Embed Size (px)
Citation preview

PPA Smyth
20. Potter J.D. Hypothyroidism and reproductive failure. Surg. Gynecol. Obstet. 150: 251, 1980.
21. Davis L.E., Leveno K.J., Cunningham G.F. Hypothyroidism complicating pregnancy. Obstet. Gynecol. 72: 108, 1988.
22. Mandell S.J., Reed Larsen P., Seely EW., Brent GA Increased need for thyroxine during pregnancy in women with primary hypothyroidism. N. Engl. J. Med. 323: 91, 1990.
23. Girling J.C., de Swiet M. Thyroxine dosage during pregnancy in women with primary hypothyroidism. Br. J. Obstet. Gynaecol. 99: 368, 1992.
25. Lazarus J.H., Othman S. Thyroid disease in relation to pregnancy. Clin. Endocrinol. 34: 91, 1991.
Thyroid Disease and Breast Cancer P.P.A. Smyth Endocrine Laboratory, Dept. of Medicine &Therapeutics, University College, Dublin, and The Breast Institute, St Vincent's Hospital, Dublin, Ireland. Key-words: Thyroid volume. thyroid ultrasound. breast cancer. gOiter, breast and thyroid.
Correspondence: Dr. P.PA Smyth, Endocrine Laboratory, Department of Medicine. Woodview, University College Dublin, Dublin 4, Ireland.
ABSTRACT. A review of the literature on the relationship between thyroid disorders and breast cancer does not provide conclusive evidence for the establishment of a causal relationship as breast cancer has been associated with hypothyroidism, hyperthyroidism and nontoxic goiter. Most reports on the association of thyroid enlargement and breast cancer have emanated from areas of endemic iodine deficiency and these reports have relied on neck palpation. The contribution of the present study is in the application of the highly sensitive technique of diagnostic ultrasound to the investigation of subtle changes in thyroid volume and anatomy in patients with breast cancer. The mean thyroid volume of 20.4±1.0 ml in 184 breast cancer patients was significantly greater than that of 12.9±1.2 ml in age-matched controls (p<0.01). Also the number of individual patients with breast can-
396
cer having enlarged thyroid glands (73/184; 39.7%) was significantly greater than the corresponding number (13/150; 8.6%) in the control group (p<0.001). There was a direct correlation between thyroid enlargement and breast tumour staging. Both mean thyroid volume and % of enlarged thyroids were identical in groups of patients scanned after (Retrospective Group) and before (Prospective Group) various therapies for breast cancer, thus excluding therapeutic intervention as a cause for thyroid enlargement. The results indicate a direct relationship between the two disorders perhaps involving a common growth stimulus and emphasise the importance of raising the consciousness of the coincidence of both disorders.
INTRODUCTION
The coincidence of the simultaneous occurrence of diseases of the thyroid and breast has long been a subject of conjecture. This coincidence can be explained in part by the fact that the two disorders predominantly affect women of a similar age. Since the report of Beatson (1) on the use of oopherectomy and thyroid extract in the treatment of breast cancer, many studies have shown a range of associations between the two disorders. Although evidence of extremes of thyroid dysfunction increasing breast cancer risks is difficult to obtain, the impression persists of some link between the two. The thyroid disorder most frequently implicated as a predisposing fact for breast cancer has been hypothyroidism or the use of L-T4 replacement therapy (2-6). An association between L-T4 replacement and breast cancer was subsequently refuted (7-9). Some reports showed an association between breast cancer and hyperthyroidism (10,11) but others (12,13) showed no evidence of such association. A retrospective study of 2,500 patients with a variety of thyroid disorders (14) showed no significant association with breast cancer and these findings were supported by other workers (9, 15, 16). An increased prevalence of thyroid antibodies was observed in patients with breast cancer (17) but another study (16) showed no change in deaths from breast cancer in patients who were antibody positive. The obvious possibility of a link between radioactive iodine 131 1 therapy for hyperthyroidism and increased risk for breast cancer was studied by Hoffman et al. (18, 19) who found no difference in breast cancer incidence when treatment with 131 1
was compared to surgery. Similarly, no increase in neoplasms was reported following either therapeutic or diagnostic doses of 131 1 for hyperthyroidism (20-22). The association between breast

cancer and non-toxic goiter has been extensively studied. Increased breast cancer in areas of endemic goiter has been reported (23-26) but no change in breast cancer incidence occurred when goiter rate decreased following iodine prophylaxis (4, 11). Finally, an increased breast cancer mortality was reported by Goldman (16) in patients who had non-toxic nodular goiter. Thus, the significance of the simultaneous occurrence of thyroid disease and breast cancer remains to be elucidated. The objective of the present study was to investigate if the availability of high resolution diagnostic ultrasound could permit the detection in patients with breast cancer of more subtle changes in thyroid volume or morphology.
