Embed Size (px)
Citation preview

Thyroid disease. Endemic Thyroid disease. Endemic and sporadic goiter. and sporadic goiter.
Thyrotoxicosis. Thyrotoxicosis. ССlinical linical picture, diagnosis and picture, diagnosis and
treatment.treatment. Breast cancer. Breast cancer. Acute mastitis. Acute mastitis.
Dishormonal disease Dishormonal disease Breast.Breast.

Palpation of Palpation of the thyroid the thyroid
glandgland ((isthmusisthmus))

Palpation of Palpation of the thyroid the thyroid gland gland ((rightright
lobelobe))

Palpation of Palpation of the thyroid the thyroid gland gland ((left left
lobelobe))

Palpation of the thyroid glandPalpation of the thyroid gland

Palpation of the thyroid glandPalpation of the thyroid gland

CLASSIFICATION OF THE GOITER CLASSIFICATION OF THE GOITER ACCORDING TO THE FORM OF ACCORDING TO THE FORM OF
ENLARGMENTENLARGMENT
• Diffuse goiter;
• Nodular goiter;
• Mixed goiter.
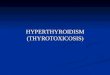
The degree of enlargementThe degree of enlargement
• 0 – the thyroid gland is not palpated;• І – the isthmus of the gland is noticeable during
swallowing and could be palpated;• ІІ – entire gland is noticeable during swallowing and
could be palpated;• ІІІ – the enlargement of gland results in evident
thickening of neck (“a thick neck”);• ІV – the gland considerably enlarged and sharply
deforms neck;• V – the enlargement reaches excessive size (goiter of
major sizes).

CLASSIFICATION OF THE GOITER CLASSIFICATION OF THE GOITER ACCORDING TO THE FUNCTIONAL ACCORDING TO THE FUNCTIONAL
STATESTATE• Euthyroid goiter (normal function);
• Hyperthyroid (excessive function);
• Hypothyroid (reduced function).

CLASSIFICATION OF THE GOITER CLASSIFICATION OF THE GOITER ACCORDING TO THE ACCORDING TO THE
LOCALIZATIONLOCALIZATION• Typical localization (anterior surface of the
neck);
• Retrosternal goiter;
• Ectopic goiter (goiter of the base of tongue, intrathoracic goiter);
• Goiter of the additional glands;
• Presternal goiter.

The nodular goiter of the III degreeThe nodular goiter of the III degree

The nodular The nodular goiter of the goiter of the
IV degreeIV degree

Goiter of major sizesGoiter of major sizes

The goiter The goiter formationformation
((intrathoracic intrathoracic goitergoiter))

Presternal goiterPresternal goiter

Clinical manifestations of Clinical manifestations of hyperthyroidism hyperthyroidism
Symptoms of hyperthyroidism include weight loss during normal or increased appetite, heat intolerance, excessive perspiration, muscle weakness, oligomenorrhea. Signs of hyperthyroidism include goiter, sinus tachycardia or atrial fibrillation, tremor, hyperreflexia, fine or thinning hair, muscle wasting.

Clinical features of Clinical features of hypothyroidism hypothyroidism
include cold intolerance, weight gain, constipation, edema (especially of the eyelids, hands, and feet), dry skin, weakness, somnolence, and menorrhagia.

