Embed Size (px)
Citation preview

C H A P T E R
15
Osteocalcin, Undercarboxylated Osteocalcin,and Glycemic Control in Human Subjects
Itamar Levinger 1, Jeffrey D. Zajac 2, Ego Seeman 2
1Victoria University, Melbourne, Australia 2University of Melbourne, Melbourne, Australia
OBESITY, DIABETES, AND LOW SERUMOSTEOCALCIN: CROSS-SECTIONALSTUDIES IN HUMAN SUBJECTS
Osteocalcin is an osteoblast-specific product that issecreted into the bone extracellular matrix and thegeneral circulation. Osteocalcin is carboxylated in theosteoblasts on three glutamic acid residues and can bedecarboxylated in resorption lacunae to becomea hormone that reaches the general circulation where itcan fulfill its endocrine functions. Studies in mice haveshown that uncarboxylated osteocalcin (ucOC) increasesinsulin secretion and sensitivity. Although there are nostudies examining whether there is a direct effect ofucOC on energy metabolism in human subjects, correla-tions between circulating osteocalcin (OC) and ucOCand measures of insulin sensitivity and glycemic controlhave been reported in several cross-sectional studies.The observations support the notion that products ofthe osteoblast, one of them being osteocalcin, modifyinsulin sensitivity, insulin secretion, and glycemiccontrol in humans.
OC-deficient mice are obese and have glucose intoler-ance [1e3]. Accordingly, several groups of investigatorshave provided consistent evidence that obese subjectsand patients with type 2 diabetes mellitus (T2DM)have lower circulating levels of OC and ucOC. Forexample, Foresta et al. [4] reported that overweightand obese individuals have a lower ucOC and ucOC/OC ratio. Kindblom et al. [5] reported that 153 diabeticelderly men (mean age 75.3) with T2DM had 21.7%lower circulating OC than 857 men without T2DM. Imet al. [6] reported 30% lower circulating OC levels inpostmenopausal women with T2DM compared to post-menopausal non-diabetic women. Likewise, Oz et al.reported men and women in their 50s with diabetes(n¼ 15 and n¼ 37, respectively) had lower OC level
181Translational Endocrinology of Bone
DOI: http://dx.doi.org/10.1016/B978-0-12-415784-2.00015-4
(~42% and ~50%, respectively) than those without dia-betes (n¼ 14 and n¼ 34, respectively). Furthermore,Levinger et al. [7] reported that men with T2DM had38% lower circulating levels of ucOC compared tonon-diabetic men. Thus, patients with T2DM have lowercirculating levels of OC and ucOC compared to individ-uals without T2DM. The question is whether there isa causal relationship between the lower OC and unOCand diabetes. This is a difficult question to address inhumans.
Kindblom et al. [5] reported that circulating OC isinversely related to body mass index (BMI), fat mass,and plasma glucose (p< 0.001). Circulating OCexplained 6.3% of the variance in plasma glucose.Multiple linear regression models adjusted for seruminsulin and fat mass suggested that plasma OC was anindependent negative predictor of plasma glucose [5].Similarly, Im et al. [6] reported that postmenopausalwomen with OC in the highest quartile had a lower fast-ing glucose and hemoglobin A1c (HbA1c) levels thanpostmenopausal women with OC in the lowest quartile.OC was also negatively correlated with glucose, insulin,HbA1c, and insulin resistance.
Hwang et al. [8] reported that a higher serum ucOCwas associated with improved glucose tolerance in199 men aged 25e60 years (mean age, 47 years) andthat the improved glucose tolerance may be related toenhanced b-cell function. More recently, the same groupreported that circulating OC levels are lower in patientswith T2DM compared to non-diabetics and that there isa correlation between OC and improved glucosetolerance, insulin sensitivity, and insulin secretion in425 men and women aged 19e82 years (mean age,53 years) [9]. Importantly, they reported that in humans,in contrast to animals, the increase in glucose tolerance,insulin sensitivity, and insulin secretion with increasedlevels of OC is independent of adiponectin levels [9].
� 2013 Elsevier Inc. All rights reserved.

