Embed Size (px)
Citation preview

International Psychogeriatrics: page 1 of 11 C© International Psychogeriatric Association 2013doi:10.1017/S1041610213000574
The neuropsychological sequelae of delirium in elderly patientswith hip fracture three months after hospital discharge
.........................................................................................................................................................................................................................................................................................................................................................................
Joost Witlox,1 Chantal J. Slor,1 René W.M.M. Jansen,1 Kees J. Kalisvaart,2
Mireille F.M. van Stijn,3 Alexander P.J. Houdijk,3 Piet Eikelenboom,4
Willem A. van Gool5 and Jos F.M. de Jonghe1
1Department of Geriatric Medicine, Medical Center Alkmaar, Alkmaar, the Netherlands2Department of Geriatric Medicine, Kennemer Gasthuis, Haarlem, the Netherlands3Department of Surgery, Medical Center Alkmaar, Alkmaar, the Netherlands4Department of Neurology, Academic Medical Center, Amsterdam, and GGZinGeest, Amsterdam, the Netherlands5Department of Neurology, Academic Medical Center, Amsterdam, the Netherlands
ABSTRACT
Background: Delirium is a risk factor for long-term cognitive impairment and dementia. Yet, the nature of thesecognitive deficits is unknown as is the extent to which the persistence of delirium symptoms and presenceof depression at follow-up may account for the association between delirium and cognitive impairment atfollow-up. We hypothesized that inattention, as an important sign of persistent delirium and/or depression, isan important feature of the cognitive profile three months after hospital discharge of patients who experiencedin-hosptial delirium.
Methods: This was a prospective cohort study. Fifty-three patients aged 75 years and older were admitted forsurgical repair of acute hip fracture. Before the surgery, baseline characteristics, depressive symptomatology,and global cognitive performance were documented. The presence of delirium was assessed daily duringhospital admission and three months after hospital discharge when patients underwent neuropsychologicalassessment.
Results: Of 27 patients with in-hospital delirium, 5 were still delirious after three months. Patients within-hospital delirium (but free of delirium at follow-up) showed poorer performance than patients withoutin-hospital delirium on tests of global cognition and episodic memory, even after adjustment for age, gender,and baseline cognitive impairment. In contrast, no differences were found on tests of attention. Patientswith in-hospital delirium showed an increase of depressive symptoms after three months. However, deliriumremained associated with poor performance on a range of neuropsychological tests among patients with fewor no signs of depression at follow-up.
Conclusion: Elderly hip fracture patients with in-hospital delirium experience impairments in global cognitionand episodic memory three months after hospital discharge. Our results suggest that inattention, as a cardinalsign of persistent delirium or depressive symptomatology at follow-up, cannot fully account for the poorcognitive outcome associated with delirium.
Key words: delirium, neuropsychology, aged care, longitudinal studies
Introduction
Delirium is a severe neuropsychiatric syndromecharacterized by an acute decline in attentionand cognition (American Psychiatric Association,2000). Although delirium is often viewed as a
Correspondence should be addressed to: Joost Witlox, Department of GeriatricMedicine, Medical Center Alkmaar, PO Box 501, 1800 AM Alkmaar,the Netherlands. Phone: +31-72-5482380; Fax: +31-72-5482197. Email:[email protected]. Received 26 Dec 2012; revision requested 9 Jan 2013; revisedversion received 4 Mar 2013; accepted 24 Mar 2013.
transient and reversible cognitive disorder, researchhas shown that it is associated with long-termcognitive impairment and dementia (Jackson et al.,2004; MacLullich et al., 2009; Witlox et al., 2010).
Neuropsychological test batteries are consideredthe “gold standard” for investigating cognitivefunctioning. Yet, most studies that examined theassociation of delirium with cognitive impairmentmerely used screening instruments which are in-appropriate for fully characterizing and quantifyingdefects in specific cognitive domains (Jackson et al.,

2 J. Witlox et al.
2004). Therefore, the precise nature of the cognitiveimpairments and the extent to which particularcognitive domains are affected after delirium remainuncertain (MacLullich et al., 2009).
