STEP 31. Anatomi sinus paranasal?A sinus is a hollow, air-filled
cavity. For the purposes of this article, a sinus will referred to
those hollow cavities that are in the skull and connected to the
nasal airway by a narrow hole in the bone (ostium). Normally all
are open to the nasal airway through an ostium. Humans have four
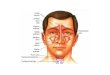
pair of these cavities each referred to as the:1. frontal sinus (in
forehead),2. maxillary sinus (behind cheeks),3. ethmoid sinuses
(between the eyes), and4. sphenoid sinus (deep behind the
ethmoids).The four pair of sinuses are often described as a unit
and termed the "paranasal sinuses." The cells of the inner lining
of each sinus are mucus-secreting cells, epithelial cells and some
cells that are part of the immune system (macrophages, lymphocytes,
and eosinophils).
Fungsi sinus:Functions of the sinuses include humidifying and
warming inspired air, insulation of surrounding structures (eyes,
nerves), increasing voice resonance, and as buffers against facial
trauma. The sinuses decrease the weight of the skull. If the
inflammation hinders the clearance of mucous or blocks the natural
ostuim, the inflammation may progress into a bacterial
infectionhttp://www.medicinenet.com/sinusitis/page2.htmAnatomi
Sinus ParanasalAda empat pasang sinus paranasal yaitu sinus
maksila, sinus frontal, sinus etmoid dan sinus sfenoid kanan dan
kiri. Sinus paranasal merupakan hasil pneumatisasi tulang-tulang
kepala, sehingga terbentuk rongga di dalam tulang. Semua sinus
mempunyai muara ke rongga hidung.Secara embriologik, sinus
paranasal berasal dari invaginasi mukosa rongga hidung dan
perkembangannya dimulai pada fetus usia 3-4 bulan, kecuali sinus
sfenoid dan sinus frontal. Sinus maksila dan sinus etmoid telah ada
saat anak lahir, sedangkan sinus frontal berkembang dari dari sinus
etmoid anterior pada anak yang berusia kurang lebih 8 tahun.
Pneumatisasi sinus sfenoid dimulai pada usia 8-10 tahun dan berasal
dari bagian postero-superior rongga hidung. Sinus-sinus ini umumnya
mencapai besar maksila 15-18 tahun.
Sinus MaksilaSinus maksila merupakan sinus paranasal yang
terbesar. Saat lahir sinus maksila bervolume 6-8 ml, sinus kemudian
berkembang dengan cepat dan akhirnya mencapai ukuran maksimal,
yaitu 15 ml saat dewasa.Sinus maksila berbentuk segitiga. Dinding
anterior sinus ialah permukaan fasial os maksila yang disebut fosa
kanina, dinding posteriornya adalah permukaan infra-temporal
maksila, dinding medialnya ialah dinding lateral rongga hidung
dinding superiornya adalah dasar orbita dan dinding inferior ialah
prosesus alveolaris dan palatum. Ostium sinus maksila berada di
sebelah superior dinding medial sinus dan bermuara ke hiatus
semilunaris melalui infindibulum etmoid.
Dari segi klinik yang perlu diperhatikan dari anatomi sinus
maksila adalah1.Dasar dari anatomi sinus maksila sangat berdekatan
dengan akar gigi rahang atas, yaitu premolar (P1 dan P2), molar (M1
dan M2), kadang-kadang juga gigi taring (C) dan gigi molar M3,
bahkan akar-akar gigi tersebut dapat menonjol ke dalam sinus,
sehingga infeksi gigi geligi mudah naik ke atas menyebabkan
sinusitis.2.Sinusitis maksila dapat menyebabkan komplikasi
orbita.3.Ostium sinus maksila terletak lebih tinggi dari dasar
sinus, sehingga drainase kurang baik, lagipula drainase juga harus
melalui infundibulum yang sempit. Infundibulum adalah bagian dari
sinus etmoid anterior dan pembengkakan akibat radang atau alergi
pada daerah ini dapat menghalangi drenase sinus maksila dan
selanjutnya menyebabkan sinusitus.