Biochemical thyroid function Biochemical thyroid function testing testing
Currently, measurement of serum TSH level and free T4 (FT4) is the best and most
efficient combination of blood tests for diagnosis of most patients with thyroid disorders.
Biochemical thyroid function Biochemical thyroid function testing testing
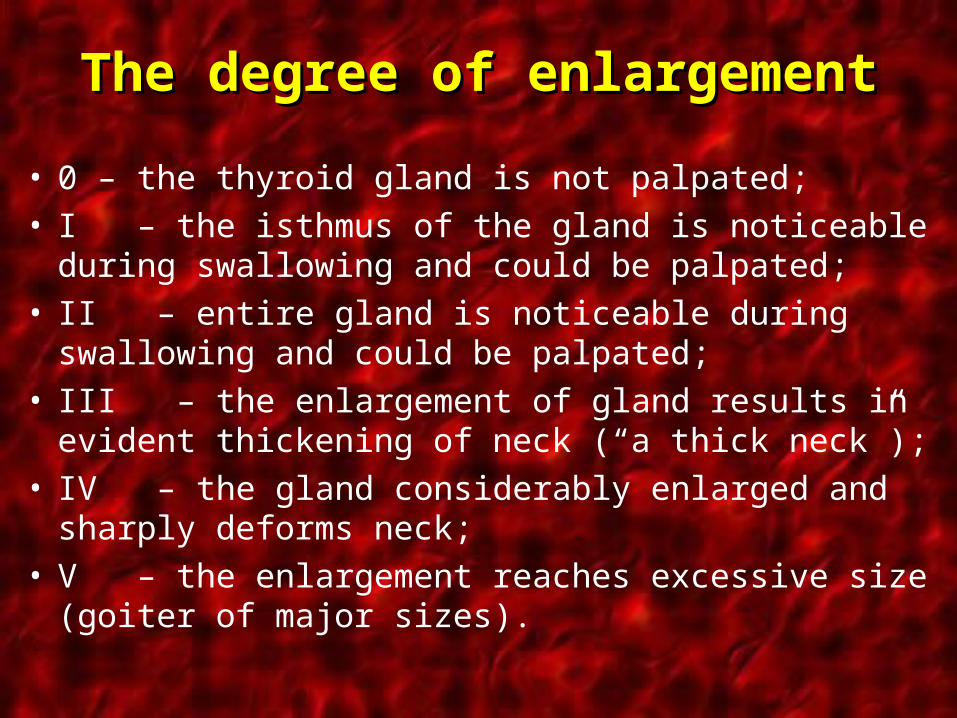
Measurement of TSH (0.3-5.0 mIU/L) by a second-generation sensitive TSH (sTSH) test is the single most useful biochemical test in the diagnosis of thyroid illness. In most ambulatory and hospitalized patients without pituitary disease, increased sTSH signifies hypothyroidism, suppressed sTSH suggests hyperthyroidism, and normal sTSH reflects a euthyroid state.

Biochemical thyroid function Biochemical thyroid function testing testing
Measurement of T3 (80-200 ng/dL) is test in
hypothyroidism. This test is useful in the occasional patient with suspected hyperthyroidism, suppressed sTSH.

Biochemical thyroid function Biochemical thyroid function testing testing
Antithyroid microsomal antibodies are found in the serum of patients with autoimmune thyroiditis (Hashimoto's thyroiditis), and measurement of these antibodies is helpful to diagnose this common cause of hypothyroidism. Anti-TSH receptor antibodies, which stimulate the TSH receptor, are detectable in more than 90% of patients with autoimmune hyperthyroidism (Graves' disease); however, their measurement is not often needed in the diagnosis of this disease.

Thyroid Function Test Thyroid Function Test Algorithm Algorithm
A useful thyroid function test algorithm (Clin Lab Med 13:673, 1993) includes sTSH assay as the initial test. If this is normal, no further tests are needed. If sTSH is elevated, FT4I and microsomal
antibodies are measured to confirm hypothyroidism, which is often autoimmune. If sTSH is suppressed, FT4I is measured to confirm
primary hyperthyroidism. If TSH is low and FT4I is
normal, T3 is measured to diagnose T3
thyrotoxicosis.

Scaning of the thyroid glandScaning of the thyroid gland

Scaning of the thyroid glandScaning of the thyroid gland
Thyroid imaging is most often accomplished with radionuclide scanning or ultrasound; other imaging modes, including computed tomographic (CT) scanning and MR scan, are useful in special circumstances.