A better understanding of the nature of thecognitive impairments following delirium mighthelp to ascertain the value of different hypothesesthat have been proposed to explain the relationshipbetween delirium and cognitive impairment atfollow-up. Delirium may persist for months andpatients with cognitive impairment at follow-upmay in fact experience persistent delirium (Coleet al., 2009). Alternatively, patients with cognitiveimpairment at follow-up may have depressionor have neurodegenerative disease (Lenze et al.,2007; Krogseth et al., 2011). The few studies thatexamined the neuropsychological profiles of elderlypatients after an episode of delirium (Katz et al.,2001; Benoit et al., 2005; Jankowski et al., 2011)have not adequately addressed the possibility thatthe presence of delirium symptoms or depressionmay have influenced performance on cognitive testsat follow-up.
The aim of the present study was to evaluatecognitive performance at follow-up in elderly hipfracture patients who did or did not experiencein-hospital delirium. We used a comprehensiveneuropsychological approach and examined to whatextent inattention, as an important sign of persistentdelirium (Meagher et al., 2010) and depression(Herrmann et al., 2007), is an important featureof the neuropsychological profile of patients whohave had delirium three months earlier during theirhospital admission.
Methods
ParticipantsThis is a prospective cohort study that was nestedwithin a clinical trial that compared the effectivenessof taurine versus placebo in reducing morbidityand one-year mortality in elderly hip fracturepatients aged 75 years and older (Clinicaltrials.gov;registration number NCT00497978). Examiningneuropsychological function, three months afterhospital discharge, was a pre-specified secondaryaim of the trial.
The approval of the regional research ethicscommittee was obtained. All patients gave signedinformed consent. Patients were recruited from aseries of consecutively admitted elderly hip fracturepatients to a non-academic teaching hospital inAlkmaar, the Netherlands. Eligibility was checkedfor all patients aged 75 years and older admittedfor primary surgical repair of hip fracture. Patientswere not eligible if they had no acute trauma,
received a total hip prosthesis, had a pathologicalfracture, were not capable (e.g. dementia in themedical case notes, aphasia, coma) or not willing toprovide informed consent or had contraindicationsregarding the administration of taurine (i.e. renalimpairment defined as a creatinine clearing lessthan 30 mL/min). As these patients are at highrisk for developing delirium, all patients receivedroutine care with prophylactic treatment of 0.5mg haloperidol, three times daily, from the timeof admission until postoperative day three, unlesscontraindications regarding its use were present(Kalisvaart et al., 2005).
All patients who developed delirium duringhospital admission were asked to participate in thefollow-up. A subgroup of patients without deliriumwas selected to participate as controls based on ran-dom selection by a computer-generated randomiza-tion code. Because we were specifically interested inthe effects of in-hospital delirium on neuropsycho-logical test performance three months after hospitaldischarge, we excluded patients with clinicallymanifest delirium at follow-up (Figure 1).
Baseline (preoperative) assessmentBaseline assessment was completed within 12 hoursafter hospital admission and before surgery. Thefollowing demographic variables were documented:age, gender, and educational level. Cognitive func-tioning was assessed with the Mini-Mental StateExamination (MMSE; Folstein et al., 1975), andpre-existent cognitive decline with the InformantQuestionnaire on Cognitive Decline in the Elderly–Short-Form (IQCODE-N; Jorm and Jacomb, 1989;de Jonghe et al., 1997). The Geriatric DepressionScale (GDS) was used as a self-inventory ofdepressive symptomatology (Sheikh and Yesavage,1986; Stek et al., 2004). The number and type ofmedical co-morbidities and medications at home,the American Society of Anesthesiologists (ASA)physical status classification system (AmericanSociety of Anesthesiologists, 2010), and the AcutePhysiology and Chronic Health Evaluation II(APACHE II; Knaus et al., 1985) score wereabstracted from the medical record. Visual acuitywas assessed with the standardized Snellen testfor visual impairment (Hetherington, 1954). Pre-fracture (instrumental) activities of daily living((I)ADL) functioning was assessed by a closerelative or caregiver with the Barthel Index (BI;Mahoney and Barthel, 1965) and the Lawton IADLscale (Lawton and Brody, 1969). Delirium wasdefined according to the criteria of the confusionassessment method (CAM), which consists of anacute onset and fluctuating course of cognitivefunction, inattention, and either disorganized

Neuropsychological sequelae of delirium 3
Number of patients with hip fracture
March 2008 – March 2009N = 257
Number in trial N = 122
- Declined to participate in FU N = 8- Died before FU N = 10- No operation N = 1
- Not able (profound dementia, aphasia, coma) N = 64- Not willing N = 20 - Renal failure N = 20- No operation or transfer to other hospital N = 13- No acute trauma, total hip prothesis, pathological # N = 11- Missed N = 4- Language barrier N = 3
Number in analyses N = 22
Not invited for FU=39
Delirium N = 46
ControlN = 76
Delirium at FU N = 5
Number in analyses N = 26
Delirium N = 27
ControlN = 26
- Declined to participate in FU N = 7- Died before FU N = 2- No operation N = 1
FU = Follow-up
Figure 1. (Colour online) Flow chart.
