Embed Size (px)
Citation preview
The Transformation The Transformation of the American of the American HospitalHospital
James G. Anderson, Ph.D.James G. Anderson, Ph.D.
Purdue UniversityPurdue University
From Community Institution From Community Institution to Business Organizationto Business Organization
Institutions are infused with values reflecting Institutions are infused with values reflecting community sentiments and goals. They also community sentiments and goals. They also perform a variety of social functions that are perform a variety of social functions that are viewed as important for the community. viewed as important for the community.
Organizations represent rational instruments Organizations represent rational instruments designed to achieve definite goals judged on designed to achieve definite goals judged on technical criteria that can be modified or technical criteria that can be modified or discarded. discarded.

Late 19Late 19thth Century Hospitals Century Hospitals
Founded as institutionsFounded as institutions Concern for the poorConcern for the poor Mutual assistanceMutual assistance VolunteerismVolunteerism Community sponsorshipCommunity sponsorship Community service versus investor returnCommunity service versus investor return

2020thth Century Hospitals Century Hospitals
Shift from donation of services to Shift from donation of services to marketing servicesmarketing services
Financing expansionFinancing expansion Profit-making activitiesProfit-making activities Competition for paying patientsCompetition for paying patients Community orientation diminishedCommunity orientation diminished Ascendance of organizational modelAscendance of organizational model Hospital mergers/closuresHospital mergers/closures

Institutions of CareInstitutions of Care (1750-1870)(1750-1870)
MDs donated their timeMDs donated their time Benefactors provided capitalBenefactors provided capital Hospital provided care vs. cureHospital provided care vs. cure Rudimentary treatment availableRudimentary treatment available

Institutions of CareInstitutions of Care (1870-1919)(1870-1919)
Shift in demand and supplyShift in demand and supply IndustrializationIndustrialization ImmigrationImmigration UrbanizationUrbanization Family fragmentationFamily fragmentation Technology developmentsTechnology developments
Antisepsis and anesthesiaAntisepsis and anesthesia Risk of deaths in hospitals declinedRisk of deaths in hospitals declined Middle class began paying for careMiddle class began paying for care
Institutions of CareInstitutions of Care (1870-1919)(1870-1919)
Number of hospitals increased from 138 to Number of hospitals increased from 138 to 4,3594,359
Number of hospital beds increased from Number of hospital beds increased from 35,604 to 421,005.35,604 to 421,005.
% white collar patients increased from 13% % white collar patients increased from 13% to 24%.to 24%.
% paying patients increased from 14% to % paying patients increased from 14% to 38%.38%.
Institutions of CareInstitutions of Care (1870-1919)(1870-1919)
Mission changed from caring to curing.Mission changed from caring to curing. Patients became viewed as a source of income. Patients became viewed as a source of income. Hospitals remained nonprofit and tax-exempt.Hospitals remained nonprofit and tax-exempt. Hospitals began to serve the broader community.Hospitals began to serve the broader community. Hospitals were founded by religious and ethnic Hospitals were founded by religious and ethnic
groups.groups. Shift in control of the hospital from lay trustees to Shift in control of the hospital from lay trustees to
medical staff. medical staff. Majority of care shifted to private paying patients. Majority of care shifted to private paying patients.

Threats to the Institution Threats to the Institution (1930-1965)(1930-1965)
Major changes:Major changes:
The development of private health insurance. The development of private health insurance. Growing government involvement in financing and Growing government involvement in financing and
regulation.regulation.
Alteration in the institutional character of hospitals.Alteration in the institutional character of hospitals.

Private InsurancePrivate Insurance The depression resulted in the founding of Blue The depression resulted in the founding of Blue
Cross/Shield. They acted as third-party between Cross/Shield. They acted as third-party between patients and providers.patients and providers.
Insurance plans were nonprofit.Insurance plans were nonprofit. They did not interfere with clinical decisions.They did not interfere with clinical decisions. Free choice of hospitals by patients.Free choice of hospitals by patients. Providers were reimbursed for charges on a fee-Providers were reimbursed for charges on a fee-
for-service basis.for-service basis. Community-based rating was used to set Community-based rating was used to set
insurance premiums. insurance premiums.
Private InsurancePrivate Insurance WWII wage/price controls encouraged WWII wage/price controls encouraged
employers to offer health insurance benefits. employers to offer health insurance benefits. The supreme court ruled that the health The supreme court ruled that the health
insurance was negotiable in collective insurance was negotiable in collective bargaining. bargaining.
The development of competition from The development of competition from commercial insurance forced BlueCross/Blue commercial insurance forced BlueCross/Blue Shield to abandon community rating. Shield to abandon community rating.
Insurance spurred higher utilization and cost. Insurance spurred higher utilization and cost.

