Embed Size (px)
Citation preview
Medical Physics
The Physics of the Lungs and Breathing
- Introduction
- How the blood and lungs interact
- Measurement of lung volume
- Pressure-airflow-volume relationships of the lungs
- The breathing mechanism
- Compliance &Airways resistance
- Work of the breathing
- Physics of some common lung diseases
References: 1- Medical Physics textbook by Cameron
2- Physics in Biology and Medicine, Third Edition by P.Davidovits
3- Physics of the Human Body, by Irving P. Herman
Objectives
To what extend human body is similar to a machine ?
• Human body must have an energy source in both phases, electrical and mechanical
• Human body consists of billions of engines (Cells)• Cardiovascular system acts as a transport ways between these engines
to supply them with fuel and exclude wastes
Fuel cycle within the machine : 1- Food is digested in the digestive system
2 - Digested food is combined with oxygen (O2) 3- Oxygenated digested food is immersed to the cells and combustion takes place to produce fuel
Why 80 % of air is nitrogen not oxygen ?
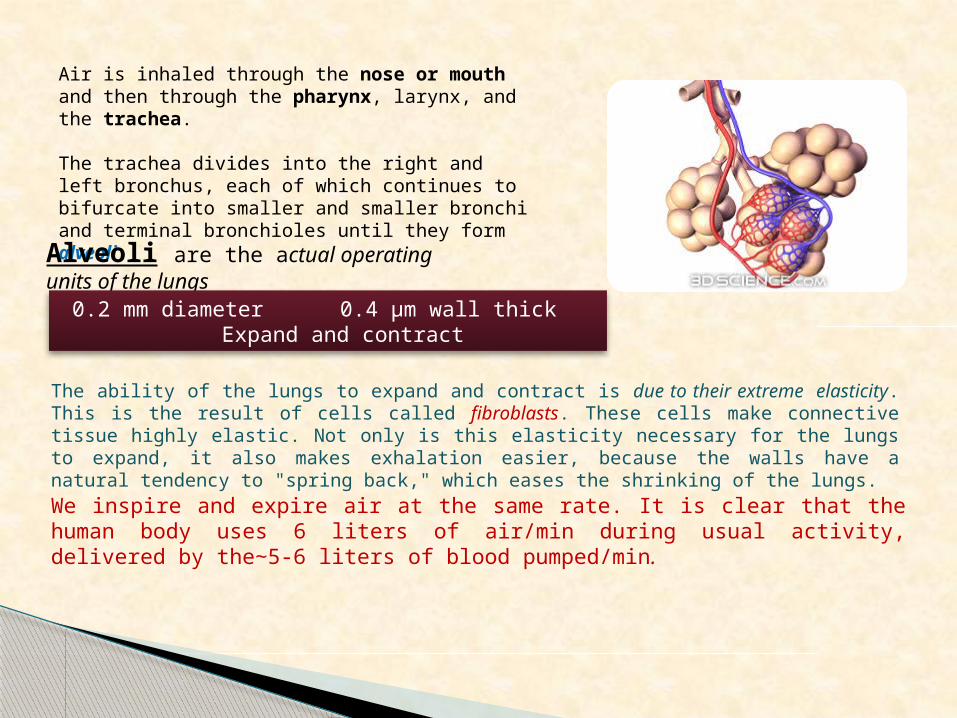
Air is inhaled through the nose or mouth and then through the pharynx, larynx, and the trachea.
The trachea divides into the right and left bronchus, each of which continues to bifurcate into smaller and smaller bronchi and terminal bronchioles until they form alveoliAlveoli are the actual operating units of the lungs
0.2 mm diameter 0.4 µm wall thick Expand and contract
The ability of the lungs to expand and contract is due to their extreme elasticity. This is the result of cells called fibroblasts. These cells make connective tissue highly elastic. Not only is this elasticity necessary for the lungs to expand, it also makes exhalation easier, because the walls have a natural tendency to "spring back," which eases the shrinking of the lungs.
We inspire and expire air at the same rate. It is clear that the human body uses 6 liters of air/min during usual activity, delivered by the 5-6 liters of blood pumped/min∼ .
How The Blood and Lungs InteractThe primary purpose of breathing is to bring fresh oxygen (O2 ) to the blood in the lungs and to
dispose carbon dioxide (CO2). Blood is pumped from the heart to the lungs under relatively low
pressure (20 mm Hg) which is about 15% of the pressure of the main body circulation. (Why ?)
