose
for which it was granted;
the patentee must be paid adequate remuneration for use under the compulsory
licence;
the decision to grant a compulsory licence and the determination of what is
adequate remuneration shall be subject to judicial review;
TRIPS AGREEMENT
Virtually since the Agreement on Trade-Related Aspects of Intellectual Property Rights
(TRIPs) entered into force as part of the newly created World Trade Organization
(WTO) in 1995, WTO Member States and interested observers have recognized
that significant gaps exist in the agreement with respect to patent protection and
26WORLD TRADE ORG., Glossary Term: Compulsory Licensing, available at
http://www.wto.org/english/thewto_e/glossary_e/compulsory_licensing_e.htm (last visited 27 February 2014).

access to life-saving medicines in developing and least-developed countries (LDCs); but
finding and agreeing on improvements to the system has proven to be a much harder
proposition.
Although multilateral treaties on patents have existed since the late nineteenth century,27
for much of the twentieth century, countries that opposed pharmaceutical product
patents simply disallowed such patents. In the mid-1980s, as many as fifty countries
prohibited pharmaceutical product patents; this list included a few developed countries,
such as Spain and Portugal, but consisted primarily of large middle- and low-income
nations, such as Brazil, India, Mexico and Egypt.28 Around this time, industries across a
variety of sectors in the United States claimed that they were suffering heavy losses
because of the absence of adequate intellectual property protection in foreign markets.
The U.S. International Trade Commission confirmed these claims, estimating that
American firms were losing about $50 billion a year from lack of overseas intellectual
property protection. This led American businesses to call upon their government to seek
greater intellectual property protection in international trade agreements.29
When the Uruguay Round of multinational trade negotiations began in 1986, the United
Stat -Related Aspects of
27 Paris Convention for the Protection of Industrial Property, July 14, 1967, 21 U.S.T. 1583, translated in G.H.C.
BODENHAUSEN, GUIDE TO THE APPLICATION OF THE PARIS CONVENTION FOR THE
PROTECTION OF INDUSTRIAL PROPERTY 17 (1968).
28 Karin Timmermans & Togi Hutadjulu, THE TRIPS AGREEMENT AND PHARMACEUTICALS, REPORT
OF AN ASEAN WORKSHOP ON THE TRIPS AGREEMENT AND ITS IMPACT ON PHARMACEUTICALS,
WORLD HEALTH ORG. 11 (2000).
29 The American pharmaceutical industry was particularly instrumental in lobbying for greater intellectual property
protections.

On January 1, 1995, the Uruguay Round of negotiations ended with the establishment of
the WTO, whose members were all required to sign on to the new, binding TRIPS
agreement.30
Section 5 of Part II of this agreement covers patents, and Articles 27 and 28, which form
the core of this section, grant pharmaceutical innovators strong patent protections. Article
27 establishes a ceiling for patentability requirements, by requiring that patents be
for any inventions . . . in all fields of technology, provided that they are new, involve an
inventive step and are capable of industrial application 31 The article confirms that TRIPS
requires all its signatories to allow pharmaceutical product patents.
Article 28, which defines the rights conferred by a patent, prohibits third parties from
the consent of the patent holder. It thus prevents generic drug manufacturers from
infringing upon pharmaceutical product patents. Together, Articles 27 and 28 of TRIPS
establish an international patent protection regime for pharmaceutical products. Over
seventy countries signed on to TRIPS at the start of 1995, including Spain, Portugal, Brazil,
India, Mexico and Egypt. Today, with over one hundred and fifty TRIPS signatories,
Articles 27 and 28 enjoy near-universal authority. Signatories that violate these Articles, or
resolution body, which may allow other signatories to impose retaliatory trade
sanctions.32
Contrary to public opinion, TRIPs does not provide for a global system of intellectual
property protection; meaning Members do not automatically recognize other M
patents. Instead, inventors must apply for protection in each Member State in which they
wish to be protected.
30 WORLD TRADE ORG., Overview: The TRIPS Agreement, available at
zttp://www.wto.org/english/tratop_e/trips_e/intel2_e.htm (last visited 27 February 2014).
31 TRIPS, supra note 7, art. 27.
32 Ruth Okediji, TRIPS Dispute Settlement and the Sources of (International) Copyright Law Part II, 49 J. OF COPYRIGHT
SOC. OF THE U.S.A. 585, 595 (2001).

TRIPs also includes a number of transitional provisions, such as granting LDCs until
January 2006 to comply with TRIPs and giving developing countries that have
never legislated on intellectual property rights until January 2000 to apply some
TRIPs provisions, while giving them until January 2005 to apply other provisions,
including several provisions of particular importance to pharmaceuticals. Importantly
(and controversially), TRIPs also includes a number of exceptions to the exclusive rights of
the patent holder. The most important of these exclusions are the general exceptions
provided by Article 30, the compulsory licensing provision of Article 31, and the parallel
importing clauses contained in Articles 28 and 5.
Many developing countries and non-governmental organizations (NGOs) rapidly grew
frustrated waiting for WTO Members to improve the situation of medicinal access in poor
countries, losing the battle against such public health epidemics as tuberculosis, malaria,
and HIV/AIDS and actively campaigned for both structural and operational changes
within the WTO. While those groups succeeded in getting public health issues on the
agenda at the Third Ministerial Conference, held in Seattle in 1999, the process of
resolving several key health issues did not solidify until the Fourth Ministerial
Conference, held in Doha, Qatar in 2001 (Doha Round).
-
The key in evaluating the policy trend of TRIPS in relation to the pharmaceutical industry
is to look through the lens of its Article 7 objective to balance two competing interests:
promoting innovation of new drugs and providing access to these drugs. For example,
nations with weak economies and public health crises want medication for their people
while innovative pharmaceutical companies want to protect their temporary exclusive
rights in order to recoup their investment and maximize profits. At that time, the original
TRIPS agreement took on a utilitarian posture. It placed more emphasis on promoting
innovation than on providing access to essential drugs, thereby favoring member nations