Government Involvement Government Involvement Medicare/Medicaid 1965:Medicare/Medicaid 1965:
Increase the federal government’s role to fill gaps Increase the federal government’s role to fill gaps in private insurance.in private insurance.
Government provided capital for health services.Government provided capital for health services. Reimbursed physicians on a fee-for-service basis.Reimbursed physicians on a fee-for-service basis. Reimbursed hospitals on a retrospective cost- Reimbursed hospitals on a retrospective cost-
reimbursement basis.reimbursement basis. Provided higher payments for inpatient care.Provided higher payments for inpatient care. Provided incentives to expand facilities and Provided incentives to expand facilities and
services.services.

Effects of Government Effects of Government InvolvementInvolvement
Health care inflation.Health care inflation. Dependence on public funds.Dependence on public funds. Reduction in philanthropy.Reduction in philanthropy. Providers reduce charity care. Providers reduce charity care. Regulation increased.Regulation increased. Hospitals expanded their managerial Hospitals expanded their managerial
responsibilities and staff.responsibilities and staff. Reemergence of for-profit hospitals. Reemergence of for-profit hospitals.

Institutional Crises Institutional Crises 1965-19901965-1990
Stagflation in the 1970s created a budget Stagflation in the 1970s created a budget crisis.crisis.
Spending on Medicare/Medicaid Spending on Medicare/Medicaid increased rapidly.increased rapidly.
Legal, budgetary, market remedies were Legal, budgetary, market remedies were proposed.proposed.
Proposed RemediesProposed Remedies
Legal: Goldfarb vs. Virginia State Bar Legal: Goldfarb vs. Virginia State Bar ruled antitrust laws apply to health care.ruled antitrust laws apply to health care.
Budgetary: DRGs changed the way Budgetary: DRGs changed the way hospitals are reimbursed.hospitals are reimbursed.
Market: HMO Act 1973 provided capital Market: HMO Act 1973 provided capital for new HMOs.for new HMOs.
Managed care strategies by employers, Managed care strategies by employers, Medicare, Medicaid.Medicare, Medicaid.

Organizational ResponsesOrganizational Responses
Hospital closures.Hospital closures. Emphasis on commercial objectives.Emphasis on commercial objectives. Abandonment of costly services, charity Abandonment of costly services, charity
care.care. Early discharge of patients.Early discharge of patients. Focus on profitable services.Focus on profitable services. Corporate rationalization.Corporate rationalization. Increased competition.Increased competition.
Decline in Institutional Decline in Institutional CharacterCharacter Decline in community control.Decline in community control. Decline in community legitimacy.Decline in community legitimacy. Loss of philanthropic support.Loss of philanthropic support. Decline in volunteerism. Decline in volunteerism. Increase in unionsIncrease in unions Providers lost initiative for assuring quality, Providers lost initiative for assuring quality,
disciplining members.disciplining members. Responsibility shifted to courts and Responsibility shifted to courts and
payers.payers.

The Future of HospitalsThe Future of Hospitals As an institution hospitals served several As an institution hospitals served several
constituencies:constituencies: (1) Local community (1) Local community
(2) Sick poor. (2) Sick poor. (3) Sponsors who donated time and (3) Sponsors who donated time and
money. (4) Work force drawn mainly from money. (4) Work force drawn mainly from community. community.
Hospitals now focus on serving those who pay Hospitals now focus on serving those who pay for health care. They have become for health care. They have become organizationsorganizations
The Future of HospitalsThe Future of Hospitals
As the hospital has pursued strategies to As the hospital has pursued strategies to improve the operating margin/bottom line, it has improve the operating margin/bottom line, it has lost its traditional legitimacy.lost its traditional legitimacy.
Revenue-generating strategies will not ensure Revenue-generating strategies will not ensure the hospital’s survival in the future.the hospital’s survival in the future.
Various physician specialty groups have Various physician specialty groups have become less dependent upon hospitals as a become less dependent upon hospitals as a site of practice. This has drawn patients away. site of practice. This has drawn patients away.
Hospitals have become large ICUs. Hospitals have become large ICUs.