PATIENTS AND METHODS Patients and controls
Patients under study were attending a specialist breast clinic, The Breast Institute, St.Vincent's Hospital, Dublin.
Breast cancer. One-hundred and eighty-four consecutive patients aged 28-89 years (mean 57.5± 13.6 years) had clinical and histological evidence of breast cancer. Ninety-one were studied retrospectively in that they had received both surgical and medical therapy before being subjected to thyroid ultrasound scans. The remaining 93 patients, termed the prospective group, had thyroid scans at the time of excision biopsy, before the diagnosis of breast malignancy. Patients were investigated for both breast and thyroid disease and any history of previous thyroid disease recorded.
Age matched controls. One-hundred and fifty nonhospitalized females aged 22-84 years (mean 51.0±8A years) served as controls.
Thyroid ultrasound scans
Thyroid ultrasound scans were performed using a scanner fitted with a hand held 7.5mHz linear transducer (Siemens SL-1, Darmstadt, Germany). The presence of solid nodules was recorded if they
Thyroid disease and breast cancer
Table 1 - Prevalence of thyroid disorders in breast cancer and age matched control populations.
Group Breast Cancer Control
Number of patients 184 150
Hyperthyroidism 6 3
Hypothyroidism 2 2
Nontoxic Goiter 18' 9
·p<O.01
were >5.0 mm diameter. Mixed echogenic patterns of >5.0 mm were also recorded as solid nodules. Only true thyroid cysts without evidence of internal echoes were so recorded. Thyroid volume was measured using transverse scans to obtain the width (W) and depth (D) of each lobe and longitudinal (L) scans to measure length. Volume of each lobe was calculated according to the formula (WxDxLxOA79) (27). The upper limit for normal thyroid volume in an iodine sufficient non-endemic goitrous area (18.0 ml. for adult females) (28) was used in this study. Thyroid volumes> 18.0 mi. were termed enlarged.
Statistical analysis
Results were analysed using Student's t-test for unpaired samples or the Chi-square test.
RESULTS Prevalence of thyroid disorders
The prevalence in the study groups of thyroid disorders past and present is shown in Table 1. There was no significant difference in the prevalence of hyperthyroidism and hypothyroidism between the breast cancer and control groups. However, the frequency of non-toxic goiter was greater in the breast cancer group than in controls (p<0.025).
Laboratory investigations
When investigations on patients with overt thyroid dysfunction were discarded, there was a remark-
Table 2 - Mean valueS±SE for serum T4, T3, TSH and PRL in breast cancer patients and control groups; N= number of patients.
N AGE T4 T3 TSH PRl (Years) (nmol/l) (nmol/l) (mUll) (ng/ml)
Breast Cancer 184 57.5± 1.0 106±2.0 2.1±0.03 2.2±0.1 5.0±OA
Control 150 51.0±0.6 116±2.0 2.2±0.04 1.9±0.08 4.5±0.29
397

PPA Smyth
** 40 MEAN 40
• VOLUME
i 30 Wi! % >18.0 ml 30 ~
i e :I Q
~ 20 * p>O.OI 20 ~ :9 * ** p>O.OI " e ~ ~
..c:: 10 Eo-<
10
0 0
CONTROL BREAST CANCER
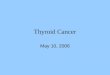
Fig. 1 - Thyroid volumes (mean±SE) and % of individual with enlarged thyroids (> 18.0 ml) in breast cancer and age-matched control groups.
able consistency in mean values±SE for serum T4, T3, TSH and PRL between the two groups as shown in Table 2.