thinking and/or altered level of consciousness(Inouye et al., 1990). The CAM algorithm wasrated on the basis of an interview with the patientand hospital staff, brief cognitive assessment withthe MMSE and the expanded digit span test(Lindeboom and Matto, 1994), and screening of themedical and nursing records for signs of delirium.The presence of delirium was assessed daily fromthe time of hospital admission until at least the fifthpostoperative day.
For the IQCODE-N, BI, and Lawton IADL,proxies were asked to describe the patient’scondition a week before the fracture as to determinefunction unbiased by the event of hip fracture itselfor any acute or sub-acute event leading to hipfracture.
Three-month follow-up assessmentA neuropsychological test battery was administeredthree months after hospital discharge by two trainedneuropsychologists. The neuropsychological bat-tery was designed to assess multiple cognitivedomains and contained standardized and validatedinstruments. It also included the MMSE, theexpanded digit span test, and the GDS, and tookapproximately one hour to complete. Most patientswere examined at home; some patients preferred tovisit the hospital.
The CAM was used to screen for deliriumat follow-up. CAM positive patients at follow-up were those that demonstrated an acutechange or fluctuation in their mental status plusthe accompanying inattention and disorganizedthinking and/or altered level of consciousness.
The Dutch version of the National AdultReading Test (DART) was used to measure pre-morbid verbal intelligence (Nelson, 1991; Schmandet al., 1992). The DART requires patients to readaloud 50 words with irregular pronunciation.
Episodic memory was examined with the Dutchversion of the verbal learning test, i.e. the GroningenFifteen Words Test (Brand and Jolles, 1985; van derElst et al., 2005). Fifteen words are presented orallyand the patient is asked to repeat as many wordsas possible when the presentation stops. After fivetrials, a 20-minute delay is interspersed at the endof which the patient is asked to recall and recognizethe previously learned words (delayed recall). Weanalyzed (1) the total number of correctly recalledwords summed over five trials; (2) the number ofcorrectly recalled words after the delay; and (3)the number of correctly recognized target and non-target words.
Attention and concentration was first assessedwith the expanded digit span test. In this test, theexaminer reads a string of digits which the patienthas to repeat in either the same (forward) or the

4 J. Witlox et al.
reverse (backward) order (Lindeboom and Matto,1994). The forward and backward tests were ana-lyzed separately with the forward span measuringconcentration, and the backward span measuringworking memory (Lezak et al., 2004). Second, theExpanded Mental Control Task (EMCT), whichconsists of 12 word lists and arithmetic progressionsthat the patient has to recite within a certainamount of time, was administered (Lindeboomet al., 1993). The following measures of the EMCTwere analyzed: (1) the combined total score; (2)total time needed to complete all items; and (3)the total number of errors. Third, a computerizedsimple reaction time (RT) task was used in whichthe patient had to press the space bar as quicklyas possible when the word “YES” appeared onthe screen. The time between stimuli presentationvaried randomly between 1 and 3 seconds. Fortytrials were administered and we analyzed (1) meanreaction time; (2) intra-trial variability of reactiontimes, i.e. standard deviation of reaction times; and(3) number of premature responses, i.e. responseduring the inter-stimulus interval.
The Clock Drawing Test measures visuocon-structive function. Patients are asked to draw a clockand set the hands of the clock at ten past eleven.Points are given for (1) drawing a closed circle; (2)correct ordering of the numbers within the clock;(3) correct spatial location of the numbers withinthe clock; and (4) inserting the hands at the correcttime (Pinto and Peters, 2009).
