Embed Size (px)
Citation preview

10/15/2015
1
Anesthesia Considerations in Obstetric Hemorrhage
Jennifer Lucero, MDAssistant Professor
Division of Obstetric Anesthesia
Post-PartumHemorrhage
• Atony• Retained Placenta• Placenta accreta• Defects in Coagulation• Vaginal laceration• Uterine Inversion
Common Things Being CommonMost Common Cause of Maternal Mortality Worldwide.• In the US roughly 3% rate of PPH• Increasing rates of transfusion Obstetrics
– Increased Cesarean Delivery– Abnormal Placentation
• Atony 80% of causes of Severe PPH
WHO Analysis of Causes of Maternal Death Systematic Review
Khan KS, Wojdyla D, Say L, et.al., Lancet 2006; 367: 1066-74
DevelopedCountries
Africa AsiaLatin Am.Caribbean
Hemorrhage 13.4% 33.9% 30.8% 20.8%
HypertensiveDisorders
16.1% 9.1% 9.1% 25.7%
Infections 2.1% 9.7% 11.6% 7.7%
Abortion 8.2% 3.9% 5.7% 12.0%
Embolism 14.9% 2.0% 0.4% 0.6%

10/15/2015
2
Flood KM, et al. Am J Obstet Gynecol. 2009; 200: 632
Accreta and Peripartum Hysterectomy
Creanga AA, et al. Obstet Gynecol. 2015; 125: 5-12
Anesthesiology 2014; 121:450-8

10/15/2015
3
Graphic Source: CMQCC California Maternal Quality Care Collaborative
Source:www.cmqcc.org/ob_hemorrhage
• Developed a Tool Kit for OB services:– Set of Best Practices (short summaries of key aspects of OB
hemorrhage)– Checklist for managing OB hemorrhage– Flow-Chart and Table Chart Summaries of approach– Implementation tools such as sample policies, procedures,
charting examples, implementation hints• All resources on-line at:
www.cmqcc.org/ob_hemorrhage
CMQCC Hemorrhage Task Force:
Source: CMQCC California Maternal Quality Care Collaborative

10/15/2015
4
• Coagulopathy persisted at ICU admissionPre-ICU resuscitation:
9 ± 1 L crystalloid12 ± 1 units PRBC5 ± 0.4 units FFP
FFP was not given until after 6 units PRBCs• In the ICU during resuscitation, patients received 10 ± 1 units FFP for coagulopathy; the ratio of FFP:PRBC was 1:1. Mean INR < 1.4 within 8 hours
� Volume restoration is accomplished by using thawed plasma as a primary resuscitation fluid in at least a 1:1 or 1:2 ratio with PRBCs� Crystalloid is minimized and serves mainly as a carrier� The blood bank activates the massive transfusion protocol and
deliver 6 units of plasma, 6 units of PRBCs, 6 packs of platelets, and 10 units of cryoprecipitate � Recombinant FVIIa is occasionally used
� “Using the damage control resuscitation approach, the lack of intraoperative coagulopathic bleeding has been remarkable, allowing surgeons to focus on surgical bleeding.”
� “Patients treated in this fashion almost always arrive in the ICU warm, euvolemic, and nonacidotic, with a normal INR and minimal edema.”

10/15/2015
5
� “In the majority of patients the abnormalities of the lethal triad are absent.”
� “These patients appear to be easily ventilated and more quickly extubated than patients with similar blood loss treated with the standard crystalloid resuscitation volumes and blood component ratios.”
Borgman et al. J Trauma 2007; 63:805-13
2003-2005 Retrospective Data From Iraq War
Volume 50, February 2010 TRANSFUSION
Plasma:RBC product transfusion ratios effect on patient survival
Survival versus ratio. (Dark Gray ) 24-hour survival; (Light Gray ) 30-day survivalVolume 50, February 2010 TRANSFUSION
PLT:RBC product transfusion ratios effect on patient survival
Survival versus ratio. (Dark Gray ) 24-hour survival; (Light Gray ) 30-day survival

