Embed Size (px)
Citation preview

J Clin Pathol 1984;37:272-278
Tuberous sclerosis: unusual associations in four casesEB ILGREN,* D WESTMORELANDtFrom the *Department of Neuropathology, Radcliffe Infirmary, Oxford, and tJohn Radcliffe Hospital,Headington, Oxford
SUMMARY Tuberous sclerosis is a rare disease with classic primary or secondary changes affectingmainly the cerebrum, skin, kidneys, and heart. Such lesions are generally hamartomatous andthus display malignant features only in rare cases. This paper describes four cases of tuberoussclerosis which were unique in their association with certain unusual congenital, metabolic, andtumorous conditions.
Gomez' recently reiewed 160 cases of tuberoussclerosis seen at the Mayo Clinic between 1935 and1964. He defined both primary and secondary fea-tures of the condition. The primary featuresincluded lesions not only in the central nervous sys-tem such as cortical and subependymal tubers andretinal hamartomas, but also in other systems, suchas the skin, including cutaneous angiofibromas andsebaceous adenomas. Secondary tuberous sclerosislesions were considered to be shagreen patches,multiple renal tumours, and cardiac rhabdomyomas.In addition to these classic lesions, a multitude ofother associated abnormalities have been describedin tuberous sclerosis.' We describe here fourpatients with tuberous sclerosis in whom several ofthe associated lesions were congenital, metabolic,and tumorous conditions that have not hitherto beendescribed.
Case histories
MATERIAL AND METHODSThe diagnostic indices of the Department of His-topathology of the John Radcliffe Hospital, Oxford,were searched over the years 1935 to 1970 for casesof tuberous sclerosis studied at necropsy. Histologi-cal slides from each of these cases were recut whennecessary and stained with haematoxylin and eosin,haematoxylin and van Gieson (HVG), phos-photungstic acid haematoxylin (PTAH) and periodicacid Schiff.
RESULTSNine cases of tuberous sclerosis with postmortemfindings were found, and four of these, because oftheir unusual features, are described in detail.
Accepted for publication 16 November 1983
CASE 1 (21 year old woman)
Clinical historyAt one year of age adenoma sebaceum wasdiagnosed. Five years later she developed epilepticfits and an electroencephalogram showed diffuseslow wave activity. At 17 years of age she developeda right spontaneous pneumothorax, which wastreated by talc pleurodesis. Bullae were seen atoperation. One year later she developed left sidedabdominal pain and was found to have bilateral"polycystic" kidneys. Shortly thereafter shedeveloped a left sided spontaneous pneumothorax,which was treated by a parietal pleurectomy. Onceagain bullae were seen at operation.At the age of 20 she was found to be hypercal-
caemic with no reduction in calcium concentrationsduring a standard hydrocortisone suppression test.The patient also had a reduced creatinine clearance.Nephrotomograms showed multiple lucent areaswithin both kidneys. Bone radiographs were nega-tive for osteitis fibrosa, although cystic changes wereseen in the terminal phalanges-changes consistentwith tuberous sclerosis lesions. Her blood pressurewas 150/95 mm Hg. Chest x ray examinationshowed "honeycomb" changes in both lung fieldsand her pulmonary function tests were abnormal(DCO 10*3, predictive 31-3). Other investigationswere normal: these included haemoglobin concen-tration; white blood cell count; erythrocyte sedimen-tation rate; blood urea, glucose, thyroxin, and plas-maprotein concentrations; electroencephalogram;electrocardiogram; and skull x ray examination.Multiple filling defects were found on the liver scan.A year later the patient underwent parathyroidec-
tomy, and four hyperplastic parathyroid glands werefound (histology showed chief cell hyperplasia).Postoperatively she was treated with dihydrotachy-
272
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from

