Embed Size (px)
Citation preview

Treatment of leptomeningeal dissemination of medulloblastoma
Report of a case with a long-term survival
C.J.T. Stevering*, F.J.M. Gabreels”, R.J.J. Lippens* *, W.O. Renier”, H.O.M. Thijs- sen * * * and H.J. ter Laak*
Introduction
Medulloblastoma is an invasive, fast growing
glioma which comprises one fifth of all intracra-
nial tumors in childhood. The tumor arises from
undifferentiated neural cells in the roof of the
developing fourth ventricle, which normally mi-
grate in dorsal and lateral direction to form the
external granular layer of the cerebellum.
Therefore, the tumor may arise anywhere along
the path taken by these cells, but is commonest
in the vermis’.‘.
Medulloblastoma extends in the meninges by
continuous infiltrative growth, and metastasizes
throughout the sub-arachnoid space of skull and
especially spinal canal. Spinal metastases may
occur anywhere in the spinal sub-arachnoid
space but show a predilection for the caudal part
as dropmetastases3.1.
Spinal metastases are either diffuse or nodu-
lar. In the former, the whole cord and its roots
may be covered by a thick layer of tumor tissue,
predominantly at the posterior side. The dis-
crete nodular metastases are often situated
upon the posterior side of the roots of the cauda
equina5.
Radicular pains, muscle weakness and cauda
equina syndrome are the predominant features.
The diagnostic procedures include besides a
neurological examination, myelography, CSF
cytology and biochemical investigationP.
There is a moderate variation on the inci-
Summary
A case report is presented of a boy suffering from medulloblastoma with grade IV spinal cord involvement and a survival of almost 3 years after the occurrence of spinal metastases. A review is given of the literature, with special attention to diagnostic procedures (CSF deter- minations, myelography) and therapeutic regimens.
Key words: Medulloblastoma, spinal cord me- tastases, CSF parameters.
dence of spinal cord involvement reported by
several authors, chiefly attributable to the use of
myelography. From the patients with newly
diagnosed medulloblastoma. 4-36% show an.
often asymptomatic, spinal cord involve-
merit’-I’. In 5-33% of the treated patients, spinal
metastases occur after an interval of 7-32
months7-1J.
Gerosa et al.‘? distinguish four degrees of spi-
nal cord involvement:
I clinical signs of spinal cord involvement with
negative CSF cytology and negative myelo-
graph y j II clinical signs of spinal cord involvement with!
questionable CSF cytology and negative
myelography,
* Institute of Neurology. * * Institute of Pediatrics and * * * tnstitute o,f Diagnostic Radiology. Department of Neuroradiology, St. Radhoud Hospital. University of Nijmegen, The Netherlands
Address for correspondence and reprint requests: F.J. M. GahreSls, Department of Child Neurology, Institute of Neurology, St. Radhoud University Hospital. Box 9101. 6500 HB Nijmegen, The Netherlands.
Accepted I .X. X5
Clin Neurol Neurosurg 1985. Vol. 87-4.
291
ffi clinical signs of spinal cord ~nvolv~nlent with positive CSF cytology and negative myelo-
graphy , IV clinical signs of spinal cord involvement with positive CSF cytology and positive myelo-
graphy. In this paper, we describe a boy with exten-
sive grade IV spinal cord involvemeflt and long- term survival, and review the literature on ma- nagement of spinal metastases of medullo-
blastoma.
Case report
In November 1978, a 7,9-year-old boy was refer- red to our department on suspicion of a poste- rior fossa tumor. After admission, a ventricu- lo-atria1 drain (Spitz-Holter) with Rickham- reservoir was placed because of raised intracra- nial pressure (Institute of Neurosurgery, Head Prof.Dr. H.A.D. Walder). A posterior fossa craniectomy revealed a tumor attached to the floor of the fourth ventricle and invading both cerebellar hemispheres. The tumor was subto- tally resected. On pathological examination, the tumor appeared to be an undifferentiated medulIablostoma.
Postoperatively, after a 21 days interval, cra- nio-spinal irradiation and adjuvant chemothe- rapy according to the protocol of the Internatio- nal Society of Paediatric Oncology (SIOP) were performedIs.
