Embed Size (px)
Citation preview

British Journal of Plastic Surgery (1990), 43, 536-540 0 1990 The Trustees of British Association of Plastic Surgeons
0007-1226/90/0043-05361$10.00
Three anteromedial fasciocutaneous leg island flaps for covering defects of the lower two-thirds of the leg
M. M. EL-SAADI and A. A. KHASHABA
Department of Plastic and Reconstructive Surgery, Zagazig University Hospital, Zagazig, Egypt
Summary-Three different fasciocutaneous island flaps based on the medial septocutaneous vessels of the leg have been successfully transferred in eight patients. The flaps are based on three segments of the anteromedial aspect of the leg where their feeding vessels were most frequently identified. These anteromedial fasciocutaneous leg island flaps are thin, reliable and safe. They are relatively easy to elevate and are useful for covering defects of the lower two-thirds of the leg.
The evolution of fasciocutaneous flaps aroused interest in the vascular anatomy of the superficial planes of the leg (Haertsch, 1981; Barclay et al., 1982; Carriquiry et al., 1985). Most authors recog- nise the presence of a few fasciocutaneous arteries along the main axis of the leg, that originate at the popliteal region and supply the proximal two-thirds of the leg (Haertsch, 1981; Barclay et al., 1982). Musculocutaneous perforators have also been re- cognised and have been the basis for the design of musculocutaneous flaps in the leg as well as elsewhere (McGraw et al., 1977).
Besides these two groups, a third set of vessels, the septocutaneous vessels, have recently been identified. These vessels originate from one of the three main deep pedicles of the leg, i.e. the anterior tibial, posterior tibia1 and peroneal vessels. Carri- quiry et al. (1985) predicted the importance of these vessels as the basis for different kinds of fasciocu- taneous flaps in the leg. They alsoelegantly classified these septocutanous vessels into three groups according to their origin : medial from the posterior tibia1 vessels, anterolateral from the anterior tibia1 vessels, and posterolateral from the peroneal ves- sels.
In this report we present three anteromedial fasciocutaneous leg island flaps based on the medial septocutaneous vessels of the leg that originate from the posterior tibia1 vessels.
Anatomy
The medial septocutaneous vessels originate from the posterior tibia1 vessels and are enclosed in the deep transverse fascial septum of the leg, i.e. the
septum that separates the soleus and gastrocnemius from the deep muscular compartment of the posterior leg. Carriquiry et al. (1985) noticed the uppermost of these vessels to pierce the fascia, passing through the tibia1 origin of the soleus just behind the medial border of the tibia. They also located the lowermost medial septocutaneous ves- sels to become superficial after passing between flexor digitorum longus and soleus muscles and Achilles tendon. Four to five of these vessels were identified and their origin and the points at which they pierce the fascia were quite variable. However, in their description the authors found three seg- ments along the medial side of the leg where these vessels were most frequently found : between 9 and 12 cm, 17 and 19 cm and 22 and 24 cm from the tip of the medial malleolus. The external diameter of these arteries also varied from 0.5 to 1.5 mm, the arteries with a larger diameter being found at the middle third of the leg.
Operative procedure
The dimensions of the defect are measured and the flap is designed in accordance with the size of the defect and the site of the nearest pedicle. Figure 1 shows an example of a flap based on the uppermost pedicle, i.e. between 22 and 24 cm from the tip of the medial malleolus. Raising of the flap starts from its posterior edge in a subfascial plane. The pedicles will appear just before the medial border of the tibia is reached. After identification and dissection of the pedicle, the flap is raised from all its edges. The great saphenous vein will often be encountered at the anterior edge of the flap and an effort should
536

THREE ANTEROMEDIAL FASCIOCUTANEOUS LEG ISLAND FLAPS FOR LOWER TWO-THIRDS OF THE LEG 537
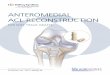
Fig. 1
Figure I-- -(A) Chronic leg ulcer over the shin of the tibia of 2 years’ duration. (B) The defect and a flap based on the uppermost segment (forceps pointing to pedicle). (C)The flap rotated 90’ to cover the defect. (D) The flap inset and sutured and donor site split skin grafted. (I?) Late postoperative view at 2 months.

538
always be made to preserve it. The flap is then transposed to cover the defect (Fig. 1C) and the donor site is split skin grafted (Fig. 1 D).
Materials and methods
Eight flaps for eight patients with chronic leg ulcers admitted to the Department of Plastic and Recon- structive Surgery, Zagazig University Hospital, were performed. Six patients were males and two were females and their ages ranged from 13 to 42 years. All our cases were chronic post-traumatic in aetiology. The duration of the ulcers ranged from 2 to 12 years, with an average of 5 years. The size of the defects ranged from 4 x 6 cm to 7 x 9 cm.
Three cases were situated over the shin of the tibia between the upper and middle thirds of the leg, for which a flap based on the uppermost segment was used. Another three cases were situated at the middle third, for which a flap based on the middle segment was performed. The last two flaps were based on the vessels of the lowermost segment, to cover ulcers in the vicinity of the medial malleolus and over the back of the calcaneum.
BRITISH JOURNAL OF PLASTIC SURGERY
Results
All the eight flaps survived completely and healing was uneventful without even minimal necrosis. From our experience the medial septocutaneous vessels are constant and situated at relatively fixed points, and each vessel was able to support a reliable island flap. The vessels were in the order of 0.5-1.5 mm in diameter. Figures 1, 2 and 3 respectively show a representative of a flap based on the upper, middle and lower segments.
In two of the three flaps based on the vessels of the uppermost segment, the vascular pedicle was identified at a distance of 22 cm from the tip of the medial malleolus, and in one flap the pedicle was found 23 cm from the same point. In the other three flaps based on the septocutaneous vessels of the middle segment, the pedicle was found at a distance of 18 cm from the tip of the medial malleolus. As for the two flaps based on the pedicle of the lowermost segment, the vessels were identi- fied at a distance of 10 cm from the tip of the medial malleolus.
The angle of rotation was around 90” in middle third defects (Fig. l), 120” in lower lesions (Fig. 2) and 160” for the flap used to cover the back of
Fig. 2
Figure Z-(A) Chronic post-traumatic leg ulcer of 3 years’ duration. (B) A flap based on the middle segment covering the defect. (C) Early postoperative view. (D) Late postoperative view of flap donor site.