Technetium thyroid scanning Technetium thyroid scanning Technetium thyroid scanning 20 minutes after the intravenous
injection of technetium-99m (99mTc) is useful in determining the size of the thyroid and in differentiating solitary functioning nodules from multinodular goiter or Graves' disease. Hypofunctioning areas (cyst, neoplasm, or suppressed tissue adjacent to autonomous nodules) are "cold," areas of increased synthesis are "hot." "Cold" nodules have a 15-20% risk of malignancy; most should be removed. "Hot" nodules are almost never malignant. 99mTc thyroid scans are most useful as adjunctive tests to assess risk of malignancy in patients with indeterminate thyroid nodule cytology or in hyperthyroid patients suspected of having a hyperfunctioning thyroid adenoma. Thyroid scanning 4-24 hours after oral iodine-131 (131I) is useful to identify metastatic differentiated thyroid tumors and to both confirm a diagnosis of Graves' disease.

Radionuclide thyroid scans of Radionuclide thyroid scans of normal thyroid glandnormal thyroid gland

Radionuclide thyroid scans of Radionuclide thyroid scans of thyroid gland (goiter)thyroid gland (goiter)

Radionuclide thyroid scans of Radionuclide thyroid scans of thyroid gland (diffuse goiter)thyroid gland (diffuse goiter)

Radionuclide thyroid scans of Radionuclide thyroid scans of thyroid gland (diffuse goiter)thyroid gland (diffuse goiter)

Radionuclide thyroid scans of Radionuclide thyroid scans of thyroid gland (nodular goiter)thyroid gland (nodular goiter)

Thyroid ultrasonography with Thyroid ultrasonography with high-frequency (7.5-10.0 MHz) high-frequency (7.5-10.0 MHz)
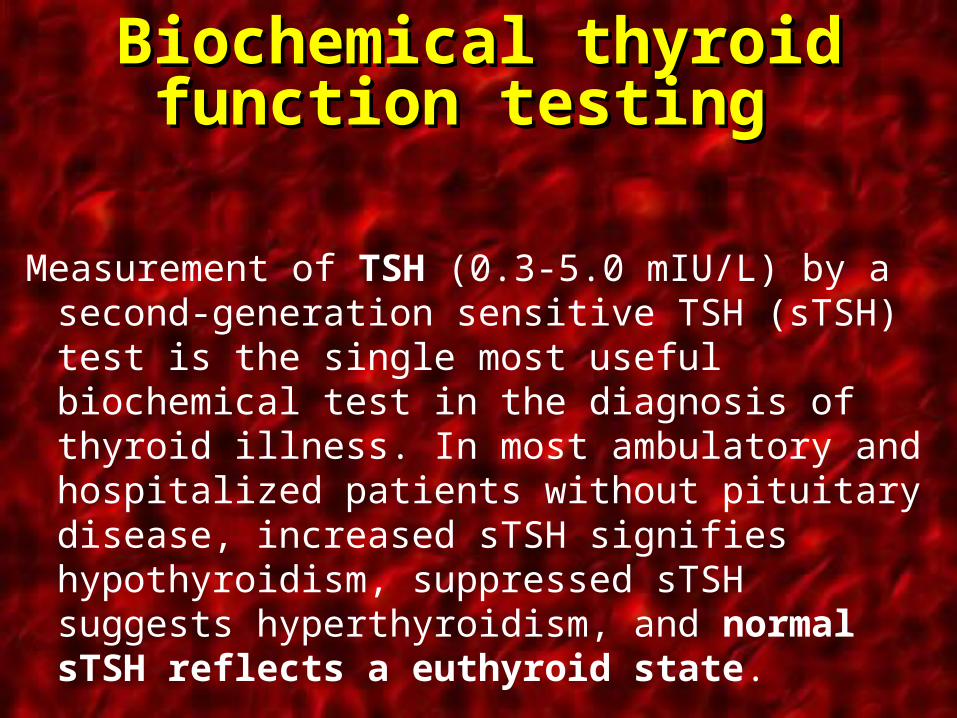
Thyroid ultrasonography with high-frequency (7.5-10.0 MHz) determines gland volume as well as the number and character of thyroid nodules. Although not completely reliable, features suggestive of malignancy on ultrasound include hypoechoic pattern, irregular margins, and microcalcifications. Ultrasound is useful to guide fine-needle aspiration (FNA) biopsy and cyst aspiration. Cysts seen on ultrasound, especially those larger than 3 cm, are malignant in up to 14% of cases.
Nodular goiterNodular goiter

Cyst of the thyroid glandCyst of the thyroid gland

Punction of the cyst of the thyroid glandPunction of the cyst of the thyroid gland

X-Ray examination, CT scanning X-Ray examination, CT scanning and MR scan and MR scan
X-Ray examination, CT scanning and MR scan of the thyroid are costly and generally are reserved for assessing substernal or retrosternal masses suspected to be goiters.

