Embed Size (px)
Citation preview

TOPIC: NEWER TREATMENT IN TOPIC: NEWER TREATMENT IN BREAST CANCERBREAST CANCER
BYChaitra.t.m9th termBangalore medical college

TOPIC: NEWER TOPIC: NEWER TREATMENT IN BREAST TREATMENT IN BREAST
CANCERCANCER
BYChaitra.t.m9th termBangalore medical college
Breast cancerBreast cancerChance of developing This at somePoint of womensLife is 13% whereas in man is <2%.
2nd leading cause of death

TYPESTYPESDuctular(85%) Lobular(1
5%)

• AGE - MORE THAN 40yrs
• GENDER- FEMALE
• GEOGRAPHY- WESTERN COUNTRIES
• ENDOCRINE- NULLIPAROUS
• NO CHILD UPTO 30yrs
• HARMONE REPLACEMENT THERAPY
• NO BREAST FEEDING
• HIGH FAT DIET
• OCPs
• OBESITY • GENETIC
RISK FACTORS
MYTHS ABOUT BREAST MYTHS ABOUT BREAST CANCERCANCER
• AntiperspirentsAntiperspirents
• Induced abortionInduced abortion
• Breast implantsBreast implants
• Environmental pollutionEnvironmental pollution
• Night shift workingNight shift working
Thought to be carcinogens
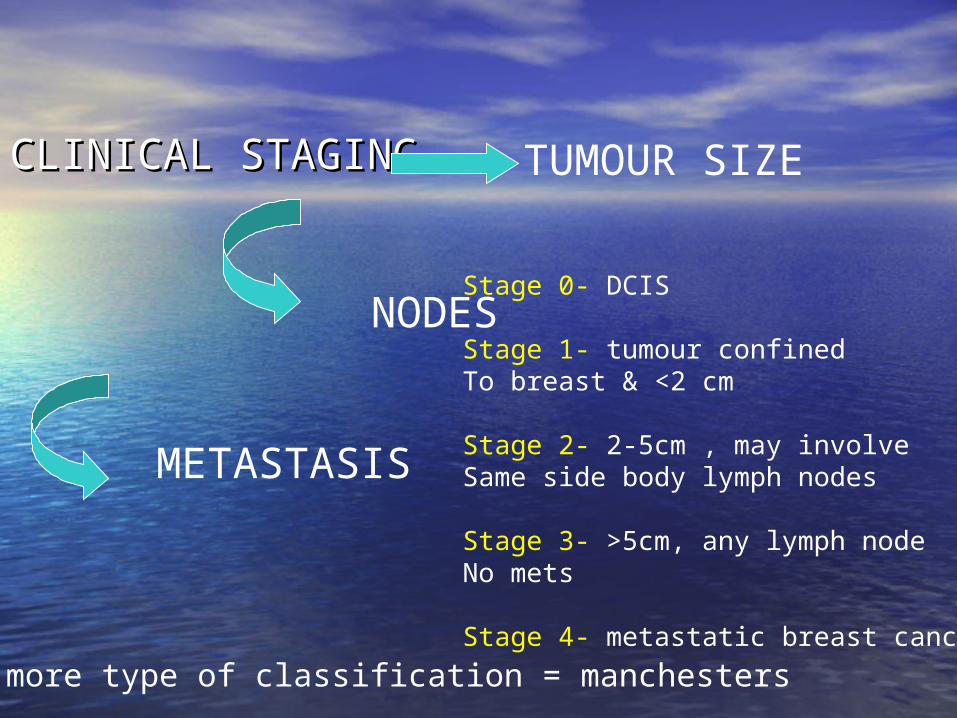
CLINICAL STAGINGCLINICAL STAGING
TUMOUR SIZE
METASTASIS
NODESStage 0- DCIS
Stage 1- tumour confinedTo breast & <2 cm
Stage 2- 2-5cm , may involve Same side body lymph nodes
Stage 3- >5cm, any lymph nodeNo mets
Stage 4- metastatic breast cancer
One more type of classification = manchesters