About one liter of the blood is in the lungs at any time but only 70 ml of that blood is in
capillaries of the lungs getting O2. (Why ?)
The surface area between air and blood in the lungs is about 80 (m2), if the 70 (ml) of blood in
the pulmonary capillaries were spread (distributed) over the total surface area, will result in the
formation of a layer of the blood about 1 μm thickness.
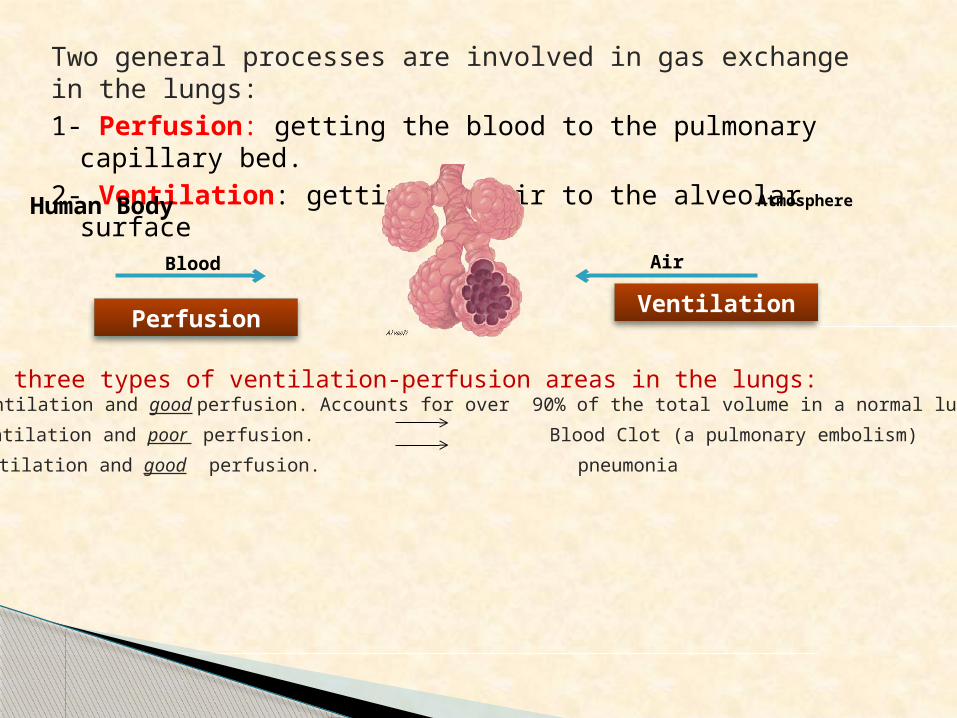
Two general processes are involved in gas exchange in the lungs:
1- Perfusion: getting the blood to the pulmonary capillary bed.
2- Ventilation: getting the air to the alveolar surface
Atmosphere
Air
Human Body
Blood
VentilationPerfusion
There are three types of ventilation-perfusion areas in the lungs:1- Good ventilation and good perfusion. Accounts for over 90% of the total volume in a normal lung.
2- Good ventilation and poor perfusion. Blood Clot (a pulmonary embolism)
3- Poor ventilation and good perfusion. pneumonia
Physical laws of diffusionDalton’s law: “If you have a mixture of several gases, each gas makes its own
contribution to the total pressure as if it was all alone.
Charles' Law: It states that temperature is proportional to pressure
Henry’s law: law of solubility of gas. It states that “At a constant temperature, the number of gas molecules dissolved in a given type and volume of liquid is directly proportional to the partial pressure of that gas”
p = kH cwhere p is the partial pressure of the solute in the gas above the solution, c is the concentration of the
solute and kH is a constant with the dimensions of pressure divided by concentration.
Fick's Law: Gas transfer through alveoli membrane is directly proportional to membrane surface area (A), partial pressure across the membrane (P) and inversely proportional to thickness of the alveoli membrane (L). [i.e., Gas transfer α A P/L].
Gas transfer velocity α
Law of Laplace: Alveoli are similar to interconnected bubbles. Inside the alveoli the pressure is (Pin) and outside them, the pressure is (Pout) with (difference in pressure) [ΔP], hence ΔP = Pin−Pout and they have a radius r.
The law of Laplace for a sphere is:
ΔP = Pin − Pout = 2T/r
Where, T is the surface tension in the sphere walls (The main source of this tension in the alveoli is not within the walls but on the surfaces).