10/15/2015
6
Principles to Reducing Maternal Hemorrhage
• Screen and identify patients at high risk• Active management of 3rd stage• Ongoing quantification of blood loss• Ongoing evaluation of patient’s vital signs• Sequential use of medications & procedures• Timely request for blood products • Massive transfusion protocol and team• Periodic hemorrhage drills and simulations
Adapted from CMQCC California Maternal Quality Care Collaborative – OB Hemorrhage Task Force 22Graphic Source: CMQCC California Maternal Quality Care Collaborative
Blood Loss:1000-1500 ml
Stage 2
SequentiallyAdvance through
Medications &Procedures
Pre-Admission
Time of admission
Identify patients with special consideration:Placenta previa/accreta, Bleeding disorder, or those who decline blood products
Follow appropriate workups, planning, preparing
of resources, counseling and notification
Screen All Admissions for hemorrhage risk:Low Risk, Medium Risk and High Risk
Low Risk: Draw blood and hold specimenMedium Risk: Type & Screen, Review Hemorrhage ProtocolHigh Risk: Type & Crossmatch 2 Units PRBCs; Review Hemorrhage Protocol
All women receive active management of 3rd stageOxytocin IV infusion or 10 Units IM, 10-40 U infusion
Standard Postpartum Management
Fundal Massage
Vaginal Birth:Bimanual Fundal MassageRetained POC: Dilation and CurettageLower segment/Implantation site/Atony: Intrauterine BalloonLaceration/Hematoma: Packing, Repair as RequiredConsider IR (if available & adequate experience)
Cesarean Birth:Continued Atony: B-Lynch Suture/Intrauterine BalloonContinued Hemorrhage: Uterine Artery Ligation
To OR (if not there); Activate Massive Hemorrhage Protocol
Mobilize Massive Hemorrhage Team TRANSFUSE AGGRESSIVELY RBC:FFP:Plts 6:4:1 or 4:4:1
IncreasedPostpartum Surveillance
Definitive SurgeryHysterectomy
Conservative SurgeryB-Lynch Suture/Intrauterine BalloonUterine Artery LigationHypogastric Ligation (experienced surgeon only)Consider IR (if available & adequate experience)
Fertility
Strongly
Desired
Consider ICUCare; Increased
Postpartum Surveillance
Verify Type & Screen on prenatal record;
if positive antibody screen on prenatal or current labs (except low level anti-D from Rhogam), Type & Crossmatch 2
Units PBRCs
CALL FOR EXTRA HELPGive Meds: Hemabate 250 mcg IM -or-
Misoprostol 600-800 SL or PO
Cumulative Blood Loss>500 ml Vag; >1000 ml CS>15% Vital Sign change -or-
HR ≥ 110, BP ≤ 85/45
O2 Sat <95%, Clinical Sx
Ongoing Evaluation:
Quantification of blood loss and
vital signs
Unresponsive Coagulopathy:After 10 Units PBRCs and full
coagulation factor replacement,may consider rFactor VIIa
HEMORRHAGE CONTINUES
Blood Loss:>1500 ml
Stage 3
Activate Massive
Hemorrhage Protocol
Blood Loss: >500 ml Vaginal
>1000 ml CS
Stage 1Activate
Hemorrhage Protocol
NO
Stage 0All Births
Transfuse 2 Units PRBCs per clinical signs
Do not wait for lab valuesConsider thawing 2 Units FFP
YES
YES NO
Ong
oing
Cum
ulat
ive
Blo
od L
oss
Eva
luat
ion
Cumulative Blood Loss>1500 ml, 2 Units Given,
Vital Signs Unstable
YESIncrease IV Oxytocin RateMethergine 0.2 mg IM (if not hypertensive)Vigorous Fundal massage; Empty Bladder; Keep WarmAdminister O2 to maintain Sat >95%Rule out retained POC, laceration or hematomaOrder Type & Crossmatch 2 Units PRBCs if not already done
Activate Hemorrhage ProtocolCALL FOR EXTRA HELP
Continued heavy bleeding
Increased Postpartum Surveillance
NO
NO
CONTROLLED
INCREASED BLEEDING
California Maternal Quality Care Collaborative (CMQCC), Hemorrhage Taskforce (2009) visit: www.CMQCC.org for detailsThis project was supported by funds received from the State of California Department of Public Health, Center for Family Health; Maternal, Child and Adolescent Health Division
Obstetric Emergency Management Plan: Flow Chart Format Release 2.0 7/9/2014
23Graphic Source: CMQCC California Maternal Quality Care Collaborative
Blood Loss:1000-1500 ml
Stage 2
SequentiallyAdvance through
Medications &Procedures
Pre-Admission
Time of admission
Identify patients with special consideration:Placenta previa/accreta, Bleeding disorder, or those who decline blood products
