Embed Size (px)
Citation preview

THE PROPHYLACTIC REQUIREMENT AND THETOXICITY OF VITAMIN D
COMMITTEE ON NUTRITION
512
PEDIATRICS, March 1963
I T Is NOW more than 40 years since Sir
Edward Mellanby1 demonstrated that
cod liver oil would prevent rickets. Since
this discovery, rickets due to vitamin D
deficiency, once a serious pediatric problem
in temperate climates, has become a com-
paratively rare clinical entity throughout
the civilized world. Nonetheless, cases of
deficiency rickets still occur in the United
23 Canada,4 Great Britain,5 and else-
where.
In temperate climates, sunlight cannot be
relied upon to provide year-round protec-
tion from rickets in infancy and early child-
hood, and vitamin D must be provided from
other sources. Until recently, the intakes of
vitamin D recommended by official organ-
izations in a number of countries could only
he achieved by administration of oral vita-
mm D supplements, since the normal diet
(even one including butter, milk, and egg
yolk) contained relatively little vitamin D.
Today, however, the situation is greatly
altered, at least in such countries as the
United States, Canada, and Great Britain.
Because the addition of supplemental vita-
mm D to various foods is sanctioned, mdi-
viduals of all ages now receive variable and
sometimes considerable amounts of vitamin
D from pasteurized, evaporated, on pow-
dered milk, margarine, certain ready-to-eat
cereals, and a variety of other foodstuffs. In-
deed, in the United States and Canada there
is now a reasonable likelihood that the in-
dividual, even the small infant, may receive
the total recommended allowance of vitamin
D from an average diet; in some instances
he will receive considerably more than the
recommended intake even when no vitamin
supplement is given.
It is well known tilat vitamin D produces
serious toxic effects if consumed for a period
in grossly excessive amounts. In addition,
ADDRESS: 1801 Hinman Avenue, Evanston, Illinois.
however, vitamin D, in amounts not much
greater than the recommended allowance,
has been incriminated as one of the fac-
tons in the pathogenesis of idiopathic hy-
percalcemia of infancy, and in this respect
even small excesses of vitamin D may oc-
casionally be injurious. Whereas in tile past
it was frequently the practice to administer
doses of vitamin D in excess of the recom-
mended allowance with the object of pro-
viding an extra measure of nutritional
safety, it is now evident that all those con-
cerned with the optimal nutrition of the
population must bear in mind the possible
untoward effects of vitamin D prescribed
for prophylaxis. This, in turn, demands that
closer attention be paid to the total intake
of vitamin D, a task that is becoming in-
creasingly difficult as each new “fortified”
food is introduced onto the market.
In the report that follows, the Committee
on Nutrition of the American Academy of
Pediatrics summarizes the evidence regard-
ing the prophylactic requirement and tile
toxicity of vitamin D, and presents certain
recommendations for use of the vitamin.
THE REQUIREMENT OF VITAMIN D
AT VARIOUS AGES
Vitamin D is believed to function in mi-
nute concentrations by regulating or po-
tentiating certain complex biochemical re-
actions at various sites in the body. The
amount necessary to achieve optimal phys-
iologic function in a given individual is de-
pendent upon a number of factors, among
which are believed to be age, rate of
growth, efficiency of intestinal absorption
(especially of fat), and coexisting disease,
but little is known concerning the influence
of these factors.
From the sections that follow, it will be
apparent that vitamin D is an essential fac-
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

COMMITFEE ON NUTRITION 513
tor in the metabolism of the growing hu-
man being, and, indeed, probably at all
ages. For the llealthy premature and full-
term infant, fairly reliable estimates of the
minimal requirements have been made.
This has been possible in pant because the
newborn infant develops evidence of vita-
mm D deficiency relatively rapidly, and in
part because, by selecting for study infants
born in the autumn, the otherwise undefin-
able amount of vitamin D contributed by
sunlight can justifiably be neglected. The
minimal requirements during later child-
hood, adolescence, adulthood, pregnancy,
and lactation have been much more difficult
to determine because sources of vitamin D
become more accessible and more varied,
because rickets rarely develops after in-
fancy, and because other satisfactory en-
tenia of minimal vitamin D deficiency have
not yet been established.
In early years there was much disagree-
ment regarding the relative efficacies of the
various forms of vitamin D. It is now be-
lieved that, microgram for microgram, vita-
mm D2 (calciferol) and vitamin D3 (ir-
radiated 7-dehydrocholesterol) have equal
potencies in the human.6 Ordinarily, vitamin
D is almost completely absorbed by the in-
testine, and the vehicle in which the vita-
mm is administered (be it oil, aqueous sus-
pension, milk, or other food) is believed not
to affect absorption7 unless the intestinal
absorption of fat is impaired. In children
with steatorrhea, the finely dispersed, water-
miscible preparations are thought to be pref-
enable on the basis of indirect evidence ob-
tamed from vitamin A absorption u#{176}
The Normal Full-term Infant
Numerous studies, most of them con-
ducted some 20 on 30 years ago, have con-
cerned the efficacy of various amounts of
vitamin D in preventing rickets,7’ 10-12 in pro-
moting intestinal absorption of 14
and in promoting linear � 16
On the basis of the above criteria, esti-
mates of minimal vitamin D requirement
range from approximately 100 U.S.P.
711 12 to approximately 400 U.S.P. units
per day’#{176}’16(1 U.S.P. unit = 1 I.U.). Doses
of vitamin D greater than 400 I.U. per day
did not result in a greaten degree of pro-
tection against 710 11 and did not
further increase retention of 14
Although there is not complete agreement
on the minimal requirement of vitamin D
to promote maximal linear growth (or even
whether vitamin D effects linear growth),
it would appear that intakes of 250 I.U.
daily are at least as effective as greater in-
takes.12, 16
Many of these early studies are now open
to question from the standpoint of modern
experimental design. However, the observa-
tion that intakes of 300 to 500 I.U. of vita-
mm D pen day resulted in rapid healing of
severe 710 provides strong evidence
concerning the probable effectiveness of the
doses proposed for prophylaxis.
The formerly high incidence of rickets
among Negro infants living in the large
metropolitan areas of the northern United
States gave rise to the impression that sun-
shine was less effective in preventing
rickets in individuals with deeply-pig-
mented skins; however, sociologic factors
made tllis difficult to prove. On the other
hand, data in the American literature sup-
ports the opinion that the amount of in-
gested vitamin D required to �
or to cure1#{176}rickets in Negro infants does
not differ from the requirements of white
infants.
The manner in which other factors, such
as chronic infection, metabolic disease, and
rapid skeletal growth influence vitamin D
requirement is not yet accurately known. In
particular, there has been argument re-
ganding the relation between calcium intake
and vitamin D requirement. Clearly, it is
necessary to provide sufficient dietary cal-
cium to meet the requirements of the grow-
ing skeleton. Similarly, sufficient vitamin D
must be provided to prevent rickets and to
promote satisfactory calcium retention.