We administered the Dutch version of the Con-trolled Oral Word Association Test (COWAT) toexamine executive function (Schmand et al., 2008).This verbal fluency task requires patients to name asmany words as possible within 60 seconds beginningwith a target letter specified by the examiner.
Proxies were asked to complete the IQCODE-Nfor the second time with reference to the situationthree months after hospital discharge.
OutcomePerformance on neuropsychological tests threemonths after hospital discharge.
Statistical analysisStatistical calculations were performed using SPSSfor Windows, version 14 (SPSS Inc., Chicago,IL). Quantitative variables are presented as mean(standard deviation, SD) or median (inter-quartilerange, IQR). The χ2 or Fisher exact tests wereused to analyze categorical variables. Continuousvariables were analyzed with Student t testsor Mann–Whitney U tests for between-groupcomparisons and paired t tests or Wilcoxon signedrank tests for within-group comparisons. The
assumption of normality was tested with theKolmogrov–Smirnov test.
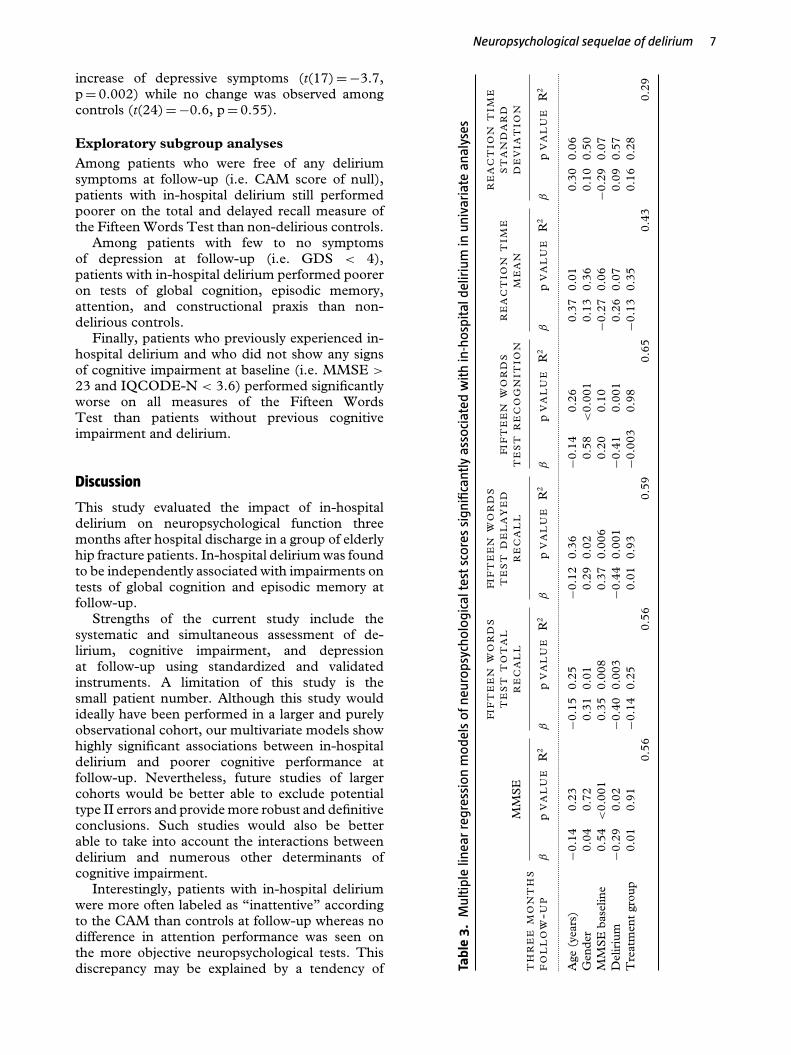
To examine whether delirium is associated withneuropsychological test performance independentof important covariates, we fitted a multiple linearregression model for those neuropsychologicalmeasures that were associated with delirium inunivariate analyses. In the multivariate models,we entered delirium as an independent variabletogether with age, gender, baseline MMSE, andtreatment allocation. These covariates were selecteda priori based on their potential to influenceneuropsychological test performance. Besides thedemographic variables such as age and gender,educational level has also been shown to affectneuropsychological test performance (van der Elstet al., 2005). However, education was not includedas a covariate into our regression models fortwo reasons: (a) preliminary analyses showed thatthe results remained unchanged whether or not thevariable “level of education” was included in themodels; and (b) given our sample size, we aimedto restrict the number of independent variables toa maximum of five. In the regression models thatare presented in the results section, we entered thebaseline MMSE, and not the baseline IQCODE-N,as a measure of pre-existent cognitive impairment.Compared with the IQCODE-N (which measuresintra-individual changes in cognitive functioning),the MMSE provides a score that can more easilybe compared between patients. We performedsensitivity analyses to examine whether inclusion ofthe IQCODE-N (instead of the MMSE) producedsimilar results. The baseline measures of theGDS and IQCODE-N were entered as covariates,instead of the MMSE, in the multivariate modelsthat examined the association between deliriumduring hospitalization and the GDS and IQCODE-N at follow-up. The core assumptions of linearregression modeling were tested for each model.Statistical significance was set at p < 0.05.
