Embed Size (px)
Citation preview
58Topical Hemostatic Agents in ObstetricHemorrhage: International Case ReportsC. Wohlmuth and J. Dela Merced
INTRODUCTION AND BACKGROUND
Topical hemostatic agents are utilized as adjuncts tocontrol intraoperative bleeding when standard surgicaltechniques (such as suturing, ligature, cautery, or pres-sure) are insufficient or impractical to implement1.Intraoperative scenarios where topical hemostaticagents may serve as adjuncts include bleeding nearvital organs or nerves, at needle-holes, from raw sur-face areas, in friable or attenuated tissue, or in patientswho are anticoagulated, have bleeding diatheses, orhave platelet dysfunction.
Physical agents and biologically active agents com-prise the two main categories of topical hemostaticproducts. Physical agents promote hemostasis utilizinga passive substrate. Biologically active agents stimulatethe coagulation cascade locally at the bleeding site1.
Biologically active topical hemostatic agents havebeen marketed in the United States for over 10 years,paralleling the recent advances in biotechnology thatresulted in rapid growth of available topical hemostaticagents2. Their use for intraoperative hemorrhage con-trol has been described by various surgical specialties,including cardiovascular, otolaryngology, urology,and others2–6. Usage in gynecologic surgery has beenreported, including laparoscopy, myomectomy,oncologic debulking and inguinal lympha-denectomy7–11.
In 2007 Moriarty et al.12 (UK) presented a casereport on the use topical hemostatic agents in massivepostpartum hemorrhage (PPH) in a patient whounderwent emergency cesarean delivery due to pla-cental abruption. Approximately 3 hours after cesareandelivery, the patient underwent laparotomy and totalabdominal hysterectomy for life-threatening hemor-rhage resulting from uterine atony that was unrespon-sive to conservative measures. The patient developeddisseminated intravascular coagulation, and, after hys-terectomy, continued to bleed from vascular venousplexuses at the vaginal vault, as well as from sutureholes. The topical hemostatic agent comprised ofgelatin–thrombin matrix, FloSealTM (Baxter Health-care Corporation, Fremont, California, USA), wasapplied to the bleeding areas. Thereafter, the authorsdescribed rapid achievement of hemostasis.
Subsequently, in 2010, Law et al. (Hong Kong)reported a case of successful control of persistent PPHfrom the placental implantation site, using FloSeal13.Two hours after cesarean delivery for placenta previa,the patient underwent re-laparotomy for persistentvaginal bleeding, where heavy bleeding from thelower uterine segment was noted. The authorsdescribed ineffective suturing for controlling bleedingin the deep placental site, and, therefore, FloSeal wasapplied. Hemorrhage control was achieved withuterine preservation.
In the same year, Fuglsang and Petersen (Denmark)published a series of 15 cases, delivered by cesarean forplacenta previa, where excessive or intractable loweruterine segment hemorrhage was successfully con-trolled with direct local topical application of hemo-static collagen fleece coated with a mixture of humanfibrinogen and thrombin (TachoSilTM, Nycomed,Denmark), at the time of cesarean section14.
Subsequently, in 2011, Tinelli (Italy) reported acase where TachoSil application successfully con-trolled hemorrhage at the uterine incision site. After ascheduled repeat cesarean section, the patient wasfound in hemorrhagic shock on postoperative day 3.At re-laparotomy, hemoperitoneum was found,resulting from constant oozing from the uterineincision site and bladder vessels. After ineffectivehemostatic suturing, TachoSil was applied with suc-cessful hemorrhage control15.
Similarly, in 2011, Wohlmuth and Dela Merced(US) reported a case of placental implantation sitehemorrhage, controlled at the time of cesarean deliv-ery, with gelatin–thrombin matrix (FloSeal) in apatient with placenta previa16.
In the case reports described, topical hemostaticagents were administered after unsuccessful utilizationof traditional PPH treatments. These included utero-tonic agents, vessel ligation, uterine compressionsutures, packing or balloon tamponade, over-sewingplacental bed bleeding sites, recombinant activatedfactor VII and consideration of uterine arteryembolization17. The ineffectiveness of the traditionalmethods of hemorrhage control in the cases of pla-centa previa was attributed to bleeding from the non-contractile lower uterine segment, large surface areas
480
of active bleeding, vascular tissue depth at the placentalsite and tissue friability13,14,16. In the event conserva-tive measures fail to control hemorrhage, hysterectomy,generally, is considered as a life-saving procedure.
Where topical hemostatic agents were usedsuccessfully at the time of cesarean delivery,re-laparotomy was avoided and uterine preservationwas achieved14,16. Additionally, with rapid access andsuccessful application of a topical hemostatic agent,the risks of prolonging bleeding time and associatedmassive blood transfusion can be decreased.