Follow appropriate workups, planning, preparing
of resources, counseling and notification
Screen All Admissions for hemorrhage risk:Low Risk, Medium Risk and High Risk
Low Risk: Draw blood and hold specimenMedium Risk: Type & Screen, Review Hemorrhage ProtocolHigh Risk: Type & Crossmatch 2 Units PRBCs; Review Hemorrhage Protocol
All women receive active management of 3rd stageOxytocin IV infusion or 10 Units IM, 10-40 U infusion
Standard Postpartum Management
Fundal Massage
Vaginal Birth:Bimanual Fundal MassageRetained POC: Dilation and CurettageLower segment/Implantation site/Atony: Intrauterine BalloonLaceration/Hematoma: Packing, Repair as RequiredConsider IR (if available & adequate experience)
Cesarean Birth:Continued Atony: B-Lynch Suture/Intrauterine BalloonContinued Hemorrhage: Uterine Artery Ligation
To OR (if not there); Activate Massive Hemorrhage Protocol
Mobilize Massive Hemorrhage Team TRANSFUSE AGGRESSIVELY RBC:FFP:Plts 6:4:1 or 4:4:1
IncreasedPostpartum Surveillance
Definitive SurgeryHysterectomy
Conservative SurgeryB-Lynch Suture/Intrauterine BalloonUterine Artery LigationHypogastric Ligation (experienced surgeon only)Consider IR (if available & adequate experience)
Fertility
Strongly
Desired
Consider ICUCare; Increased
Postpartum Surveillance
Verify Type & Screen on prenatal record;
if positive antibody screen on prenatal or current labs (except low level anti-D from Rhogam), Type & Crossmatch 2
Units PBRCs
CALL FOR EXTRA HELPGive Meds: Hemabate 250 mcg IM -or-
Misoprostol 600-800 SL or PO
Cumulative Blood Loss>500 ml Vag; >1000 ml CS>15% Vital Sign change -or-
HR ≥ 110, BP ≤ 85/45
O2 Sat <95%, Clinical Sx
Ongoing Evaluation:
Quantification of blood loss and
vital signs
Unresponsive Coagulopathy:After 10 Units PBRCs and full
coagulation factor replacement,may consider rFactor VIIa
HEMORRHAGE CONTINUES
Blood Loss:>1500 ml
Stage 3
Activate Massive
Hemorrhage Protocol
Blood Loss: >500 ml Vaginal
>1000 ml CS
Stage 1Activate
Hemorrhage Protocol
NO
Stage 0All Births
Transfuse 2 Units PRBCs per clinical signs
Do not wait for lab valuesConsider thawing 2 Units FFP
YES
YES NO
Ong
oing
Cum
ulat
ive
Blo
od L
oss
Eva
luat
ion
Cumulative Blood Loss>1500 ml, 2 Units Given,
Vital Signs Unstable
YESIncrease IV Oxytocin RateMethergine 0.2 mg IM (if not hypertensive)Vigorous Fundal massage; Empty Bladder; Keep WarmAdminister O2 to maintain Sat >95%Rule out retained POC, laceration or hematomaOrder Type & Crossmatch 2 Units PRBCs if not already done
Activate Hemorrhage ProtocolCALL FOR EXTRA HELP
Continued heavy bleeding
Increased Postpartum Surveillance
NO
NO
CONTROLLED
INCREASED BLEEDING
California Maternal Quality Care Collaborative (CMQCC), Hemorrhage Taskforce (2009) visit: www.CMQCC.org for detailsThis project was supported by funds received from the State of California Department of Public Health, Center for Family Health; Maternal, Child and Adolescent Health Division
Obstetric Emergency Management Plan: Flow Chart Format Release 2.0 7/9/2014
Graphic Source: CMQCC California Maternal Quality Care Collaborative
CMQCC Obstetric Care Summary
10/15/2015
7
Holcomb et al. JAMA 2015; 313: 471-82
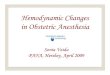
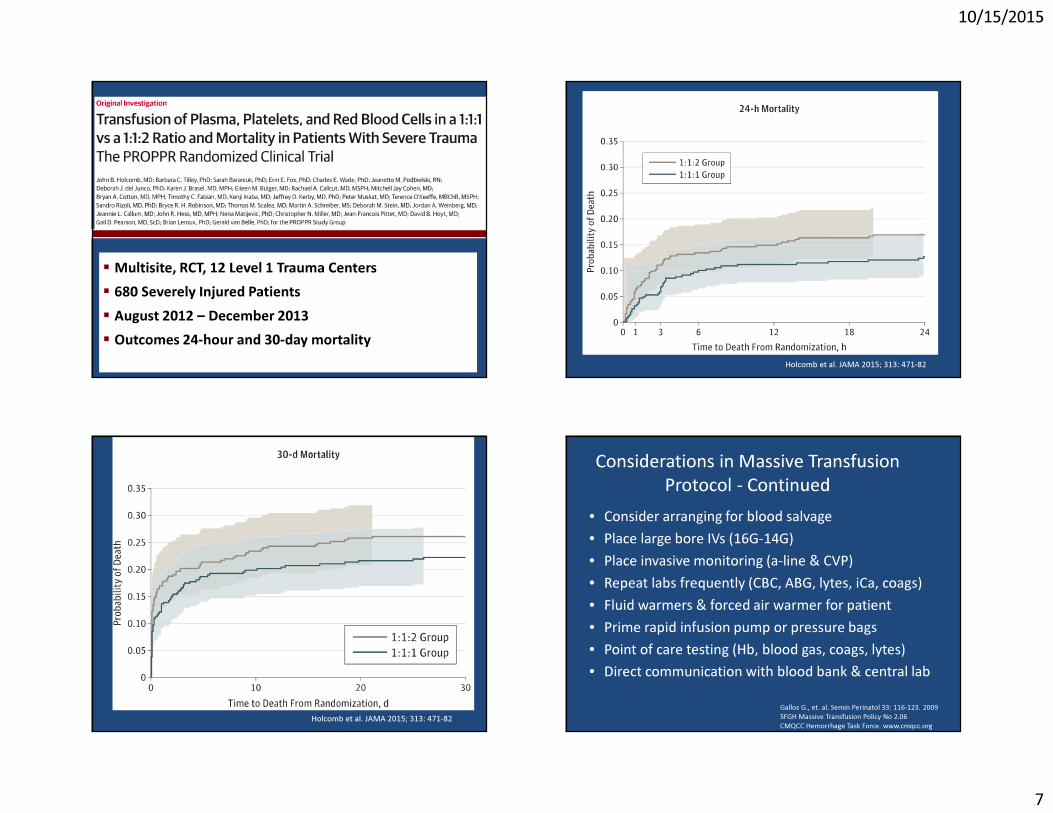
� Multisite, RCT, 12 Level 1 Trauma Centers � 680 Severely Injured Patients� August 2012 – December 2013� Outcomes 24-hour and 30-day mortality
Holcomb et al. JAMA 2015; 313: 471-82
Holcomb et al. JAMA 2015; 313: 471-82
Considerations in Massive Transfusion Protocol - Continued
• Consider arranging for blood salvage• Place large bore IVs (16G-14G)• Place invasive monitoring (a-line & CVP)• Repeat labs frequently (CBC, ABG, lytes, iCa, coags)• Fluid warmers & forced air warmer for patient• Prime rapid infusion pump or pressure bags• Point of care testing (Hb, blood gas, coags, lytes)• Direct communication with blood bank & central lab
Gallos G., et. al. Semin Perinatol 33: 116-123. 2009SFGH Massive Transfusion Policy No 2.06CMQCC Hemorrhage Task Force. www.cmqcc.org