Retrosternal goiterRetrosternal goiter

Retrosternal Retrosternal goiter goiter
((X-Ray and CTX-Ray and CT))

Retrosternal goiterRetrosternal goiter

Retrosternal goiterRetrosternal goiter

Retrosternal goiterRetrosternal goiter

Retrosternal Retrosternal goitergoiter

Retrosternal goiter Retrosternal goiter ((electro X-Rayelectro X-Ray))

Retrosternal goiterRetrosternal goiter
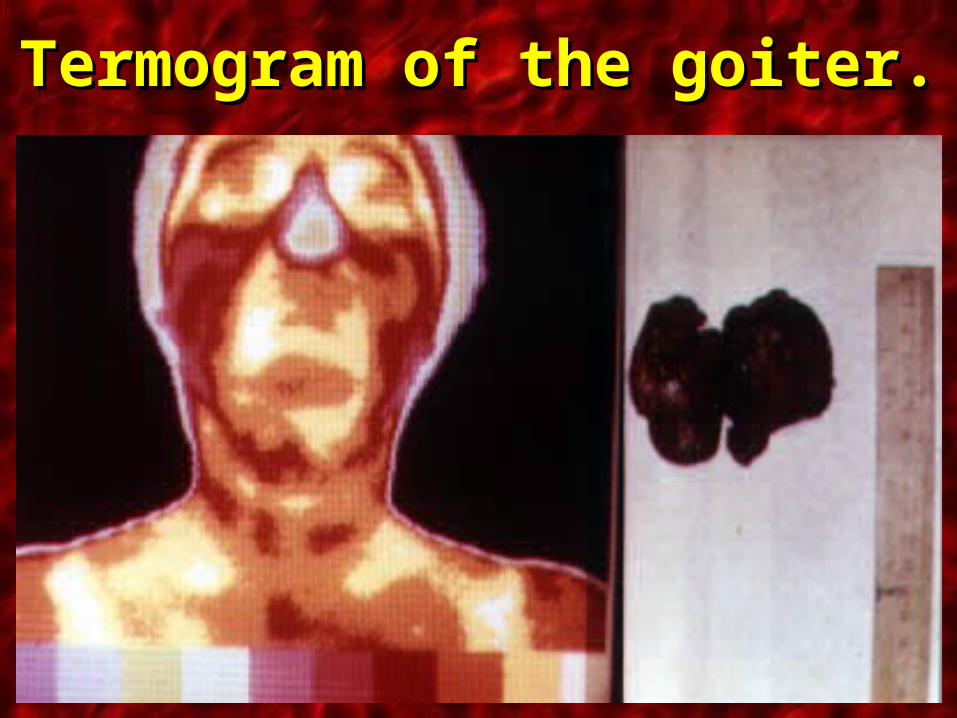
Termogram of the goiterTermogram of the goiter..

Trachea deformationTrachea deformation

Complication of the goiterComplication of the goiter ((tracheomalatia tracheomalatia ))

Autoimmune diffuse toxic goiter Autoimmune diffuse toxic goiter (Graves' disease) (Graves' disease)
Autoimmune diffuse toxic goiter (Graves' disease) is the most common cause of hyperthyroidism and may be caused by stimulating immunoglobulins directed against the TSH receptor. Graves' disease may be treated with antithyroid drugs, ablation with radioactive iodine (RAI), or surgery, depending on the clinical situation.