However, having satisfied the minimum
needs in these two respects, there is no
reason to postulate any specific relation be-
tween D requirement and calcium intake.
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

514 VITAMIN D
This principle is of special importance in
considering the vitamin dosage of the
breast-fed infant, since, per calorie, the cal-
cium content of human milk is approxi-
mately one-third to one-quarter that of a
cow’s milk formula.17 However, both from
theoretical considerationsl8 and practical
observation, the calcium requirements of the
normal full-term infant are satisfactorily
met by human milk, and there is no reason
to increase the prophylactic dose of vitamin
D to more than 400 I.U. per day for the
breast-fed infant.
In many parts of Europe, the custom of
giving daily vitamin supplements to babies
has never been established. In these regions,
it is the practice to administer to infants,
usually under direct medical supervision,
single large oral or intramuscular doses
(Stossen) of vitamin D at intervals. mdi-
vidual doses of 300,000 I.U. at intervals of
l,� to 3 months have been suggested.’9 The
Committee endorses the view of Lightwood
and Stapleton2#{176} that such administration of
vitamin D is unphysiologic and has no use-
ful place in countries where daily vitamin
D prophylaxis has become established prac-
tice.
The Premature Infant
Although the various techniques used to
determine the vitamin D requirement of
full-term infants have been applied to pre-
mature infants, it has been more difficult to
establish the requirement. In part at least,
this has been because of the relatively
greater requirement for calcium. The skele-
ton of tile infant born 6 weeks prematurely
contains approximately half as much cal-
cium as that of the full-term infant.21
Cleanly, it is axiomatic that the premature
infant should be given sufficient calcium to
satisfy the needs of the rapidly growing
skeleton. Since the average accretion of
calcium during the last 2 months of fetal life
has been estimated at approximately 200
mg per day,18 an intake of calcium that
will permit retention of this amount must
be provided. The relatively low calcium
content of human milk makes such reten-
tion unlikely, even when the intake of vita-
mm D is sufficient to permit maximal intes-
final absorption. Disregard of this principle
by early investigators22 may explain the
statement that premature infants frequently
developed rickets when receiving intakes of
vitamin D as great as 5,000 lU. per day.
More recent studies in which large groups
of formula-fed premature infants were ob-
served clinically, roentgenographically, and
biochemically indicate that rickets could
usually be prevented and normal calcium
and phosphorus homeostasis maintained
with vitamin D intakes as low as 100 to 200
I.U. per day.12 23 Rates of growth in body
length are reported to have been as rapid
with intakes of 100 to 200 I.U. daily as
with intakes of 400 to 1,200 I.U. 23
Recent studiesl4 ne-emphasize tile necessity
of commencing vitamin D prophylaxis with-
in the first 2 weeks of life.
The Pre-school and School Child
There is no doubt that vitamin D is re-
quired beyond infancy, since nutritional
rickets occurs occasionally in older chil-
525 However, the requirement of vita-
mm D is more difficult to ascertain at this
age than in infancy because of the slower
rate of skeletal growth, the greater oppor-
tunity to ingest foods fortified with vitamin
D, and the tendency to receive more ex-
posure to sunlight. Because clear-cut evi-
dence of rickets occurs so rarely beyond in-
fancy, this manifestation cannot be em-
ployed as a dependable index by which to
determine vitamin D requirement in this
age group. On the basis of unpublished cal-
cium retention studies, Stearns estimated
that the requirement of growing children is
of the order of 400 I.U. per day.26 There is
no question that this intake provides an am-
pie supply of vitamin D for normal children.
However, it should be recalled that before
the current trend toward widespread vita-
mm D enrichment of food, a balanced diet
and outdoor play practically always pro-
vided sufficient vitamin D to prevent de-
tectable evidence of vitamin D deficiency
even though, in a great many instances, the
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

TABLE I
RECOMMENDED DIETARY ALLOWANCES FOR
VITAMIN D, (1.U./DAY)
Age Group
Infants
Premature0-24 mo
Children
�-1Q yr
Adolescents (male &female)
13-19 yr
Adults
Male
Female
NonpregnantPregnancy. lot half
Pregnancy, 2nd half
Lactation
U.S.A.#{176}
400
400
400
400
400
400
Canadat
400-800
400
400
400�
400
400
Great
Britain
. . (8001)
800 (400jJ)
400
400
400
600
800
0 Total daily vitamin 1) intake to maintain good nutrition in
healthy persons (not only in the average person but in substantiallyall normal persons) in the United States under current conditions of
living. The recommendation is meant to afford a margin of sufficiencyabove minimal requirements and to provide a buffer against addedneeds of various stresses other than disease or nutrient repletion.(Food and Nutrition Board. National Academy of Sciences-National Research Council; Recommended Dietary Allowances;1958; Publication 589, Washington, D.C.)
t Recommended total daily vitamin D intake to maintain goodnutrition of healthy persons and to provide a margin of safety.(Canadian Bulletin on Nutrition; A Dietary Standard for Canada;Vol. 3, No. 2, Ottawa, August. 1938.)
� Total daily vitamin D intake “believed sufficient to establishand maintain a good nutritional state in representative individuals
of the groups concerned. It is recognized that in every group theremust be cases where the need is greater than that of the average.”(British Medical Association; Nutrition Committee; Report; 1930,London.)
I Recommendation of Medical Research Council Conference onHypercalcaemia in Infants (1936). Not published. Quoted in Refer-
ence 5.!l Recommendation of Joint Sub-committee on Welfare Foods
(1937).’
#{182}Adolescents 18-15 years.
COMMITI’EE ON NUTRITION 515
youngsters had not received any vitamin
supplements, and the computed intake of
vitamin D was considerably less than the
figure recommended above.
Obviously, additional data are needed to
delineate the minimal requirement in this
age group.
The Adolescent
The determination of the minimal vita-
mm D requirement of the adolescent pre-
sents the same problems as those met for
children. Some years ago, it was considered
that rapid skeletal growth during this period
necessitated a considerably greaten intake
of vitamin D (up to 3,900 I.U. pen day).27
However, when studies were made in
healthy adolescents under conditions of op-
timal calcium and phosphorus intake, maxi-
mal calcium retention was achieved with
intakes of 400 I.U. pen day.28
The Adult
Calcium retentions have been measured
in a number of healthy adults consuming
average unfortified diets with standardized
intakes of calcium and varying supplemental
intakes of vitamin D. In none of these
studies was a consistent difference in cal-
cium retention detected before and during
the administration of vitamin D supple-
ments.2’ For this reason it has sometimes
been implied that healthy adults do not re-
quire vitamin D, and no allowances are rec-
ommended by the various national commit-
tees (Table I).