Topical hemostatic agent use in complicated obstet-ric genital laceration was reported by Whiteside et al.(US), in 201018. A 21-year-old primipara patient wasfound to have a right labial hematoma that developed2 hours after spontaneous vaginal delivery of twinswith immediate repair of vaginal lacerations. Thehematoma disrupted the suture line of the originalrepair. Despite additional suturing and vaginal pack-ing, the hematoma continued to expand, leading to a10 cm wide hematoma extending from the superiorlabia majora to the ischial fossa. At surgical explorationand evacuation, poor tissue quality was encountered,with suturing attempts unsuccessful in the presence offriable tissue. Direct pressure applied to the surgicalbed did not control hemorrhage, including pressureapplied with adjunctive use of microfibrillar collagenhemostat powder, a non-biologically active topicalhemostatic agent. With application of biologicallyactive, prohemostatic fibrin sealant (TISSEELTM,Baxter Healthcare Corporation, Fremont, California,
USA), hemostasis with tissue sealing was promptlyachieved.
In 2009, a similar case of TISSEEL use in managingPPH from obstetric trauma was reported by Dhulkotiaet al.19 (UK).
BIOLOGICALLY ACTIVE TOPICAL HEMOSTATICAGENTS
Because the published case reports of successful topicalhemostatic agent use in obstetric hemorrhage are ofresorbable biologically active products, the focus ofdiscussion in this chapter is on this category of topicalhemostatic agents, specific to those agents reported.
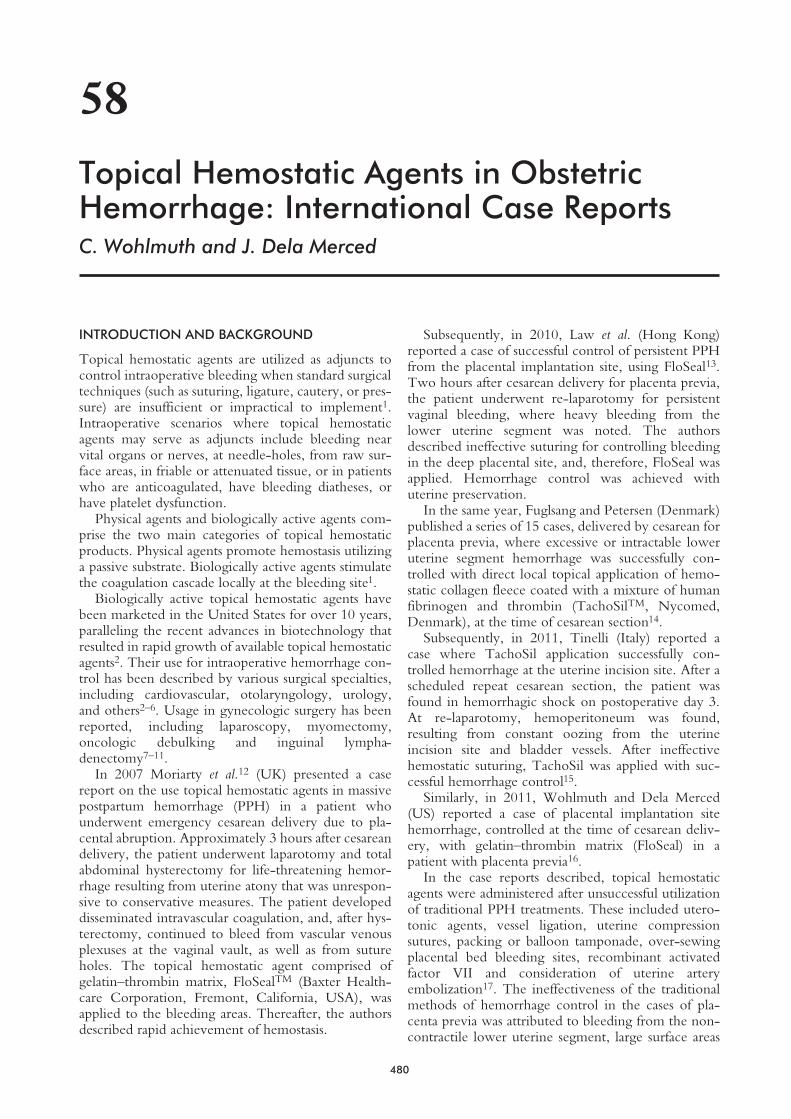
Biologically active topical hemostatic agents stimu-late the coagulation cascade, primarily through thetransformation of fibrinogen to fibrin by thrombin’senzymatic action (Figure 1).
The multitude of topical hemostatic agents availablevaries in composition, mechanism of action andmethod of use. The surgeon should be familiar withthe various products’ similarities and differences beforeuse2 (Table 1).