Whats new in Breast cancer
treatment
PATIENT INVOLVEMENT•Health education
TECHNOLOGY•Diagnostic•Treatment
POST OP•Better arm function•Cosmesis•Quality of life
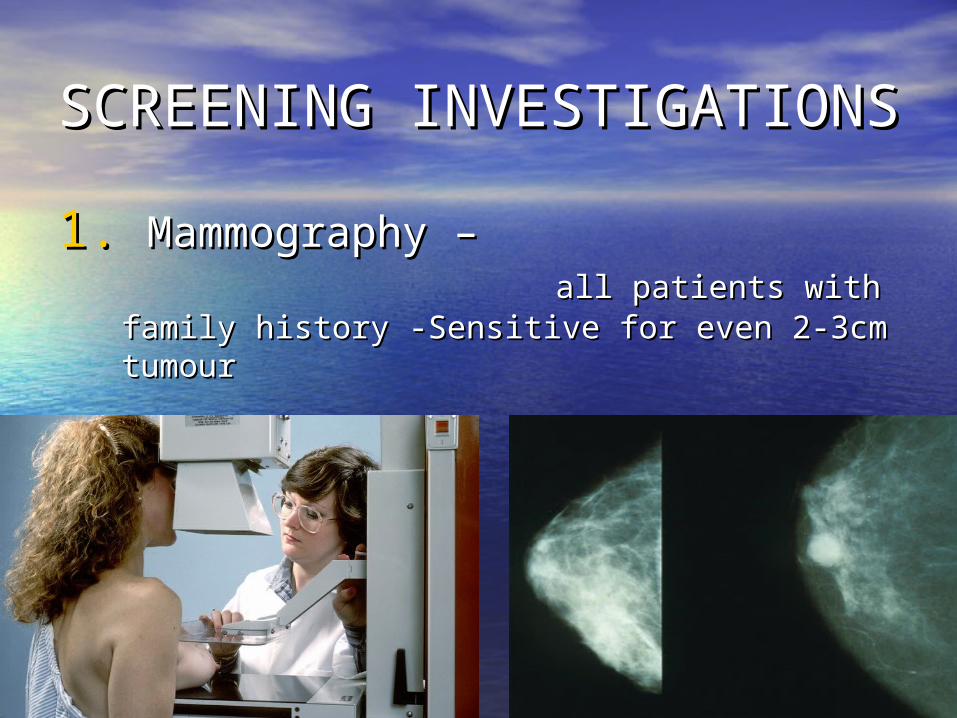
SCREENING SCREENING INVESTIGATIONSINVESTIGATIONS
1.1. Mammography – Mammography – all patients with family history -Sensitive for all patients with family history -Sensitive for even 2-3cm tumoureven 2-3cm tumour

2. Clinical breast examination
3. Breast self examination
DIAGNOSTIC INVESTIGATIONSDIAGNOSTIC INVESTIGATIONS
1.1. DiagnosticDiagnostic mammography mammography2.2. UltrasonographyUltrasonography3.3. Biopsy Biopsy - F N A C - F N A C - core biopsy - core biopsy
- surgical biopsy-lumpectomy/ - surgical biopsy-lumpectomy/ stereotactic stereotactic localisation localisation (nonpalpable tumours)(nonpalpable tumours)
4.4. Scintimammography ( Scintimammography (99mm Tc- Sestamibi99mm Tc- Sestamibi))5.5. MRI (localisation ) MRI (localisation )6.6. CT CT7.7. PET(mets work up & effective chemotherapy) PET(mets work up & effective chemotherapy)
METS WORK UPCXRLFTLIVER USGIsotope bone scan
SURGERYSURGERYHalsteds –radical mastectomy
Patey’s –modified radical mastectomy
BREAST CONSERVATIVE SURGERY= (wide local excision-margin +/-) /QUART{quadrantectomy+axillary dissection+Radiotherapy}
newNo lymphedema/no limb dysfunction
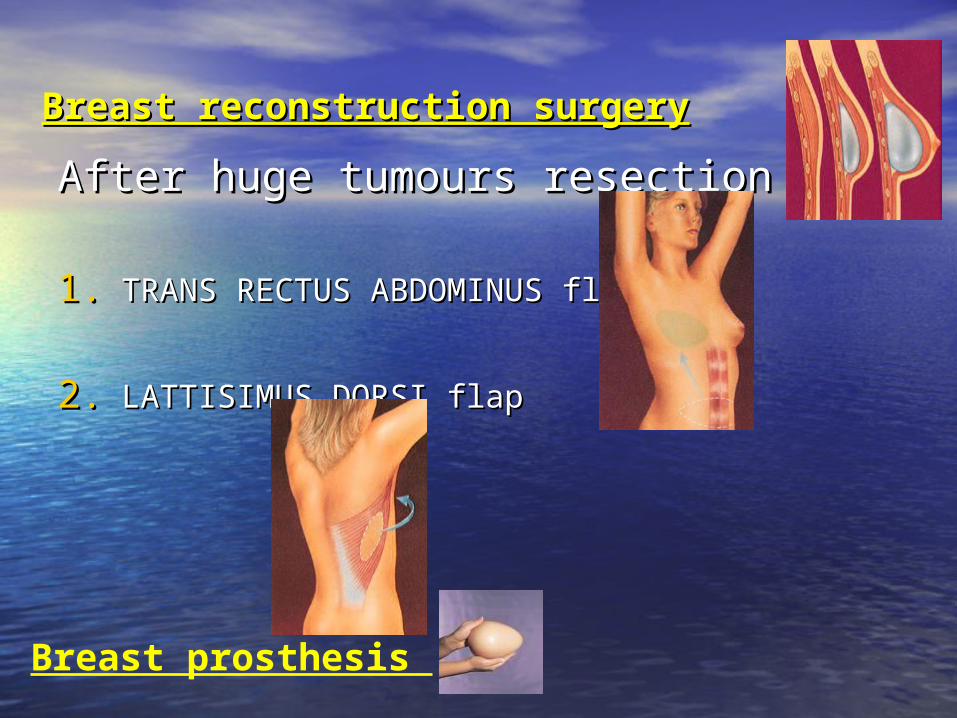
Breast reconstruction surgeryBreast reconstruction surgery
After huge tumours resectionAfter huge tumours resection
1.1. TRANS RECTUS ABDOMINUS flapTRANS RECTUS ABDOMINUS flap
2.2. LATTISIMUS DORSI flapLATTISIMUS DORSI flap
Breast prosthesis