Number and Types of Number and Types of Hospitals in the U.S.Hospitals in the U.S.
Total Number of All U.S. Total Number of All U.S. RegisteredRegistered* * Hospitals Hospitals 5,7645,764
Number of U.S. Number of U.S. CommunityCommunity** Hospitals 4,895 ** Hospitals 4,895 Number of Nongovernment Not-for-Profit Number of Nongovernment Not-for-Profit
CommunityCommunity Hospitals 2,984 Hospitals 2,984 Number of Investor-Owned (For-Profit) Number of Investor-Owned (For-Profit)
CommunityCommunity Hospitals 790 Hospitals 790 Number of State and Local Government Number of State and Local Government
CommunityCommunity Hospitals 1,121 Hospitals 1,121

The Changing Environment ofUS Hospitals
• Hospital industry of 1980s: – largely autonomous – worried about government regulation and rate setting • Hospital industry of 1990s: – losing power to managed care – facing public and private payment constraints • Hospital industry of 2000s: – largely consolidated but bifurcated; some doing exceedingly well and others not
Looking Back to 1980s – WhatWe Thought Would Happen• Paul Starr in The Social Transformation ofAmerican Medicine (1982) described the future ofthe hospital industry.

Looking Back to 1980s – WhatWe Thought Would Happen
• Paul Starr in The Social Transformation of American Medicine (1982) described the future of the hospital industry.

Pathways to Regional/ NationalHealth Care Conglomerates
• Changes in hospital ownership to for-profit • Horizontal integration through the development of multi-hospital systems • Diversification and corporate restructuring into “poly-corporate” enterprises • Vertical integration into HMOs • Increased industry concentration of ownership and control Source
Key Questions
• What came to pass and what did not in Starr predictions for hospital industry? • What does this mean for the hospital industry and markets today? • How has this affected hospital financial circumstances?
Horizontal Integration ofHospitals
• Hospitals are increasingly part of multihospital arrangements: – 30.8% were in systems in 1979 – 53.6% were in systems in 2001 with an additional 12.7% in looser health networks • However, systems are still predominantly non-profit and are local in focus

Number and Types of Number and Types of Hospitals in the U.S.Hospitals in the U.S.
Number of Federal Government Hospitals 239 Number of Federal Government Hospitals 239
Number of Nonfederal Psychiatric Hospitals Number of Nonfederal Psychiatric Hospitals 477 477
Number of Nonfederal Long Term Care Number of Nonfederal Long Term Care Hospitals 130 Hospitals 130
Number of Hospital Units of Institutions (Prison Number of Hospital Units of Institutions (Prison Hospitals, College Infirmaries, Etc.) 23 Hospitals, College Infirmaries, Etc.) 23
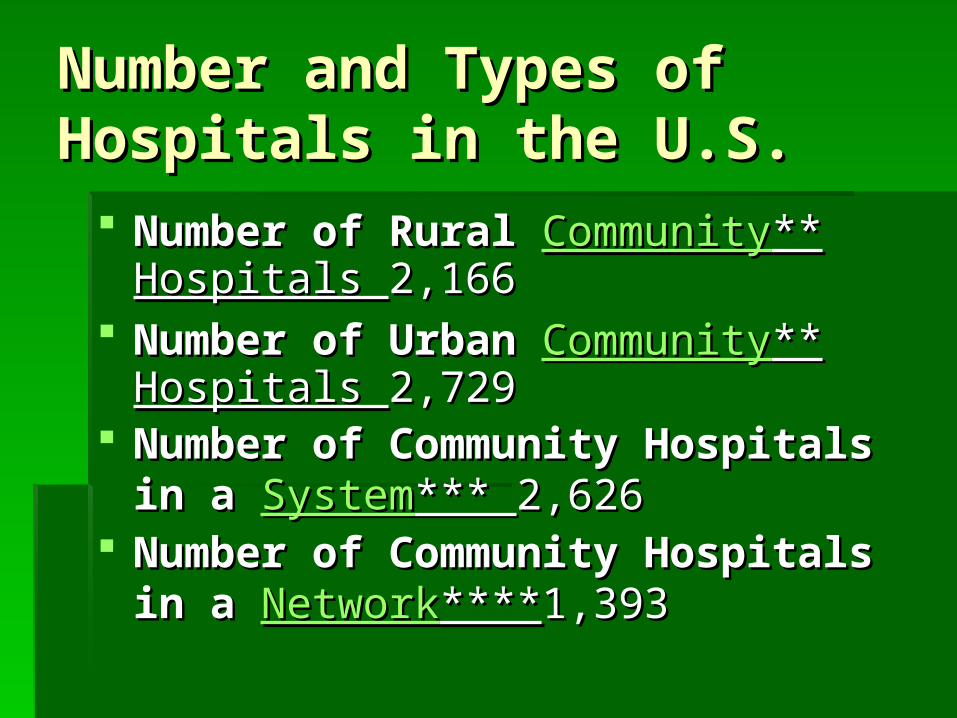
Number and Types of Number and Types of Hospitals in the U.S.Hospitals in the U.S.
Number of Rural Number of Rural CommunityCommunity** Hospitals ** Hospitals 2,1662,166
Number of Urban Number of Urban CommunityCommunity** ** Hospitals Hospitals 2,729 2,729
Number of Community Hospitals in a Number of Community Hospitals in a SystemSystem*** *** 2,6262,626
Number of Community Hospitals in a Number of Community Hospitals in a NetworkNetwork********1,3931,393