Liquid pro-hemostatic fibrin sealant (TISSEEL) wasapproved by the United States Food and DrugAdministration (FDA) in 1998 as an adjunct tohemostasis in cardiopulmonary bypass and splenicinjury surgeries. It is comprised of human fibrinogenand human thrombin. At the time of usage, the twocomponents are combined to produce fibrin, mimick-ing the final stage of the coagulation cascade20. The
481
Topical Hemostatic Agents in Obstetric Hemorrhage: International Case Reports
GELATINCELLULOSE
COLLAGEN
XI XIa
IX IXa
X Xa
VIIa VIITissue Thromboplastin
(Tissue Factor)Ca++
PF3Ca++
VIII
CONTACTACTIVATION
Collagen from damagedvascular endothelium
Ca++
PF3Ca++
Prothrombin
Thrombin converts fibrinogen to fibrin
Thrombin
Fibrinogen Fibrinmonomer
Fibrinpolymer
XIIIXIIIa Ca++
INTRINSIC PATHWAY EXTRINSIC PATHWAY
RESTINGPLATELETS
PLATELETACTIVATION
VIIIvWFGP1b
FibronectinTISSUE DAMAGE
HMW Kininogen
Pre-kallikrein Kallikrein
XII XIIa
PLATELETGRANULERELEASEFACTORS
Va V
Fibrin clot
Figure 1 Coagulation cascade. Topical hemostatic agents containing cellulose, collagen, or gelatin stimulate the coagulation cascadethrough contact activation. Biologically active agents contain, either singly or in combination, thrombin and/or fibrinogen. Whencombined, thrombin’s enzymatic action transforms fibrinogen into fibrin, augmenting the final stages of the coagulation cascade. FromBaxter Healthcare Corporation, with permission

482
POSTPARTUM HEMORRHAGE
Hem
osta
ticag
ent
Sour
cePr
oduc
ttra
dena
me
FDA
†ap
prov
alH
owsu
pplie
dB
iolo
gica
llyac
tive
mec
hani
smR
esor
ptio
ntim
eR
ecom
men
ded
use
Prec
autio
ns
Fibr
inse
alan
tsp
ray
Hum
anfib
rino
gen,
hum
anth
rom
bin,
synt
hetic
apro
tinin
TIS
SEE
L™19
98Li
quid
spra
yW
hen
com
bine
d,th
rom
bin’
sen
zym
atic
actio
ntr
ansfo
rms
fibri
noge
nin
tofib
rin,
augm
entin
gfin
alst
ages
ofco
agul
atio
nca
scad
e
Imm
edia
teW
here
tissu
ead
here
nce
isde
sired
inad
ditio
nto
hem
osta
sis
Alle
rgic
reac
tion
toap
rotin
inD
ono
tinj
ecti
ntra
vasc
ular
lyD
ono
tuse
for
seve
reor
brisk
blee
ding
.M
ade
from
hum
anpl
asm
aan
dm
ayca
rry
risk
oftr
ansm
ittin
gin
fect
ious
dise
ase
Gel
atin
–thr
ombi
nm
atri
xB
ovin
ege
latin
,hu
man
thro
mbi
nFl
oSea
l™19
99V
iscou
sge
lU
pon
cont
actw
ithbl
ood,
the
fibri
noge
nso
urce
,co
ncen
trat
edth
rom
bin
with
inth
ege
latin
mat
rix
conv
erts
fibri
noge
nin
tofib
rin
6–8
wee
ksR
ange
ofde
gree
sof
blee
ding
,fr
omoo
zing
tosp
urtin
g;W
here
tissu
eta
mpo
nade
effe
ctis
desir
ed;
Irre
gula
rw
ound
surf
aces
Swel
lvol
ume
20%
Alle
rgic
reac
tion
tobo
vine
mat
eria
lD
ono
tinj
ecti
ntra
vasc
ular
lyM
ade
from
hum
anpl
asm
aan
dm
ayca
rry
risk
oftr
ansm
ittin
gin
fect
ious
dise
ase
Exc
ess
FloS
eals
houl
dbe
rem
oved
byge
ntle
irri
gatio
n
Fibr
inse
alan
tpa
tch
Equ
ine
colla
gen,
hum
anth
rom
bin,
hum
anfib
rino
gen
Tac
hoSi
l®20
10Fl
eece
patc
hA
neq
uine
colla
gen
spon
geis
coat
edon
one
side
with
fibri
noge
nan
dth
rom
bin,
whi
ch,u
pon
cont
actw
ithph
ysio
logi
calf
luid
s,fo
rma
fibri
nse
alan
tpat
ch
13w
eeks
††La
rge
blee
ding
raw
surf
ace
area
s;W
here
prom
otin
gtis
sue
seal
ing
isde
sired
inad
ditio
nto
hem
osta
sis
Alle
rgic
reac
tion
toeq
uine
prot
eins
Do
notu
sein
trav
ascu
larly
Do
notu
sefo
rse
vere
orbr
iskbl
eedi
ngM
ade
from
hum
anpl
asm
aan
dm
ayca
rry
risk
oftr
ansm
ittin
gin
fect
ious
dise
ase
Rem
ove
unat
tach
edpi
eces
*Off-
labe
luse
† Foo
dan
dD
rug
Adm
inist
ratio
n,U
nite
dSt
ates
.††
Tac
hoSi
l®Pr
escr
ibin
gIn
form
atio
nLe
afle
t,re
vise
d:[0
4/20
10].