10/15/2015
8
• Prepare for general anesthesia• Vasopressors immediately available • All uterotonics immediately available• Supply of calcium chloride to prevent low ionized
calcium levels from rapid transfusion• Foley to measure urine & SCDs• Reserve ICU bed
Gallos G., et. al. Semin Perinatol 33: 116-123. 2009SFGH Massive Transfusion Policy No. 2.06CMQCC Hemorrhage Task Force. www.cmqcc.org
Considerations in Massive Transfusion Protocol - Continued
• Request additional blood products as needed in “packs” of correct ratio (Prbcs:FFP:Plts)
• Consider cryoprecipitate (Fibrinogen < 100 mg/dL)• Consider factor VIIa (off-label hemostatic use)
– Only after approximately 10 units prbcs and factor replacement• Person for recording/tallying blood products & EBL• Bring “Code Cart” into OR• Plan for Blood Bank to prioritize Transfusion labs• Make time to debrief after event with all disciplines
Gallos G., et. al. Semin Perinatol 33: 116-123. 2009; SFGH Massive Transfusion Policy No. 2.06; CMQCC Hemorrhage Task Force. www.cmqcc.org
Considerations in Massive Transfusion Protocol - Continued
Consideration of Cell Salvage
• Cell salvage in obstetrics should be considered in cases at risk for severe hemorrhage or for individuals in whom allogenic blood can not be used…- Placenta accreta / increta / percreta- Massive uterine fibroids- Jehovah’s Witnesses- Difficult cross-matching
Opinion Statements• “If the diagnosis or strong suspicion of placenta accreta is
formed before delivery…Cell saver technology should be considered if available as well as the appropriate location and timing for delivery…”
(American College of Obstetricians and Gynecologists (ACOG), Practice Bulletin, No. 76, October 2006, Postpartum Hemorrhage)