Hospital Beds, Hospital Beds, Admissions and ExpensesAdmissions and Expenses
Total Staffed Beds in All U.S. Total Staffed Beds in All U.S. RegisteredRegistered* Hospitals * Hospitals 965,256 965,256
Staffed Beds in Staffed Beds in CommunityCommunity** Hospitals 813,307** Hospitals 813,307 Total Admissions in All U.S. Total Admissions in All U.S. RegisteredRegistered* Hospitals * Hospitals
36,610,535 36,610,535 Admissions in Admissions in CommunityCommunity** Hospitals 34,782,742** Hospitals 34,782,742 Total Expenses for All U.S. Total Expenses for All U.S. RegisteredRegistered* Hospitals * Hospitals
$498,103,754,000 $498,103,754,000 Expenses for Expenses for CommunityCommunity** Hospitals ** Hospitals
$450,124,257,000 $450,124,257,000
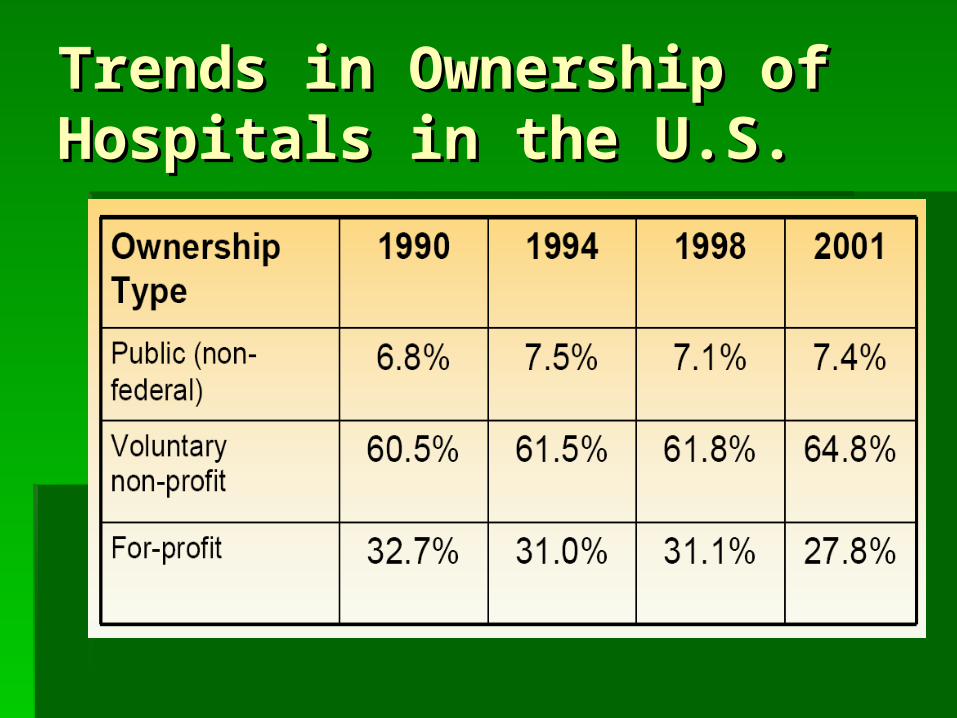
Trends in Ownership of Trends in Ownership of Hospitals in the U.S.Hospitals in the U.S.