Sinus FrontalSinus frontal yang terletak di os frontal mulai
terbentuk sejak bulan ke empat fetus, berasal dari sel-sel resesus
frontal atau dari sel-sel infundibulum etmoid. Sesudah lahir, sinus
frontal mulai berkembang pada usia 8-10 thn dan akan mencapai
ukuran maksimal sebelum usia 20 thn.Sinus frontal kanan dan kiri
biasanya tidak simetris, satu lebih besar dari pada lainnya dan
dipisahkan oleh sekret yang terletak di garis tengah. Kurang lebih
15% orang dewasa hanya mempunyai satu sinus frontal dan kurang
lebih 5% sinus frontalnya tidak berkembang.Ukurannya sinus frontal
adalah 2.8 cm tingginya, lebarnya 2.4 cm dan dalamnya 2 cm. Sinus
frontal biasanya bersekat-sekat dan tepi sinus berleku-lekuk. Tidak
adanya gambaran septumn-septum atau lekuk-lekuk dinding sinus pada
foto Rontgen menunjukkan adanya infeksi sinus. Sinus frontal
dipisakan oleh tulang yang relatif tipis dari orbita dan fosa
serebri anterior, sehingga infeksi dari sinus frontal mudah
menjalar ke daerah ini.Sinus frontal berdraenase melalui ostiumnya
yang terletak di resesus frontal. Resesus frontal adalah bagian
dari sinus etmoid anteroir.
Sinus EtmoidDari semua sinus paranasal, sinus etmoid yang paling
bervariasi dan akhir-akhir ini dianggap paling penting, karena
dapat merupakan fokus infeksi bagi sinus-sinus lainnya. Pada orang
dewasa bentuk sinus etomid seperti piramid dengan dasarnya di
bagian posterior. Ukurannya dari anterior ke posterior 4-5 cm,
tinggi 2.4 cmn dan lebarnya 0.5 cm di bagian anterior dan 1.5 cm di
bagian posterior.Sinus etmoid berongga-rongga, terdiri dari sel-sel
yang menyerupai sarang tawon, yang terdapat di dalam massa bagian
lateral os etmoid, yang terletak di antara konka media dan dinding
medial orbita. Sel-sel ini jumlahnya bervariasi antara 4-17 sel
(rata-rata 9 sel). Berdasarkan letaknya, sinus etmoid dibagi
menjadi sinus etmoid anterior yang bermuara di meatus medius dan
sinus etmoid posterior yang bermuara di meatus superior. Sel-sel
sinus etmoid anterior biasanya kecil-kecil dan banyak, letaknya di
bawah perlekatan konka media, sedangkan sel-sel sinus etmoid
posterior biasanya lebih besar dan lebih sedikit jumlahnya dan
terletak di postero-superior dari perlekatan konka media.Di bagian
terdepan sinus etmoid enterior ada bagian yang sempit, disebut
resesus frontal, yang berhubungan dengan sinus frontal. Sel etmoid
yang terbesar disebut bula etmoid. Di daerah etmoid anterior
terdapat suatu penyempitan yang disebut infundibulum, tempat
bermuaranya ostium sinus maksila. Pembengkakan atau peradangan di
resesus frontal dapat menyebabkan sinusitis frontal dan
pembengkakan di infundibulum dapat menyebabkan sisnusitis
maksila.Atap sinus etmoid yang disebut fovea etmoidalis berbatasan
dengan lamina kribosa. Dinding lateral sinus adalah lamina
papirasea yang sangat tipis dan membatasi sinus etmoid dari rongga
orbita. Di bagian belakang sinus etmoid posterior berbatsan dengan
sinus sfenoid.
Sinus SfenoidSinus sfenoid terletak dalam os sfenoid di belakang
sinus etmoid posterior. Sinus sfenoid dibagi dua oleh sekat yang
disebut septum intersfenoid. Ukurannya adalag 2 cmn tingginya,
dalamnya 2.3 cm dan lebarnya 1.7 cm. Volumenya bervariasi dari
5-7.5 ml. Saat sinus berkembang, pembuluh darah dan nerbus di
bagian lateral os sfenoid akan menjadi sangat berdekatan dengan
rongga sinus dan tampak sebagai indentasi pada dinding sinus
etmoid.Batas-batasnya ialah, sebelah superior terdapat fosa serebri
media dan kelenjar hipofisa, sebelah inferiornya atap nasofaring,
sebelah lateral berbatasan dengan sinus kavernosus dan a.karotis
interna (sering tampak sebagai indentasi) dan di sebelah
posteriornya berbatasan dengan fosa serebri posterior di daerah
pons.
Kompleks Ostio-MeatalDi meatus medius, ada muara-muara saluran
dari sinus maksila, sinus frontal dan sinus etmoid anterior. Daerah
ini rumit dan sempit dan dinamakan kompleks ostio-meatal (KOM),
terdiri dari infundibulum etmoid yang terdapat di belakang prosesus
unsinatus, resesus frontalis, bula etmoid dan sel-sel etmoid
anterior dengan ostiumnya dan ostium sinus maksila.