Results
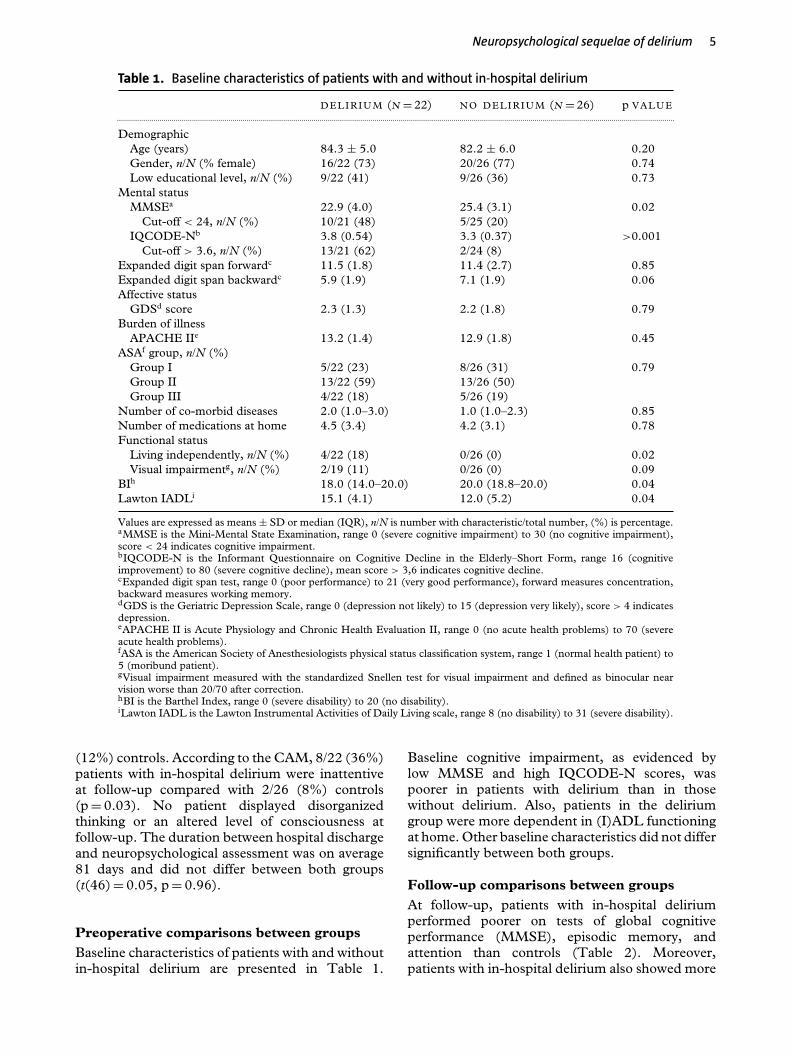
A total of 53 patients with and without deliriumduring hospitalization underwent comprehensiveneuropsychological testing three months afterhospital discharge (Figure 1). Five patients (allof whom also experienced delirium in thehospital) were diagnosed with delirium at follow-upaccording to CAM criteria. Thus, 48 patients freefrom clinically manifest delirium at follow-up, ofwhom 22 had previously experienced delirium, wereavailable for our analyses. Ten of 22 (45%) patientswith previous delirium scored one or two pointson the CAM at follow-up compared with 3/26
Neuropsychological sequelae of delirium 5
Table 1. Baseline characteristics of patients with and without in-hospital delirium
D E LIRIUM (N = 22) NO DELIRIUM (N = 26) p VALUE...................................................................................................................................................................................................................................................................................