10/15/2015
9
Opinion Statements• “Cell salvage is recommended for women in whom an
intraoperative blood loss of more than 1500 ml is anticipated. Cell salvage should only be used by healthcare teams who use it regularly and have the necessary expertise and experience. Consent should be obtained and its use in obstetric patients should be subject to audit and monitoring.””
(RCOG Guideline No. 27, October 2005 – Placenta Previa and Placenta Accreta)
TOOLS TO HELP? SOME NEW AND SOME OLD
Role of Interventional Radiology
Uterine Artery Catheterization
Pledgets
Slurry
Coils
n-Butyl Cyanoacrylate
Embolization Agents

10/15/2015
10
IR for AtonyClinical Success
Study Year n Success %Ornan D et al.Obstet Gynecol
2003 28 96%
Boulleret C et al.CVIR
2004 35 100%
Zwart JJ et al.Am J Obstet Gynecol
2009 114 85%
Kirby JM et al.JVIR
2009 43 79%
Obstet Gynecol 2009;113:992-9
• 100 patients over 13 years
• Outcomes– Clinical success in 89 patients (89%)– 7 of the 11 patients (64%) underwent hysterectomy– Buttock necrosis (1%)
– Puncture site hematoma (1%)
• Conclusion– Patients who failed embolization had higher rate of estimated
blood loss (more than 1,500 mL) and higher transfusion requirements (more than 5 units of PRBCs)
• 28 studies were included in the systematic review
• 460 out of 503 (91.45%) women resumed menstruation
• 168 women desired another pregnancy– 126 (75%) achieved conception following embolization
• Conclusion: Uterine-sparing radiological techniques do not appear to adversely affect the menstrual and fertility outcomes in most women; however, the number and quality of the available evidence is of concern
BJOG 2014;121:382-8
Interventional RadiologyInvasive Placenta
• Different disease process than uterine atony
• Requires a multidisciplinary team– Maternal fetal medicine (OB team)– Surgical gynecology (gyn onc)– Interventional radiology
– Diagnostic radiology (antenatal MRI)– Scheduled deliveries– Use of multidisciplinary team is associated with a significant
reduction in morbidity (p=0.005)
• Need randomized clinical trials/registry dataJ Obstet Gynaecol Can 2013; 35:417–425

10/15/2015
11
rFVIIaCost: ~ $5000.00
•A review of the FDA’s Reporting System from 1999 to 2004•A total of 431 AE reports for rFVIIa were found, of which 168 reports described 185 thromboembolic events•Unlabeled indications accounted for 151 of the reports, most with active bleeding (n=115)•In 36 (72%) of 50 reported deaths, the probable cause of death was the thromboembolic event•Conclusion: RCTs are needed to establish the safety and efficacy of rFVIIa in patients without hemophilia
� A 2008 review noted 118 cases of massive postpartum hemorrhage treated with rFVIIa.�Median dose was 71.6 mcg/kg� rFVIIa was reported to be effective in stopping or reducing bleeding in 90% of reported cases� Caution in interpreting results as they are from uncontrolled studies� RCTs needed to determine efficacy, dose, & safety
Review of Factor VIIa in Severe Obstetric PPH
Franchini M., et. al., Semin Thromb Hemost 2008; 34:104-112
Butwick et al. Curr Opin Anesthesiol 2015; 28;275-84
�Fibrinogen

10/15/2015
12
Charbit et al. J Thromb Haemost 2007; 5:266-273 Charbit et al. J Thromb Haemost 2007; 5:266-273
ThromboelastographyROTEM- Thromboelastometry (Germany)
ROTEM

10/15/2015
13
Butwick et al. Curr Opin Anesthesiol 2015; 28;275-84
PROTOCOL SUMMARY
FULL TITLE OF STUDY: Tranexamic acid for the treatment of postpartum haemorrhage: An international, randomised, double blind, placebo controlled trial
SHORT TITLE: WORLD MATERNAL ANTIFIBRINOLYTIC TRIAL
TRIAL ACRONYM: THE WOMAN TRIAL
PROTOCOL NUMBER: ISRCTN76912190
EUDRACT NUMBER: 2008-008441-38 CLINICALTRIALS.GOV ID: NCT00872469

10/15/2015
14
Summary• Recognition and Preparedness• Multidisciplinary Team • Good Communication and Team Work• Massive Transfusion Protocols• Role of Cell Salvage in Predictable
Hemorrhage• Potential Role of Devices and Pharmacologic
Interventions