Ultrasound scanning abnormalities
Normal echogenicity was observed in 89 patients but ultrasound scanning abnormalities, solid nodules or cysts, were present in 74 (40.2%) and 21 (11.4%) respectively. Thyroid scanning abnormalities (nodules and cysts) were detected in 51.6% of patients with breast cancer compared to 10.7% of controls and this difference was highly significant (p<0.001).
Thyroid volume
The distribution of individual thyroid volumes in the breast cancer group covered a broad range varying from 5.2 to 96.0 ml. Mean thyroid volumes and the percentage of individual patients having significant thyroid enlargement (volume> 18.0 ml) are shown in Figure 1. It can be seen that the mean volume of 20.4± 1.0 ml in the patients with breast cancer was significantly greater than that of 12.9± 1.2 ml in age matched controls (p< 0.01). Also the
number of individual patients with breast cancer having enlarged thyroid glands (73/184; 39.7%) was significantly greater than the corresponding number (13/150; 8.6%) in the control group (p<0.001 ).
Clinical correlations
Table 3 shows the results of attempts to relate enlarged thyroid volumes in patients with breast cancer to a number of other indices including tumor size, ovarian status and the influence of the antiestrogen Tamoxifen. Data from the 173 patients shown in Table 3 in whom results of accurate staging were available, show that mean thyroid volume increased with increasing tumor size (T3> T2, > T1) and this reached significance at T3 (p<0.05). Even more significant was the number of individual patients within each tumor staging group who had enlarged thyroids which reached a maximum in patients with breast tumors graded T3 or greater in whom 52.2% had enlarged thyroid volumes (p<0.02 compared to T1). When patients were divided on the basis of ovarian status, 62 were premenopausal and 122 postmenopausal . Both mean thyroid volumes and the percentage of patients having enlarged thyroid glands were significantly greater in the postmenopausal group (p<0.01 in each case). Finally the effect of Tamoxifen therapy was investigated in 98 patients, 50 of whom had been on long term therapy and 48 age matched breast cancer patients who had received no Tamoxifen. The respective mean thyroid volume and percentage enlarged thyroid volumes were not significantly different.
Retrospective vs prospective studies
To exclude the possibility that the enlarged thyroid volume observed in 39.7% of patients with breast cancer might arise from therapeutic intervention for breast cancer, sequential patients attending the breast clinic had thyroid ultrasound scans performed. This was done at the time of excision biopsy for discrete breast lumps (i.e. before the diagnosis of breast malignancy) . Patients from this se-
Table 3 - Relationship of thyroid volume to clinical indices in breast cancer patients. T1- T3 represent breast tumor staging.
Breast Tumour Ovarian Status Tamoxifen (Staging) Premenopausal Postmenopausal Yes No
T1 T2 T3
Number of patients 40 87 46 62 122 48 50
Thyroid volume (Mean±SE) 17.9±1.7 19.6±1.5 22.8±2.0 17.2±0.4 22.5± 1.5 20.4± 1.8 19.2±2.0
% of volumes> 18.0 ml 27.5 358 52.2 28.3 47.2 38.2 32.0
398

Thyroid disease and breast cancer
Table 4 - Comparison of mean thyroid volumestSE and % with enlarged thyroids in patients scanned following (Retrospective Group) and before (Prospective Group) commencement of therapies for breast cancer.
Group Number of patients Age Yrs
Control 150 51 .0±0.68
Breast Cancer 184 57.4±0.97
Retrospective 93 58.1±1.46
Prospective 91 56.7±1.26
ries subsequently diagnosed clinically and histologically as having breast cancer were therefore termed the Prospective Group (n=91) . Findings from this group were compared to those obtained in patients who had been studied after a variety of therapies for breast cancer (Retrospective Group, n=93). A comparison of results obtained is shown in Table 4. This table shows that both mean thyroid volumes and the percentage of individual patients having enlarged thyroids were basically identical between the Retrospective and Prospective Groups indicating that thyroid gland enlargement appeared to be independent of therapeutic intervention for breast cancer.