Fungsi Sinus ParanasalSampai saat ini belum ada kesesuaian
pendapat mengenai fisiologi sinus paranasal. Beberapa pendapat:a.
Sebagai pengatur kondisi udara (air conditioning)Sinus berfungsi
sebagai ruang tambahan untuk memanaskan dan mengatur kelembaban
udara inspirasi. Keberatan terhadap teori ini ialah karena ternyata
tidak didapati pertukaran udara yang definitive antara sinus dan
rongga hidung. Lagipula mukosa sinus tidak mempunyai vaskularisasi
dan kelenjar yang sebanyak mukosa hidung.
b. Sebagai penahan suhu (termal insulators)Sinus paranasal
berfungsi sebagai penahan (buffer) panas, melindungi orbita dan
fossa serebri dari suhu rongga hidung yang berubah-ubah.c. Membantu
keseimbangan kepalabila udara dalam sinus diganti dengan tulang,
hanya akan memberikan pertambahan berat sebesar 1% dari berat
kepala, sehingga teori dianggap tidak bermakna.d. Membantu
resonansi suaraAkan tetapi ada yang berpendapat, posisi sinus dan
ostiumnya tidak memungkinkan sinus berfungsi sebagai resonator yang
efektif. Lagipula tidak ada korelasi antara resonansi suara dan
besarnya sinus pada hewan-hewan tingkat rendah.e. Sebagai peredam
perubahan tekanan udaramisalnya pada waktu bersin atau membuang
ingus.f. Membantu produksi mucusjumlahnya kecil dibandingkan dengan
mucus dari rongga hidung, namun efektif untuk membersihkan partikel
yang turut masuk dengan udara inspirasi karena mucus ini keluar
dari meatus medius, tempat yang paling strategis.THT FK UI
2. Mengapa pasien menguluh pilek tidak sembuh sejak 4 bulan yg
lalu?Retained mucus, when infected, leads to sinusitis. Another
mechanism hypothesizes that because the sinuses are continuous with
the nasal cavity, colonized bacteria in the nasopharynx may
contaminate the otherwise sterile sinuses. These bacteria are
usually removed by mucociliary clearance; thus, if mucociliary
clearance is altered, bacteria may be inoculated and infection may
occur, leading to sinusitisThe pathophysiology of rhinosinusitis is
related to 3 factors: Obstruction of sinus drainage pathways (sinus
ostia) Ciliary impairment Altered mucus quantity and quality
Obstruction of sinus drainage Obstruction of the natural sinus
ostia prevents normal mucus drainage. The ostia can be blocked by
mucosal swelling or local causes (eg,trauma, rhinitis), as well as
by certain inflammation-associated systemic disorders and immune
disorders. Systemic diseases that result in decreased mucociliary
clearance, including cystic fibrosis, respiratory allergies, and
primary ciliary dyskinesia (Kartagener syndrome), can be
predisposing factors for acute sinusitis in rare cases. Patients
with immunodeficiencies (eg, agammaglobulinemia, combined variable
immunodeficiency, and immunodeficiency with reduced immunoglobulin
G [IgG] and immunoglobulin A [IgA]bearing cells) are also at
increased risk of developing acute sinusitis. Mechanical
obstruction because ofnasal polyps, foreign bodies, deviated septa,
or tumors can also lead to ostial blockage. In particular,
anatomical variations that narrow the ostiomeatal complex,
including septal deviation, paradoxical middle turbinates, and
Haller cells, make this area more sensitive to obstruction from
mucosal inflammation. Usually, the margins of the edematous mucosa
have a scalloped appearance, but in severe cases, mucus may
completely fill a sinus, making it difficult to distinguish an
allergic process from infectious sinusitis. Characteristically, all
of the paranasal sinuses are affected and the adjacent nasal
turbinates are swollen. Air-fluid levels and bone erosion are not
features of uncomplicated allergic sinusitis; however, swollen
mucosa in a poorly draining sinus is more susceptible to secondary
bacterial infection. Hypoxia within the obstructed sinus is thought
to cause ciliary dysfunction and alterations in mucus production,
further impairing the normal mechanism for mucus clearance.