Alveoli are lined with a liquid called surfactant, therefore they have tendency to get smaller due to surface tension of the surfactant. Surfactant is a unique liquid because it is unlike all liquids, it has not a constant surface tension. Surface tension of the surfactant is mainly depends on the alveoli surface area.
Bubbles from liquids of low surface tension last longer than those of higher surface tension, Why?
Because liquids with higher surface tension form bubbles with high pressure inside so rupture of these bubbles are easier.
Receiving various signals from the nervous system, the diaphragmatic muscles contract and the diaphragm moves downward. As the diaphragm depresses, it creates vacuum in the lungs and air rushes into the lungs to fill it. As the diaphragm relaxes, it pushes the molecules closer together, increasing the internal pressure in the lungs. The air flows from the lungs into the lower pressure outside the body.
Inhalation: Diaphragm contracts and moves downwards. Lung volume gets larger, creating a negative pressure difference Pressure inside the lung becomes less than outside Air rushes in
Exhalation: Diaphragm relaxes and rises up Lung volume decreases, creating a positive pressure difference Pressure inside the lung becomes more than outside Air rushes out
Action of the breathing
Other lung functions :
(1) Keeping the pH (acidity) of the blood constant. (2) Lungs are involved in heat exchange and fluid balance in the body by warming and
moisturizing the air we inspire. (3) Voice production, voice is produced by a controlled outflow of air from the lungs, a
person inhales rapidly and more deeply before speaking in order to have more time to produce voice sounds.
Exercising
Resting
Time
Oxygen Partial
Pressure (PO2)
mmHg
40
60
120
160
100
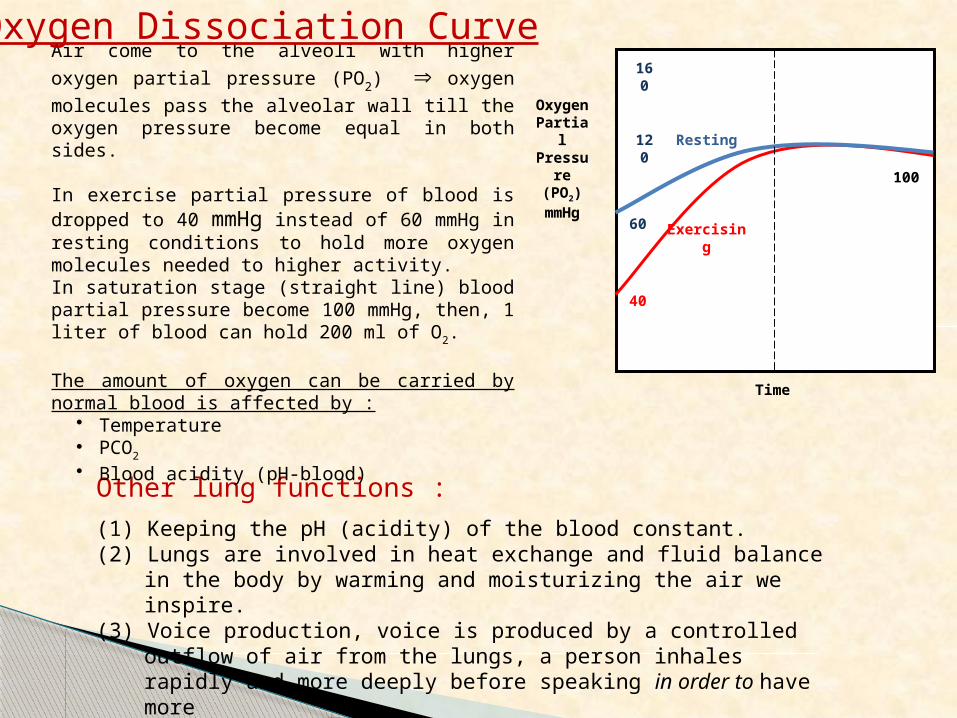
Air come to the alveoli with higher oxygen partial pressure (PO2) oxygen molecules pass the alveolar wall till the oxygen pressure become equal in both sides.
In exercise partial pressure of blood is dropped to 40 mmHg instead of 60 mmHg in resting conditions to hold more oxygen molecules needed to higher activity.In saturation stage (straight line) blood partial pressure become 100 mmHg, then, 1 liter of blood can hold 200 ml of O2.
The amount of oxygen can be carried by normal blood is affected by :
• Temperature• PCO2
• Blood acidity (pH-blood)
Oxygen Dissociation Curve
Carbon monoxide poisoningCO has a very secure attachment with the same sites that oxygen binds with in the blood molecules. This combination is 250 times higher than the oxygen so it blocks them.