In June 1982, the boy was readmitted to our department because of headache, and periods of nausea and vomiting. During the clinical ob- servation period, he developed radicular pains in the legs, a broad-based gait and a restriction of the head mobility in all directions. The ankie jerks disappeared, and both the signs of Lher- mitte and of Lasbgue bilateral became progres- sively positive on 10”.
A CT scan with contrast enhancement de- monstrated signs of slight central atrophy, but no evidence of recurrent tumor in the posterior fossa. Analysis of the intensive xanthochromic CSF showed an increased total protein content of 17.1 g/l, and 3 weeks later even 27 8/l (normal 0.15-0.32 g/I). Lactate and pyruvate levels in CSF were increased to respectively 5200 umoVt (normal 1300-1500 ymoV1) and 156 pmoI/l (nor- mal 91-135 ~rno~l). Glucose concentration was
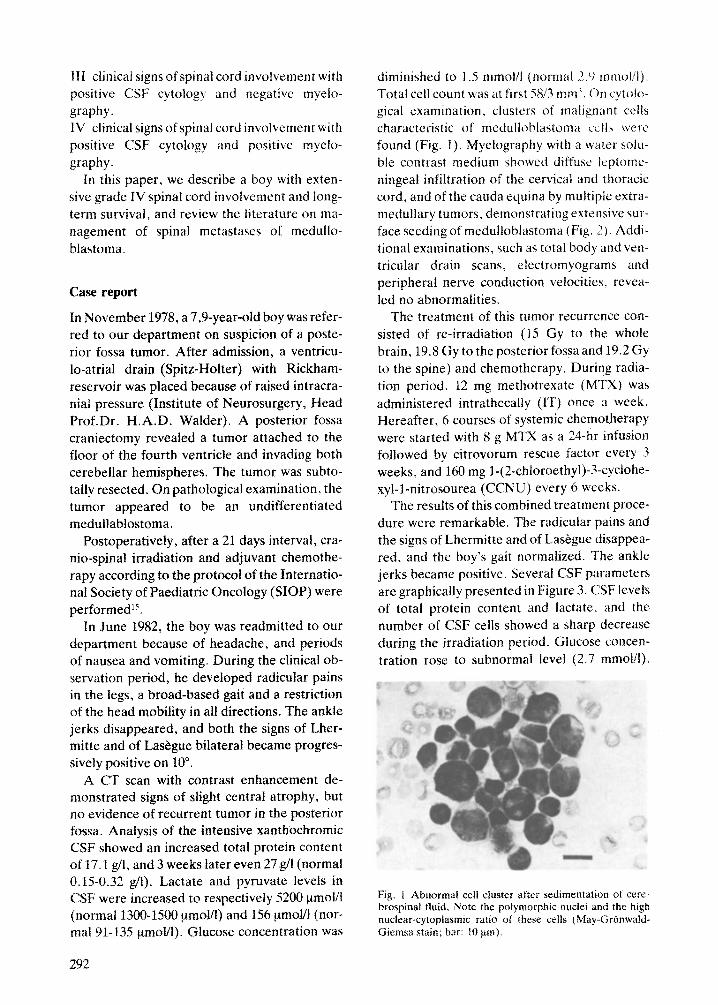
diminished to 1.5 mmolll tnormal 2.9 mmoiil j. Total cell count was at first 5X/3 mm’. T)n s$olo- gical examination, clusters of malignant cells characteristic of medullohlastoma tells were’ found (Fig. I). Mye~ograph!/ with a water solu- ble contrast medium showed diffuse leptome- ningeai infiltration of the cervical and thoracic cord, and of the cauda equina by muhipie extra- medullary tumors, demonstrating extensive sur- face seeding of medulloblastoma (Fig. ‘7). Addi- tional examinations, such as total body and ven-
tricular drain scans. electromyograms and peripheral nerve conduction velocities, revea- led no abnormalities.
The treatment of this tumor recurrence con- sisted of re-irradiation (15 Gy to the whole brain, 19.8 Gy to the posterior fossa and 19.2 Gy to the spine) and chemotherapy. During radia- tion period, 12 mg methotrexate (MTX) was administered intrathecaliy (IT) once a week. Hereafter. 6 courses of systemic chemotherapy were started with 8 g MTX as a 24hr infusion followed by citrovorum rescue factor every 3 weeks, and 160 mg I-(2”chloroethyl)-3-cyclohe- xyl-1-nitrosourea (CCNU) every 6 weeks.
