Embed Size (px)
Citation preview
Transcatheter ASD
closure, sans X-rays
Peter Ewert MD
Robert Beekman MD

Transcatheter closure of ASD’swithout fluoroscopy
Current transcatheter methods of defect closure require fluoroscopy with radiation exposure.
A recent study (Ewert et al.) demonstrates effectiveness of diagnostic, sizing and implantation procedures using echographic guidance, performed without fluoroscopy.
19 of 22 patients underwent successful defect closure without fluoroscopy.
All procedures were uneventful with the exception of one case of atrial flutter during diagnostic catheterization, cardioverted to sinus rhythm before implantation.
Ewert P, et al. Circulation 2000;101:847-849

In the absence of fluoroscopy, the diagnostic procedure still requires oxymetry of shunt volumes and pressure recordings from PA and RV using a Swan-Ganz catheter.
Defect is crossed with a multipurpose catheter (inner lumen 1.5 mm, length 65-70 cm).
An inner Fogarty balloon catheter is inflated and gently pulled back to precisely locate tip of first guidewire.
The sizing maneuver is performed over the wire.
Ewert P, et al. Circulation 2000;101:847-849
Transcatheter closure of ASD’swithout fluoroscopy

Diagnosis
Transesophageal long axis view. A diagnostic catheter is placed in the VCS to draw a blood sample for oxymetry.
Legend LA left atrium RA right atrium RAA right atrial appendage VCS superior caval vein ASD atrial septal defect

The sizing balloon has been inflated in front of the orifice of the left upper PV. The sizing catheter is guided over a wire in the left upper PV.
LegendLAA left atrial appendagePV pulmonary veinLV left ventricle* sizing balloon
Sizing

Defect closure is performed with the Amplatzer septal or PFO occluder device.
The Amplatzer occluder device has been the one device used for closure under echo guidance without fluoroscopy due to its rotational symmetry (no difficulties with obtaining the correct echo slice).
This device also has a relatively high metal content and is more uniformly echodense.
Ewert P, et al. Circulation 2000;101:847-849
Transcatheter closure of ASD’swithout fluoroscopy

An occluder has been advanced through a long sheath inserted into the left upper PV. Here, the sheath is pulled back with the occluder held in place. The distal end of the device begins to unfold.
Legend LA left atrium PV pulmonary vein LAA left atrial appendage* occluder device
Implantation (i)

The left atrial disc is configured behind the aortic root and can now be pulled back into the defect.
Legend LA left atrium AO aortic root* occluder device
Implantation (ii)

The occluder is completely configured inside the defect but yet connected to the delivery cable. Pulling reveals a stable position.
Legend LA left atrium RA right atrium AO aortic root* occluder device
Implantation (iii)

One disadvantage to this technique is the fact that the operator sees only echo slices of the catheter rather than the shadow of the catheter as would be seen under fluoroscopy.
The operator must become accustomed to this procedure and should be very disciplined, moving the catheter only when it is seen under imaging.
Transesophageal echo might be required for a longer period of time during the procedure.
Ewert P, et al. Circulation 2000;101:847-849
Transcatheter closure of ASD’swithout fluoroscopy
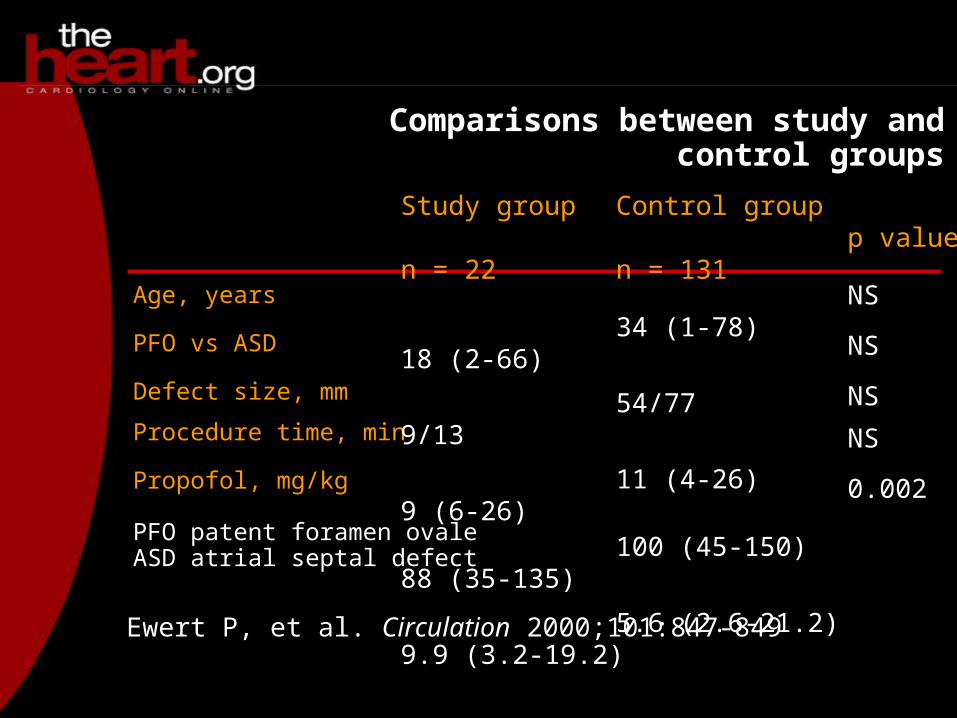
Comparisons between study and control groups
Age, years
PFO vs ASD
Defect size, mm
Procedure time, min
Propofol, mg/kg
PFO patent foramen ovale ASD atrial septal defect
Ewert P, et al. Circulation 2000;101:847-849
Study group
n = 22
18 (2-66)
9/13
9 (6-26)
88 (35-135)
9.9 (3.2-19.2)
Control group
n = 131
34 (1-78)
54/77
11 (4-26)
100 (45-150)
5.6 (2.6-21.2)
p value
NS
NS
NS
NS
0.002

Septal closures without fluoroscopy should not be performed outside the cath lab, and fluoroscopy should remain readily available if complications arise.
Closure under echo guidance alone should be restricted to experienced centers, and operators should be well trained under echo guidance with backgrounds in the fluoroscopic approach.
Ewert P, et al. Circulation 2000;101:847-849
Transcatheter closure of ASD’swithout fluoroscopy

“One of [our surgical colleagues’] major concerns about what we have to offer is the radiation exposure. So I think that you have probably convinced them that catheter therapy is clearly the treatment of choice for these defects.”
Dr Robert Beekman Director, Division of CardiologyChildren's Hospital Medical CenterCincinnati, OH
Transcatheter closure of ASD’swithout fluoroscopy





![[Beekman House] Heraldry and Regalia of War](https://img.dokumen.tips/doc/110x75/55721386497959fc0b9278c2/beekman-house-heraldry-and-regalia-of-war.jpg)