12.1
‘In
anim
alst
udie
s,T
acho
Silp
rogr
essiv
ely
biod
egra
des
with
only
afe
wre
mna
nts
left
afte
r13
wee
ks.A
fter
com
plet
ebi
odeg
rada
tion,
nore
mna
nts
ofth
eT
acho
Silp
atch
rem
aine
din
the
body
.’
Tab
le1
Top
ical
hem
osta
ticag
ents
inm
anag
emen
tofp
ostp
artu
mhe
mor
rhag
e,in
publ
ished
case
repo
rts*

aprotinin component serves as an antifibrinolyticagent. TISSEEL adheres to wound surfaces, achievinghemostasis as well as tissue sealing or gluing. In hemor-rhage scenarios, where tissue adherence is desired inaddition to hemostasis, liquid fibrin sealant may bepreferred.
TISSEEL is supplied as both freeze-dried kits andpre-filled syringes. The freeze-dried kit is stored at2–25�C. The pre-filled syringe is frozen and stored at−20�C or less. In preparing the freeze-dried kit, toprevent premature clotting, separate syringes are usedfor reconstituting, as well as applying, the sealer pro-tein and thrombin. In preparing the frozen pre-filledsyringe, thawing can be performed at room tempera-ture for up to 48 hours, on the sterile field using33–37°C sterile water bath, or off the sterile field usingwater bath or incubator. In geographic regions lackingfreezing capabilities, liquid fibrin sealant use is limitedto the freeze-dried formulation (Figure 2).
Gelatin–thrombin hemostatic matrix (FloSeal)received FDA approval in 1999 as an adjunct tohemostasis when ligature or conventional proceduresare ineffective or impractical. A matrix of bovine gela-tin and human thrombin, it provides a concentratedsource of thrombin within cross-linked gelatin gran-ules21 (Figure 3).
To activate the hemostatic matrix coagulationmechanism, blood must be present to provide thefibrinogen source. Upon contact with blood, the con-centrated thrombin converts fibrinogen to fibrin. As ahigh viscosity gel, the gelatin–thrombin matrix fluidityconforms to irregular wound surfaces, thus fillingdefects and crevices3,16. Additionally, gelatin–thrombin matrix provides a tamponade effect, as gela-tin granules expand approximately 20% within about10 minutes of application. Furthermore, FloSeal isdescribed to be ‘effective on surgical bleeding, fromoozing to spurting’21. The combination of fluidity,tamponade and arterial bleed effectiveness deemsgelatin–thrombin hemostatic matrix a recommendedhemostatic product in cases of irregular woundsurfaces or hard-to-reach surfaces and of a range ofdegrees of bleeding from oozing to spurting3,21.
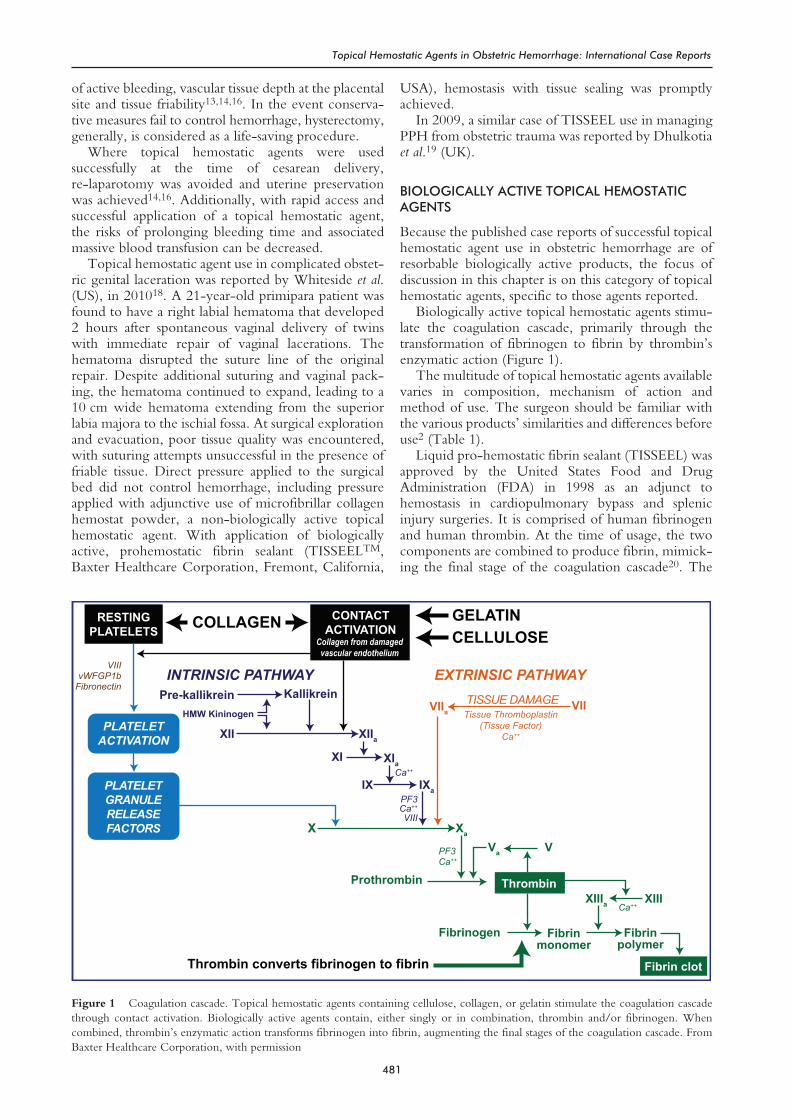
Gelatin–thrombin hemostatic matrix is supplied as afreeze-dried kit containing: gelatin matrix in a 10 mlsyringe, a vial of human thrombin (lyophilized), a vialof calcium chloride solution, and mixing accessories(bowl for thrombin, two 5 ml syringes, Luer connec-tor and applicator tips). After reconstitution oflyophilized thrombin in calcium chloride solution,gelatin matrix granules are added to the mix by passingthrombin and gelatin between the two syringes. Themixing procedure is reported to take 2 minutes13 (Fig-ures 4 and 5). FloSeal is stored between 2°C and 25°C(36°F and 77°F), and should not be frozen (see alsoChapter 57).