Impaired ciliary function Contrary to earlier models of sinus
physiology, the drainage patterns of the paranasal sinuses depend
not on gravity but on the mucociliary transport mechanism. The
metachronous coordination of the ciliated columnar epithelial cells
propels the sinus contents toward the natural sinus ostia. Any
disruption of the ciliary function results in fluid accumulation
within the sinus. Poor ciliary function can result from the loss of
ciliated epithelial cells; high airflow; viral, bacterial, or
environmental ciliotoxins; inflammatory mediators; contact between
2 mucosal surfaces; scars; andKartagener syndrome.[16] Ciliary
action can be affected by genetic factors, such as Kartagener
syndrome. Kartagener syndrome is associated with immobile cilia and
hence the retention of secretions and predisposition to sinus
infection. Ciliary function is also reduced in the presence of low
pH, anoxia, cigarette smoke, chemical toxins, dehydration, and
drugs (eg, anticholinergic medications and antihistamines).
Exposure to bacterial toxins can also reduce ciliary function.
Approximately 10% of cases of acute sinusitis result from direct
inoculation of the sinus with a large amount of bacteria. Dental
abscesses or procedures that result in communication between the
oral cavity and sinus can produce sinusitis by this mechanism.
Additionally, ciliary action can be affected after certain viral
infections. Several other factors can lead to impaired ciliary
function. Cold air is said to stun the ciliary epithelium, leading
to impaired ciliary movement and retention of secretions in the
sinus cavities. On the contrary, inhaling dry air desiccates the
sinus mucous coat, leading to reduced secretions. Any mass lesion
with the nasal air passages and sinuses, such as polyps, foreign
bodies, tumors, and mucosal swelling from rhinitis, may block the
ostia and predispose to retained secretions and subsequent
infection. Facial trauma or large inoculations from swimming can
produce sinusitis as well. Drinking alcohol can also cause nasal
and sinus mucosa to swell and cause impairment of mucous drainage.
Altered quality and quantity of mucus Sinonasal secretions play an
important role in the pathophysiology of rhinosinusitis. The mucous
blanket that lines the paranasal sinuses contains
mucoglycoproteins, immunoglobulins, and inflammatory cells. It
consists of 2 layers: (1) an inner serous layer (ie, sol phase) in
which cilia recover from their active beat and (2) an outer, more
viscous layer (ie, gel phase), which is transported by the ciliary
beat. Proper balance between the inner sol phase and outer gel
phase is of critical importance for normal mucociliary clearance.
If the composition of mucus is changed, so that the mucus produced
is more viscous (eg, as in cystic fibrosis), transport toward the
ostia considerably slows, and the gel layer becomes demonstrably
thicker. This results in a collection of thick mucus that is
retained in the sinus for varying periods. In the presence of a
lack of secretions or a loss of humidity at the surface that cannot
be compensated for by mucous glands or goblet cells, the mucus
becomes increasingly viscous, and the sol phase may become
extremely thin, thus allowing the gel phase to have intense contact
with the cilia and impede their action. Overproduction of mucus can
overwhelm the mucociliary clearance system, resulting in retained
secretions within the
sinuses.http://emedicine.medscape.com/article/232670-overview#a4Colds,
bacterial infections, allergies, asthma, and other health
conditions can cause sinusitis. Acute Sinusitis Acute sinusitis
usually is caused by a viral or bacterial infection. The common
cold, which is caused by a virus, may lead to swelling of the
sinuses, trapping air and mucus behind the narrowed sinus openings.
Both the nasal and the sinus symptoms usually go away within 2
weeks. Sometimes, viral infections are followed by bacterial
infections. Many cases of acute sinusitis are caused by bacteria
that frequently colonize the nose and throat, such as Streptococcus
pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis.
These bacteria typically do not cause problems in healthy people,
but in some cases they begin to multiply in the sinuses, causing
acute sinusitis. NIAID supports studies to better understand the
factors that put people at risk for bacterial sinusitis. People who
have allergies or other chronic nasal problems are prone to
episodes of acute sinusitis. In general, people who have reduced
immune function, such as those with HIV infection, are more likely
to have sinusitis. Sinusitis also is common in people who have
abnormal mucus secretion or mucus movement, such as people with
cystic fibrosis, an inherited disease in which thick and sticky
mucus clogs the lungs. Chronic Sinusitis (Rhinosinusitis) In
chronic sinusitis, also known as chronic rhinosinusitis, the
membranes of both the paranasal sinuses and the nose thicken
because they are constantly inflamed. This condition can occur with
or without nasal polyps, grape-like growths on the mucous membranes
that protrude into the sinuses or nasal passages. The causes of
chronic rhinosinusitis are largely unknown. NIAID supports basic
research to help explain why people develop this chronic
inflammation. Most people with sinusitis have facial pain or
tenderness in several places, and their symptoms usually do not
clearly indicate which sinuses are inflamed. The pain of a sinus
attack arises because trapped air and mucus put pressure on the
membranes of the sinuses and the bony wall behind them. Also, when
a swollen membrane at the opening of a paranasal sinus prevents air
from entering into the sinuses, it can create a vacuum that causes
pain. People with sinusitis also have thick nasal secretions that
can be white, yellowish, greenish, or blood-tinged. Sometimes these
secretions drain in the back of the throat and are difficult to
clear. This is referred to as post-nasal drip or post-nasal
drainage. Chronic post-nasal discharge may indicate sinusitis, even
in people who do not have facial pain.However, facial pain without
either nasal or post-nasal drainage is rarely caused by
inflammation of the sinuses. People who experience facial pain but
no nasal discharge often are diagnosed with a pain disordersuch as
migraines, cluster headaches, or tension-type headachesrather than
sinusitis. Less common symptoms of acute or chronic sinusitis
include the following: Tiredness Decreased sense of smell Cough
that may be worse at night Sore throat Bad breath Fever
On very rare occasions, acute sinusitis can result in brain
infection and other serious complications.