DISCUSSION
A review of the literature on the relationship between thyroid disorders and breast cancer does not provide conclusive evidence for the establishment of a causal relationship. Thyroid enlargement has been previously reported in association with breast cancer but these reports which relied on neck palpation have emanated from areas of endemic iodine deficiency (23-26) and indeed a direct role for iodine deficiency in promoting breast disease has been postulated (29, 30) . The contribution of the present study is in the application of the highly sensitive technique of diagnostic ultrasound to the investigation of subtle changes in thyroid volume and anatomy in patients with breast cancer. The underlying cause of the finding of enlarged thyroids in such a high proportion of these patients (39.7%) compared to age-matched controls without evidence of breast disease (S.6%) remains unknown. The finding of a significant direct correlation between thyroid enlargement and breast tumour size suggests the presence of a common growth stimulus with increasing potency reflected by gland size in both organs. The finding of significantly greater thyroid volume and % thyroid enlargement in postmenopausal compared to premenopausal breast cancer patients probably re-
399
Thyroid Volume Mean±SE N (%) of volumes >18.0 ml
12.9±1.2 13 (8.6)
20.4±1.0 73 (39.7)
200±1.2 39(41.9)
20.6±1.6 36 (39.6)
flects the improvement in dietary iodine intake in the younger population (31) . However, the fact that there is a direct association between the two conditions rather than thyroid enlargement occurring as a consequence of various therapies for breast cancer is strongly supported by the finding of a remarkable concurrence between results obtained in patients studied retrospectively or prospectively . Thus we are lead to speculate on the possibility of the endocrine, paracrine or autocrine growth stimuli identified in the thyroid (29) also exerting an action on the breast. The consequences of thyroid enlargement for the genesis or natural history of breast cancer remain unknown although one report (16) showed increased mortality (Standardised Mortality Rate:SMR=2.S) in breast cancer patients who had non-toxic nodular goiter and were receiving L-T4 suppression therapy. Perhaps the most important outcome of the demonstrated association between thyroid enlargement and breast cancer will be to emphasise the importance of raising the consciousness of the coincidence of both disorders.
ACKNOWLEDGMENTS
The author gratefully acknowledges the contribution of the following in making this work possible: Professor N.J. O'Higgins, Senior Oncology Nurse M.J. Murray and the the medical, nursing and clerical staff of the Breast Institute, St. Anthony's Rehabilitation Center; the staff of the Endocrine Laboratory, UCD Woodview, in particular the expert technical assistance of Mr. D.F. Smith and Ms. A.M. Hetherton, and the financial support of the Royal Col lege of Surgeons in Ireland.
REFERENCES
1. Beatson G.T. On the treatment of inoperable cases of carcinoma of the mamma: suggestions for a new method of treatment, with illustrative cases. Lancet 2: 104, 1896.
2. Loeser A.A. A new therapy for prevention of post-operative re-

PPA. Smyth
currences in genital and breast cancer: a six-years study of prophylactic thyroid treatment. Br. Med. J. 2: 1380,1954.
3. Stoll BA Breast cancer and hypothyroidism. Cancer 18:1431, 1965.
4. Backwinkel K., Jackson AS. Some features of breast cancer and thyroid deficiency. Cancer 17: 1174, 1964.
5. Takatani 0., Okumoto T., Kosano H., Nishida N., Hiraide M., Tamakuma S. Relationship between the levels of serum thyroid hormones or estrogen status and the risk of breast cancer genesis in Japanese women. Cancer Res. 49: 3109, 1989.
6. Kapdi C.C., Wolfe J. Breast cancer: relationship to thyroid supplements for hypothyroidism. JAMA 236: 1124, 1976.
7. Gorman CA, Becker D.V., Greenspan F.S., Levy R.P., Oppenheimer J.H., Rivlin R.S., Robbins J., Van derLaan J. American Thyroid Association statement: breast cancer and thyroid hormone therapy. Ann. Intern. Med. 86: 502, 1977.
8. Wallace R.B., Sherman B.M., Bean JA, Leeper J. Thyroid hormone use in patients with breast cancer: absence of an association. JAMA 239: 46, 1978.
9. Brinton LA, Hoffman DA, Hoover R., Fraumeni J.F. Relationship of thyroid disease and use of thyroid supplements to breast cancer risk. J. Chronic Dis. 37: 877, 1984.
10. Wanebo H.J., Benua R.S., Rawson RW. Neoplastic disease and thyrotoxicosis. Cancer 19: 1523, 1966.
11. Moossa AR., Price Evans DA, Brewer AC. Thyroid status and breast cancer; reappraisal of an old relationship. Ann. R. Coil. Surg. Engl. 53: 178,1973.