The results of this combined treatment proce- dure were remarkable. The radicutar pains and the signs of Lhermitte and of LasBgue disappea- red, and the boy’s gait normalized. The ankle jerks became positive. Several CSF parameters are graphically presented in Figure 3. CSF levels of total protein content and lactate. and the number of CSF cells showed a sharp decrease during the irradiation period. Glucose concen- tration rose to subnormal level (2.7 mmolil).
Fig. 1 Abnormal cell cluster after sedimentation ot axe-
hrospinal fluid. Note the polymorphic nuclei and the high nuclear-c~toplasmic ratio of these cells ~Ma~-(;r~nwald~ Giemsa stain; bar: 10 pm).
292

Fig. 2 Diffuse leptomeningeal infiltration of the thoracic cord (left) and of the cauda equina (right)
Electromyography revealed a slight axonal neu-
ropathy of the lower extremities.
In May 1983, the boy was admitted for eva-
luation. Physical examination showed an identi-
cal picture. On computed tomography of the
head with contrast enhancement, no evidence of
posterior fossa recurrence could be found. At
myelography, the leptomeningeal tumor infil-
tration had disappeared, but there was a non-
filling with contrast medium of some lumbo-
sacral root sleeves. This latter phenomenon
might be attributable either to arachnitis secun-
dary to radiation, chemotherapy, the previous
myelography or due to tumor remnants (Fig. 4).
CSF total protein content and lactate were still
increased, and glucose was diminished (2.4
mmoV1). Peripheral nerve conduction velocities
were still normal. Electronmicroscopic appea-
rance of CSF cells suggested malignant abnor-
malities. On account of the CSF and myelogra-
phic findings, chemotherapy was continued
with 6 courses of 10 mg MTX IT and 160 mg
CCNU every 6 weeks.
Till the moment of finishing this paper (april
1985), the boy’s neurological examination re-
mains normal, except the absence of ankle jerks
and some periods of vomiting. CSF levels of
total protein content and lactate still remain
increased.
Endocrinologic examination reveals a growth
retardation (3.5 cm/2 years). The levels of
growth hormone were less than 1 VU/ml. The
concentration of thyroxine in plasma was bor-
derline low (66 clg/lOO ml). Secundary sex cha-
293

CSF PARAMETERS
I I Celli (/3mm3) (______)
160 t 1 :: I ,
1
Protein
;m9/1;
8 gr MTX 21 h infusion _ every six weeks.
1EOmg CCNU every three weeks.
tOmg MTX IT = every four weeks.
l6Omg CCNU every six weeks.
: : I= 12mg MTX If
5000- 100-
:
3000- 60- i
2000- 40-
lOOO- 20-
. <.
RT= 15 Gy whole brain 19.8 Gy posterior fossa 19.2 Gy spine
Fig. 3 CSF total protein content, total cell count and lactate level showed a sharp decrease after introduction of radio- and chemotherapy. On account of CSF and myelographic findings another course of chemotherapy was started in july 1983.
racteristics have not been developed till now (age 13,5 years).
The results of intelligence quotient testing using the Wechsler Intelligence Scale for Child- ren (WISC). declined mildly over the past 6 years. Besides, the boy exhibits serious emotio- nal and personality disturbances.
Discussion
The numerous reports on treatment of recurrent medulloblastoma do not offer a consistent the- rapeutic regimen. Moreover, the number of pa- tients in each study is too small to make statisti- cal analysis possible. The mean survival in spinal cord involvement after retreatment is estimated roughly to amount 12-13 months4JLJ3J6. In the majority of the patients the picture of spinal metastases is obscured by a coexisting, or a later on developing, posterior fossa tumor recurrence’2.14.17.
We have gained satisfying results on retreat-
ment of a boy with an isoiated grade It sprn;,i cord involvement. The boy is neurologicall~
well without evidence of recurrent disease JO months after retreatment.
Prompt reaction of the physician on the non- specific symptoms headache. nausea and vomi-
ting has probable contributed to the early detec. tion of the spinal metastases. Gross dccompen- sation of the spinal nervous system could consequently be prevented.