3. Mengapa didapatkan hidung tersumbat dan batuknya tidak
berdahak?Hidung tersumbat:Sinus paranasal adalah bagian dari
traktus respiratorius yang berhubungan langsung dengan nasofaring.
Sinus secara normal steril. Dengan adanya obstruksi, flora normal
nasofaringeal dapat dapat menyebabkan infeksi. Bila terjadi edema
di kompleks ostiomeatal, mukosa yang letaknya berhadapan akan
saling bertemu, sehingga silia tidak dapat bergerak dan lendirnya
berhadapan akan saling bertemu, dan lendir tidak dapat dialirkan.
Maka terjadi gangguan drainase dan ventilasi di dalam sinus,
sehingga silia menjadi kurang aktif dan lendir yang diproduksi
mukosa sinus menjadi lebih kental dan merupakan media yang baik
untuk tumbuhnya bakteri patogen. Bila sumbatan berlangsung terus,
akan terjadi hipoksia dan retensi lender, sehingga timbul infeksi
oleh bakteri anaerob. Selanjutnya terjadi perubahan jaringan
menjadi hipertrofi, polipoid atau pembentukan polip dan kista.4.
Mengapa penderita sering mengeluh sakit kepala di sekitar mata?
Sinusitis is an inflammation of the membranes lining the paranasal
sinusessmall air-filled spaces located within the skull or bones of
the head surrounding the nose. Sinusitis can be caused by an
infection or other health problem. Symptoms include facial pain and
nasal discharge, or runny nose. Nearly 30 million adults in the
United States are diagnosed with sinusitis each year, according to
the Centers for Disease Control and Prevention. The paranasal
sinuses comprise four pairs of air-filled spaces: Frontal
sinusesover the eyes in the brow area Ethmoid sinusesjust behind
the bridge of the nose, between the eyes Maxillary sinusesinside
each cheekbone Sphenoid sinusesbehind the ethmoids in the upper
region of the nose and behind the eyes
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes
of Health National Institute of Allergy and Infectious
Diseaseshttps://www.niaid.nih.gov/topics/sinusitis/Documents/sinusitis.pdf
5. Mengapa didapatkan ingus kental?Acute Sinusitis Acute
sinusitis usually is caused by a viral or bacterial infection. The
common cold, which is caused by a virus, may lead to swelling of
the sinuses, trapping air and mucus behind the narrowed sinus
openings. Both the nasal and the sinus symptoms usually go away
within 2 weeks. Sometimes, viral infections are followed by
bacterial infections. Many cases of acute sinusitis are caused by
bacteria that frequently colonize the nose and throat, such as
Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella
catarrhalis. These bacteria typically do not cause problems in
healthy people, but in some cases they begin to multiply in the
sinuses, causing acute sinusitis. NIAID supports studies to better
understand the factors that put people at risk for bacterial
sinusitis. People who have allergies or other chronic nasal
problems are prone to episodes of acute sinusitis. In general,
people who have reduced immune function, such as those with HIV
infection, are more likely to have sinusitis. Sinusitis also is
common in people who have abnormal mucus secretion or mucus
movement, such as people with cystic fibrosis, an inherited disease
in which thick and sticky mucus clogs the lungs.