12. Kalache A, Vessey P., McPherson M. Thyroid disease and breast cancer: findings in a large case-control study. Br. J. Surg. 69: 434, 1982.
13. Chalstrey L.J., Benjamin B. High incidence of breast cancer in thyroid cancer patients. Br. J. Cancer 20: 670, 1966.
14. Hedley A~J., Jones S.I., Spiegelhalter D.J., Clements P., Bewsher P.D., Simpson J.G., Weir R.D. Breast cancer in thyroid disease: Fact or fallacy. Lancet 1: 1321,1981.
15. Goldman M.B. Thyroid diseases and breast cancer. Epidemiol. Rev. 12: 16,1990.
16. Goldman M.B., Monson R.R., Maloof F.
400
Cancer mortality in women with thyroid disease. Cancer Res. 50: 2283, 1990.
17. Itoh K., Maruchi N. Breast cancer in patients with Hashimoto's thyroiditis. Lancet 2: 1119,1975.
18. Hoffman D.A., McConahey W.M., Fraumeni J.F., Kurland LT Cancer incidence following treatment of hyperthyroidism. Int.J.Epidemiol.11:218,1982.
19. Hoffman DA Late effects of 1-131 therapy in the United States. In: Boice J.D. Jr., Fraumeni J.F. Jr. (Eds.), Radiation carcinogenesis: epidemiology and biological significance. Raven Press, New York, 1984, p. 273.
20. Holm L.E. Malignant disease following iodine-131 therapy in Sweden. In: Boice J.D. Jr., Fraumeni J.F. Jr. (Eds.), Radiation carcinogenesis: epidemiology and biological significance. Raven Press, New York, 1984, p. 263.
21. Goldman M.B., Maloof F., Monson R.R., Aschengrau A, Cooper D.S., Ridgway E.C. Radioactive iodine therapy and breast cancer: a follow-up study of hyperthyroid women. Am. J. Epidemiol. 127: 969,1988.
22. Holm L.-E., Wiklund K.E., Lundell G.E., Bergman N.A., Bjelkengren G., Ulla Britt C., Ericsson E.S., Ebbe C., Cederquist M.E., Lidberg R., Lidberg S., Harriet V., Wickbund H.V., Boice J.D. Cancer risk in population examined with diagnostic doses of 131 1. J. Natl. Cancer Inst. 81: 302,1989.
23. Spencer J.G.C. The influence of the thyroid in malignant disease. Br. J. Cancer 8: 393, 1954.
24. Bogardus G.M., Finley JW. Breast cancer and thyroid disease. Surgery 49:461,1961.
25. Doll R., Muir C., Waterhouse J. Cancer incidence in five continents. Int. Agency for Research on Cancer, 1966.
26. Adamopoulos D.A., Vassilarus S., Kapolla N., Papadiamantis J., Georgiakodis F., Michalkis A Thyroid disease in patients with benign and malignant mastopathy. Cancer 57: 125, 1986.
27. Brunn J., Block U., Ruf G., Bos I., Kunze w.P., Scriba P.C. Volumetrie der Schilddrusenlappen mittels Real-timeSonographie. Dtsch. Med. Wschr. 106: 1338,1981.
28. Gutekunst R., BeckerW., Hoermann R., OlbrichtTh., Pfannenstiel P. Ultraschalldiagnostik der Schilddruse. Dtsch. Med. Wschr. 113: 1109,1988.

29.Eskin BA Iodine metabolism and breast cancer. Trans. N.Y. Acad. Sci . 11:915, 1970.
30. Ghent W.R ., Eskin BA Iodine deficiency breast syndrome. In: Medeiros Neto G ., Gaitan E. (Eds.), Frontiers in Thyroidology. Raven Press, New York, 1986, Vol. 2, p. 1021.
401
Thyroid disease and breast cancer
31. Smyth P.P.A., Hetherton A.M., O'Carroll D., Smith D.F., O'Halloran M.J., O'Donovan O.K. Iodine intake in Ireland. An update. Ir. J. Med. Sci. 157: 377, 1988.
32. Dumont J.E. , Maenhaut C. , Pirson I. , Baptist M., Roger P.P. Growth factors controlling the thyroid gland. Bailliere's Clin. Endocrinol. Metabol. 5: 727, 1991.