Tuberous sclerosis: unusual associations in four cases
sterol, and six days after operation was normocal-caemic and several months later normotensive. At22 years of age the patient developed haemoptysisand one year later developed paroxysmal nocturnaldyspnoea due to cor pulmonale. In addition, she hadabdominal pain, tachycardia (140 beats/min), andcongestive heart failure -(jugular venous pressure
raised about 5 cm) and was also found to bethyrotoxic. Shortly before her death right and leftventricular heaves and a third heart sound with ves-
icular breath sounds within the apices of both lungswere noted on examination. The day before she diedthe patient developed sepsis. Laboratory investiga-tions at this time showed the following: haemoglo-bin 9 g/dl, a raised erythrocyte sedimentation rate(28 mm in the first hour), calcium concentration2-35 mmolI, normal liver function tests, a reducedserum iron concentration (6 ,ug/l, normal 13-32 ,ug/1), and a raised thyroxine concentration (216 ug/l,normal 75-145 ,ug/l). A blood film showed 260leucocytes but none of them polymorphonuclear.Four blood cultures were negative. Lymphocytesaccounted for 76% and monocytes for 20% of theleucocytes.
Family historyThe patient's mother, who also had a slight degreeof adenoma sebaceum, was found to have headachesat the age of 51 and also to be hypertensive andhypercalcaemic. Hyperparathyroidism was diag-nosed and four hyperplastic parathyroid glands wereremoved.
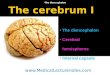
Pathological findingsNervous system. Although the brain was of normalsize (1250 g), some gyri were abnormally small andfirm with numerous cortical tubers. (Fig. 1 and 2)On section there were "candle gutterings" along thesurfaces of both lateral veittricles. The brain stemand cerebellum showed areas of abnormal firmnesspredominantly in the white matter. Histologically,there were numerous malformed cortical layers (Fig.3) in the cerebrum and these contained largeabnormally shaped cells probably either neuronal orastrocytic in origin (Fig. 4). There was alsocalcification in small areas of the cerebrum and giantheterotopic neurones in the brain stem and cerebel-lum.Heart. The heart showed right ventricular hypertro-phy. There was also a rhabdomyoma within the apexof the left ventricle, and mural thrombi were foundover the endocardium of both ventricles.Skin. There were multiple areas of adenomasebaceum over the skin of the nose and cheek andnumerous subungual fibromata.Liver. The liver was enlarged (2050 g) and con-tained six white nodules, the largest of which meas-ured 6 cm in diameter. Microscopically, several ofthese were found to be angiomyolipomata.Pancreas. There was a large islet cell tumour (Fig. 5)adjacent to the pancreas.Lungs. Multiple small cysts and nodules around 1cm in diameter were found throughout each lung.Histologically, the pulmonary lesions containednumerous macrophages and many small nodules ofproliferating smooth muscle. In addition, the small
Fig. 1 Cerebral hemispheres(1-low power) showing typicalcortical "tubers" with firm,raised, smooth, somewhatexpanded, umbilicated gyralcrests.
273
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from

2lgren, Westmoreland
g Fig. 2 Detail of Fig. 1.
F 4 I o F.- 3. Sie x 20.Fig. 4 Detail of Fig. 3. Silver x 200.
Fig. 3 Microscopic section ofcortex showing moderatedisorganisation ofnormal laminar pattern with occasionalgroups of very large cells either neuronal or astrocytic incharacter. Silver x 50.
pulmonary arterioles were rather hypertrophic.Adrenal and pituitary glands. Adenomata werefound in the right adrenal gland and in the pituitarygland.Kidney and para-aortic lymph nodes. Both kidneyswere considerably enlarged, the left kidney weighing765 g (19 x 12 x 9 cm) and the right kidney weigh-ing 500 g (18 x 9 x 5 cm). The right kidneyappeared to be largely replaced by a focally haemor-rhagic angiomyolipoma while the left kidney con-tained both angioliposarcoma as well as areas ofadenocarcinoma (Fig. 6). The adjacent para-aortic
274
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from

Tuberous sclerosis: unusual associations in four cases
-s.-~
S49.- .. = w .. ,....
.. _r. ..
r ~ :
r ~ ~ ~ ~ ,__ b*.
_ _ ~%et.-.__S9L1b+-RiX¼.
Fig. 5 Islet cell tumour of the pancreas showingcompressed pancreatic acini (top) and tumour (below).Haematoxylin and eosin x 50.
f*
4>t**o^,£
ptts
Vt.f* ''
C\ \ 40 t* ^1 $
*'.tst: f* &sw* # -4,s9
~~ ~~I'
Fig. 6 Renal cell adenocarcinoma and angioliposarcoma.(a) Normal renal tubule with focal dysplasia (arrow).(b) Adenocarcinoma. (c) Angioliposarcoma with tumourin vessel. Haematoxylin and eosin x 200.
I
._
275
a&O. d
1.
0-ft-1 I .
. .'..%4wl- -.. too -
I.-
q.
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from