https://www.niaid.nih.gov/topics/sinusitis/Documents/sinusitis.pdf
6. Mengapa pasien setelah obatnya habis keluhan timbul
kembali?Karena pengobatanya hanya simpotamatis saja.Untuk
mengurangi gejalanya aja. Kerusakan sebenarnya belum teratasi
sehingga pas obatnya abis bisa timbul lagi keluhannya.7. Mengapa
ingus terasa keluar di tenggorokan?Sistem mukosiliar:Pada dinding
lateral hidung terdapat 2 aliran transport mukosiliar dari
sinus.Lendir yg bersala dr sinus anterior bergabung di infundibulum
etmoid disalurkan ke nasoparing di deoan muara tuba
eustachii.Lendir yg berasala dari sinus posterior bergabung di
ressesus spenoethmoidalis dialirkan ke nasoparing di postero
superior muara tuba eustachii. Sinusistis didapati post nasal
drip.THT FK UI8. Pemeriksaan fisik hidung yang dilakukan dan
interpretasinya?Pemeriksaan Sinus ParanasalUntuk mengetahui adanya
kelainan pada sinus paranasal dilakukan inspeksi dari luar,
palpasi, rinoskopi anterior, rinoskopi posterior, transiluminasi,
pemeriksaan radiologic dan sinuskopi,
InspeksiYang diperhatikan adalah adanya pembengkakan pada muka.
Pembengkakan di pipi sampai kelopak mata bawah yang berwarna
kemerah-merahan mungkin menunjukkan suatu sinusitis maksilaris
akut. Pembengkakan di kelopak mata atas mungkin menunjukkan suatu
sinusitis frontalis akut.Sinusitis etmoid akut jarang menyebabkan
pembengkakan ke luar, kecuali bila telah terbentuk abses.
PalpasiNyeri tekan pada pipi dan nyeri ketuk di gigi menunjukkan
adanya sinusitis maksila. Pada sinusitis frontal terdapat nyeri
tekan di dasar sinus frontal yaitu oada bagian medial atap orbita.
Sinusitis etmoid menyebabkan rasa nyeri tekan di daerah kantus
medius.
TransiluminasiTransiluminasi mempunyai manfaat yang terbatas,
hanya dapat dipakai untuk memeriksa sinus maksila dan sinus
frontal, bila fasilitas pemeriksaan radiologiktidak tersedia.Bila
terdapat kista yang besar di dalam sinus maksila, akan tampak
terang pada pemeriksaan transiluminasi, sedangkan pada foto rontgen
tampak adanya perselubungan berbatas tegas di dalam sinus
maksila.Transiluminasi pada sinus frontal hasilnya lebih meragukan.
Besar dan bentuk kedua sinus ini seringkali tidak sama. Gambaran
yang terang berarti sinus berkembang dengan baik dan normal,
sedangkan gambaran yang gelap mungkin hanya menunjukkan sinus yang
tidak berkembang.
Pemeriksaan RadiologikBila dicurigai adanya kelainan di sinus
paranasal,maka dapat dilakukan pemeriksaan radiologik. Posisi rutin
yang dipakai ialah posisi Waters, P.A, dan lateral. Posisi Waters
terutama untuk melihat adanya kelainan di sinus maksila, frontal
dan etmoid. Posisi posterior anterior untuk menilai sinus frontal
dan posisi lateral untuk menilai sinus frontal, sphenoid dan
etmoid.Metode mutakhir yang lebih akurat untuk melihat kelainan
sinus paranasal adalah pemeriksaan CT-scan.
SinuskopiPemeriksaan ke dalam sinus maksila menggunakan
endoskop. Endoskop dimasukkan melalui lubang yang dibuat di meatus
inferior atau di fossa kanina.Dengan sinuskopi dapat dilihat
keadaan di dalam sinus, apakah ada sekret, polip, jaringan
granulasi, massa tumor atau kista, bagaimana keadaan mukosa dan
apakah ostiumnya terbuka.
9. DD ? Often, healthcare providers can diagnose acute sinusitis
by reviewing a persons symptoms and examining the nose and face.
Doctors may perform a procedure called rhinoscopy, in which they
use a thin, flexible tube-like instrument to examine the inside of
the nose. If symptoms do not clearly indicate sinusitis or if they
persist for a long time and do not get better with treatment, the
doctor may order a computerized tomography (CT) scana form of X-ray
that shows some soft tissue and other structures that cannot be
seen in conventional X-raysto confirm the diagnosis of sinusitis
and to evaluate how severe it is. Laboratory tests that a
healthcare professional may use to check for possible causes of
chronic rhinosinusitis include: Allergy testing Blood tests to rule
out conditions that are associated with sinusitis, such as an
immune deficiency disorder A sweat test or a blood test to rule out
cystic fibrosis Tests on the material inside the sinuses to detect
a bacterial or fungal infection An aspirin challenge to test for
AERD. In an aspirin challenge, a person takes small but gradually
increasing doses of aspirin under the careful supervision of a
healthcare professional.