Collagen–thrombin–fibrinogen patch (TachoSil)was granted FDA approval in April 2010 as an adjunctto hemostasis in cardiovascular surgery. An equinecollagen sponge is coated on one side with fibrinogenand thrombin22. Upon contact with physiological
483
Topical Hemostatic Agents in Obstetric Hemorrhage: International Case Reports
Figure 2 Fibrin sealant liquid spray application. From BaxterHealthcare Corporation, with permission
Figure 3 Cross-linked gelatin granules, approximately 0.5 mmdiameter, create open spaces that allow high concentrations ofthrombin to surround each gelatin particle. From Baxter HealthcareCorporation, with permission
Figure 4 Gelatin–thrombin matrix kit. From Baxter HealthcareCorporation, with permission
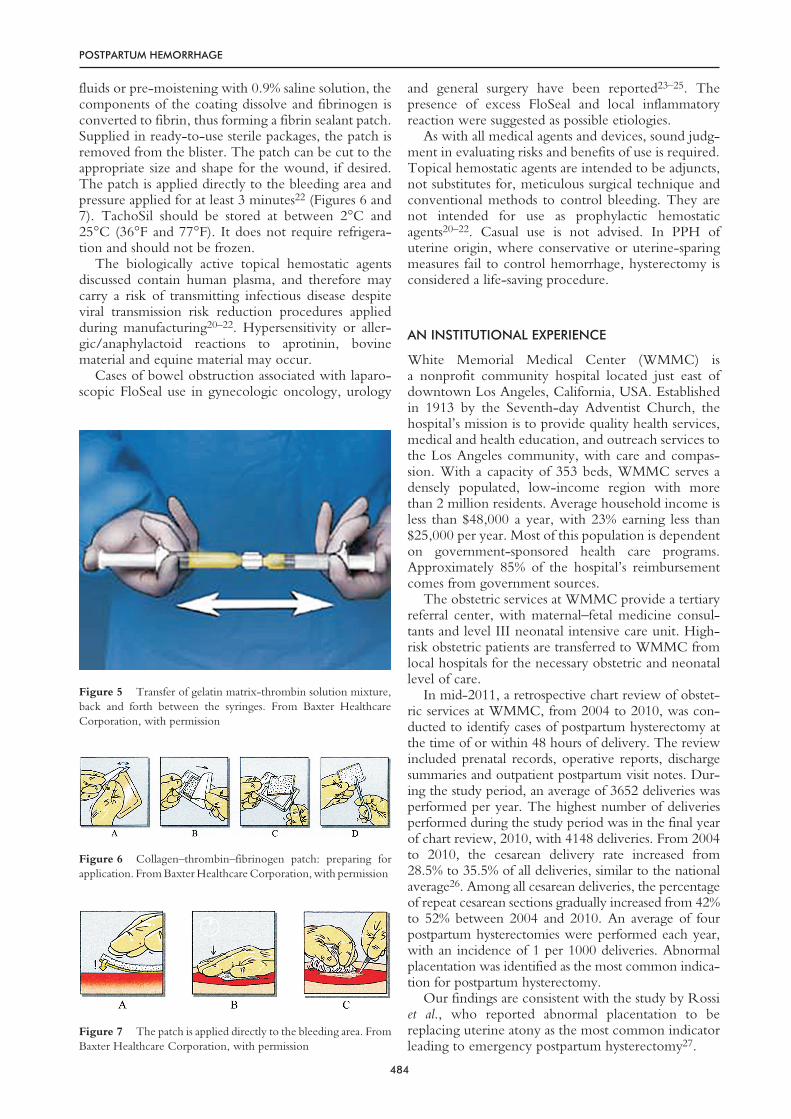
fluids or pre-moistening with 0.9% saline solution, thecomponents of the coating dissolve and fibrinogen isconverted to fibrin, thus forming a fibrin sealant patch.Supplied in ready-to-use sterile packages, the patch isremoved from the blister. The patch can be cut to theappropriate size and shape for the wound, if desired.The patch is applied directly to the bleeding area andpressure applied for at least 3 minutes22 (Figures 6 and7). TachoSil should be stored at between 2°C and25°C (36°F and 77°F). It does not require refrigera-tion and should not be frozen.