In our department a conscientious follow-up scheme after treatment of primary and metasta- tic medulloblastoma has been adopted. Twice a year neuroIogica1 status, investigation of CSF and CT myelography are carried out. CSF levels of total protein, lactate, pyruvate and glucose, and CSF cytologic findings together with mor- phology from CT myelography appear to be im-
portant criteria in documentating the course of spinai cord involvement”,‘“. We propose to carry out a CT myelography for .judgement of the morphological status of the spinal cord and arachnoid space. Particularly the usefulness of total conventional myelography and determina- tions of CSF polyamines have been mentioned by some authors”. CT myelography, as propo- sed, is to be carried out in a very restricted way by using 4-7 ml of a water soluble contrast me- dium and imaging on previous diseased levels and on predetermined lumbar, thoracic, cervi- cal and cisternal levels’“. The determination of polyamines is not yet possible in our department _
The additional value of CSF determinations of total protein content, lactate, pyruvate and glucose is of importance in the follow-up and demonstrates the efficacy of the treatment pro- cedure. Total protein content often shows an increase on spinal cord tumors. An increase of lactate and pyruvate concentrations, in accor- dance with a diminution of glucose concentra- tion, may also occur in brain tumorsLS. HOW- ever, multipleintrathecal injectionsof MTX and radiotherapy may bring about a rise of total protein content and cell countzc’.
As for primary medulloblastoma, treatment of spinal metastases consists of surgery, irradia- tion and (poly)chemotherapy, as single moda- lity or in combinationy,‘~.~~. For solitary spinal lesions decompressive iaminectomy can supply some palliation. However. irradiation is the
294
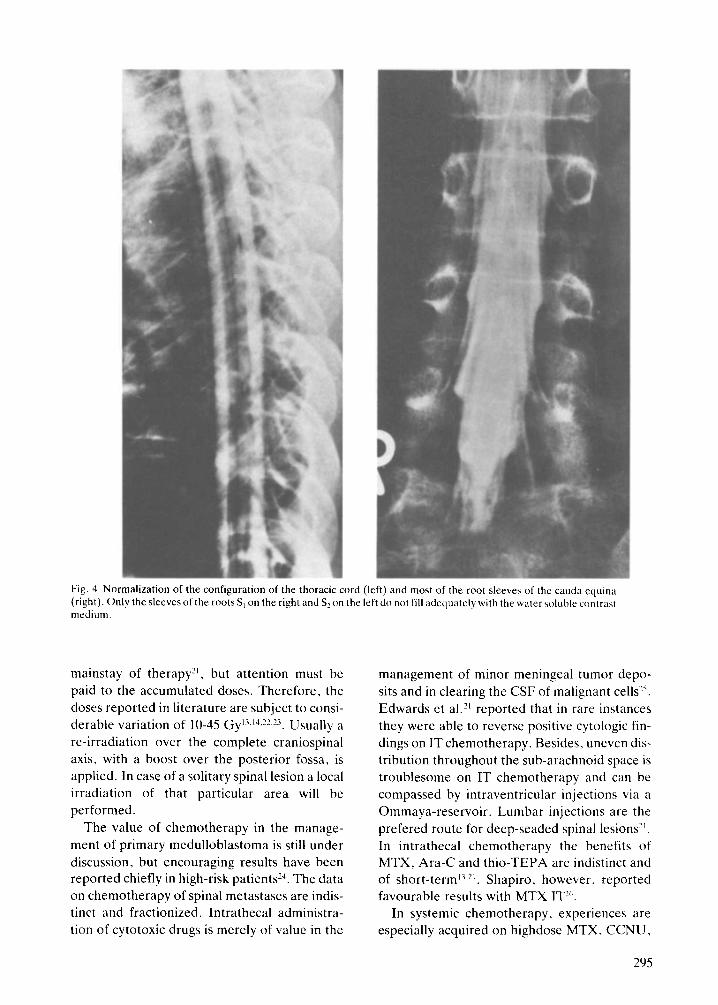
Fig. 4 Normalization of the configuration of the thoracic cord (left) and most of the root sleeves of the cauda cquina
(right). Only the sleeves of the roots S, on the right and S? on the left do not fill adequately with the watersoluhle contrast
medium.
mainstay of therapy?‘, but attention must be
paid to the accumulated doses. Therefore, the
doses reported in literature are subject to consi-
derable variation of 10-45 Gy’“~‘Q?~‘“. Usually a
re-irradiation over the complete craniospinal
axis, with a boost over the posterior fossa, is
applied. In case of a solitary spinal lesion a local
irradiation of that particular area will be
performed.