Sinusitis (frontal, ethmoid, maksila,spenoid)Sinusitis Maksila
Sinus maksila disebut juga antrum High-more merupakan sinus
paranasal yang terbesar.1,9 Saat lahir sinus maksila bervolume 6-8
ml, sinus kemudian berkembang dengan cepat dan akhirnya mencapai
ukuran maksimal, yaitu 15 ml saat dewasa dan merupakan sinus yang
sering terinfeksi, oleh karena9: 1. Merupakan sinus paranasal yang
terbesar. 2. Letak ostiumnya lebih tinggi dari dasar, sehingga
aliran sekret (drainase) dari sinus maksila hanya tergantung dari
gerakan silia. 3. Dasar sinus maksila adalah dasar akar gigi
(prosesus alveolaris), sehingga infeksi gigi dapat menyebabkan
sinusitis maksila. 4. Ostium sinus maksila terletak di meatus
medius, di sekitar hiatus semilunaris yang sempit, sehingga mudah
tersumbat.
Sinusitis maksilaris akut biasanya menyusul suatu infeksi
saluran nafas atas yang ringan. Alergi hidung kronik, benda asing,
dan deviasi septum nasi merupakan factor-faktor predisposisi lokal
yang paling sering ditemukan. Deformitas rahang wajah, terutama
palatoskisis, dapat menimbulkan masalah pada anak. Anak-anak ini
cenderung menderita infeksi nasofaring atau sinus kronik dengan
angka insidens yang lebih tinggi. Sedangkan ganguan geligi
bertanggung jawab atas sekitar 10 persen infeksi sinus maksilaris
akut.Gejala infeksi sinus maksilaris akut berupa demam, malaise dan
nyeri kepala yang tak jelas yang biasanya reda dengan pemberian
analgetik biasa aspirin. Wajah terasa bengkak, penuh, dan gigi
terasa nyeri pada gerakan kepala mendadak, misalnya sewaktu naik
atau turun tangga11,15,16. Seringkali terdapat nyeri pipi khas yang
tumpul dan menusuk, serta nyeri pada palpasi dan perkusi. Sekret
mukopurulen dapat keluar dari hidung dan terkadang berbau busuk.
Batuk iritatif non produktif seringkali ada. Selama berlangsungnya
sinusitis maksilaris akut, pemeriksaan fisik akan mengungkapkan
adanya pus dalam hidung, biasanya dari meatus media, pus atau
sekret mukopurulen dalam dalam nasofaring.11,18 Signs dan symptoms
sinusitis maksilaris kronis kongesti hidung, sakit tenggorokan
(dari postnasal), pada sekitar mata pipi atau dahi sakit lunak dan
bengkak, sakit kepala, demam, penciuman berkurang, batuk, sakit
gigi, susah bernafas, mudah lelah. Hal ini di keluhkan lebih dari 1
minggu.
Sinusitis berdasarkan kausanyaSinusitis berdasarkan waktu (akut
atau kronis)There are two basic types of sinusitis: Acute, which
lasts up to 4 weeks Chronic, which lasts more than 12 weeks and can
continue for months or years .
https://www.niaid.nih.gov/topics/sinusitis/Documents/sinusitis.pdf
10. Pemeriksaan penunjang apa yang disarankan?
11. Terapi apa yang diberikan kepada pasien?Acute Sinusitis
Medications can help ease the symptoms of acute sinusitis.
Healthcare providers may recommend pain relievers or
decongestantsmedicines that shrink the swollen membranes in the
nose and make it easier to breathe. Decongestant nose drops and
sprays should be used for only a few days, as longer term use can
lead to even more congestion and swelling of the nasal passages. A
doctor may prescribe antibiotics if the sinusitis is caused by a
bacterial infection.Chronic Rhinosinusitis Chronic rhinosinusitis
can be difficult to treat. Medicines may offer some symptom relief.
Surgery can be helpful if medication fails. Medicine Nasal steroid
sprays are helpful for many people, but most do not get full relief
of symptoms with these medicines. Saline (salt water) washes or
nasal sprays can be helpful because they remove thick secretions
and allow the sinuses to drain. Doctors may prescribe oral
steroids, such as prednisone, for severe chronic rhinosinusitis.