Diffuse goiterDiffuse goiter

Diffuse goiterDiffuse goiter

Diffuse goiterDiffuse goiter

Diffuse goiterDiffuse goiter
( (Pathological Pathological exophthalmexophthalm))
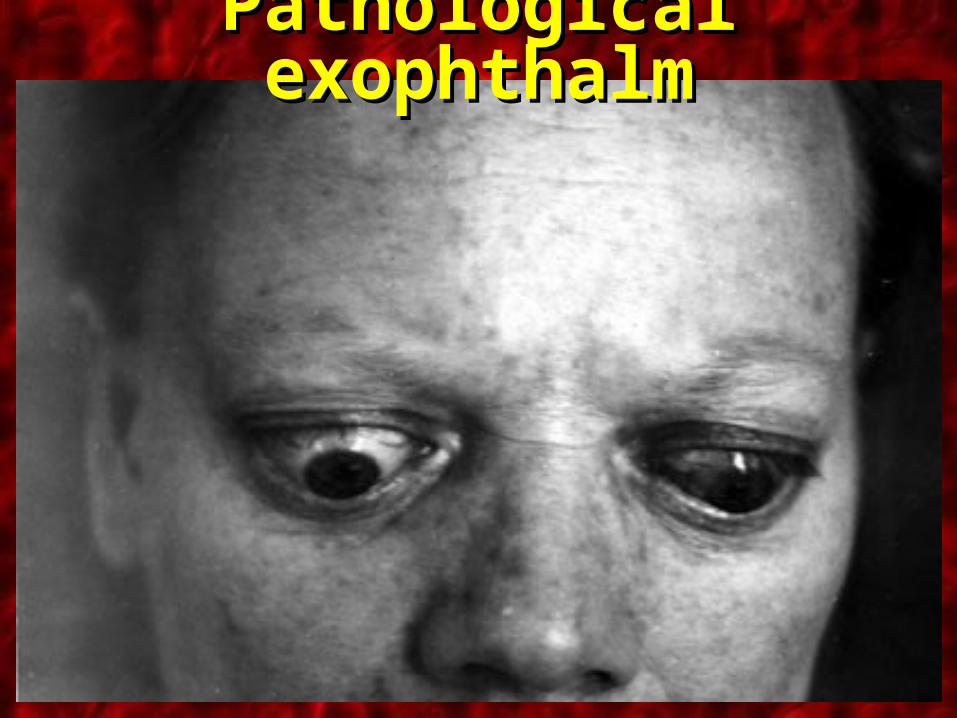
Pathological exophthalmPathological exophthalm

Pathological Pathological exophthalmexophthalm

External signs of the thyroid gland External signs of the thyroid gland diseasesdiseases

Treatment of the Graves' DiseaseTreatment of the Graves' Disease
Thionamide drugs, such as propylthiouracil (PTU) or methimazole, are the initial therapy in most cases. PTU (100-300 mg p.o. t.i.d.) is given for 4-6 weeks until the patient becomes euthyroid; then the dosage usually is decreased (PTU, 100 mg p.o. t.i.d.). The patient is then treated empirically for 6-18 months, at which time the drugs are withdrawn. Clinical features that favor remission include small gland size and mild hyperthyroidism of recent onset, although overall, long-term remission is achieved in less than 20-30% of patients.

Treatment of the Graves' DiseaseTreatment of the Graves' Disease
Antithyroid drugs also are used to prepare thyrotoxic patients for surgery or ablative therapy. PTU may be given during pregnancy at reduced doses, especially if thyroidectomy is necessary in the second trimester. Minor adverse reactions occur infrequently and include rash, hepatitis, arthralgias, and a lupuslike syndrome. Agranulocytosis is a rare (0.5%) but serious side effect of thionamide therapy.

Treatment of the Graves' DiseaseTreatment of the Graves' DiseaseAblation with RAI is the treatment of choice for
most patients with Graves' disease. A dose of 5-10 mCi of 131I is given orally and is 75% effective after 4-12 weeks. In the 25% of patients with persistent thyrotoxicosis after 12 weeks, double the initial dose is repeated. After treatment, there is a high incidence (70%) of eventual permanent hypothyroidism, which is managed easily by replacement therapy. There are virtually no other long-term side effects of RAI (i.e., no significantly increased risk of thyroid cancer, leukemia, or teratogenicity).