The biologically active topical hemostatic agentsdiscussed contain human plasma, and therefore maycarry a risk of transmitting infectious disease despiteviral transmission risk reduction procedures appliedduring manufacturing20–22. Hypersensitivity or aller-gic/anaphylactoid reactions to aprotinin, bovinematerial and equine material may occur.
Cases of bowel obstruction associated with laparo-scopic FloSeal use in gynecologic oncology, urology
and general surgery have been reported23–25. Thepresence of excess FloSeal and local inflammatoryreaction were suggested as possible etiologies.
As with all medical agents and devices, sound judg-ment in evaluating risks and benefits of use is required.Topical hemostatic agents are intended to be adjuncts,not substitutes for, meticulous surgical technique andconventional methods to control bleeding. They arenot intended for use as prophylactic hemostaticagents20–22. Casual use is not advised. In PPH ofuterine origin, where conservative or uterine-sparingmeasures fail to control hemorrhage, hysterectomy isconsidered a life-saving procedure.
AN INSTITUTIONAL EXPERIENCE
White Memorial Medical Center (WMMC) isa nonprofit community hospital located just east ofdowntown Los Angeles, California, USA. Establishedin 1913 by the Seventh-day Adventist Church, thehospital’s mission is to provide quality health services,medical and health education, and outreach services tothe Los Angeles community, with care and compas-sion. With a capacity of 353 beds, WMMC serves adensely populated, low-income region with morethan 2 million residents. Average household income isless than $48,000 a year, with 23% earning less than$25,000 per year. Most of this population is dependenton government-sponsored health care programs.Approximately 85% of the hospital’s reimbursementcomes from government sources.
The obstetric services at WMMC provide a tertiaryreferral center, with maternal–fetal medicine consul-tants and level III neonatal intensive care unit. High-risk obstetric patients are transferred to WMMC fromlocal hospitals for the necessary obstetric and neonatallevel of care.
In mid-2011, a retrospective chart review of obstet-ric services at WMMC, from 2004 to 2010, was con-ducted to identify cases of postpartum hysterectomy atthe time of or within 48 hours of delivery. The reviewincluded prenatal records, operative reports, dischargesummaries and outpatient postpartum visit notes. Dur-ing the study period, an average of 3652 deliveries wasperformed per year. The highest number of deliveriesperformed during the study period was in the final yearof chart review, 2010, with 4148 deliveries. From 2004to 2010, the cesarean delivery rate increased from28.5% to 35.5% of all deliveries, similar to the nationalaverage26. Among all cesarean deliveries, the percentageof repeat cesarean sections gradually increased from 42%to 52% between 2004 and 2010. An average of fourpostpartum hysterectomies were performed each year,with an incidence of 1 per 1000 deliveries. Abnormalplacentation was identified as the most common indica-tion for postpartum hysterectomy.
Our findings are consistent with the study by Rossiet al., who reported abnormal placentation to bereplacing uterine atony as the most common indicatorleading to emergency postpartum hysterectomy27.
484
POSTPARTUM HEMORRHAGE
Figure 5 Transfer of gelatin matrix-thrombin solution mixture,back and forth between the syringes. From Baxter HealthcareCorporation, with permission
Figure 6 Collagen–thrombin–fibrinogen patch: preparing forapplication. From Baxter Healthcare Corporation, with permission
Figure 7 The patch is applied directly to the bleeding area. FromBaxter Healthcare Corporation, with permission

Our institutional experience includes other obstet-ric hemorrhage cases that were successfully managedwith topical hemostatic agents, in addition to our casereport of placenta previa hemorrhage16.