Hospital Diversification:Prediction
• Many predicted hospitals would get involved with several different health and non-health related ventures: – outpatient services such as dialysis – nursing homes, retirement centers – retail pharmacies – durable medical equipment distributors – hearing aid and eyeglass stores – managing & leasing medical office space – management consulting services – real estate management

Hospital Diversification:Reality
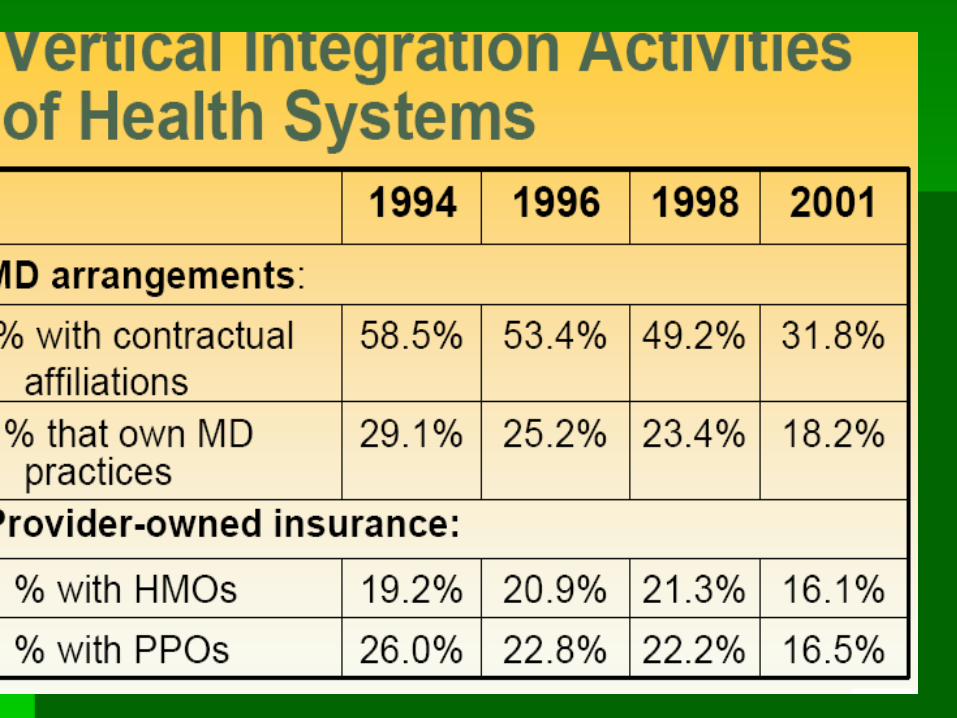
• Hospitals experimented but increasingly focused on services closely tied to traditional inpatient/outpatient care • Hospitals added and dropped services largely depending on reimbursement opportunities • Hospital strategy currently focuses on being a technology leader in a market not being a diversified corporation Vertical

Concentration of Ownershipand Control
• Prediction: Multi-hospital systems would centralize not only ownership but control – Starr believed that shift in locus of control would occur as national/regional systems formed • Reality: Research indicates: – most systems are local not regional or national – about 70% of systems delegate certain authorities to affiliated hospitals – substantial variability exists in mixture of centralized/decentralized control

Why Were So ManyPredictions Wrong?
• Assumed pressures on hospitals would be unrelenting and uni-directional • Did not consider increased ability of hospitals to fend off pressures as they consolidated • Did not recognize extent of organizational inertia • Did not recognize the importance of local connections • Did not realize the resilience of non-profit form even in face of financial distress

So What Does HospitalIndustry Look Like Now?
• Many hospitals are consolidated in local health systems or networks • Systems and networks vary markedly in degree of centralized control: – at one extreme, parent organization establishes all policy and makes all key decisions – at other extreme, system/network is basically a “shell”, perhaps centralized administrative functions and centralized capital financing • A large minority of hospitals not involved, either by choice or because undesirable
Concentration of Ownership and Control • Prediction: Multi-hospital systems would centralize not only ownership but control – Starr believed that shift in locus of control would occur as national/regional systems formed • Reality: Research indicates: – most systems are local not regional or national – about 70% of systems delegate certain authorities to affiliated hospitals – substantial variability exists in mixture of centralized/decentralized control
ReferenceReference
L.R. Burns, “The Transformation of the L.R. Burns, “The Transformation of the American Hospital: From Community American Hospital: From Community Institution toward Business Enterprise”, in Institution toward Business Enterprise”, in Comparative Social ResearchComparative Social Research, , C. Calhoun (ed.), JAI Press, Inc., Vol. 12 C. Calhoun (ed.), JAI Press, Inc., Vol. 12 (1990), pp. 77-112. (1990), pp. 77-112.