Treatment of the Graves' DiseaseTreatment of the Graves' Disease
Ablation with RAI is the treatment of choice for most patients with Graves' disease. Contraindications to radiotherapy include pregnant women, newborns, patients who refuse, or patients with low RAI uptake (<20%) in the thyroid. Treatment of children or young adults (younger than 30 years) with RAI is controversial because of presumed long-term oncogenic risks.

Thyroidectomy for Graves' diseaseThyroidectomy for Graves' disease
Thyroidectomy for Graves' disease may be indicated for children or, patients unresponsive to medical therapy, or patients who refuse RAI.
A bilateral subtotal thyroidectomy should be performed with the goal of leaving a 1- to 2-g vascularized cuff of thyroid on each side. However, some centers advocate total thyroidectomy as primary treatment to decrease recurrence rate of goitrous disease. Risks of surgery are extremely small (<1%) in experienced hands but include hypoparathyroidism and injury to the recurrent laryngeal nerve.

SubtotalSubtotal subfascialsubfascial resection resection of the thyroid glandof the thyroid gland

Operation. Retrosternal goiter.Operation. Retrosternal goiter.

Resection of the thyroid glandResection of the thyroid gland

OperationOperation right-side hemithyroidectomyright-side hemithyroidectomy

SubtotalSubtotal subfascialsubfascial resection of the resection of the thyroid glandthyroid gland

Thyroidectomy for Graves' diseaseThyroidectomy for Graves' disease
Surgery results in hypothyroidism less frequently than does RAI (N Engl J Med 311:426, 1984). The long-term incidence of recurrent hyperthyroidism after surgery is approximately 10%. Patients with recurrent hyperthyroidism after thyroidectomy should be treated with RAI.

Management of complications after Management of complications after thyroidectomy thyroidectomy
Hemorrhage is a rare but serious complication of thyroidectomy that usually occurs within 6 hours of surgery. Management can require control of the airway by endotracheal intubation and can rarely mandate urgent opening of incision and evacuation of hematoma before returning to the operating room for wound irrigation and ligation of the bleeding point.

Management of complications after Management of complications after thyroidectomy thyroidectomy
Transient hypocalcemia commonly occurs 24-48 hours after thyroidectomy but infrequently requires treatment. Patients who are markedly symptomatic or who have serum calcium below 7 mg/dL are given 1-2 ampules (10-20 mL) of 10% calcium gluconate i.v. over 1-2 minutes followed by temporary oral calcium carbonate (500 mg p.o. t.i.d.). More prolonged intravenous replacement is achieved by mixing 6 ampules of 10% calcium gluconate (540 mg elemental calcium) in D5W, 500 mL, for infusion at 1 mL/kg per hour. Permanent hypoparathyroidism is uncommon after total thyroidectomy. Normal parathyroid tissue removed or devascularized at the time of total thyroidectomy may be autotransplanted into sternocleidomastoid muscle to prevent postoperative hypocalcemia

Management of complications after Management of complications after thyroidectomy thyroidectomy
Recurrent laryngeal nerve (RLN) injury is a devastating complication of thyroidectomy that should occur rarely (<1%). Unilateral RLN injury causes hoarseness, and bilateral injury compromises the airway, necessitating tracheostomy. Repeat neck exploration, thyroidectomy for extensive goiter or Graves' disease, and thyroidectomy for fixed, locally invasive cancers are procedures particularly prone to RLN injury. Intentional (as with locally invasive cancer) or inadvertent transection of the RLN can be repaired primarily or with a nerve graft, although the efficacy of these repairs is not known. Temporary RLN palsies can occur during thyroidectomy, and these usually resolve over a period of 4-6 weeks.

Management of complications after Management of complications after thyroidectomy thyroidectomy
Recurrent laryngeal nerve (RLN) injury
The external branch of the superior laryngeal nerve may be injured if not identified during ligation of the superior thyroid pole vascular bundle. This injury results in weakness of the patient's voice at high pitch. The best prevention of these injuries is a thorough understanding of the anatomy of these nerves.