CO victims are placed in oxygen chamber to enhance their PO2 with 3 atm that enhance the PO2 by a factor 15. This treatment is not long tern treatment because higher O2 is toxic.
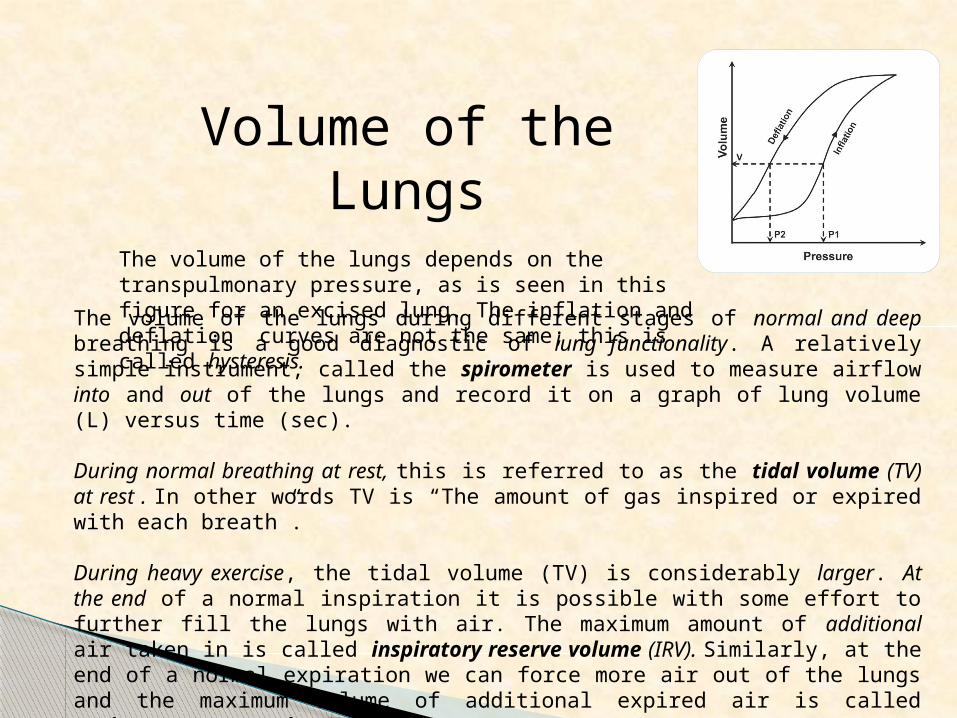
Volume of the LungsThe volume of the lungs depends on the transpulmonary pressure, as is seen in this figure for an excised lung. The inflation and deflation curves are not the same; this is called hysteresis.
The volume of the lungs during different stages of normal and deep breathing is a good diagnostic of lung functionality. A relatively simple instrument, called the spirometer is used to measure airflow into and out of the lungs and record it on a graph of lung volume (L) versus time (sec). During normal breathing at rest, this is referred to as the tidal volume (TV) at rest . In other words TV is “The amount of gas inspired or expired with each breath”.
During heavy exercise, the tidal volume (TV) is considerably larger. At the end of a normal inspiration it is possible with some effort to further fill the lungs with air. The maximum amount of additional air taken in is called inspiratory reserve volume (IRV). Similarly, at the end of a normal expiration we can force more air out of the lungs and the maximum volume of additional expired air is called expiratory reserve volume (ERV).