15. OSTEOCALCIN, UNDERCARBOXYLATED OSTEOCALCIN, AND GLYCEMIC CONTROL IN HUMAN SUBJECTS182
Kanazawa et al. [10] reported that ucOC was negativelycorrelated with percent body fat, fasting glucose, andHbA1c in 180 men with T2DM. The same group [11]examined the correlation between OC and metabolicand cardiovascular risk factors in 179 men and 149 post-menopausal women with T2DM. After adjustment forage, BMI, and serum creatinine, OC was negativelycorrelated with glucose and HbA1c in men and women.In men, OC correlated with brachialeankle pulse wavevelocity and intima-media thickness after adjustmentfor systolic blood pressure, LDL cholesterol, HDLcholesterol, HbA1c, and the Brinkmann index. Othershave also reported that OC is negatively correlatedwith premature myocardial infarction [12].
These data indicate that higher circulating OC anducOC correlate with greater insulin sensitivityand lower circulating glucose levels. Higher BMI andpercent body fat correlate with lower OC and ucOClevels. Bullo et al. [13] reported that OC and ucOC corre-lated with higher fasting insulin concentrations afteradjustment for covariates. However, the correlationwas observed only in individuals not taking oral antidi-abetic drugs. Yeap et al. [14] reported that OC wasnegatively correlated with waist circumference, glucose,and triglyceride levels and insulin resistance. Men withmetabolic syndrome had lower OC levels, elevatedglucose, and triglyceride levels. Similarly, Saleem et al.[15] reported that OC levels were inversely correlatedwith BMI, fasting glucose, and insulin resistance andpositively correlated with adiponectin after adjustmentfor age and sex. Thus, these cross-sectional studiessuggest that elevated levels of OC and ucOC are associ-ated with lower body fat and better glycemic control.Due to the cross-sectional nature of the studies causalitycannot be determined.
OSTEOCALCIN AND GLYCEMICCONTROL: INTERVENTIONAL STUDIES
To date, there is no study demonstrating ucOC (orOC) administration in humans regulates either insulinaction or insulin secretion. We therefore examine thequestion of whether indirect interventions known toaffect glycemic control also affect OC and ucOC levels.Kazanawa et al. [16] examined the effects of improvedglycemic control usingmetformin, insulin, and sulfonyl-urea in 50 patients with poorly controlled T2DM. HbA1cdecreased from 10 to 8.8%. Serum OC increased by1.94 ng/ml (p¼ 0.004). UcOC also increased, but notsignificantly. The change in circulating OC, not ucOC,correlated with the change of HbA1c (r¼�0.3,p¼ 0.03). Similarly, Sayinalp et al. [17] examined theeffects of glycemic control in 27 men with poorlycontrolled T2DM (HbA1c >9%, fasting plasma glucose
>7.8 mmol/L). Improved glycemic control was accom-panied by increased circulating OC and OC correlatednegatively with HbA1c. Similarly, 8-week treatmentwith hypoglycemia agents in 59 patients with T2DMresulted in increased OC levels and reduced glucosevariability [18]. Thus, changes in OC are related tochanges in glycemic control and higher levels of OCare associated with improvements in serum glucose.However, the results of the above studies are difficultto interpret because of the use of insulin, metformin,sulfonylurea, and a-glucosidase inhibitor, medicationsthat may affect OC and ucOC [7,10,11,16,19].
Bullo et al. [13] has examined whether the changes inOC and ucOC over 2 years were associated with insulinsecretion and sensitivity in community-dwelling menaged 55e80 years. Increase in OC was associated withan increase in insulin secretion (b coefficient: 2.87; 95%CI: 0.23, 5.52; p¼ 0.033), and changes in ucOCwere asso-ciated with an improvement in insulin resistance(HOMA-IR, b coefficient: 20.31; 95% CI: 20.60, 0.03;p¼ 0.032). Similarly, Pittas et al. [20] reported thatin 380 older adults (mean age¼ 71 years, BMI¼26.9 kg/m2, 5% with diabetes) OC was associated withbaseline fasting plasma glucose, fasting insulin, insulinsensitivity, plasma high-sensitivity C-reactive protein,IL-6, and BMI and body fat. Furthermore, those in thehighest tertiles of serum OC had lower fasting glucosethan those in the lowest OC tertile (p< 0.01). Thosewith higher serum OC during follow-up had fewer risesin fasting plasma glucose after 3 years.