From physiologic considerations, this is
probably not strictly correct. It is more
likely that the amount of vitamin D needed
for the maintenance of normal calcium and
phosphorus metabolism in adults is so low
that the requirement is readily met by the
average diet and by casual exposure to sun-
light. The hypothesis of a small require-
ment is strengthened by a number of re-
ports of adults with osteomalacia attributed
to vitamin D deficiency. One report men-
tions 15 nuns who developed radiographic
and clinical signs of osteomalacia during
World War II while confined to a convent
under conditions of poor nutrition.30 The
other 33 record isolated cases, in
each of which food faddism had led to ex-
tremely low intakes of vitamin D containing
foods. In one case33 the vitamin D intake
was estimated to be less than 20 I.U. pen
day. Although the bizarre diets were also
extremely low in calcium, it is probable that
vitamin D deficiency was the important fac-
ton, particularly since there is evidence that
low calcium intakes per se lead to osteoporo-
sis rather than to osteomalacia.34
The Pregnant and Lactating Woman
The reports of osteomalacia in pregnant
and lactating Chinese 536 constitute
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

516 VITAMIN D
evidence that these states impose physio-
logic stresses upon the normal calcium and
phosphorus metabolism of the adult. Al-
though the calcium content of the diets of
the women was poor, the osteomalacia re-
sponded to vitamin D rather than to extra
calcium. These studies have therefore been
taken to indicate that amounts of vitamin
D greater than those needed by the normal
adult are required for optimal nutrition dur-
ing the last trimester of pregnancy and dun-
ing lactation. However, data regarding the
actual requirements are lacking.
In addition, provision should be made in
tile diet for the extra calcium required by
the growing fetus (approximately 200 mg
are deposited per day during the last 2
months of pregnancy) and by lactation (ap-
proximately 200 to 300 mg are excreted per
day).18
Summary: Recommended Allowances at
Various Ages
Allowances currently recommended in
the United States, Great Britain, and Can-
ada are shown in Table I. The recommen-
dations are seen to be in reasonably close
agreement. As indicated, there are minor
differences in the terms of reference. How-
ever, it should be noted that in all instances
the figures are intended to be taken as rep-
resenting the total recommended daily in-
take of vitamin D from all ingested sources,
assuming no exposure to ultraviolet radia-
tion, assuming the consumption of adequate
(luantities of calcium and phosphorus(values about which, incidentally, there is
still much argnment�4) and incorporating a
safety factor beyond the minimum daily re-
quirement of the normal individual.
The Committee on Nutrition believes that
available data support the view that for full-
term infants fed cow’s milk formulas or
human milk a total intake of 400 I.U. vita-
mm D per day from all dietary sources is a
suitable allowance to prevent rickets and to
promote optimal calcium and phosphorus
metabolism. The same dose, perferably pro-
vided as a water miscible suspension,37 is
considered to be suitable for premature in-
fants fed commonly employed formulas of
cow’s milk. The higher recommendation of
the British authorities (Table I) is intended
to provide an additional safety factor, but
there does not appear to be scientific proof
that tile extra amount is actually more ef-
fective. For both full-term and premature
infants tile range of individual variation has
been well investigated. It may he assumed
that this dose provides a moderate safety
factor, and that few, if any, normal infants
will develop rickets while receiving such an
intake. Vitamin D prophylaxis should be
commenced within the first 2 weeks of
life.
There is no question that in certain lo-
cales and under proper conditions prophy-
lactic amounts of vitamin D can be acquired
from sunlight during the summer months.
However, to cover all contingencies, the
Committee considers that an attempt should
be made to ensure the provision of tile 400
I.U. allowance from ingestible sources on
a year-round basis.
Available data do not provide accurate es-
timates of the minimum requirement be-
yond the period of infancy. For children
and adolescents, the Committee recom-
mends a total dietary intake of 400 I.U. of
vitamin D per day from all sources as a safe
allowance. As indicated below, in the
United States such an intake will ordinarily
be acquired from fortified foods witllout
administration of a vitamin supplement. In
Canada, the same situation frequently ob-
tains in individual cases, but cannot he so
generally relied upon.
The small requirement of tile healthy
adult is satisfactorily met by casual ex-
posure to sunlight and by the consumption
of usual unenniched foods, and no vitamin
D supplementation is necessary unless spe-
cifically indicated by reason of occupation
or other unusual circumstance. A total daily
intake of 400 I.U. of vitamin D is con-
sidered adequate to provide for added de-
mands during the second half of pregnancy
and during lactation.
It is the opinion of the Committee that
there is no necessity to exceed tile recom-
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

COMMITTEE ON NUTRITION 517
mended allowance during convalescence
from acute infections. Similarly, for most
chronic conditions, the recommended allow-
ance is probably adequate.
THE DANGERS OF VITAMIN D
Notwithstanding lack of knowledge con-
cerning minimal requirements, the Com-
mittee believes a daily intake of 400 I.U.
of vitamin D can be expected to prevent
detectable vitamin D deficiency in the nor-
mal infant or child consuming adequate
amounts of calcium. Furthermore, there is
no evidence to indicate that larger amounts
of vitamin D would be more effective in
any way. On the other hand, because nowa-
days many infants and children un-
doubtedly receive more than 400 I.U. of
vitamin D daily, and because there is in-
controvertible evidence that prolonged in-
take of vitamin D in large doses produces
hypercalcemia with its numerous sequelae,
it has become imperative to define the safe
upper limits of vitamin D intake.
Many years ago Hess and Lewis38 demon-
strated that very large doses of vitamin D
would produce hypercalcemia. Since that
time hypervitaminosis D has been reported
in many individuals, a considerable number
of whom were infants and children. There
appears to be a fairly wide range of sus-
ceptibility to the toxic actions of vitamin D
and it has been estimated that approxi-
mately 20% of normal adults who receive
100,000 I.U. of vitamin D daily for several
weeks or months will develop hypercal-
cemia.38 Hypencalcemia is accompanied by
anorexia, nausea, weight loss, polyunia, con-
stipation, and reversible azotemia. If hyper-
calcemia continues generalized vascular cal-
cification, nephrocalcinosis and irreversible
renal insufficiency eventually supervene. In
terms of unit body weight, dosages in the
region of 1,000 to 3,000 I.U./kg/day for
several weeks or months are toxic in the
adult, and evidence suggests that this unit
dose manifests approximately the same de-
gree of toxicity in infants under 2 years of
age.1#{176}For a 1-year-old infant, this amount
of vitamin D would represent a total dose
of between 10,000 and 30,000 I.U. per
day.
The Risk of Vitamin D Toxicity
in Infancy
The dosages mentioned above are at least
25 times greater than the prophylactic re-
quirement. On the other hand, Jeans &
Stearns40 suggested in 1938 that daily in-
takes of vitamin D in the range of 1,800 to
6,300 I.U. inhibited linear growth of normal
infants and were therefore undesirable. Be-
cause the series of infants was small, and
because considerable variability was ob-
served in the individual growth patterns of
experimental and control subjects, the data
are difficult to interpret. The study has not
been confirmed by other workers, and there
has been little concern until relatively ne-
cently about administering prophylactic
doses of vitamin D in the order of 2,000
I.U. daily.