THREE ANTEROMEDIAL FASCIOCUTANEOUS LEG ISLAND FLAPS FOR LOWER TWO-THIRDS OF THE LEG 539
Fig. 3
Figure &(A) Chronic post-traumatic ulcer of back of calcaneum of 12 years’ duration. (B) The extent of excision and the design of a flap based on the lowermost segment. (C) Immediate postoperative view. (D) The flap and donor site 2 months later

540
calcaneum (Fig. 3). In this last flap a strip of skin about 2 cm wide from donor site to defect was excised to accommodate the flap. Excision of this bridge segment of unaffected tissue was advanta- geous in allowing space for postoperative oedema.
The patients were fully satisfied and up and about within a short period of time. Average hospitalisa- tion time was one week.
Discussion
Credit goes to Ponten in 1981 who was the first to introduce us to fasciocutaneous flaps and start a new era in “simple” reconstruction of lower limb defects. His early design along the vertical axis of the leg with a proximal pedicle has been modified by the use of transverse flaps with a lateral or medial pedicle (Thatte, 1982). Still later, as courage developed, flaps with a distal pedicle started to appear in the literature (Donski and Fogdestam, 1983).
Amarante et al. (1986) dissected 10 cadavers to look for anastomotic arteries from the posterior tibia1 artery. They always found two perforating cutaneous arteries and accompanying veins at about 4 cm and 6.5 cm above the medial malleolus. The authors described a distally based fasciocuta- neous flap which was used successfully in four patients.
The safety with which fasciocutaneous flaps of the lower limb could be islanded has only relatively recently been demonstrated (Walton and Bunkis, 1984; Moscona et al., 1985). Fasciocutaneous free flap units harvested from the posterior calf region and based on a descending subfascial branch of the popliteal artery have also been reported with success (Walton and Bunkis, 1984). Torii et al. (1987), in a communication comparable to ours, reported a fasciocutaneous island flap based on the anterola- teral septocutaneous vessels of the leg that was used in three patients. Their flap was useful for covering the knee and the upper half of the leg.
In this report we present our experience with three anteromedial fasciocutaneous leg island Saps based on the medial septocutaneous vessels of the leg. These three flaps clearly exhibit the following advantages :
1. The flaps are thin, reliable and easy to elevate. 2. Based on the three segments described, almost
any site in the lower two-thirds of the leg, including the difficult areas of the back of calcaneum and Achilles tendon, can be covered.
BRITISH JOURNAL OF PLASTIC SURGERY
The pedicles are constant and situated at relatively fixed points that are easily visualised and each of them can support an island flap effectively. The arc of rotation is extensive and the flaps can be made to fit the defect exactly and comfortably without axial tension or kinking. Operative time and donor site morbidity are kept to a minimum and the patient remains conveniently supine during the operation.
References
Amarante, J., Costa, H., Reis, J. and Soares, R. (1986). A new distally based fasciocutaneous flap of the leg. British Journal of Plastic Surgery, 39,338.
Barclay, T. L., Cardoso, E., Sharpe, D. T. and Crockett, D. J. (1982). Repair of lower leg injuries with fasciocutaneous flaps. British Journal of Plastic Surgery, 35, 127.
Carriqoiry, C., Costa, M. A. and Vasconez, L. 0. (1985). An anatomic study of the septocutaneous vessels of the leg. Plastic and Reconstructive Surgery, 76,354.
Donski, P. K. and Fogdestam, I. (1983). Distally based fasciocu- taneous flap from the sural region. A preliminary report. Scandinavian Journal of Plastic and Reconstructive Surgery, 17, 191.
Haertsch, P. (1981) The surgical plane of the leg. British Journal of Plastic Surgery, 34,464.
McGraw, J. B., Dibbell, D. G. and Carraway, J. H. (1977). Clinical definition of independent myocutaneous vascular territories. Plastic and Reconstructive Surgery, 60, 341.
Moscona A. R., Govrin-Yehudaia, J. and Hirschowitz, B. (1985). The island fasciocutaneous flap: a new type of flap for defects of the knee. British Journal of Plastic Surgery, 35,s 12.
Ponten, B. (1981). The fasciocutaneous flap: its use in soft tissue defects of the lower leg. British Journal qfPIastic Surgery, 34, 215.
Thatte, R. L. (1982). One-stage random-pattern de-epithelialised “turn-over” flaps in the leg. British Journal of Plastic Surgery, 35,281.
Torii. S., Namiki, Y. and Hayashi, Y. (1987). Anterolateral leg island flap. British Journal af Plastic Surgery, 40,236.
Walton, R. L. and Bunkis, J. (1984). The posterior calf fasciocutaneous free flap. Plastic and Reconstructive Surgery. 74,x.
The Authors
M. M. El-Saadi, MD, Lecturer in Plastic Surgery A. A. Khashaha, MD, Lecturer in Plastic Surgery
Department of Plastic and Reconstructive Surgery, Zagazig University Hospital, Zagazig, Egypt.
Requests for reprints to: Dr Ahmed Khashaba, MD, 4 Dr Ahmed Nada St., Heliopolis, Cairo, Egypt.
Paper received 23 November 1989. Accepted 9 April 1990 after revision.