The value of chemotherapy in the manage-
ment of primary medulloblastoma is still under
discussion, but encouraging results have been
reported chiefly in high-risk patients14. The data
on chemotherapy of spinal metastases are indis-
tinct and fractionized. lntrathecal administra-
tion of cytotoxic drugs is merely of value in the
management of minor meningeal tumor depo-
sits and in clearing the CSF of malignant cells’.
Edwards et al.” reported that in rare instances
they were able to reverse positive cytologic fin-
dings on IT chemotherapy. Besides. uneven dis-
tribution throughout the sub-arachnoid space is
troublesome on IT chemotherapy and can be
compassed by intraventricular injections via a
Ommaya-reservoir. Lumbar injections are the
prefered route for deep-seaded spinal lesions”.
In intrathecal chemotherapy the benefits of
MTX, Ara-C and thio-TEPA are indistinct and
of short-termii,Z’. Shapiro. however, reported
favourable results with MTX IT”‘.
In systemic chemotherapy, experiences are
especially acquired on highdose MTX. CCNU,
295

procarbazine and vincristine. Systemic adminis- tration of cytotoxic drugs by intravenous infu- sions is limited by the blood-brain barrier sys- tem. To obtain an effective CSF concentration of a drug, systematically given, a high dosage scheduie of the infusions is required over a suffi- ciently long period of time. This method can achieve a minor improvement on spinal cord involvement onlyZ3. Positive cytologic findings or increased CSF polyamines could not be re- versed by Levin et al. Ii. Whereas Mooney et al.” reported no response to high-dose MTX, Rosen et a12# noticed encouraging results. Res- ponses have been reported on the use of CCNU, procarbazine and v~ncristine, as single drug or in combination10.‘?.i”.2”,?Y, although the combina-
tion of procarbazine and CCNU may cause bone marrow toxicity, especially following cra- niospinal irradiation’“.
In the retreatment of spinal medulIoblas- toma, radiotherapy remains the most important therapeutic modality. The value of adjuvant chemotherapy is controversial, although we have gained satisfying results in the treatment of a boy with an extensive grade IV spinal cord involvement. The additional radiotherapy ( 15 Gy to the whole brain, 19.8 Gy to the posterior fossa and 19.2 Cy to the spine) and chemothe- rapy (MTX IT, high-dose MTX, CCNU) were well tolerated.
References
RUBINSTEIN IJ. The cerebellar medulloblastoma: its ori- gin, differentiations morphologjcai variants, and biolo- gicaf behavior. In: Vinken PJ, Bruyn GW, eds. Hand- book of clinical neurology, Vol 18. Amsterdam: North- Holland Publishing Co, 1975; 167-72. ARSENI c, CIIJREA AV. Statistical survey of 276 cases of medulloblastoma (193% 1978). Acta Neurochir (Wien) 1981: 57:159-62. WILLIS RA. The spread of tumors in the human body. London: Butterworth & Co, 1973; 259-60. MCFARLAND DR,HORWITZ A,SAENGER EL, BAHRGK. Me- dulloblastoma: a review of prognosis and survival. Br J Radio1 1969; 42: 198-214. RUSSELL D.S. RUBINSTEIN II. Pathology of tumors of the nervous system. London: Edward Arnold. 1973; 340. MARToN LJ,~DWARDS~s,LEVINV~,LUBICHWP,WlLSONCB.
CSF polyamines: a new and important means of monito- ring patiens with medulloblastoma. Cancer 1981: 41:757-60. DEUTSCH M, REIGEL DH. Myelography and cytology in the treatment of medulloblastoma. Int J Radiat Oncol Biol Phys 1981; ?:721-5. noRwART RH,WAREWM,NORMAND,LEV~N VA. Complete myetographic evaluation of spinal metastases from me- duIloblastoma. Radiology 1981; 139:403-X.
MAZZA C, PASGUALIN A, DA PIAN R, iJ0NAIi I I Ic'illrllcI1I
oE medulloblastoma in children: long-term result\ following surgery. radiotherapy and chemotherap!- Acta Neurochir (Wien) 198 I ; 57: 163-75. BERRY MI', JENKIN RDT, KEEN CW, NAIR BD. SIMPSo& \\J.