However, in 1952 reports from Great
Britain and Switzerland drew attention to
a small group of infants with unexplained
ypt2 Shortly after the initial
reports were published, cases of infantile
hypercalcemia commenced to be diagnosed
in increasing numbers throughout the
British Isles. In its rare severe form42 hy-
pencalcemia was associated with mental ne-
tardation, osteosclerosis, severe azotemia
and other bizarre features. In its relatively
more common mild form,4’ which typically
commenced between the second and tenth
month of life, there was fairly sudden onset
of anorexia, vomiting, polydipsia, weight
loss, and failure to thrive, and the serum
calcium was elevated above 12 mg/100 ml
(often to 15 mg/100 ml or higher). Mild,
usually reversible azotemia frequently de-
veloped.
Because many of the features resembled
those of hypervitaminosis D, it was logical
that attention should be focused upon the
possibility that vitamin D was implicated in
the pathogenesis of this new and important
health problem. It was found that the hy-
percalcemia was controlled when all sources
of vitamin D were withheld and a very low
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

518 VITAMIN D
calcium intake instituted, although tile ad-
ditional features of the severe form did not
disappear.
In 1953 and 1954 at a time when approxi-
mately 100 new cases of hypercalcemia
were being diagnosed annually in Great
Britain, an extensive survey of infant feed-
ing practices in Great Britain revealed that,
as a result of the then liberal enrichment of
national dried milk powder and infant
cereals with vitamin D, a normal infant con-
suming an average diet plus the recom-
mended daily supplement of vitamin D (at
that time 700 to 800 I.U.) might readily in-
gest 4,000 I.U. of vitamin D per day.43
On the other hand, idiopathic hypercal-
cemia cannot be explained solely on the
basis of excessive vitamin D intake. For one
thing, it was noted that not all affected in-
fants were ingesting as much as 4,000 I.U.
of vitamin D per day. For instance, in a
study of 38 cases from Glasgow, 26 (two-
thirds) had received less than 2,000 I.U.
per day, and 8 (one-fifth) had received less
than 1,000 lU. per day.44 Further, it should
he recalled that, of the large number of
British infants who during one period are
presumed to have ingested 3,000 to 4,000
lU. per day, relatively few suffered any de-
tectable ill effects.
To account for some of the contradictory
findings, it has been suggested that patients
with idiopathic hypercalcemia may be hy-
persensitive to vitamin D45 or, alternatively,
that they may have an inborn disturbance
in cholesterol metabolism�#{176} which causes
tile accumulation of vitamin D or of some
abnormal metabolite with vitamin D-like ac-
748 The fact that none of the affected
infants had been entirely breast-fed�9 sug-
gests that tile higher calcium content or
some other feature of cow’s milk may also
be a factor.
Although it is obvious that infants who
develop hypercalcemia differ in some fun-
damental way from normal infants, it is
hard to escape the still-circumstantial evi-
dence which appears to relate the condition
with vitamin D. As a result of recommenda-
tions of the British Paediatrie Association
Committee on Hypercalcaemia41 and of the
Joint Subcommittee on Welfare Foods,5
measures were taken to reduce the average
intake of vitamin D of British infants by
halving the potency of National Cod Liver
Oil and by considerably reducing the
amounts of vitamin D added to dried milk
powders and to infant cereals. It has been
estimated that the average intake of vitamin
D has probably been reduced to between
one-third and one-half the former quantity
as a result of these measures.
Obviously, careful evaluation of the pres-
ent incidence of idiopathic hypercalcemia
in Britain is essential before conclusions can
be drawn regarding the importance of vita-
mm D in the etiology of the condition. Un-
fortunately, this information is not yet ac-
curately known. However, according to an-
notations in the British Medical Journal�#{176}and in Lancet5#{176} in 1960, many pediatricians
believe that the incidence of the disease has
fallen since the recommendations regarding
vitamin D intake were carried out. It is very
tempting therefore, to suggest that vitamin
D and idiopathic hypercalcemia are caus-
ally related. On the other hand, because it
is not yet possible to weigh the many com-
plex factors, it seems unwarranted to draw
final conclusions regarding the etiologic role
of vitamin D until the results become avail-
able of a comprehensive study which is cur-
rently being undertaken by the British
Paediatric Association Committee on Hy-
percalcaemia.
ESTIMATES OF VITAMIN D INTAKES INTHE UNITED STATES AND CANADA
AT VARIOUS AGES
The large number of vitamin prepara-
tions and of commonplace commercially-for-
tified foodstuffs on the North American
market provide a variable and virtually un-
avoidable intake of vitamin D which,
though difficult to estimate, may often be
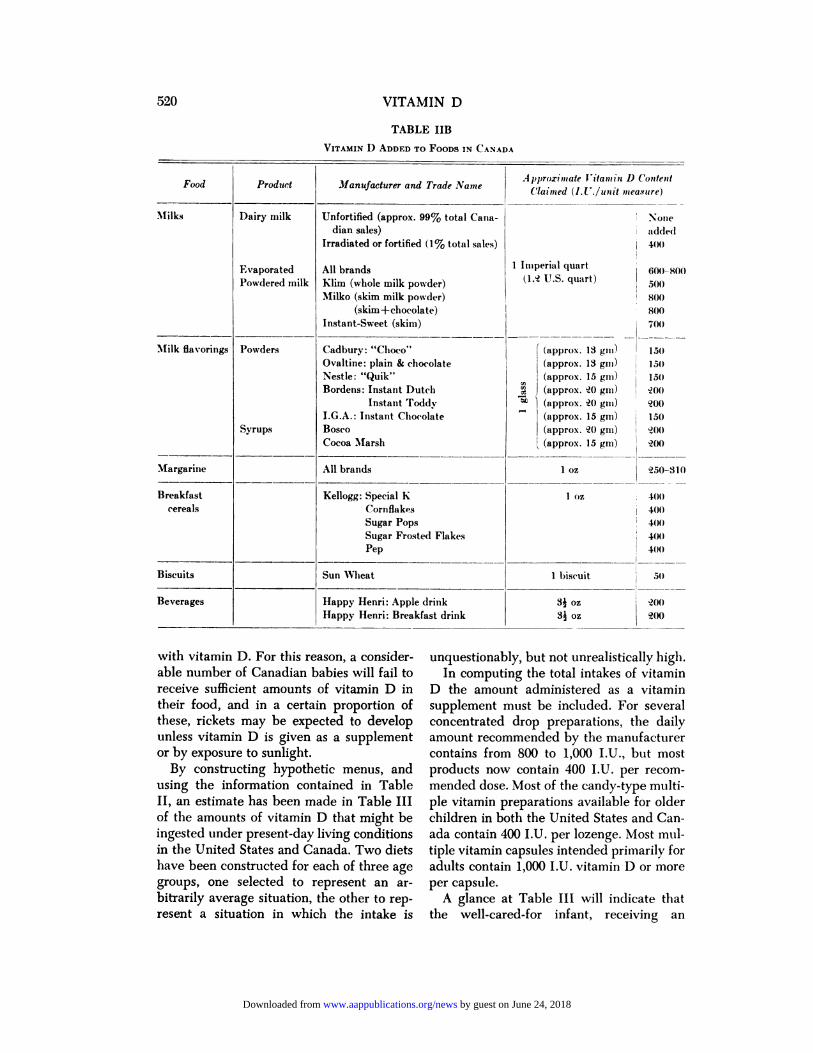
considerable. Table II gives information
concerning some of the foods currently en-
riched with vitamin D in the United States
and Canada. Because of frequent changes
by the manufacturers, this information is
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

COMMITTEE ON NUTRITION 519
TABLE hA
VITAMIN D ADDED TO FOODS IN U.S.A.