276
Ai''e : ,* -.
V~~~~~~~~~Y,,
Fig. 7 Infiltration ofpara-aortic lymph nodes byangiomyoliposarcoma. Haematoxylin and eosin x 50.
lymph nodes measured up to 2 5 cm in diameter andappeared to be replaced by soft pink tissue. His-tologically, the latter resembled areas of renalangiomyoliposarcoma and this could be seen invad-ing small vessels within the lymph node (Fig. 7).
Summary ofpathological changes:1 Cortical tubers2 Cardiac rhabdomyoma3 Subungual fibromas4 Adenoma sebaceumAssociated with:1 Multiple endocrine adenomatosis affectingpituitary gland, adrenal gland, parathyroid gland,and pancreas (islet cell tumour).2 Renal angiomyoliposarcoma and adenocar-cinoma with regional lymph node metastases3 Pulmonary and hepatic angiomyolipomata
CASE 2 (6 week old boy)
Clinical historyThe clinical history was lost, although it is knownthat the patient's mother and brother had tuberoussclerosis.
Pathological findingsNervous system. The cerebrum showed multiple cor-tical nodules, which were prominent in the left tem-poral (3 cm in diameter) and right frontal (3 cm indiameter) lobes. There was also "candle guttering"along the surfaces of the lateral ventricles with sub-
ligren, Westmoreland
ependymal gliosis in the region of the thalamus andthe caudate nucleus.Heart. There was a rhabdomyoma within the leftventricular myocardium. An infantile aortic coarcta-tion was also found.Lungs. The lungs were focally atelectatic and therewas meconium stained material within the bronchi.Kidney. There were small cysts within the proximaltubules of both kidneys.
Summary ofpathological lesions:1 Cerebral tubers2 Cardiac rhabdomyoma3 Renal cystsAssociated with:1 Infantile type of aortic coarctation
CASE 13 (2 month old girl)
Clinical historyOnly a limited history was available. The child waswell before her admission except for a history ofcontinued nasal discharge. The culture of the dis-charge was positive for Staphylococcus aureus. Thepatient was also hypercalcaemic before death.
Pathological findingsNervous system. The brain contained numerousgiant heterotopic neurones round the aqueduct ofsylvius, lower brain stem, and cerebrum.Heart. The heart showed biventricular hypertrophyand contained a fibromuscular tumour obstructingthe outflow tract of the left ventricle.
Fig. 8 Universalis calcinosis. Focal deposits ofcalcium canbe seen in the subdural connective tissue. Von Kossa x 40.
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from

Tuberous sclerosis: unusual associations in fouir cases
UF t
Skin. There was a diffuse patchy pigmentation of theskin. Numerous subcutaneous nodules, plaques, andridges were found particularly along the left side ofthe back, neck, and face, some of which were centr-ally ulcerated. Histologically, there was much focalsubcutaneous calcification (Fig. 9) which resembledthat seen in universalis calcinosis.Lungs. The lungs were focally atelectatic withnumerous areas of fibrosis and lymphocytic infiltra-tion.
Summary ofpathological lesions:1 Neuronal heterotopias2 Cardiac fibromyomas
277
Fig. 9 Dysplasia andhyperplasia ofcerebellar mantlelayer. Haematoxylin and eosin.(a) Lower power x 40. (b) Highpower x 150.
Associated with:1 Universalis calcinosis2 Pulmonary fibrosis
CASE 4 (8 week old girl)
Clinical historyOnly a limited history was available. The patient hada three week history of respiratory distress andpostprandial vomiting before death. On examina-tion she was found to be a thin small baby withspasticity of all four limbs and bilateral talipes, hold-ing her arms in flexion and legs in extension.
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from