Shea et al. [21] also examined the correlation betweenOC and ucOC with insulin resistance at baseline(n¼ 348) and after 3 years (n¼ 162) in non-diabeticmen and women (mean age 68 years). In contrast, theyreported that lower circulating ucOC was not associatedwith higher insulin resistance. However, those in thelowest tertile of total OC and carboxylated OC at base-line had higher insulin resistance at baseline. The authorconcluded that in older adults, total OC and carboxyl-ated OC, but not ucOC, were associated with lowerinsulin resistance.
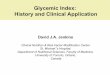
Exercise (muscle contraction) is known to improveinsulin sensitivity and glycemic control. Fernandez-Real et al. [22] examined the relationship between OC,insulin sensitivity, and secretion in a cross-sectionalstudy of 149 men (mean age¼ 50.2 years). They reporteda linear relationship between circulating OC and insulinsensitivity and insulin secretion (Fig. 15.1). This correla-tion was more evident in lean men than those who wereoverweight. In the intervention studies, diet only led toa mean weight loss of 7.3% with modest increase incirculating OC. In the diet plus physical activity group,mean weight loss was 8.7%, but circulating OCincreased. The increase in OC level was related to thereduction in visceral fat mass and increase in lean

FIGURE 15.1 Linear relationship between circulating osteocalcin and insulin sensitivity in 149 men of the cross-sectional study (single lineand correlation coefficient) and in lean men (95% confidence interval) for the mean and correlation coefficient in the upper left. Adapted from
Fernandez-Real et al. [22].
INTERVENTIONAL STUDIES MANIPULATING VITAMIN K LEVELS 183
mass and muscle strength. In addition, the OC level atthe end of the activity intervention was related toincreased insulin sensitivity (r¼ 0.49; p¼ 0.03) andnegatively correlated with fasting triglycerides(r¼�0.54; p¼ 0.01). The authors concluded that OCmay participate in regulating insulin sensitivity inhuman subjects as it does in mice. Such a conservationof functions is expected since, to the best of our knowl-edge, no molecule identified as a hormone in rodentshas been shown to have lost this function in humans.
Levinger et al. [7] examined whether the reduction inserum glucose level after acute aerobic and power exer-cise is related to change in ucOC in 28 middle-aged menwith and without T2DM (mean age¼ 52.4 and meanBMI¼ 32.1 kg $m�2). At baseline, ucOC correlatednegatively with glucose levels (r¼�0.53, p¼ 0.003)and HbA1c (r¼�0.37, p¼ 0.035). Both aerobic andpower exercise increased OC and ucOC and reducedserum glucose levels. In patients with T2DM, thepercentage change in OC and ucOC levels correlatedwith the percentage change in glucose levels post-exercise (r¼�0.51, p¼ 0.038). The change in OC anducOC levels from pre- to post-exercise were predictorsfor the change in glucose levels post-exercise, with slightsuperiority of ucOC.
Thus, these two studies suggest that exercise has aneffect on circulating levels of OC and ucOC and thatthere is a correlation between the change in OC anducOC and the improvements in glycemic control. More-over, improvements in insulin sensitivity and glycemic
control with exercise may, at least in part, be mediatedby OC and ucOC. How exercise influences OC anducOC is not known and warrants further investigation.