Food Product Manufacturer and Trade NameApproxnnate Vitamin D Content
.
Claimed (lU/unit nzea.ntre)
Milks Dairy Milk
Evaporated
Powdered
Fortified (approx 85% total sales)
All brands
Klim (whole) & most powdered infant for-
mulas
Skim milks (powdered)
1 U.S. quart
1 IJ.S. quart (reconstit.)
1 U.S. quart (reconstit.)
400
400
400
0
Milk flavorings Powders
Syrups
Ovaltine (plain or chocolate)
Hershey-Instant Cocoa Mix
Nestle-”Quick”
Borden’s Dutch Chocolate
Baker’s-Instant Choc. Mix
Bosco
Cocoa Marsh
I (approx. 15 gm)� (approx. 15 gas)
� (approx. �0 gm)
“� (approx. 15 gm)
(approx. �0 gm)
(approx. �0 gm)
(approx. 15 gm)
150
150
100
100
100
150
50
Margarine Parkay, Kraft
All-Sweet, Blue Bonnet, Fleishman’s, Good-
Luck, Imperial, Mazola
1 oz
I oz
�50
1�5
Breakfast (ereals Kellogg-All Bran
Cornflakes
Special K
Sugar Pops
Pep
Concentrate
General Mills-Hi-Pro
Quaker-Life
Coco-Wheats
1 serving (1 oz)
400
�00
�00
W0
�00
�00
150
80
80
\Iiscellaneous Bread
CandyBeverage
Special Sunbeam Bread (a premium prod-
uct only)
Swiss BarStuart’s Instant Vita Drink
1 slice
I bar
I glass
(1 teaspoon powder)
100
400
I ,000
only approximate. The recorded figures are
computed from the manufacturers’ label
claims and represent minimum values, since
it is customary manufacturing practice to
add an “overage” to allow for possible de-
tenioration, etc. Overage may constitute as
much as 100% or more of the label claim in
tile United States. In Canada, regulations
prescribe that a given food may contain not
less than 400 or more than 800 I.U. of vita-
mm D in a reasonable daily intake of that
food,5’ but despite the regulations, the over-
age permitted within the limits of good
manufacturing practice undoubtedly re-
mains a factor to be considered.
There are certain differences between the
United States and Canadian figures. In the
United States, vitamin D is added to virtu-
ally all evaporated milk in a concentration of
400 I.U. per reconstituted U.S. quart, and
a similar amount is added to 85% of all dairy
milk marketed in the United States (al-
though the latter figure may decrease as
a result of the recent re-introduction of
unfortified dairy milk by certain super-
markets). In Canada, all brands of evapo-
rated milk contain approximately 600 to 800
I.U. vitamin D per reconstituted Imperial
quart (i.e., 500 to 700 I.U. per reconstituted
U.S. quart). However, in contrast to custom
in the United States, less than 1% of dairy
milk on the Canadian market is enriched
by guest on June 24, 2018www.aappublications.org/newsDownloaded from
520 VITAMIN D
TABLE JIB
VITAMIN D ADDED TO FOODS IN CANADA
Food Product Manufacturer and Trade NameA pprox-iiiiate J itam in D Content
, . .Claimed (IJ ./untt measure)
Milks Dairy milk
Evaporated
Powdered milk
Unfortified (approx. 99% total Cairn-
dian sales)
Irradiated or fortified (1% total sales)
All brands
Klim (whole milk powder)
Milko (skim milk powder)
(skim+chocolate)
Instant-Sweet (skim)
None
� ad(le(l
� 400
I lIlIperial quart � 600�S00
(1,� U.S. quart) �
� 800
800
700
I (approx. 13 gui) l3�
(approx. 13 gin) � Isoa (approx. 15 gIll) � 1.50� (approx. �0 gill) � �0()
M ) (approx. �0 gui) �oo“#{176} (approx. 15 gm) 150
(approx. �2() gill) �200
� (approx. 1.5 gnl) �200
�IiIk flavorings Powders
Syrups
Cadbury: “Choco”
Ovaltine: plain & chocolate
Nestle: “Quik”
Bordens: Instant Dutch
Instaiit Toddy
I.G.A. : Instant Chocolate
Bosco
Cocoa Marsh
Margarine All brands I oz �50-31()
Breakfast
cereals
Kellogg: Special K
Cornflakes
Sugar Pops
Sugar Frosted Flakes
Pep
I 01 400
400
400
400
4(8)
Biscuits Sun Wheat I biscuit 50
Beverages Happy Henri: Apple drink
Happy Henri: Breakfast drink34 oz
34 oz
�200
C200
with vitamin D. For this reason, a consider-
able number of Canadian babies will fail to
receive sufficient amounts of vitamin D in
their food, and in a certain proportion of
these, rickets may be expected to develop
unless vitamin D is given as a supplement
or by exposure to sunlight.
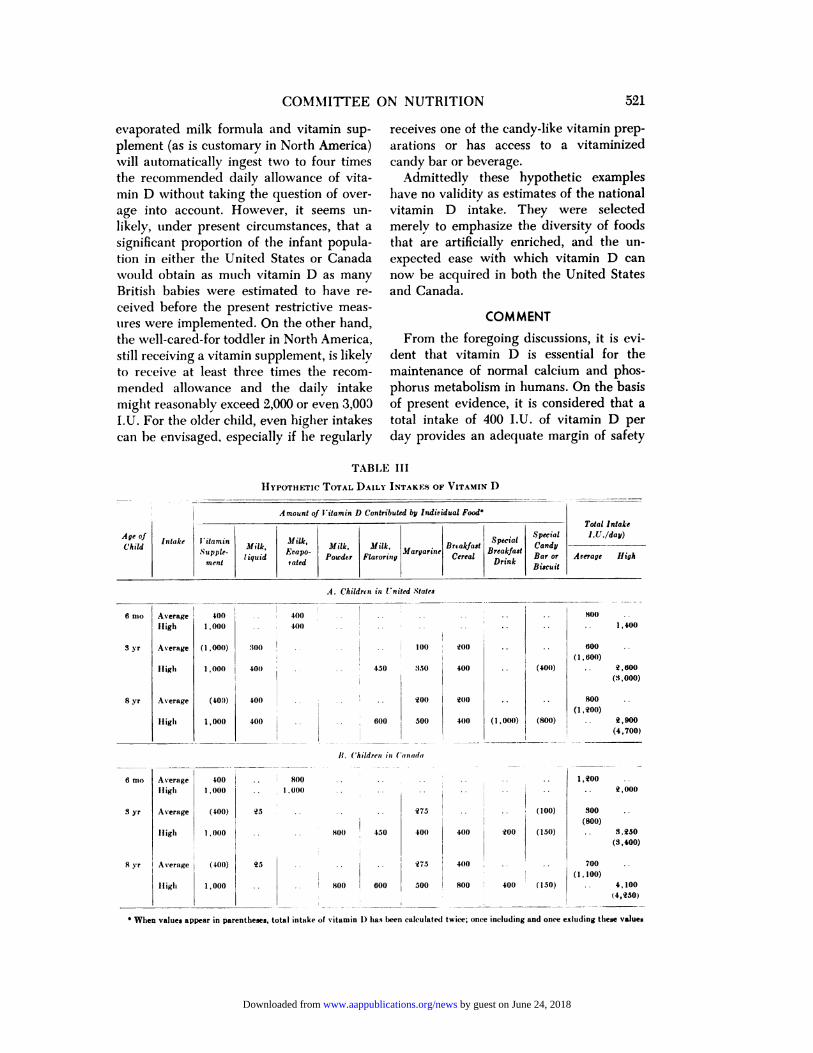
By constructing hypothetic menus, and
using the information contained in Table
II, an estimate has been made in Table III
of the amounts of vitamin D that might be
ingested under present-day living conditions
in the United States and Canada. Two diets
have been constructed for each of three age
groups, one selected to represent an an-
bitranily average situation, the other to rep-
resent a situation in which the intake is
unquestionably, but not unrealistically high.