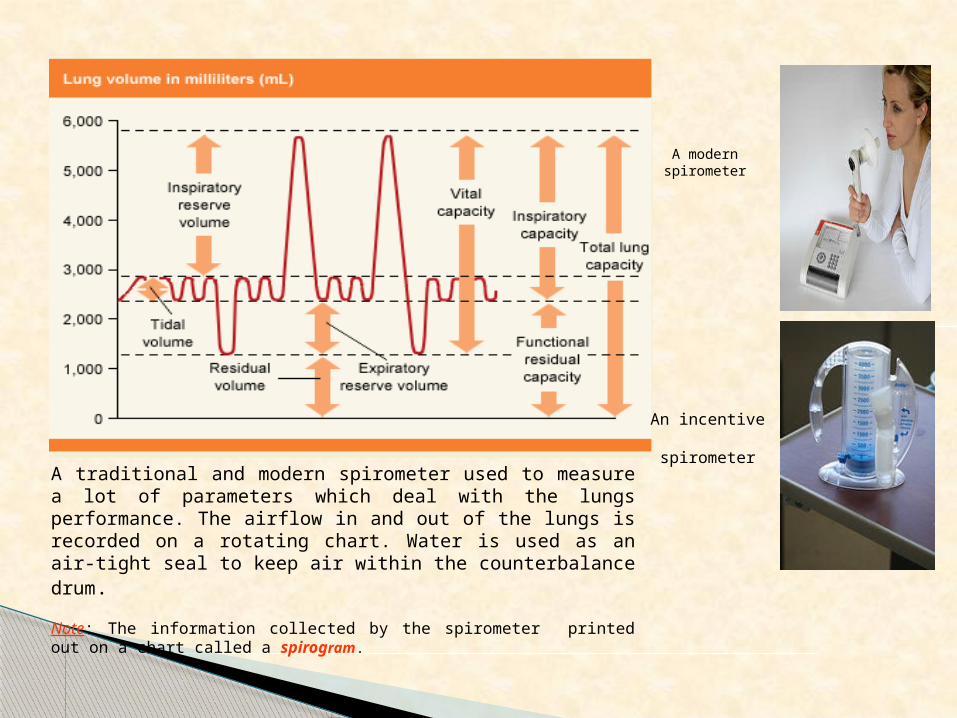
A traditional and modern spirometer used to measure a lot of parameters which deal with the lungs performance. The airflow in and out of the lungs is recorded on a rotating chart. Water is used as an air-tight seal to keep air within the counterbalance drum.
Note: The information collected by the spirometer printed out on a chart called a spirogram.
A modern spirometer
An incentive spirometer
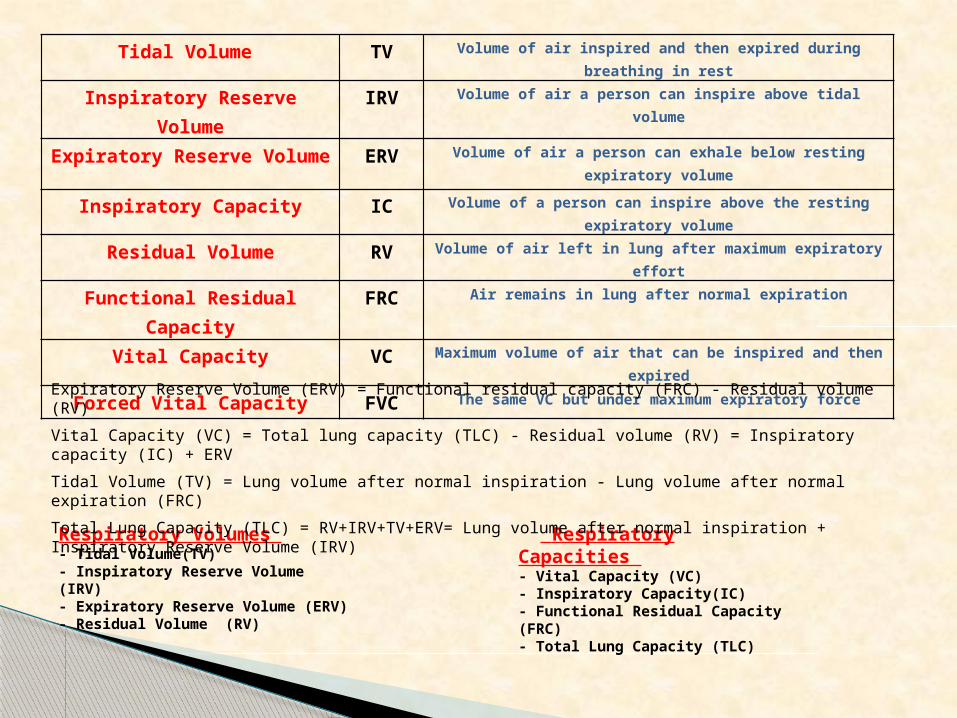
Tidal Volume TV Volume of air inspired and then expired during breathing in rest
Inspiratory Reserve Volume IRV Volume of air a person can inspire above tidal volume
Expiratory Reserve Volume ERV Volume of air a person can exhale below resting expiratory volume
Inspiratory Capacity IC Volume of a person can inspire above the resting expiratory volume
Residual Volume RV Volume of air left in lung after maximum expiratory effort
Functional Residual Capacity FRC Air remains in lung after normal expiration
Vital Capacity VC Maximum volume of air that can be inspired and then expired
Forced Vital Capacity FVC The same VC but under maximum expiratory force
Respiratory Volumes - Tidal Volume(TV) - Inspiratory Reserve Volume (IRV) - Expiratory Reserve Volume (ERV) - Residual Volume (RV)