However, oral steroids are powerful medicines that can cause side
effects such as weight gain and high blood pressure if used over
the long term. Oral steroids typically are prescribed when other
medicines have failed. Desensitization to aspirin may be helpful
for patients with AERD. During desensitization, which is performed
under close medical supervision, a person is given gradually
increasing doses of aspirin over time to induce tolerance to the
drug. Surgery When medicine fails, surgery may be the only
alternative for treating chronic rhinosinusitis. The goal of
surgery is to improve sinus drainage and reduce blockage of the
nasal passages. Sinus surgery usually is performed to: Enlarge the
natural openings of the sinuses Remove nasal polyps Correct
significant structural problems inside the nose and the sinuses if
they contribute to sinus obstruction
Although most people have fewer symptoms and a better quality of
life after surgery, problems can reoccur, sometimes even after a
short period of time. In children, problems can sometimes be
eliminated by removing the adenoids. These gland-like tissues,
located high in the throat behind and above the roof of the mouth,
can obstruct the nasal
passages.https://www.niaid.nih.gov/topics/sinusitis/Documents/sinusitis.pdfAntibiotics:d
Amoxicillin often is the drug of choice for childrenand adults. It
is generally effective, inexpensive,and well tolerated.
Trimethoprim-sulfamethoxazolecan be used as an alternative drug in
adults. Resistanceis more commonly seen in children, and it
isrecommended that the clinician refer to their localbiogram
profile of antibiotic resistance. For patientswho do not respond to
amoxicillin, high-doseamoxicillin-clavulanate (90 mg/kg amoxicillin
and6.4 mg/kg clavulanate, not to exceed 2 g every12 hours) is
recommended. For patients allergicto or intolerant of amoxicillin,
alternatives includecephalosporins, macrolides, or quinolones.d
Acute sinusitis generally responds to treatment for10 to 14 days.
Some physicians continue treatmentfor 7 days after the patient is
well to ensure completeeradication of the organism and prevent
relapse.It is important to instruct the patient tocomplete the
course of antibiotics.d A reasonable approach would be to start the
patienton amoxicillin for 3 to 5 days and determinewhether the
signs and symptoms are improving.If the patients symptoms are
improving, continuethis treatment until the patient is well for 7
days(generally a 10- to 14-day course). If after 3 to 5days the
patient has not shown improvement,switch to a different antibiotic,
such as high-doseamoxicillin-clavulanate or cefuroxime
axetil.Corticosteroids:d The use of nasal corticosteroids might be
helpful inpatients with acute and chronic sinusitis.d Although
efficacy has not yet been proved, theshort-term use of oral
corticosteroids as an adjunctin treating patients with acute
sinusitis is reasonablewhen the patient fails to respond to initial
treatment,demonstrates nasal polyposis, or has demonstratedmarked
mucosal edema.Saline-mucolytics:d Saline nasal sprays or lavage
might be a useful adjunctby liquefying secretions and decreasing
therisk of crusting near the sinus ostia.d There is no conclusive
evidence that mucolytics,such as guaifenesin, are useful adjuncts
in treatingacute sinusitis.a-Adrenergic decongestants:d Topical
decongestants (eg,oxymetazolinean dphenylephrine)and oral
decongestants (eg, pseudoephedrine)reduce mucosal blood flow,
decrease tissueedema and nasal resistance, and might
enhancedrainage of secretions from the sinus ostia.d The use of
topical decongestants beyond 3 to 5days might induce rhinitis
medicamentosa, withassociated increased congestion and
refractorinessto subsequent decongestant
therapy.https://www.aaaai.org/Aaaai/media/MediaLibrary/PDF%20Documents/Practice%20and%20Parameters/sinusitis2005.pdf12.
Komplikasi ?Sinusitis does not cause any significant mortality by
itself. However, complicated sinusitis may lead to morbidity and,
in rare cases, mortality.Approximately 40% of acute sinusitis cases
resolve spontaneously without antibiotics. The spontaneous cure for
viral sinusitis is 98%. Patients with acute sinusitis, when treated
with appropriate antibiotics, usually show prompt improvement. The
relapse rate after successful treatment is less than 5%.In the
absence of response within 48 hours or worsening of symptoms,
reevaluate the patient. Untreated or inadequately treated
rhinosinusitis may lead to complications such asmeningitis,
cavernous sinus thrombophlebitis, orbital cellulitis or abscess,
andbrain abscess.In patients with allergic rhinitis, aggressive
treatment of nasal symptoms and signs of mucosal edema, which can
cause obstruction of the sinus outflow tracts, may decrease
secondary sinusitis. If the adenoids are chronically infected,
removing them eliminates a nidus of infection and can decrease
sinus
infection.http://emedicine.medscape.com/article/232670-overview#a7