Case 1
A 35-year-old patient, gravidity 2, parity 1, delivered aterm male infant by vacuum assisted vaginal delivery.No vaginal or cervical lacerations were noted.Approximately 3 hours after delivery, the patientreported sudden onset profuse vaginal bleeding associ-ated with Valsalva. At examination, a ruptured vaginalhematoma was noted, extending from the rupture siteat the 6 o’clock position in the distal vagina at the levelof the introitus, to the full length of the vagina withhematoma dissection of the rectovaginal septum andinto the right ischial fossa. The depth of the defect wasestimated to be 10 cm. Multiple scattered arterial andvenous bleeding sites were diffusely distributed overthe length of the rectovaginal septum, which was ana-tomically distorted by the marked distention of thehematoma. An attempt to suture was ineffective in thepresence of friable attenuated tissue and large surfacearea of bleeding. Because the rectal mucosa wasin close proximity and at risk when suturing thesurrounding poor quality tissue, use of a topical hemo-static agent was chosen. Gelatin–thrombin matrix waspreferred due to the presence of arterial bleeding, largehard-to-reach and irregular surface area, tamponadeeffect feature and desire for a non-adhering agent inorder to leave an open drainage site. Bleeding wascontrolled in less than 2 minutes after one applicationof hemostatic gel. In the presence of brisk bleeding, apowder form topical hemostatic agent was not chosendue to risk of being washed away in the flow of bloodbefore adequate polymerization of fibrin could occur.
Case 2
A 44-year-old multiparous patient presented withruptured amniotic membranes in a pre-viable mid-trimester gestation. After passing the fetus vaginally,the patient developed a prolonged prothrombintime, prolonged activated thromboplastin time andthrombocytopenia, with the total clinical picture con-sistent with coagulopathy of sepsis. Furthermore, thepatient continued to have profuse vaginal bleeding,assessed to be from coagulopathy and possibly placentaaccreta, as retained placenta was diagnosed in thispatient with prior cesarean deliveries. Coordinatingthe timing for blood replacement to correct thecoagulopathy-based source of bleeding, with the tim-ing for prompt surgical removal of the placental-basedsource of bleeding, is critical in optimizing outcomes.Continued blood loss, whether from coagulopathy ofsepsis or from abnormal placentation or both, canexacerbate the underlying condition with the devel-opment of hemorrhagic shock and progressive
disseminated intravascular coagulation. As multi-unitblood transfusions were administered, placental deliv-ery was performed by manual removal. Findings weresuggestive of placenta accreta. The patient underwentemergency hysterectomy, with intraoperative bleed-ing consistent with on-going coagulopathy. Thepelvic raw surfaces were large, as extensive lysisof adhesions was required in order to complete thehysterectomy. With massive blood transfusion inprogress and administration of recombinant activatedfactor VII28, control of bleeding at the vaginal cuff andpelvic raw surfaces was achieved with the adjunctiveuse of gelatin–thrombin hemostatic matrix.
The institutional experience at WMMC is similarto the case reports by Moriarty, Fuglsang and White-side12,14,18.
DISCUSSION
Recent advances in biotechnology have added bio-logically active features to topical hemostatic agents.These are shown to be effective in controllingintraoperative bleeding in several surgical specialties,including controlled clinical trials of cardiac surgery3.In PPH, current literature is comprised of case reports,totaling 20 cases. Seventeen cases were reported forhemorrhage associated with placenta previa13,14,16.Two of these were associated with obstetricgenital injury18,19. One case was associated withdisseminated intravascular coagulation at emergencyhysterectomy12.
With a rising cesarean delivery rate26 and the associ-ated increased risk for placenta previa and placentaaccreta29, the presence of 17 cases in the literatureof PPH associated with placenta previa successfullymanaged with resorbable bioactive topical hemostaticagent invites further investigation and considerationfor both adjunct and primary treatment with topicalhemostatic agents13,14,16.
As an adjunct intervention when standard surgicalmethods fail to control hemorrhage, topicalhemostatic agents may have a more primary rolewhere surgical intervention is difficult, such as inunder-resourced geographic regions, with limited orno access to emergency surgical facilities, blood bank-ing resources, parenteral administration of medicationcapabilities and invasive radiology embolization.Availability and accessibility of topical hemostaticagents, with features of quick preparation and easyapplication, may decrease morbidity and mortalityassociated with delayed treatment of hemorrhage.
Although the use of topical hemostatic agents inmanaging PPH in peer-reviewed literature is limitedto case reports, further studies may provide informa-tion to solidify topical hemostatic agents as an adjunctor primary treatment in PPH.
The authors have no financial interest or otherrelationship with the manufacturers of the productsdiscussed in this manuscript.
