Embed Size (px)
Citation preview

Deepika Reddy MD Department of Endocrinology

Management of hyperglycemic crisis Review need for inpatient glycemic control Brief overview of relevant trials Case based review of diabetes management strategies/review guidelines

Pathophysiology of DKA and HHS
Kitabchi A E et al. Dia Care 2006;29:2739-2748
Copyright © 2011 American Diabetes Association, Inc.

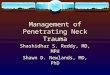
Protocol for the management of adult patients with DKA. *DKA diagnostic criteria: serum glucose >250 mg/dl, arterial pH <7.3, serum bicarbonate <18 mEq/l, and
moderate ketonuria or ketonemia.
Kitabchi A E et al. Dia Care 2006;29:2739-2748
Copyright © 2011 American Diabetes Association, Inc.

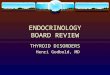
Protocol for the management of adult patients with HHS. HHS diagnostic criteria: serum glucose >600 mg/dl, arterial pH >7.3, serum bicarbonate >15 mEq/l, and minimal
ketonuria and ketonemia.
Kitabchi A E et al. Dia Care 2006;29:2739-2748
Copyright © 2011 American Diabetes Association, Inc.

Patients with known diabetes Patients with undiagnosed diabetes Stress hyperglycemia

Has an effect on Morbidity (including infection rates) Mortality Length of stay

Previous History DM New hyperglycemia
Normoglycemic
2030 consecutive adult patients admitted between July and October 1998
38% had hyperglycemia*
Umpierrez et al. J Clin Endocrinol Metab. 2002;87:978-982. slide from desantis ACPONLINE
*Hyperglycemia defined as admission or FPG ≥126 mg/dL or random BG ≥200 mg/dL

0
5
10
15
20
25
30
35
Normoglycemia Known Diabetes Newhyperglycemia
0
5
10
15
20
25
30
35
Normoglycemia Known Diabetes Newhyperglycemia
1.7%
16%*
3%
10% 11%
31%†
Total Inpatient Mortality
ICU Mortality
*P<0.01
n=1886
†P<0.01
n=243
Umpierrez et al. J Clin Endocrinol Metab. 2002;87:978-982 slide from desantis ACPONLINE .

0
0.5
1
1.5
2
2.5
3
3.5
4
<150 150-175 175-200 200-225 225-250 >250
Rat
e of
infe
ctio
n, %
3-day average postoperative blood glucose, mg/dL
P=0.001
Note inflection
point
Rates of deep sternal wound infection in 4864 patients with diabetes who underwent an open-heart surgical procedure
Furnary et al. Endocr Pract. 2004;10(suppl 2):21-33.

Reprinted from Furnary AP, et al. J Thorac Cardiovasc Surg. 2003;125:1007–1021 with permission from American Association for Thoracic Surgery. Purple: No DM
CII
10
8
6
4
0
Mortality (%)
87 88 89 90 91 92 93 94 98 99 00
Year
Patients with diabetes
Patients without DM diabetes
2
95 96 97 01

HYPERGLYCEMIA Index of disease severity
0
5
10
15
<150 150-175
176-200
201-225
226-250
>250
CardiacNon-Cardiac
0.9% 1.3% 2.3%
4.1% 6.0%
14.5%
Average post-op glucose
Mo
rta
lity
%
Furnary et al J Thorac Cardiovasc Surg 2003;125:1007-21

13
Intensive therapy to achieve blood glucose levels of 80–110 mg/dL reduced mortality (‐34%), sepsis (‐46%), dialysis (‐41%), blood transfusion (‐50%), and polyneuropathy (‐44%)
van den Berghe G, et al. N Engl J Med. 2001;345:1359–1367.
-60
-50
-40
-30
-20
-10
0
Reduction (%)
Mortality Sepsis Dialysis Polyneuropathy Blood
Transfusion
34%
46% 41%
44% 50%
N = 1,548

NEJM 2001;345:1359-67

Blood Glucose Overall Survival
VISEP Trial
Days
Conventional therapy Intensive therapy
0 1 2 3 4 5 6 7 8 9
Mea
n B
lood
Glu
cose
(m
g/dL
)
10 11 12 13 14 0
50
100
150
200
0 10
20
30
40
50
60
70
80
90 100
Days
Prob
abili
ty o
f Su
rviv
al (
%)
Conventional therapy (n=290)
Intensive therapy (n=247)
0
20
40
60
80
100
Brunkhorst FM et al. N Engl J Med. 2008;358:125-139.
Data from 537 patients: 247 received IIT goal: 80 – 110 mg/dL: mean BG 112 mg/dL 290 received CIT goal: 180 – 200 mg/dL: mean BG 151 mg/dL IIT, intensive insulin therapy; CIT, conventional insulin therapy.