INTERVENTIONAL STUDIESMANIPULATING VITAMIN K LEVELS
Another possible intervention is to alter circulatinglevels of ucOC by administration or deprivation ofvitamin K and examine whether the increase or decreasein circulating levels of ucOC has an effect on glycemiccontrol. Vitamin K is found in green leafy vegetablesand is required for OC carboxylation [23]. VitaminK supplementation increases carboxylation and lowerscirculating ucOC [24] and, as such, vitamin K supple-mentation should increase insulin resistance and serumglucose levels. Kumar et al. [25] reported that 12 monthsof vitamin K1 (phylloquinone) administration in post-menopausal women reduced ucOC by ~200% but therewas no increase in insulin resistance. However, thisstudy examined ucOC and glycemic control at rest, notafter a meal or after glucose loading which may affectthe results. Kumar et al. [25] suggested that the differingfindings from studies in mice may be related to the dele-tion of OC genes in mice which led to abnormal ucOClevel during development, whereas in humans thereduction in ucOC levels was induced later in life. Assuch, it may not have similar effects on insulin resis-tance. In addition, increases in hepatic insulin clearance

15. OSTEOCALCIN, UNDERCARBOXYLATED OSTEOCALCIN, AND GLYCEMIC CONTROL IN HUMAN SUBJECTS184
may have masked the increase in insulin production bythe pancreatic b cells, but there was no evidence tosupport this hypothesis. Nevertheless, these findingsare inconsistent with the findings in mice and in somecross-sectional and interventional studies in humans.
Low circulating vitamin K should be associated withbetter glycemic control. However, in one study [26], menwith low vitamin K intake had lower insulin responseand higher plasma glucose 30min after glucose loading.This and the findings from Kumar et al. do not supportthe hypothesis that ucOC is essential for glycemiccontrol in humans. If OC also plays a role in insulinsecretion and sensitivity in human subjects, it mayexplain why insulin resistance does not increase in theKumar et al. [25] study. Further studies are needed toclarify the connection between vitamin K supplementa-tion and deficiency, OC, ucOC, and glycemic control inhumans.
WHAT IS THE ACTIVE FORM OFOSTEOCALCIN IN HUMANS?
In mice, ucOC, but not OC, participates in energymetabolism [1]. In the studies described above bothOC and ucOC appear to be associated with increasesin insulin sensitivity and glycemic control in humans.The active form of OC in humans is unknown, mostlikely because there are methodological limitationssuch as absence of specific commercially availableassays used to detect ucOC. There are two mainmethods to analyze ucOC in humans, immunoassayafter absorption of carboxylated OC on a hydroxyl-apatite column following the method described byGundberg et al. [27] and electrochemiluminescenceimmunoassay (ELISA). The hydroxyl-apatite column isconsidered as the gold standard and it analyzes totalOC, carboxylated OC, and ucOC in one analysis whichenables assessment of the ucOC/OC ratio. This methodis expensive. The electrochemiluminescence immuno-assay is accurate between 0.39 and 50 ng/mL, coveringthe clinically important range. Assessment of reproduc-ibility testing showed inter-assay CV¼ 1.5e5.9%. Theelectrochemiluminescence immunoassay for ucOC wasvalidated against the hydroxyapatite binding assay[28]. The main limitations of the electrochemilumines-cence immunoassay are that it is specific for ucOC andas such OC must be analyzed with a different assay sothe ucOC/OC ratio cannot be determined. Importantly,the ELISA may overestimate ucOC levels as the anti-body used may be attached to N-terminal fragments ofOC [27]. To date, many studies have used the electroche-miluminescence immunoassay as it is more convenientand easier to perform compared to the hydroxyl-apatitebinding method. Thus, development of valid, reliable,
and easy to use ELISA is needed to further explore thecontribution of ucOC to energy metabolism. At thistime it is difficult to determine which OC form is directlyinvolved in increasing insulin sensitivity and glycemiccontrol in humans, although it seems unlikely that thebiology of osteocalcin would differ that much betweenmice and humans.
ENDOSTEAL SURFACE AREA,REMODELING, AND GLYCEMIC
CONTROL
The cellular machinery of bone modeling and remod-eling is the final common pathway mediating the effectsof all genetic and environmental factors on the materialcomposition and structure of bone and therefore bonestrength [29]. Bone modeling may be formative orresorptive (not only formative) and is both the maincellular mechanism responsible for the change in bonesize, shape, and architecture during growth in humansubjects and the main mechanism responsible forgrowth and renewal of bone in rodent speciesthroughout life. Modeling by bone formation (withoutprior resorption) or resorption (not followed by forma-tion) occurs at different locations. Bone remodeling isresponsible for renewal of osteonal bone in humansubjects. Remodeling involves the resorption thendeposition of a volume of bone matrix at the samelocation by teams of cells forming the basic multicellularunit (BMU).