In computing the total intakes of vitamin
D the amount administered as a vitamin
supplement must be included. For several
concentrated drop preparations, the daily
amount recommended by the manufacturer
contains from 800 to 1,000 I.U., but most
products now contain 400 I.U. per recom-
mended dose. Most of the candy-type multi-
pie vitamin preparations available for older
children in both the United States and Can-
ada contain 400 I.U. per lozenge. Most mul-
tiple vitamin capsules intended primarily for
adults contain 1,000 I.U. vitamin D or more
per capsule.
A glance at Table III will indicate that
the well-cared-for infant, receiving an
by guest on June 24, 2018www.aappublications.org/newsDownloaded from
COMMITTEE ON NUTRITION
TABLE Ill
Age of
ChildIntake Vitamin
Supple-
ment
Amount of Vitamin D Contributed by lndiriduaJ FOOd#{176}
Milk,
1 iquid
.�fiLk, Milk,
Lrapo-Powder
vated
MargarineMilk.
Flavoring
Ilvtakfast
Cereal
Special
Breakfast
Drink
Special
Candy
Bar or
Biscuit
6 nio
S yr
8 yr
Total Intake
lU/day)
Arerage High
Average
High
Average
Iligli
Average
high
400
1 , 000
(1,000)
1 , 000
(400)
1 , 000
000
401)
400
400
400 �- - - -
400 - - - -
. - - - - . �
100
- . - - 450 850
- - � - - . . �oo
. . � --� 600 500
�O0
400
�00 ..
400 (1,000)
II. (‘hiletren in (anada
(400)
(800)
(100)
(150)
6 nio Average 400 . . 800
High 1,000 . 1,000
S yr Average (400) �3 ..
Iligh 1,000 -.
8 yr Average (-100) 23 - -
Ilighi 1,000 . - -
800
1,400
600
(1 , 600)
. q,600
(3,000)
800 ..
(I ,�00)
. 2,900
(4,700)
1,200
. 2,01)0
300(800)
. 3.230
(3,400)
700 ..
(1 , 100)
. - 4,100
(4,230)
1400 � 450
� 800 � 600
275
400
275
500
400
400
800
�oo
400 � (150)
S When values appear in parentheses, total intake of vitamin 0 has been calculated twice; ome including and once exhuding these values
evaporated milk formula and vitamin sup-
plement (as is customary in North America)
will automatically ingest two to four times
the recommended daily allowance of vita-
mill D without taking the question of over-
age into account. However, it seems un-
likely, under present circumstances, that a
significant proportion of the infant popula-
tion in either the United States or Canada
�vould obtain as much vitamin D as many
British babies were estimated to have re-
ceived before tile present restrictive meas-
tires were implemented. On the other hand,
the well-cared-for toddler in North America,
still receiving a vitamin supplement, is likely
to receive at least three times tile recom-
mended allowance and the daily intake
might reasonably exceed 2,000 or even 3,003
I.U. For the older child, even higher intakes
can he envisaged. especially if he regularly
521
receives one of the candy-like vitamin prep-
arations or has access to a vitaminized
candy bar or beverage.
Admittedly these hypothetic examples
have no validity as estimates of the national
vitamin D intake. They were selected
merely to emphasize the diversity of foods
tilat are artificially enriched, and the un-
expected ease with which vitamin D can
now be acquired in both the United States
and Canada.
COMMENT
From the foregoing discussions, it is evi-
dent that vitamin D is essential for the
maintenance of normal calcium and phos-
phorus metabolism in humans. On the basis
of present evidence, it is considered that a
total intake of 400 I.U. of vitamin D per
day provides an adequate margin of safety
HYPOTHETIC TOTAL DAILY INTAKES OF VITAMIN D
.4. (‘F,ildnn in (nited Slates
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

522 VITAMIN D
to protect substantially all normal growing
individuals from detectable evidence of
vitamin D deficiency.
At the same time, it is known that exces-
sive amounts of vitamin D are toxic. The
low limit of toxicity is not cleanly defined,
but British experience with the problem of
idiopathic hypercalcemia suggests that this
toxic level may, on rare occasions, be as low
as 3,000 to 4,000 I.U. per day for susceptible
individuals in tile infant age group, and
sometimes considerably lower.
Until relatively recently, the average diet
contained very little vitamin D and could
not necessarily be relied upon to prevent
vitamin D deficiency during growth, par-
ticularly during infancy. The use of vitamin
D supplements was therefore promoted, and
there was widespread acceptance of this
public health measure throughout North
America. However, when it became evident
that rickets had not been entirely eliminated
by this measure, the decision was made to
enrich commercial milks with vitamin D,
and tile outstanding success of this program
gave impetus for the addition of this and
other vitamins to a variety of foods. At the
present time, a wide range of common food-
stuffs contain added vitamin D, and it is
obvious that the oven-all vitamin D intake
of all ages of the population has risen ap-
pneciably in the United States and Canada.
Calculations indicate that the amount of
vitamin D now acquired from the diet alone
may readily exceed tile recommended daily
allowance, sometimes by a considerable
amount.
Although the exact cause of idiopathic
hypercalcemia of infancy remains to be
established, there is now a large amount of
evidence which incriminates vitamin D as
an important etiologic factor. Despite the
fact that infantile hypencalcemia has, until
now, been much less common on this conti-
nent than in Great Britain, more than 30
cases have already been reported in North
America since 1954 and existence of a num-
ben of unpublished cases is known to mem-
bens of the Committee.