VISEP Trial
Brunkhorst FM et al. N Engl J Med. 2008;358:125-139.
IIT (n=247)
CIT (n=290) P
Mortality rate, % 28 days 90 days
24.7 39.7
26.0 35.4
0.74 0.31
% of Patients with glucose ≤40 mg/dL 17.0% 4.1% <0.001
SOFA* score (mean) 95% CI
7.8 7.3-8.3
7.7 7.3-8.2
0.16
*SOFA – sequental organ failure assessment

NEJM2009;360:1283-97
NICE SUGAR

Griesdale et al., CMAJ 2009;180:821
Favors IIT Favors Control Hypoglycemic events

A 60 year old gentleman with a history of smoking is
admitted to the hospital with pneumonia. He is started on antibiotics and nebuliser treatments. He has a blood sugar on initial evaluation of 150

Would you start point of care blood sugar monitoring in this patient?
If blood sugars remain elevated would you get a HbA1c?

Test Normal Prediabetes Diabetes
Hemoglobin A1C
<5.7% 5.7-6.4% >6.5 %

The patient continues to have blood sugars in the 180 to 200 range. What would you do?
What are blood sugar goals in the hospital setting? What treatment would you use for blood sugar control in the hospital?
If using insulin what regimen would you use?

The endocrine society guidelines recommend: Pre‐meal blood gluose <140 mg/ dL.Random blood glucose <180 mg/ dL
In other words 140‐180 desired, in some situations 110‐140 acceptable. Blood sugars outside of these ranges ( <110 or >180 ) not acceptable

ADA/AACE Inpatient Task Force Endocrine Practice 2009;15;1-17
ADA/AACE Target Glucose Levels in ICU Patients
ICU setting: Insulin infusion should be used to control
hyperglycemia Starting threshold of no higher than 180 mg/dl Once IV insulin is started, the glucose level should
be maintained between 140 and 180 mg/dl Lower glucose targets (110-140 mg/dl) may be
appropriate in selected patients Targets <110 mg/dL are not recommended
Recommended 140-180
Acceptable 110-140
Not recommended < 110
Not recommended >180
ADA/AACE Inpatient Task Force Endocrine Practice 2009;15;1-17

ADA/AACE Inpatient Task Force Endocrine Practice 2009;15:1-17
ADA/AACE Target Glucose Levels in non‐ICU Patients
Non-ICU setting: Pre-meal glucose targets <140 mg/dL Random BG <180 mg/dL To avoid hypoglycemia, reassess insulin
regimen if BG levels fall below 100 mg/dL Occasional patients may be maintained with
a glucose range below or above these cut-points
Hypoglycemia= BG < 70 mg/dl Severe hypoglycemia= BG < 40 mg/dl

What would you use to treat the patient? Stop Orals Use Basal Insulin

Medication Primary complication
Sulfonylurea Hypoglycemia
Metformin Lactic acidosis, careful peri‐op, if getting dye
TZD CHF, CAD, Bladder CA
Alpha glucosidase inhibitors Diarrhea
Incretin Only helpful when eating, GI side‐effects

Stop orals Treat with Insulin Use basal (either with supplemental scale or bolus)
0.4 or 0.5 unit/kg/day in normal patients.50% of this would be basal needs.
0.3 units/kg/ day in elderly and renal failure 0.2 or 0.25 units/kg a day if NPO

Hyperglycemia is unfavorable, but hypoglycemia is also associated with adverse outcomes
To avoid hypoglycemia, the insulin regimen should be reassessed if blood glucose levels fall below 100 mg/ DL

Patient on tube feeds or parenteral nutrition Started on meds that cause hyperglycemia

Patient on tube feeds or parenteral nutrition Started on meds that cause hyperglycemia

What regimen should the patient use at home? What other aspects of care should be addressed?


Multidisciplinary Team Extends Beyond Caregivers
GLYCEMIC CONTROL
COMMITTEE
Endocrin-ologists
Hospitalists
P&T Committee
Nursing groups
Other internists
Pharmacists
Critical Care physicians
Patient Safety
Committee
Forms Committee Nutritionists/
Dietitians
Patient Representa-
tives
Hospital Informatics
Performance Improvement/
QI staff
Unit clerks/ secretaries
Chief residents/ residency program
directors Biomedical,
medical records, CPOE expertise
Departmental committees
Surgery, Trauma,
Orthopedics, Anesthesiology
leaders
Lab
Maynard et al. SHM Glycemic Control Workgroup. Available at: :http://www.hospitalmedicine.org/AM/Template.cfm? Section=Quality_Improvement_Resource_Rooms1&Template=/CM/HTMLDisplay.cfm&ContentID=4337.
OR or
Perioperative Committees