DemographicAge (years) 84.3 ± 5.0 82.2 ± 6.0 0.20Gender, n/N (% female) 16/22 (73) 20/26 (77) 0.74Low educational level, n/N (%) 9/22 (41) 9/26 (36) 0.73
Mental statusMMSEa 22.9 (4.0) 25.4 (3.1) 0.02
Cut-off < 24, n/N (%) 10/21 (48) 5/25 (20)IQCODE-Nb 3.8 (0.54) 3.3 (0.37) >0.001
Cut-off > 3.6, n/N (%) 13/21 (62) 2/24 (8)Expanded digit span forwardc 11.5 (1.8) 11.4 (2.7) 0.85Expanded digit span backwardc 5.9 (1.9) 7.1 (1.9) 0.06Affective status
GDSd score 2.3 (1.3) 2.2 (1.8) 0.79Burden of illness
APACHE IIe 13.2 (1.4) 12.9 (1.8) 0.45ASAf group, n/N (%)
Group I 5/22 (23) 8/26 (31) 0.79Group II 13/22 (59) 13/26 (50)Group III 4/22 (18) 5/26 (19)
Number of co-morbid diseases 2.0 (1.0–3.0) 1.0 (1.0–2.3) 0.85Number of medications at home 4.5 (3.4) 4.2 (3.1) 0.78Functional status
Living independently, n/N (%) 4/22 (18) 0/26 (0) 0.02Visual impairmentg, n/N (%) 2/19 (11) 0/26 (0) 0.09
BIh 18.0 (14.0–20.0) 20.0 (18.8–20.0) 0.04Lawton IADLi 15.1 (4.1) 12.0 (5.2) 0.04
Values are expressed as means ± SD or median (IQR), n/N is number with characteristic/total number, (%) is percentage.aMMSE is the Mini-Mental State Examination, range 0 (severe cognitive impairment) to 30 (no cognitive impairment),score < 24 indicates cognitive impairment.bIQCODE-N is the Informant Questionnaire on Cognitive Decline in the Elderly–Short Form, range 16 (cognitiveimprovement) to 80 (severe cognitive decline), mean score > 3,6 indicates cognitive decline.cExpanded digit span test, range 0 (poor performance) to 21 (very good performance), forward measures concentration,backward measures working memory.dGDS is the Geriatric Depression Scale, range 0 (depression not likely) to 15 (depression very likely), score > 4 indicatesdepression.eAPACHE II is Acute Physiology and Chronic Health Evaluation II, range 0 (no acute health problems) to 70 (severeacute health problems).fASA is the American Society of Anesthesiologists physical status classification system, range 1 (normal health patient) to5 (moribund patient).gVisual impairment measured with the standardized Snellen test for visual impairment and defined as binocular nearvision worse than 20/70 after correction.hBI is the Barthel Index, range 0 (severe disability) to 20 (no disability).iLawton IADL is the Lawton Instrumental Activities of Daily Living scale, range 8 (no disability) to 31 (severe disability).
(12%) controls. According to the CAM, 8/22 (36%)patients with in-hospital delirium were inattentiveat follow-up compared with 2/26 (8%) controls(p = 0.03). No patient displayed disorganizedthinking or an altered level of consciousness atfollow-up. The duration between hospital dischargeand neuropsychological assessment was on average81 days and did not differ between both groups(t(46) = 0.05, p = 0.96).
Preoperative comparisons between groupsBaseline characteristics of patients with and withoutin-hospital delirium are presented in Table 1.
Baseline cognitive impairment, as evidenced bylow MMSE and high IQCODE-N scores, waspoorer in patients with delirium than in thosewithout delirium. Also, patients in the deliriumgroup were more dependent in (I)ADL functioningat home. Other baseline characteristics did not differsignificantly between both groups.
Follow-up comparisons between groupsAt follow-up, patients with in-hospital deliriumperformed poorer on tests of global cognitiveperformance (MMSE), episodic memory, andattention than controls (Table 2). Moreover,patients with in-hospital delirium also showed more

6 J. Witlox et al.
Table 2. Global cognitive and affective performance and neuropsychological test scores at threemonths follow-up of patients with and without in-hospital delirium
DELIRIUM (N = 22) NO DELIRIUM (N = 26) p VALUE...............................................................................................................................................................................................................................................................................................