Thus, in the face of existing evidence,
the Committee on Nutrition considers that
practitioners and public health authorities
should strive to ensure that the total vitamin
D intake of all infants reaches tile recom-
mended allowance of 400 I.U. per day, but
at the same time, they should make con-
certed efforts to restrict the upper limit of
intake for all sources to an amount as close
to this figure as is practicable. This de-
mands tilat cognizance be taken of the
amount of vitamin D contributed by the
formula and other components of the diet
before prescribing a vitamin D supplement,
and that attention be paid to the amount of
vitamin D provided by the supplement
chosen.
It demands, also, that efforts be intensi-
fled to dispel from the minds of parents tile
concept of vitamins as tonics, with the
hope of reducing the all-too-prevalent prac-
tice of vitamin D “over-insurance” in tile
home.�� Although there is no specific evi-
dence that daily intakes of vitamin D in tile
order of 2,000 to 3,000 I.U. produce de-
letenious effects on individuals beyond in-
fancy, it should be realized that tue present
trend in nutrition is imposing a new situa-
tion upon the children and adults of North
America, the long-term effects of which are
entirely unknown.
The addition of vitamin D to practically
all commercial milk supplies in the United
States has been amply justified by the dra-
matic reduction which it brought about in
the incidence of rickets. By inference, simi-
lan benefits would presumably be observed
in Canada by broadening tile present milk-
fortification program to include dairy milk.
On the other hand, the milk consumption
habits of North American children ensure a
uniformity and dependability of intake
which does not apply to other foodstuffs.
Hence, the enrichment of a large variety of
additional foods with vitamin D cannot be
similarly justified.
SUMMARY AND RECOMMENDATIONS
Despite inadequacies in information con-
cerning the minimum prophylactic require-
ment of vitamin D for all age groups be-
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

COMMITTEE ON NUTRITION 523
yond infancy, there is no doubt that a total
intake of 400 I.U. per day is adequate to
prevent vitamin D deficiency in substan-
tially all normal children from birth through
adolescence.
Evidence derived from the study of idio-
pathic hypercalcemia suggests that certain
infants excessively sensitive to the toxic ac-
tion of vitamin D may, on rare occasions,
be adversely affected by daily intakes of
3,000 to 4,000 I.U. and sometimes consider-
ably less. Because of the prevalent practice
of food fortification in the United States
and Canada, there is now a definite possi-
hility that the individual, even the young
infant, may ingest considerably more than
tile recommended vitamin D allowance, andintakes of 2,000 to 3,500 lU. pen day are
possible, particularly beyond infancy. Al-
though there has been no specific evidence
that intakes of this order produce deleteni-
oils effects beyond infancy, it is pointed out
that tile long-term consequences of this new
nutritional situation on older children or
adults are entirely unknown.
In view of these considerations tile Com-
mittee on Nutrition recommends that efforts
he taken to ensure a total vitamin D intake
of 400 I.U. per day by all infants and chil-
dren. At the same time, an attempt should
1)e made to restrict the intake from all
sources to an amount not greatly in excess
of tilis figure.
The value of carefully planned enrich-
ment of commercial milk supplies with vita-
mm D has been clearly demonstrated. How-
ever, the present practice of enriching foods
other than milk and infant formula prod-
ucts is not justified, and discontinuation of
this practice is to be recommended. Under
the present circumstances, cognizance
should be taken of the amount of vitamin
D acquired by tile individual from food
sources before prescribing a vitamin D sup-
plement.
In keeping with present concepts regard-
ing vitamin D requirement, commercial
vitamin D supplements should be adjusted
to contain not more than 400 I.U. per
dose.
COMMITI-EE ON Nu-nirnoN
Richard W. Blumberg, M.D.
Gilbert B. Forbes, M.D.
Donald Fraser, M.D.
Arild E. Hansen, M.D.
Charles U. Lowe, M.D.
Nathan J. Smith, M.D.
Michael J. Sweeney, M.D.
Samuel J. Fomon, M.D., Chairman
REFERENCES1. Mellanby, E. : Accessory food factors (vita-
mins) in the feeding of infants. Lancet, 1:
856, 1920.2. FoiLs, R. H., Jr., Park, E. A., and Jackson, D.:
The prevalence of rickets at autopsy duringthe first two years of age. Johns Hopkins
Hosp. Bull., 91:480, 1952.
3. Committee on Nutrition, American Academy
of Pediatrics: Infantile scurvy and nutri-
tional rickets in the United States. PEDI-
ATRICS, 29:646, 1962.
4. Fraser, D., and Salter, R. B. : The diagnosisand management of the various types of
rickets. Pediat. Clin. N. Amer. (May) 417,
1958.5. Great Britain Ministry of Health. Report of the
joint Sub-Committee on Welfare Foods
(Chairman, Lord Cohen of Birkenhead),London, Her Majesty’s Stationery Office,
1957.
6. Harris, L. J. : Vitamin D and bone; In The
Biochemistry and Physiology of Bone; edited
by Bourne, C. H. ; New York, Acad. Press,
1956, p. 617.
7. Drake, T. C. H. : Comparison of the anti-
rachitic effects on human beings of vitamin
D from different sources. Amer. J. Dis.Child., 53:754, 1937.
8. Kramer, B., Sobei, A. E., and Cottfried, S. P.:Serum levels of vitamin A in children : a
comparison following the oral and intra-
muscular administration of vitamin A in
oily and in aqueous mediums. Amer. J. Dis.
Child., 73:543, 1947.
9. May, C. D., and Lowe, C. U. : The absorptionof orally administered emulsified lipid in
normal children and in children with steator-
rhea. J. Clin. Invest., 27:226, 1948.
10. Flood, J. S., and Ravitch, I. : The antirachitic
efficiency of irradiated cholesterol. J. Pediat.,11:521, 1937.
1 1. Rhoads, T. F., et al.: Studies on the growthand development of male children receivingevaporated milk : I. The effect of various
vitamin supplements on growth in length
and incidence of rickets during the first two
years of life. J. Pediat., 19: 169, 1941.
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

524 VITAMIN D
12. May, E. W., and Wygant, T. M. : Rachiticstudies : III. An evaluation of methods of
antirachitic treatment. Arch. Pediat., 56:426,
1939.
13. Houet, R. : Recherches sur le metabolisme deIa vitamine D: III. Determination du besoin
joumalier en vitamine chez Ic nourrisson.
Ann. Paediat., 167:225, 1946.
14. Stearns, C. : Calcium, phosphorus and vitamin
D requirements in infants, II: In Infant
Metabolism; edited by Scheinberg, I. H.,
New York, Macmillan. 1956, p. 80.
15. Steams, C., Jeans, P. C., and Vandecar, V.:
The effect of vitamin D on linear growth
in infancy. J. Pediat., 9: 1, 1936.
16. Slyker, F., et al.: Relationship between vita-
mm D intake and linear growth in infants.
Proc. Soc. Exp. Biol. Med., 37:499, 1937.
17. Macy, I. C., Kelley, H. J., and Sloan, R. E.:
The Composition of Milks. National Acad-
emy of Sciences-National Research Council,
Publication 254, Washington, D.C., 1953,
p. 63.