ADJUVANT THERAPYADJUVANT THERAPY==(Chemotherapy/harmonotherapy/radiotherapy/immunotherapy)
.RADIOTHERAPY- 1. to tumour bed only
2. peroperative
3. palliative
ChemotherapyChemotherapy- - (given in 6 cycles at (given in 6 cycles at an interval of 28 days with heamatological an interval of 28 days with heamatological monitoring)monitoring)
• conventional CMF regime conventional CMF regime
• Newer less toxic drugs Newer less toxic drugs
1.1.anthracyclines-anthracyclines-adriamycin/cyciophadriamycin/cyciophosphamideosphamide
2.2.taxanestaxanes-paclitaxel/docetaxel-paclitaxel/docetaxelIndications-•Lymph node positive tumour•Poor prognostic lymph node negative•As palliative therapy•As neoadjuvant therapy
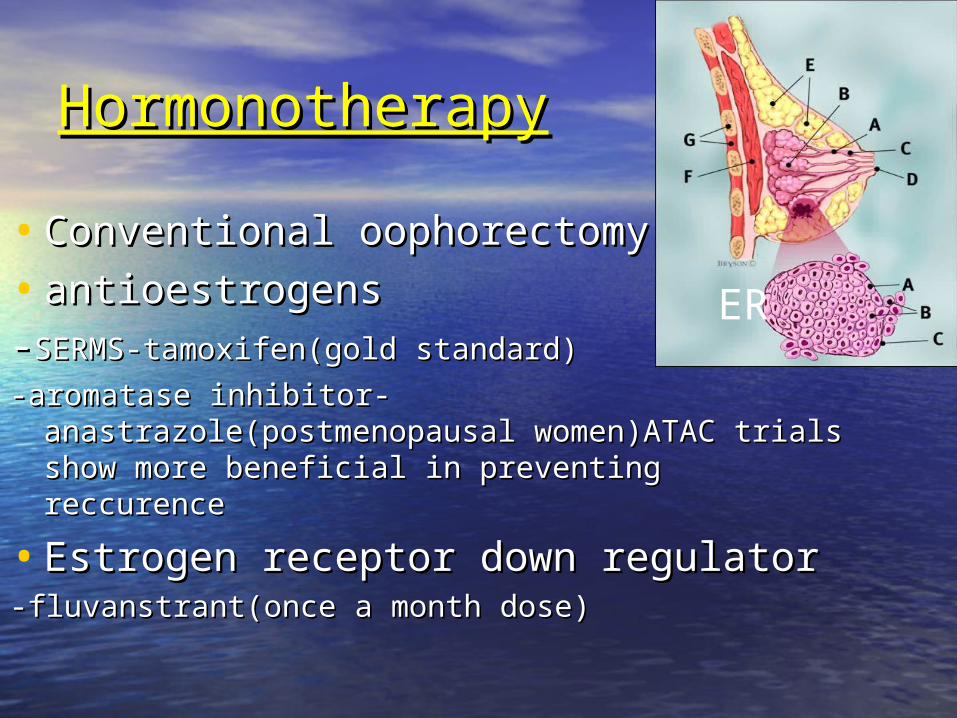
HormonotherapyHormonotherapy
• Conventional oophorectomyConventional oophorectomy
• antioestrogensantioestrogens--SERMS-tamoxifen(gold standard)SERMS-tamoxifen(gold standard)
-aromatase inhibitor-anastrazole(postmenopausal -aromatase inhibitor-anastrazole(postmenopausal women)ATAC trials show more beneficial in women)ATAC trials show more beneficial in preventing reccurencepreventing reccurence
• Estrogen receptor down regulatorEstrogen receptor down regulator-fluvanstrant(once a month dose)-fluvanstrant(once a month dose)
ERER
• HER2 receptor positive cancer (25%)do HER2 receptor positive cancer (25%)do respond to herceptinrespond to herceptin
(herceptin trial shows 50% relapse (herceptin trial shows 50% relapse prevention)prevention)
• FDA approved FDA approved avastinavastin is a trial drug which is a trial drug which acts on VEGF preventing tumour acts on VEGF preventing tumour progression progression