485
Topical Hemostatic Agents in Obstetric Hemorrhage: International Case Reports

References
1. Peralta E. Overview of topical hemostatic agents used in theoperating room. 2011. http://www.uptodate.com/contents/overview-of-topical-hemostatic-agents
2. Achneck HE, Sileshi B, Jamiolkowski RM, et al. A compre-hensive review of topical hemostatic agents. Ann Surg 2010;251:217–28
3. Oz MC, Cosgrove DM 3rd, Badduke BR, et al. Controlledclinical trial of a novel hemostatic agent in cardiac surgery.The Fusion Matrix Study Group. Ann Thorac Surg 2000;69:1376–82
4. Gall RM, Witterick IJ, Shargill NS, Hawke M. Control ofbleeding in endoscopic sinus surgery: use of a novel gela-tin-based hemostatic agent. J Otolaryngol 2002;31;5:271–4
5. Hong YM, Loughlin KR. The use of hemostatic agents andsealants in urology. J Urol 2006;176:2367–74
6. Gazzeri R, Galarza M, Neroni M, Alfieri A, Giordano M.Hemostatic matrix sealant in neurosurgery: a clinical andimaging study. Acta Neurochir 2011;153:148–55
7. Angioli R, Ludovico M, Roberto M, et al. Feasibility of theuse of novel matrix hemostatic sealant (FloSeal) to achievehemostasis during laparoscopic excision of endometrioma.J Min Inv Gynecol 2009;16:153–6
8. Ebert AD, Hollauer A, Fuhr N, Langolf O, Papadopoulos T.Laparoscopic ovarian cystectomy without bipolar coagulationor sutures using a gelatin-thrombin matrix sealant (FloSeal):first support of a promising technique. Arch Gynecol Obstet2009;280:161–5
9. Raga F, Sanz-Cortez M, Bonilla F, et al. Reducing blood lossat myomectomy with use of a gelatin-thrombin matrixhemostatic sealant. Fertil Steril 2009;92:356–60
10. Madhuri TK, Tailor A, Butler-Manuel S. Use of surgicalsealant in debulking surgery for advanced ovarian carcinoma –case report. Eur J Gynaecol Oncol 2010;31:582–3
11. Han LY, Schimp V, Oh JC, Ramirez PT. A gelatin matrix-thrombin tissue sealant (FloSeal) application in the manage-ment of groin breakdown after inguinal lymphadenectomyfor vulvar cancer. Int J Gynecol Cancer 2004;14:621–4
12. Moriarty KT, Premila S, Bulmer PJ. Use of FloSeal haemo-static gel in massive obstetric haemorrhage: a case report. Br JObstet Gynaecol 2008;115:793–5
13. Law WL, Chor CM, Leung TY. Use of hemostatic gel inpostpartum hemorrhage due to placenta previa. ObstetGynecol 2010;116:528–30
14. Fuglsang K, Petersen LK. New local hemostatic treatment forpostpartum hemorrhage caused by placenta previa at cesareansection. Acta Obstet Gynecol 2010;89:1346–9
15. Tinelli A. Post-cesarean section hemorrage treated by a colla-gen patch coated with the human coagulation factors. J ClinicCase Reports 2011;1:1000e102
16. Wohlmuth C, Dela Merced J. Gelatin-thrombin hemostaticmatrix in the management of placental site postpartumhemorrhage, a case report. J Reprod Med 2011;56:271–3
17. Doumouchtsis SK, Papageorghiou AT, Arulkumaran S.Systemic review of conservative management of postpartumhemorrhage: what to do when medical treatment fails. ObstetGynecol Surv 2007;62:540–7
18. Whiteside J, Asif RB, Novello RJ. Fibrin sealant for manage-ment of complicated obstetric lacerations. Obstet Gynecol2010;115:403–4
19. Dhulkotia JS, Alazzam M, Galimberti A. TISSEEL formanagement of traumatic postpartum haemorrhage. ArchGynecol Obstet 2009;279:437–9
20. Baxter Healthcare Corporation. TISSEEL [Fibrin Sealant]Full Prescribing Information. Hayward, California, USA:Baxter Healthcare Corporation, 2010
21. Baxter Healthcare Corporation. FloSeal Hemostatic MatrixInstructions for Use. Hayward, California, USA: BaxterHealthcare Corporation, 2010
22. Baxter Healthcare Corporation. TachoSil® PrescribingInformation Leaflet. 2010. www.baxtersurgery.com/resources/pdfs/TachoSil
23. Clapp B, Santillan A. Small bowel obstruction after FloSealuse. JSLS 2011;15:361–4
24. Suzuki Y, Vellinga TT, Istre O, Einarsson JI. Small bowelobstruction associated with use of a gelatin-thrombin matrixsealant (FloSeal) after laparoscopic gynecologic surgery. JMinim Invasive Gynecol 2010;17:641–5
25. Hobday CD, Milam MR, Milam RA, Euscher E, Brown J.Postoperative small bowel obstruction associated with use ofhemostatic agents. J Minim Invasive Gynecol 2009;16:224–6
26. Hamilton BE, Martin JA, Ventura SJ. United States Depart-ment of Health and Human Services, Centers for DiseaseControl and Prevention, National Center for HealthStatistics, National Vital Statistics Reports 2009;57:12
27. Rossi AC, Lee RH, Chmait RH. Emergency postpartumhysterectomyy for uncontrolled postpartum bleeding, asystematic review. Obstet Gynecol 2010;115:637–44
28. Bouwmeester FW, Jonkhoff AR, Verheijen RH, van GeijnHP. Successful treatment of life-threatening postpartumhemorrhage with recombinant activated factor VII. ObstetGynecol 2003;101:1174–6
29. Miller DA, Chollet JA, Goodwin TM. Clinical risk factors forplacenta previa-placenta accreta. Am J Obstet Gynecol 1997;177:210–4
486
POSTPARTUM HEMORRHAGE