18. Leitch, I., and Aitken, F. C. : The estimation
of calcium requirement : a re-examination.
Nutr. Abstr. Rev., 29:393, 1959.
19. Fanconi, C., and Waligren, A. (eds.): Lehr-
buch der Padiatrie. Basel. Schwabe, 1958,
p. 151.
20. Lightwood, R., and Stapleton, T. : National
policies for the prevention of rickets. Ann.
Paediat., 188:270, 1957.
21. Widdowson, E. M., and Spray, C. M. : Chemi-
cal development in utero. Arch. Dis. Child.,26:205, 1951.
22. Davidson, L. T., and Merritt, K. K. : Viosterol
in the prophylaxis of rickets in premature
infants. Amer. J. Dis. Child., 48:281, 1934.
23. Glaser, K., Parmalee, A. H., and Hoffman,
W. S. : Comparative efficacy of vitamin D
preparations in prophylactic treatment of
premature infants. Amer. J. Dis. Child., 77:
1, 1949.
24. Chisolm, J. J., Jr., and Harrison, H. E. : Amino-
aciduria in vitamin D deficiency states in
premature infants and older infants with
rickets. J. Pediat., 60:206, 1962.
25. FoILs, R. H., Jr., et al.: Prevalence of rickets
in children between two and fourteen years
of age. Amer. J. Dis. Child., 66: 1, 1943.
26. Stearns, C. : Nutritional health of infants, chil-
dren and adolescents. Proceedings of the
Natural Food and Nutrition Institute, U.S.
Department of Agriculture Handbook 56,1952, p. 59.
27. Johnston, J. A. : Factors influencing retention
of nitrogen and calcium in period of growth:VI. The calcium and vitamin D require-
ments of the older child. Amer. J. Dis.
Child., 67:265, 1944.28. Jeans, P. C.: Vitamin D. J.A.M.A., 143:177,
1950.29. NIcKay, H., et a!.: The effect of vitamin D on
calcium retentions. j. Nutr., 26:153, 1943.
30. Van Buchem, F. S. P. : Osteomalacia: Patho-
genesis and treatment. Brit. Med. J., 1:
933, 1959.
31. McCance, R. A. : The problem of adaptation
to low calcium intakes. Transactions of
Macy Conference on Metabolic Interrela-
tions with Special Reference to Bone, 5:
166, 1953.
32. Hill, M. : A case of food faddism which led
to osteomalacia. Nutrition, 2:319, 1956.
33. Rose, C. A., Lumb, F. H., and Dent, C. E.:
Discussion on generalized aches and pains
from metabolic bone disease. Proc. Roy. Soc.
Med., 50:371, 1957.
34. Jackson, W. P. U. : Effects of altered nutrition
on the skeletal system; the requirement of
calcium in man. In Recent Advances in
Human Nutrition, with Special Reference to
Clinical Medicine; edited by Brock, j. F.;
London, Churchill, 1961, p. 293.
35. Maxwell, J. P., et al: Further studies in adult
rickets (osteomalacia) and foetal rickets.
Proc. Roy. Soc. Med., 32:287, 1939.
36. Liu, S. H., et al.: Calcium and phosphorus
metabolism in osteomalacia : II. Further
studies on the response to vitamin D of pa-
tients with osteomalacia. Chinese Med. J.,49:1, 1935.
37. Harrison, H. E. : Rickets. In Brennemann-
McQuarrie-Kelley: Practice of Pediatrics.
Hagerstown, Maryland; W. F. Prior, 1961,
vol. I, part, II, Chap. 36, p. 35.
38. Hess, A. F., and Lewis, j. M. : Clinical experi-ence with irradiated ergosterol. J.A.M.A.,
91:783, 1928.
39. Anning, S. T., et a!.: The toxic effects ofcalciferol. Quart. J. Med., 17:203, 1948.
40. Jeans, P. C. , and Stearns, G. : The effect of
vitamin D on linear growth in infancy: II.
The effect of intakes above 1,800 U.S.P.
units daily. J. Pediat., 13:730, 1938.
41. Lightwood, R. : Idiopathic hvpercalcaemia
with failure to thrive: nephrocalcinosis.
Proc. Roy. Soc. Med., 45:401, 1952.
42. Fanconi, C., et al: Chronische hypercalcamie,kombiniert mit osteosklerose, hyperazotamie,minderwuchs und kongenitalen missbil-
dungen. Helvet. Pediat. Acta., 7:314, 1952.
43. British Paediatric Association, Committee on
Hypercalcaemia : Hypercalcaemia in infants
and vitamin D. Brit. Med. J., 2: 149, 1956.
44. Graham, S. : Idiopathic hypercalcaemia. Post-
grad. Med., 25:67, 1959.
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

COMMITTEE ON NUTRITION 525
45. Lowe, K. C., et al.: The idiopathic hyper-calcaemic syndromes of infancy. Lancet, 2:
101, 1954.
46. Forfar, J. 0., et al.: Idiopathic hypercalcaemiaof infancy : clinical and metabolic studies
with special reference to the aetiological role
of vitamin D. Lancet, 1 :981, 1956.
47. Fellers, F. X., and Schwartz, R. : Etiology of
the severe form of idiopathic hypercalcemia
of infancy: a defect in vitamin D metabol-
ism. New Engl. J. Med., 259: 1050, 1958.
48. Smith, 1). W., Blizzard, R. M., and Harrison,
H. E. : Idiopathic hypercalcemia : a case re-
port with assays of vitamin D in the serum.
PEDIATRICS, 24:258, 1959.
49. Aetioiogy of idiopathic hypercaicaemia. Brit.
Med. J., 1:335, 1960.
50. Idiopathic hypercalcaemia of infants. Lancet,
2:138, 1960.
51. Department National Health and Welfare.
Food and Drugs Act and Regulations.Ottawa, August 9, 1961.
52. Forbes, G. B. : Overnutrition for the child:
blessing or curse? Nutr. Rev., 15: 193, 1957.
by guest on June 24, 2018www.aappublications.org/newsDownloaded from

1963;31;512Pediatrics THE TOXICITY OF VITAMIN D
COMMITTEE ON NUTRITION: THE PROPHYLACTIC REQUIREMENT AND
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/31/3/512including high resolution figures, can be found at:
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlentirety can be found online at: Information about reproducing this article in parts (figures, tables) or in its
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 24, 2018www.aappublications.org/newsDownloaded from
1963;31;512Pediatrics THE TOXICITY OF VITAMIN D
COMMITTEE ON NUTRITION: THE PROPHYLACTIC REQUIREMENT AND
http://pediatrics.aappublications.org/content/31/3/512the World Wide Web at:
The online version of this article, along with updated information and services, is located on
Copyright © 1963 by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois, 60007.been published continuously since 1948. Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it has
by guest on June 24, 2018www.aappublications.org/newsDownloaded from





