ImmunotherapyImmunotherapy
• Make tumour cells to be recognised Make tumour cells to be recognised as foreignas foreign
• Boost up host immunity to destroy Boost up host immunity to destroy themthem
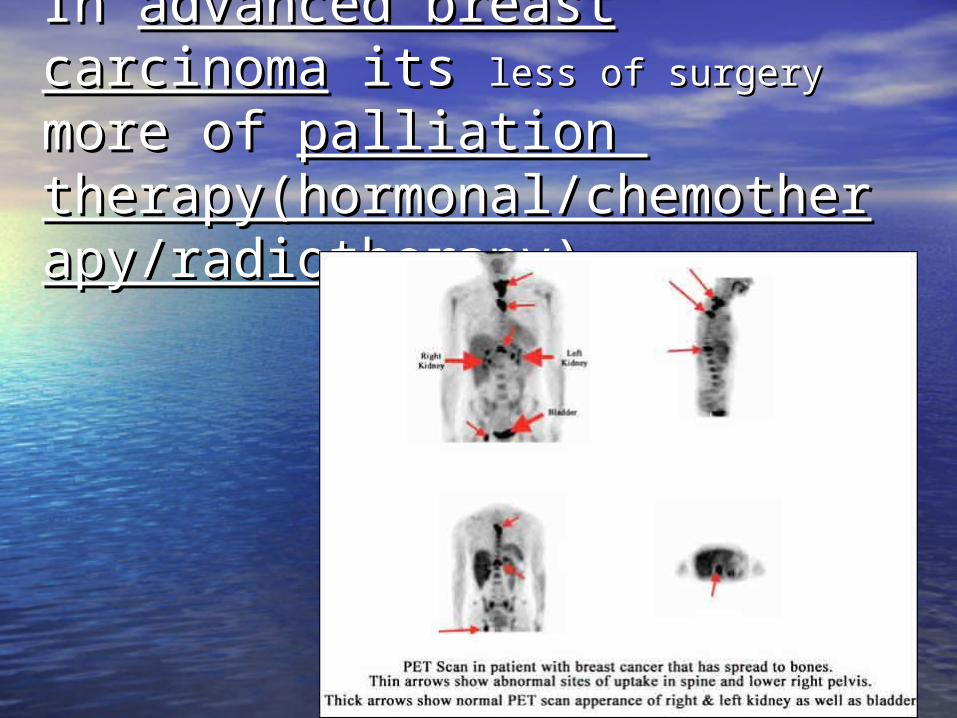
In In advanced breast carcinomaadvanced breast carcinoma its its less of surgeryless of surgery more of more of palliation palliation
therapy(hormonal/chemotheratherapy(hormonal/chemotherapy/radiotherapypy/radiotherapy))

Australian couple who underwentfertility tretment following detection of massive cancer running in family.

Complementary medicineComplementary medicine
• MeditationMeditation
• AcupunctureAcupuncture
• NutritionNutrition
• Vitamin tabletsVitamin tablets

"The smaller the tumor, the greater your options. So if you feel something you're concerned about,
you need to get in and get it taken care of. That's a key thing. Because a lot
of people have this fear that they're going to lose their breast, and it's
just not true anymore."
Take home Take home MESSAGEMESSAGE
• Patient education regarding BSEPatient education regarding BSE (breast self examination) is the key (breast self examination) is the key point in our country.point in our country.
• With numerous options in treatment With numerous options in treatment of carcinoma breast is now a realistic of carcinoma breast is now a realistic challenge to we doctors and we got challenge to we doctors and we got to to individualise the treatmentindividualise the treatment
THANK YOU





