Remodeling modifies the structure of bone by addingand removing bone upon the outer (periosteal) envelopeand each of the three (intracortical, endocortical, andtrabecular) contiguous components of its inner (endos-teal) envelope. The mineralized bone matrix is thatmaterial “within” the periosteal envelope or surfaceand “outside” the three components of the inner enve-lope (Fig. 15.2).
OC is a bone formation marker and reflects, in part,the surface extent of bone remodeling. As bonemodeling and remodeling throughout life are surface-dependent processes [30], we examined whether thestructural configuration of bone, specifically its surfaceto volume ratio, is related to remodeling and to regula-tion of OC and ucOC and therefore regulation of bloodglucose levels. Remodeling of bone matrix requires thesurface to be initiated upon [31,32]. If signals arisefrom the osteoblasts of the bone remodeling unit, thegreater the remodeling intensity, the greater the numberof osteoblast cells. Bone matrix volume assembled withmore surface is assembled with less mass and facilitatesthe need to maintain itself with fewer energy require-ments while assembling a mechanically sound architec-ture. As such, it appears that during evolution the

(A) (B)
FIGURE 15.2 Structure of bone. (A) Cortical and trabecular bone, the periosteal (external) surface and the three (endocortical, trabecular,intracortical) contiguous components of the endosteal (internal) surface upon which matrix remodeling is initiated. (B) The intracortical surfaceformed by the lining of Haversian and Volkmann canals traverses the cortex. These canals are seen as pores in cross-section. Reconstructed withhigh-resolution quantitative CT. Please see color plate section. Adapted from Zebaze et al. [31].
ENDOSTEAL SURFACE AREA, REMODELING, AND GLYCEMIC CONTROL 185
skeleton has adapted to be strong and light, which mayassist the body to conserve energy. On the other hand,the skeleton requires a constant supply of energy formodeling to allow growth and therefore ambulationand survival in the face of danger, and remodeling inorder to prevent fractures (which in ancient timesreduced the chance of survival) [33].
Bjornerem et al. [34] has examined the intracortical,endocortical, and trabecular bone surface area of thedistal tibia and distal radius in 185 healthy femaletwin pairs aged 40 to 61 years using high-resolutionperipheral quantitative computed tomography(HR-pQCT). They also examined the correlationbetween bone surface and markers of remodeling.They reported that intracortical surface area andintracortical porosity (surrogate of surface area) arecorrelated with remodeling markers such as OC, cross-linking telopeptides of type I bone collagen (CTX), andprocollagen type 1 aminoterminal propeptide (P1NP)in both distal radius and distal tibia, while trabecularsurface area was negatively correlated with thosemarkers (Fig. 15.3). The authors concluded thatthe configuration of bonedand especially larger
intracortical and endocortical surface areadis likely tocontribute to the intensity of remodeling; the larger thesurface, the greater the accessibility of the bone matrixvolume to being remodeled. However, the relationshipbetween those bone surfaces and glycemic control wasnot studied.
No study has examined the connection between theintracortical, endocortical, and trabecular bone surfaceand glycemic control. It is accepted that patients withtype 1 diabetes mellitus (T1DM) are characterized bylower BMD [35] and patients with T2DM have normalto high BMD [36] but the connection to surface area isunknown. Preliminary data from our research group(unpublished) suggests that in middle-aged men,porosity of the compact-appearing cortex of the tibiaand radius, the transitional zone, and the fraction ofthe medullary cavity correlate with serum OC anducOC (r ranging from 0.33 to 0.72, p< 0.05) [37]. Conse-quently, total, cortical, and trabecular vBMD correlatednegatively with serum ucOC. Furthermore, circulatingucOC correlated negatively with serum glucose andHbA1c in this cohort. However, no detectable correla-tions where found between porosity of the compact-

FIGURE 15.3 Bone remodeling markers osteocalcin and b-carboxyterminal cross-linking telopeptides of type I bone collagen (b-CTX)correlated directly with tibia intracortical and endocortical surface area/cortical tissue volume (TV) but inversely with trabecular surface area/trabecular TV. Adapted from Bjornerem et al. [34].