Respiratory Capacities - Vital Capacity (VC) - Inspiratory Capacity(IC) - Functional Residual Capacity (FRC) - Total Lung Capacity (TLC)
Expiratory Reserve Volume (ERV) = Functional residual capacity (FRC) - Residual volume (RV)
Vital Capacity (VC) = Total lung capacity (TLC) - Residual volume (RV) = Inspiratory capacity (IC) + ERV
Tidal Volume (TV) = Lung volume after normal inspiration - Lung volume after normal expiration (FRC)
Total Lung Capacity (TLC) = RV+IRV+TV+ERV= Lung volume after normal inspiration + Inspiratory Reserve Volume (IRV)
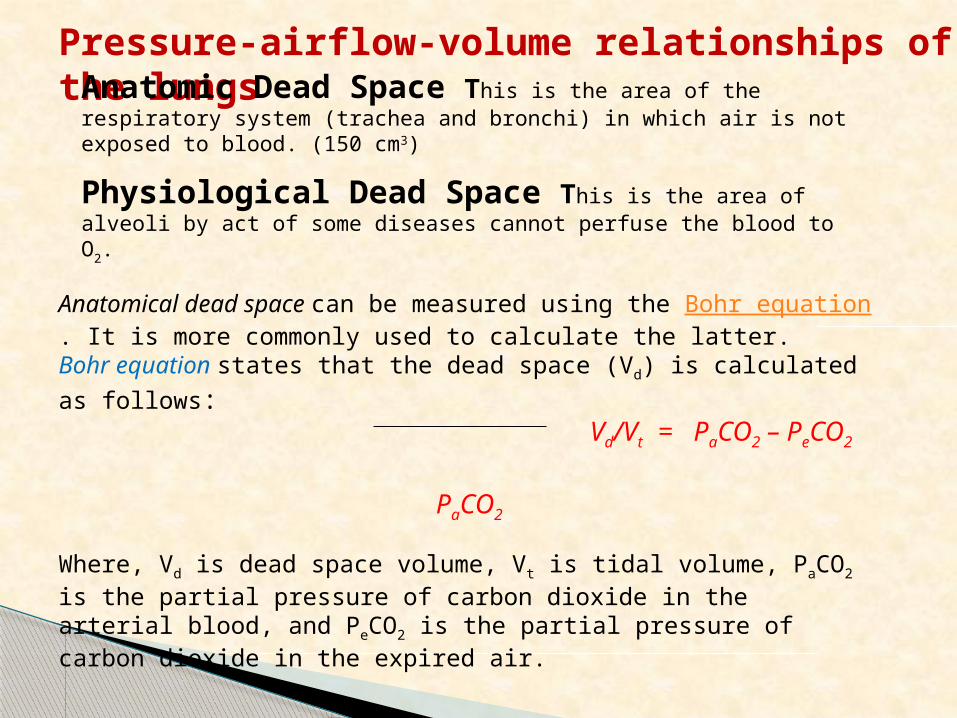
Pressure-airflow-volume relationships of the lungs
Anatomical dead space can be measured using the Bohr equation. It is more commonly used to calculate the latter. Bohr equation states that the dead space (Vd) is calculated as follows: Vd/Vt = PaCO2 – PeCO2
PaCO2
Where, Vd is dead space volume, Vt is tidal volume, PaCO2 is the partial pressure of carbon dioxide in the arterial blood, and PeCO2 is the partial pressure of carbon dioxide in the expired air.
Anatomic Dead Space This is the area of the respiratory system (trachea and bronchi) in which air is not exposed to blood. (150 cm3)
Physiological Dead Space This is the area of alveoli by act of some diseases cannot perfuse the blood to O2.