that enjoy the majority of pharmaceutical innovation. Recognizing this inequity, the
WTO decided to place more emphasis on public health.33
In 2001, the WTO Ministerial Conference officially initiated the Doha Agenda with a
declaration [hereinafter Doha Declaration] that acknowledged the need to recognize a
sovereign nation's right to protect public health, even at the expense of intellectual
property rights. Namely, the Doha Declaration affirmed a sovereign nation's authority to
grant compulsory licenses during national emergencies and to define what constitutes a
national emergency. A country that was suffering a major epidemic could compel
licensure for domestic production of patented medication that they could not otherwise
afford.
Still, the Doha Declaration fell short of its objective to "promote access to medicines for
all." Even with a compulsory license, many countries with severe health epidemics did
not have the means or capacity to manufacture drugs. Nonetheless, TRIPS required that
the majority of manufacture and sales resulting from compulsory licensing must be
limited within the domestic market. Furthermore, the license was non-assignable; a
country in dire straits could not assign a compulsory license to a nearby country that had
adequate capacity to manufacture and sell generic versions of the drug at an affordable
price. Recognizing these shortcomings, the WTO met again in 2003 to continue
negotiating on the Doha Agenda at the Fifth Ministerial Conference in Cancun.34 There,
they passed the Implementation Decision which extended compulsory licensing
provisions by temporarily removing limitations on exports of drugs under a compulsory
license to countries that could not manufacture drugs themselves.35 This decision was
adopted by the General Council in consideration of the Chairperson's statement, in which
33 http://www.nyulawglobal.org/globalex/TRIPS_Compulsory_Licensing.html#_B._Evolution_and_Trend of TRIPS: Th 34 The accounts of day-to-day discussions and negotiations can be found on the WTO website. WTO
Ministerial Conferences, Cancun 5th Ministerial, at
http://www.wto.org/english/thewto_e/minist_e/min03_e/min03_e.htm
35 WTO General Council Decision, Implementation of Paragraph 6 of the Doha Declaration on the TRIPS Agreement and Public Health, WT/L/540, (Aug. 30, 2003), at http://www.wto.org/english/tratop_e/trips_e/implem_para6_e.htm

he reassured the members that compulsory licensing is to be used in good faith and
stressed the need to prevent diversion of supplied drugs.36
In 2005, during a ministerial conference in Hong Kong, the General Council agreed to
make the Implementation Decision permanent by amending TRIPS. Now, a country that
is eligible for compulsory licensing but lacks sufficient drug manufacturing capacity can
import drugs from an exporting member that is also operating under a compulsory
license, subject to certain conditions.37 That is, the TRIPS Council must be notified before
a cross-border compulsory license can be issued, but approval is not required. However,
remedial measures to resolve conflicts from alleged abuse of the system remain vague.
Thus, the TRIPS Council's sentiment, with respect to their goal of striking a balance
between the competing Article 7 interests, has shifted from favoring IPRs to favoring
wider access to drugs for the benefit of public health. There are, however, uncertainties as
to whether the amendment will achieve its purpose.
Despite the WTO's tremendous efforts to create a diplomatic compulsory licensing
system that improve access to prescription medicine, the latest TRIPS amendment did not
resolve several existing issues and even created some new concerns. Particularly
troublesome are the lack of specific requirements in determining eligibility for compulsory
licensing, risks of arbitrage and production of counterfeit drugs, and whether TRIPS, in its
current construction, will actually help developing countries gain accessory to essential
drugs.
36 WTO Intellectual Property, General Council Chairperson's Statement (30 August 2003), at http://www.wto.org/english/tratop_e/trips_e/gc_stat_30aug03_e.htm 37 The Hong Kong Declaration defined an "exporting member" as a WTO member nation that manufactures drugs under a compulsory license to export to nations that require a compulsory license but lack the capacity to produce drugs domestically.

ISSUES TO ADDRESS
1. How far has your country been successful in meeting the health clauses in MDGs? How can your methods be translated into international action?
2. What is the best way to define a life saving drug? How can the International and National Lists of Life Saving Drugs be reconciled?
3. What role can the public sector play in bettering medical aid access?
4. What problems are faced by your country with regards to access to essential medicines? How have they been addressed? What is the rate of success of these measures?
5. What pricing mechanism can be employed to make the cost of medicines less exorbitant?
6. How does the patenting of drugs effect price of essential drugs? What is the concept of -
7. What can countries do to reconcile their public health needs with the need to grant patent protections to drugs?
AREAS OF RESEARCH
1. Meaning of life saving drugs
2. Past international agreements and obligations relating to life saving drugs
3. Barriers to access to such drugs and remedies for the same
4. Meaning of patents and provisions relating to patents under the TRIPS Agreement of the WTO
5. Suggestions to improve the conflict between patent protection and access to life saving drugs.