278
Pathological findingsNervous system. At necropsy, both cerebral hemis-pheres were found to be nodular. Microscopically,these areas were considerably gliotic, containingneuronal heterotopias often consisting of epen-dymoblasts forming rosettes. In addition, focal cor-tical and subependymal glial abnormalities wereseen in many parts of the cerebrum and the brainstem. There was considerable focal proliferation anddisorganisation of the mantle layer of the cerebel-lum (Fig. 9) with local invasion of the subarachnoidspace.Skin. There were numerous shagreen patches overthe face.
Summary ofpathological lesions:1 Cortical tubers with neuronal heterotopias of thecerebrum2 Shagreen patchesAssociated with:I Cerebellar dysplasia and possibly neoplasia(medulloblastoma)
Discussion
Tuberous sclerosis is relatively rare and occurs inabout one in 100 000 to 170 000 people in the gen-eral population (see Table 13.4 in Kuntz andGomez2). Its infrequency is also strongly suggestedby Gomez's study,' in which he found only 160 casesin 1-5 million patients seen at the Mayo Clinic over30 years.Most cases of tuberous sclerosis recorded to date
have had classic primary or secondary lesions.' Thepatients described in this report are exceptionalsince certain congenital, metabolic, and tumorousconditions were seen in association with their tuber-ous sclerosis. The multiple endocrine adenomatosissyndrome found in case 1 has not, to our knowledge,been described before in association with tuberoussclerosis, although Gutman3 recorded an islet celltumour of the pancreas in patients with this disor-der. Case 1 is even more unusual in its associationwith an angioliposarcoma4 and a renal cell car-cinoma,56 since most renal tumours in tuberoussclerosis are benign. Case 2 is unusual in its associa-tion with aortic coarctation since only one such casehas been described previously.7 Universalis cal-cinosis, which was found in case 3, has not previ-ously been seen in patients with tuberous sclerosis.Finally, in case 4 the finding of a pronounced prolif-eration of the cerebellar mantle layer is most strik-ing. Cerebellar lesions, as described by Reagan,8 are
Ilgren, Westmorelandseen infrequently in patients with tuberous sclerosisin.comparison with the relatively common cerebraltubers.9 Moreover, the precise nature of the cerebel-lar changes seen in case 4, whether dysplastic orneoplastic, remain speculative. Urich " describedfocal cerebellar dystopias ranging from "minor mal-formations to total cortical disorganisation". Thesubarachnoid space invasion found in case 4, how-ever, is more likely to be neoplastic change than adystopic or dysplastic alteration and thus resemblesan "incipient medulloblastoma".
I am indebted to Mr Ron Beesley for cutting andstaining many of the sections described. I am grate-ful to Mr John Hayward for photographic assistanceand to Mrs G Ilott for typing of the manuscript. I amalso grateful to Dr Michael Dunnill for reviewingthe sections described in this paper and for hisencouragement and to Dr RH Lindenbaum, Chur-chill Hospital, and Dr Jennifer Dennis, Park Hospi-tal, for their comments. Finally, I am grateful to DrJoan Rivett, Department of Pathology, Stoke Man-deville Hospital, for the postmortem report andblocks of case 1.
References
'Gomez MR, ed. Clinical experience at the Mayo clinic. In:Tuberous sclerosis. New York: Raven Press, 1979:27-54.
2 Kuntz NL, Gomez MR. Genetics, population studies, andpathogenesis. In: Tuberous sclerosis. New York: Raven Press,1979: 207-20.
Gutman A, Lephkowitz M. Tuberous sclerosis associated withspontaneous hypoglycaemia. Br Med J 1959;ii: 1065-8.
4 Hartveit F, Harreaker B. A report of 3 angiolipomyomata and 1angioliposarcoma. Acta Pathol Microbiol Scand1960;49:329-6.
Kavaney P, Fielding I. Angiomyolipoma and renal cell carcinomain the same kidney. Neurology 1963;6:643-6.
6 Berg J. Angiomyosarcoma of kidney (malignant hamartomatousangiomyolipoma) in a case with solitary metastasis from bron-chogenic carcinoma. Cancer 1955;8: 759-63.
7Rabinowicz T. Les tumeurs cerebrales chez l'homme. Bull AcadSuisse Sci Med 1968;24: 144-67.
Reagan TJ. Neuropathology. In: Tuberous sclerosis. New York:Raven Press, 1979:69-84.
Van Bogaert L, Paillas JE, Berard-Badier M, Payan H. Etude surla sclerose tubereuse de Bourneville a forme cerebelleuse. RevNeurol 1958;98:673-89.
0 Urich H. Malformations of the nervous system, perinatal dam-age, and related conditions in early life. In: Blackwood W,Corsellis J, McMinimy W, eds. Greenfield's neuropathology.London: Arnold Press, 1977:361-470.
Requests for reprints to: Dr EB Ilgren, Senior Registrar,Department of Neuropathology, Radcliffe Infirmary,Oxford OX2 6HE, England.
on March 26, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.3.272 on 1 March 1984. D
ownloaded from
![InsectArcade: A hybrid mixed reality insect-robot system ...placed[19, 20]), is composed by the proto-cerebrum, deuto-cerebrum and trito-cerebrum. The proto-cerebrum carries the optic](https://img.dokumen.tips/doc/110x75/5e3e8c8bcd87563f096bceb8/insectarcade-a-hybrid-mixed-reality-insect-robot-system-placed19-20-is.jpg)