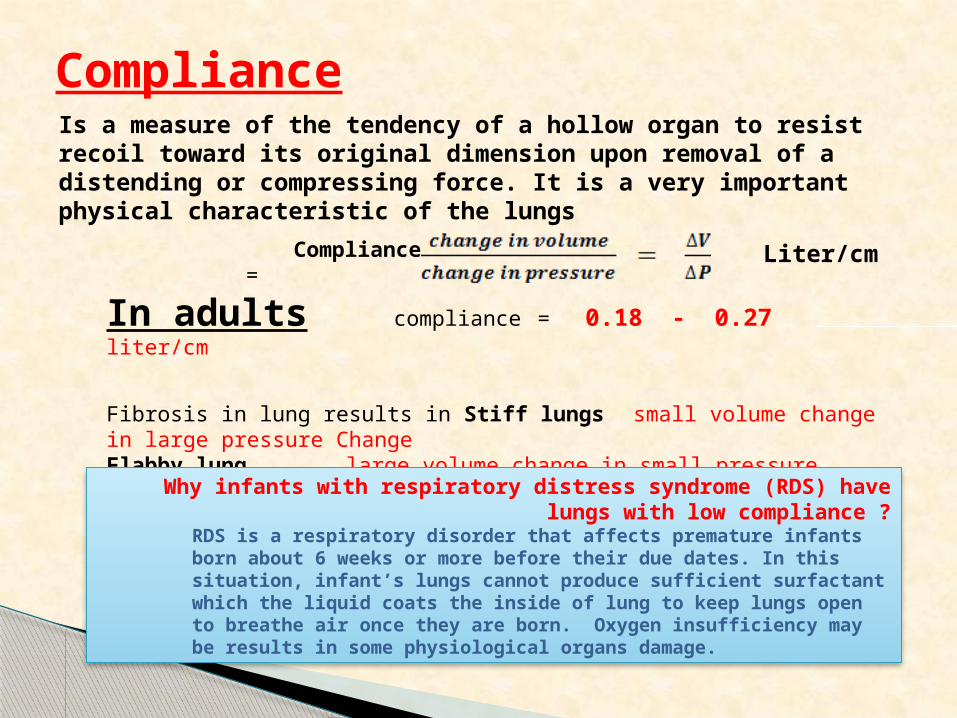
Is a measure of the tendency of a hollow organ to resist recoil toward its original dimension upon removal of a distending or compressing force. It is a very important physical characteristic of the lungs
Compliance
Compliance =
In adults compliance = 0.18 - 0.27 liter/cm
Fibrosis in lung results in Stiff lungs small volume change in large pressure ChangeFlabby lung large volume change in small pressure Change
Liter/cm
Why infants with respiratory distress syndrome (RDS) have lungs with low compliance ?RDS is a respiratory disorder that affects premature infants born about 6 weeks or more before their due dates. In this situation, infant’s lungs cannot produce sufficient surfactant which the liquid coats the inside of lung to keep lungs open to breathe air once they are born. Oxygen insufficiency may be results in some physiological organs damage.
Airway Resistance
We can breath in more rapidly than we breath out. During inspiration the forces on the airways tend to open them further; while, during expiration the forces tend to close the airways and thus restrict airflow. For a given lung volume, the expiratory flow rate reaches a maximum and remains constant; it might even decrease slightly with increased expiratory force. Patients with obstructive airway disease such as asthma or emphysema find that an increased effort to breathe out decrease the flow rate considerably. The flow of air in the lungs is analogous to the flow of current in an electrical circuit.
“Ohm’s law for air flow looks like Ohm’s law for electrical circuits, with voltage replaced by pressure difference ΔP and current replaced by the rate of air flow ΔV /Δt or V.
Airway resistance (R) is the ratio of ΔP/V [cm H2O (liter/sec)].
The airway resistance produced by the vocal cords causes a sizable pressure increase in the trachea is dependent on the:
(1) Dimensions of the tube.
(2) Viscosity of the gas.
Airway Resistance
Ohm’s law for electric circuit: V= IR then R = V/I (Volt/A)Airways resistance is given by the following equation: R= ∆P/V where V = ∆V/∆t (rate of air flow )
The time constant (t) of the lung is related to the airway resistance (R) and the compliance (C= ΔV/ΔP)
t = RC (sec)Time constant of the lung is complicated since many parts of the lung are interconnected. If one part of the lung has a larger time constant than other parts, it will not get its share of the air and that part of the lung will be poorly ventilated. The amount of work done in normal breathing account for a small fraction of the total energy consumed by the body (about 2% at rest) but the work of breathing during heavy exercise may amount to 25% of the body's total energy.