15. OSTEOCALCIN, UNDERCARBOXYLATED OSTEOCALCIN, AND GLYCEMIC CONTROL IN HUMAN SUBJECTS186
appearing cortex of the tibia and radius, the transitionalzone and the fraction of the medullary cavity and serumglucose or HbA1c. As such the preliminary data suggestthat a larger bone surface area facilitates remodeling andmay, indirectly, be related to glycemic control inhumans. Nevertheless, future studies with a large cohortshould be performed in order to investigate the contri-bution of bone surface area to glycemic control inhumans. It is still not clear whether the intracortical,endocortical, and trabecular bone surface are directlyrelated to insulin sensitivity and glycemic control but,if so, this provides opportunities for designing newpharmacological and non-pharmacological interven-tions to treat both bone diseases and T2DM. Furtherwork is under way exploring these relationships.
OSTEOCALCIN AND GLYCEMICCONTROL: CONCLUSIONS AND
CLINICAL IMPLICATIONS
Animal models have shown that ucOC participates inenergy metabolism. There is growing evidence inhuman subjects to support the hypothesis that higherlevels of circulating ucOC are related to better glycemiccontrol [33]. Daily injections of recombinant OC at 3 or30 ng/g/day reduce blood glucose levels and improveglucose tolerance and insulin sensitivity in mice fed
a normal diet [38]. The improvement in blood glucoselevels, glucose tolerance, and insulin sensitivity wasrelated to the increase in b-cell mass and insulin secre-tion. Furthermore, daily injections of recombinant OCpartially restored insulin sensitivity and glucose toler-ance in mice fed a high-fat diet. Other benefits reportedincluded higher number of skeletal muscle’s mitochon-dria, increased energy expenditure, and protectionfrom diet-induced obesity [38]. The authors concludedthat daily injections of recombinant OC improve glyce-mic control as well as prevent the development ofT2DM.
Whether ucOC plays a role in insulin secretion andsensitivity in humans and whether daily injection ofucOC treatment restores glycemic control in humansare unknown. If ucOC plays a role in glucose metabo-lism in humans it will provide avenues for designingnew drugs that imitate these pathways for obese personsand patients with T2DM. Clearly, drugs which increaseboth insulin secretion and insulin sensitivity withoutweight gain would in many ways be the ideal agentsfor treating diabetes. Furthermore, targeting bonemetabolism as a pathway to control whole body glucosehomeostasis will be important as current therapies arelimited in their specificity and effectiveness and mayhave a negative effect on bone health. CirculatingucOC is associated with increased insulin sensitivityand glycemic control in humans. Whether this

REFERENCES 187
association is causal will require prospective studies.There are neither longitudinal studies nor mechanisticstudies to support the unOC hypothesis in humans.Themechanism bywhich ucOCmay affect insulin sensi-tivity and secretion and glycemic control in humans isstill largely unknown but it may resemble that in mice.If this regulatory mechanism of glucose metabolismoccurs to a significant degree in humans it could havemajor effects on improving the treatment of T2DM.Thus, the exciting data in mice identifying a regulatoryrole of ucOC have not yet been definitively replicatedin humans. However, preliminary reports suggest thatit is likely there will be a similar effect in humans. Themagnitude of this effect and whether it will be clinicallysignificant still remain to be defined.
Acknowledgments
Dr. Itamar Levinger is a Heart Foundation Postdoc-toral Research Fellow.
References
[1] Lee NK, Sowa H, Hinoi E, et al. Endocrine regulation of energymetabolism by the skeleton. Cell 2007;130:456e69.
[2] Clemens TL, Karsenty G. The osteoblast: an insulin target cellcontrolling glucose homeostasis. J Bone Miner Res 2011;26:677e80.
[3] Ferron M, Hinoi E, Karsenty G, Ducy P. Osteocalcin differen-tially regulates beta cell and adipocyte gene expression andaffects the development of metabolic diseases in wild-typemice. Proc Natl Acad Sci USA 2008;105:5266e70.
[4] Foresta C, Strapazzon G, De Toni L, et al. Evidence for osteo-calcin production by adipose tissue and its role in humanmetabolism. J Clin Endocrinol Metab 2010;95:3502e6.