Radiation treatment for medulloblastom;i i\ 2 i-your review. J Neurosurg 1981: SS:43-51. GEKOSA MA. UI STEFANO E,ol.lVl A, CARTERI A. Multidisci- plinary treatment of medulloblastoma: a 5-year expc- rience with the SIOP-trial. Childs Brain 1% 1; 8: 107- 18. I.EVINVA,VESTNYSPS,EDWARDSMS,liIhL. ~IITpToVurPXtt
in survival produced by sequential therapies in the treat- ment of recurrent medulloblastoma. Cancer 1YX3: 51: 1364-70. SIVERMAN CL, SIMPSON JR. Cerebellar medaltoblastoma: the importance of posterior fossa dose to survival and patterns of failure. Int J Radiat Oncol Biof Phys 19X2; 8: 1869-76. NEIDHAKDT MK. Die Behandlung des Medultoblastoms aus ptidiatrisch-onkologischer Sicht. Strahlentherapic 1982; 158:76-81. PARK TS,HOFFMANHJ, HENDRICK ~B.Ii~MPIfR~YS RP,BEC-
KER LE. Medulloblaston~: clinical presentation and ma- nagement. Experience at the Hospital for Sick Children, Toronto, 1950-1980. J Neurosurg 1983; 58:543-52. SMITH CE, LONG DM, JONES TIC. LEVITT SW. Medulloblas- toma: an analysis of time-dose relationships and recur- rent patterns. Cancer 1973; 32:722-t% SAYK J. The cerebrospinal fluid in brain. In: Vinken PJ, Bruyn GW, eds. Handbook of clinical neurology, Vol 16. Amsterdam: North-Holland Publishing Co, 1974; 370-71. 392. PETTERSON H,NARWOOD-NASH DCF.~T andmyelog~~pby of the spine and cord. Berlin: Springer Verlag, 1982. LIPPENS RJJ. Methotrexate in the central nervous system prophylaxis of children with acute lymphobfastie Ieuke- mia. Thesis. Catholic University Nijmegen. i981. EDWARDS MS, LEVIN VA,SEAGLR ML. MILTON CB. fntrathe- cal chemotherapy for leptomeningeal dissemination of medullohlastoma. Childs Brain IYNI: X:444-51. C~So170 A, RUONCRISTIANI p. M~dull(~l~lastoma in child- hood. Multidisciplinary treatment. <‘hiIds Brain 1982: 9:299-X)8. BAMBERG M, SCHMITTI;, yu~sr Lg. ETAI.. ‘I’herapie und Prognose des MeduIlobiast~)ms. Forschritte durch neuenartige Bestrahlungste~hniken. St~hlenth~rap;~ 1980; 156: l-17. BLOOM IiJo. Intracranial tumors: response and resistance to therapeuticendeavors. 1970-1980. Int J Radiat Oncol Biol Phys 1982; 8: 1083-I 13. BLOOM HJG. Combined modality therapy for jnt~cranial tumors. Cancer 197.5; 35: 1 I l-20. SHAPIRO WR. Chemotherapy of l?rimary malignant brain tumors in children. Cancer 1975; X:965-72. MOUNEY c, S~UHAMI R. PR~~CIIAR~ J. Recurrentmed~ilo- blastoma. Lack of response to high-dose methotrexate. Cancer Chemother Pharmacol 1983; 10:135-h. ROSENG,CHAVlMIF,NIRENBERGA,MOSENDEc,MEHTABM.
High-dose methotrexate with citrovorum factor rescue for the treatment of CNS tumors in children. Cancer Treat Rep 1977; 61:f&-90. BLOOM HJG. Medulloblastoma: prognosis and prospects. Int J Radist Oncol Biol Phys 1977; 2: 1031-i.
296
![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://img.dokumen.tips/doc/110x75/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)












![Medulloblastoma: [Print] - eMedicine Neurology · accounts for approximately 7-8% of all intracranial tumors and 30% of ... Incidence of medulloblastoma is 1.5-2 cases per ... Medulloblastoma:](https://img.dokumen.tips/doc/110x75/5b7fc2317f8b9ae6088caa0e/medulloblastoma-print-emedicine-accounts-for-approximately-7-8-of-all.jpg)