Physics of some common lung diseases
1- Emphysema The destruction of lung tissue reduces the springiness of the lungs. The lungs
become more compliant-a small change in pressure produces a larger than normal change in the volume [C=∆V/∆P]. Much of the work of breathing is done in overcoming the resistance of the airways R = ∆P/V
In emphysema walls of the alveoli are damaged by inflammation, hence alveoli can lose their natural elasticity and become overstretched and ruptured. Their will be a reduced number and strength of the springs which result in expansion of the chest wall and narrowing of the major airways causing an increase in airway resistance.
1- The lungs become flabby and expands as the reduced tension allows the chest wall to expand.
2- The tissues do not pull very hard on the airways, permitting the narrowed airways to collapse easily during expiration.
The person who has emphysema could be tested by being unable to blow out a candle.
2- Asthma
Asthma is another common obstructive disease, that causes the airways of the lungs to swell and narrow (its volume decreases). The basic problem is also expiratory difficulty due to the increased airway resistance [R= ∆P/V].
Some of this resistance is apparently due in part to swelling (edema) and mucus in the smaller airways, but much of it is due to contraction of the smooth muscles around the large airway. Lung compliance [C = ∆V/∆P ] is normal.
Functional residual capacity (FRC) [Lung volume after normal expiration] may be higher than normal, since the patient often starts to inspire before completing a normal expiration.
Common asthma triggers include:* Pet hair or dander * Dust * weather changes* Chemical Pollution * Pollen * Infections* Smoking
Aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) provoke asthma in some patients.
Many people with asthma have a personal or family history of allergies or eczema. Others have no history of allergies.
3- Fibrosis
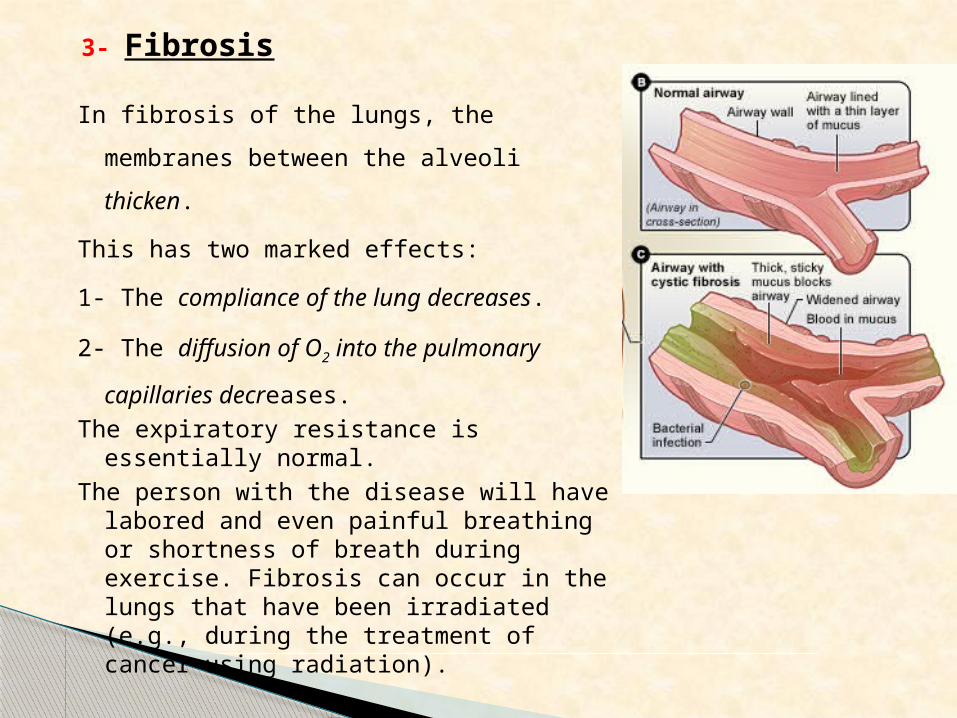
In fibrosis of the lungs, the membranes between the
alveoli thicken.
This has two marked effects:
1- The compliance of the lung decreases.
2- The diffusion of O2 into the pulmonary capillaries
decreases.
The expiratory resistance is essentially normal.
The person with the disease will have labored and even painful breathing or shortness of breath during exercise. Fibrosis can occur in the lungs that have been irradiated (e.g., during the treatment of cancer using radiation).
Medical Physics


![Human Body Exergy Balance: Numerical Analysis of an Indoor ... · Human body system [1]. A human body energy balance model, or twonode model, - was used for the human body system“](https://img.dokumen.tips/doc/110x75/6000b436c5a9c34ccd5461ab/human-body-exergy-balance-numerical-analysis-of-an-indoor-human-body-system.jpg)