[5] Kindblom JM, Ohlsson C, Ljunggren O, et al. Plasma osteo-calcin is inversely related to fat mass and plasma glucose inelderly Swedish men. J Bone Miner Res 2009;24:785e91.
[6] Im JA, Yu BP, Jeon JY, Kim SH. Relationship between osteocalcinand glucose metabolism in postmenopausal women. ClinicaChim Acta. Int J Clin Chem 2008;396:66e9.
[7] Levinger I, Zebaze R, Jerums G, Hare DL, Selig S, Seeman E.The effect of acute exercise on undercarboxylated osteocalcin inobese men. Osteoporos Int 2011;22:1621e6.
[8] Hwang YC, Jeong IK, Ahn KJ, Chung HY. The uncarboxylatedform of osteocalcin is associated with improved glucose toler-ance and enhanced beta-cell function in middle-aged malesubjects. Diabetes Metab Res Rev 2009;25:768e72.
[9] Hwang YC, Jeong IK, Ahn KJ, Chung HY. Circulating osteo-calcin level is associated with improved glucose tolerance,insulin secretion and sensitivity independent of the plasmaadiponectin level. Osteoporos Int 2012;23:1337e42.
[10] Kanazawa I, Yamaguchi T, Yamauchi M, et al. Serum under-carboxylated osteocalcin was inversely associated with plasmaglucose level and fat mass in type 2 diabetes mellitus. Osteo-poros Int 2011;22:187e94.
[11] Kanazawa I, Yamaguchi T, Yamamoto M, et al. Serum osteo-calcin level is associated with glucose metabolism and athero-sclerosis parameters in type 2 diabetes mellitus. J ClinEndocrinol Metab 2009;94:45e9.
[12] Goliasch G, Blessberger H, Azar D, et al. Markers of bonemetabolism in premature myocardial infarction (</¼ 40 yearsof age). Bone 2011;48:622e6.
[13] Bullo M, Moreno-Navarrete JM, Fernandez-Real JM, Salas-Salvado J. Total and undercarboxylated osteocalcin predictchanges in insulin sensitivity and beta cell function in elderlymen at high cardiovascular risk. Am J Clin Nutr 2012;95:249e55.
[14] Yeap BB, Chubb SA, Flicker L, et al. Reduced serum totalosteocalcin is associated with metabolic syndrome in older menvia waist circumference, hyperglycemia, and triglyceride levels.European J Endocrinol/European Federation of EndocrineSocieties 2010;163:265e72.
[15] Saleem U, Mosley Jr TH, Kullo IJ. Serum osteocalcin is associ-ated with measures of insulin resistance, adipokine levels, andthe presence of metabolic syndrome. Arteriosc Thromb VascBiol 2010;30:1474e8.
[16] Kanazawa I, Yamaguchi T, Yamauchi M, et al. Adiponectin isassociated with changes in bone markers during glycemiccontrol in type 2 diabetes mellitus. J Clin Endocrinol Metab2009;94:3031e7.
[17] Sayinalp S, Gedik O, Koray Z. Increasing serum osteocalcinafter glycemic control in diabetic men. Calcif Tissue Int1995;57:422e5.
[18] Bao YQ, Zhou M, Zhou J, et al. Relationship between serumosteocalcin and glycaemic variability in Type 2 diabetes. ClinExp Pharmacol Physiol 2011;38:50e4.
[19] Oz SG, Guven GS, Kilicarslan A, Calik N, Beyazit Y, Sozen T.Evaluation of bone metabolism and bone mass in patients withtype-2 diabetes mellitus. J Natl Med Assoc 2006;98:1598e604.
[20] Pittas AG, Harris SS, Eliades M, Stark P, Dawson-Hughes B.Association between serum osteocalcin and markers of meta-bolic phenotype. J Clin Endocrinol Metab 2009;94:827e32.
[21] Shea MK, Gundberg CM, Meigs JB, et al. Gamma-carboxylationof osteocalcin and insulin resistance in older men and women.Am J Clin Nutr 2009;90:1230e5.
[22] Fernandez-Real JM, Izquierdo M, Ortega F, et al. The relation-ship of serum osteocalcin concentration to insulin secretion,sensitivity, and disposal with hypocaloric diet and resistancetraining. J Clin Endocrinol Metab 2009;94:237e45.
[23] Szulc P, Chapuy MC, Meunier PJ, Delmas PD. Serum under-carboxylated osteocalcin is a marker of the risk of hip fracture inelderly women. J Clin Invest 1993;91:1769e74.
[24] Binkley NC, Krueger DC, Engelke JA, Foley AL, Suttie JW.Vitamin K supplementation reduces serum concentrations ofunder-gamma-carboxylated osteocalcin in healthy young andelderly adults. Am J Clin Nutr 2000;72:1523e8.
[25] Kumar R, Binkley N, Vella A. Effect of phylloquinone supple-mentation on glucose homeostasis in humans. Am J Clin Nutr2010;92:1528e32.
[26] Sakamoto N, Nishiike T, Iguchi H, Sakamoto K. Relationshipbetween acute insulin response and vitamin K intake in healthyyoung male volunteers. Diabetes Nutr Metab 1999;12:37e41.
[27] Gundberg CM, Nieman SD, Abrams S, Rosen H. Vitamin Kstatus and bone health: an analysis of methods for determina-tion of undercarboxylated osteocalcin. J Clin Endocrinol Metab1998;83:3258e66.
[28] Vergnaud P, Garnero P, Meunier PJ, Breart G, Kamihagi K,Delmas PD. Undercarboxylated osteocalcin measured witha specific immunoassay predicts hip fracture in elderly women:the EPIDOS Study. J Clin Endocrinol Metab 1997;82:719e24.
[29] Parfitt A. Skeletal heterogeneity and the purposes of boneremodelling: implications for the understanding of osteopo-rosis. In: Marcus R, Feldman D, Nelson D, Rosen C, editors.Osteoporosis. San Diego, CA: Academic; 2008. p. 71e89.

15. OSTEOCALCIN, UNDERCARBOXYLATED OSTEOCALCIN, AND GLYCEMIC CONTROL IN HUMAN SUBJECTS188
[30] Epker BN, Frost HM. A histological study of remodeling at theperiosteal, haversian canal, cortical endosteal, and trabecularendosteal surfaces in human rib. Anatom Rec 1965;152:129e35.
[31] Zebaze RM, Ghasem-Zadeh A, Bohte A, et al. Intracorticalremodelling and porosity in the distal radius and post-mortemfemurs of women: a cross-sectional study. Lancet 2010;375:1729e36.
[32] Parfitt A. The physiologic and clinical significance of bonehistomorphometric data. In: Recker R, editor. Bone Histo-morphometry Techniques and Interpretstion. Boca Raton: CRCPress; 1983. p. 142e223.
[33] Ducy P. The role of osteocalcin in the endocrine cross-talkbetween bone remodelling and energy metabolism. Dia-betologia 2011;54:1291e7.
[34] BjorneremA,Ghasem-ZadehA,BuiM,et al.Remodelingmarkersare associated with larger intracortical surface area but smallertrabecular surface area: a twin study. Bone 2011;49:1125e30.
[35] Danielson KK, Elliott ME, LeCaire T, Binkley N, Palta M. Poorglycemic control is associated with low BMD detected inpremenopausal women with type 1 diabetes. Osteoporos Int2009;20:923e33.
[36] Dennison EM, Syddall HE. Aihie Sayer A, Craighead S, PhillipsDI, Cooper C. Type 2 diabetes mellitus is associated withincreased axial bone density in men and women from theHertfordshire Cohort Study: evidence for an indirect effect ofinsulin resistance? Diabetologia 2004;47:1963e8.
[37] Levinger I, Zebaze R, Ghasem-Zadeh A, et al. Increased intra-cortical porosity is associated with higher serum under-carboxylated osteocalcin in middle-aged men. ANZBMS. GoldCoast; 2011.
[38] Ferron M, McKee MD, Levine RL, Ducy P, Karsenty G.Intermittent injections of osteocalcin improve glucose metab-olism and prevent type 2 diabetes in mice. Bone 2012;50:568e75.