MMSEa 23.1 (4.5) 26.8 (2.7) 0.002IQCODE-Nb 4.0 (0.67) 3.3 (0.43) 0.001GDSc 5.1 (3.5) 2.5 (2.1) 0.004Expanded digit span forwardd 10.5 (2.7) 10.5 (2.8) 0.96Expanded digit span backwardd 5.5 (2.5) 6.6 (1.9) 0.11DARTe 71.2 (15.8) 62.6 (16.9) 0.10Fifteen Words Test total recall 20.3 (5.9) 29.7 (8.2) <0.001Fifteen Words Test delayed recall 1.1 (1.7) 5.1 (2.9) <0.001Fifteen Words Test recognition 22.1 (3.8) 26.5 (3.2) 0.001EMCTf total 17.7 (5.8) 20.3 (2.8) 0.09EMCTf total time (seconds) 272 (123) 224 (80) 0.16EMCTf total error 6.5 (1.8–15.0) 3.0 (1.5–7.5) 0.11Clock drawing 2.0 (1.0–3.0) 3.5 (2.0–4.0) 0.06COWATg total 19.2 (8.1) 23.5 (11.0) 0.25RTh total error 1.0 (0.0–6.0) 1.0 (0.0–3.5) 0.43RTh mean (milliseconds) 543 (383–911) 338 (283–457) 0.01RTh standard deviation (milliseconds) 355 (112–608) 126 (80–225) <0.05BI i 17.0 (12.5–20.0) 19.0 (17.8–20.0) 0.23Lawton IADLj 19.9 (6.4) 16.2 (6.4) 0.14
Values are expressed as means ± SD or median (IQR).aMMSE is the Mini-Mental State Examination, range 0 (severe cognitive impairment) to 30 (no cognitive impairment), score< 24 indicates cognitive impairment.bIQCODE-N is the Informant Questionnaire on Cognitive Decline in the Elderly–Short Form, range 16 (cognitiveimprovement) to 80 (severe cognitive decline), score >57 (i.e. mean score > 3,6) indicates cognitive decline.cGDS is the Geriatric Depression Scale, range 0 (depression not likely) to 15 (depression very likely), score > 4 indicatesdepression.dExpanded digit span test, range 0 (poor performance) to 21 (very good performance), forward measures concentration,backward measures working memory.eDART is the Dutch Adult Reading Test, a measure of pre-morbid verbal intelligence, range 0 (no words correctly pronounced)to 100 (all words correctly pronounced).fEMCT is Expanded Mental Control Task measures attention, range total score 0 (poor performance) to 24 (very goodperformance).gCOWAT is the Controlled Oral Word Association Test, a measure of executive function with higher scores indicating a betterperformance.hRT is the simple Reaction Time task, a measure of attention.iBI is the Barthel Index, range 0 (severe disability) to 20 (no disability).jLawton IADL is the Lawton Instrumental Activities of Daily Living scale, range 8 (no disability) to 31 (severe disability).
signs of depression (GDS) and cognitive decline(IQCODE-N) at follow-up than controls (Table 2).After adjustment for relevant confounders, theassociation between in-hospital delirium and globalcognitive performance (MMSE), episodic memory,and depressive symptoms (GDS) remainedsignificant (Table 3). When sensitivity analyseswere performed, in which the baseline MMSEwas substituted by the baseline IQCODE-N, theassociation between in-hospital delirium and theMMSE at follow-up did not remain significant (datanot shown).
Preoperative to follow-up comparisonsThe degree of change in the MMSE over the courseof three months between patients with and withoutin-hospital delirium was not significant (Table 4).
However, a comparison within groups revealedthat the MMSE of control patients improved overtime (t(24) =−4.5, p < 0.001) while no changewas observed in the delirium group (t(20) =−0.1,p = 0.92).
In contrast, the degree of change over time in theIQCODE-N between both groups was significant(Table 4) with more deterioration notable in thedelirium group (t(15) =−3.2, p = 0.006) but not inthe control group (t(25) = −0.46, p = 0.65).
None of the between- and within-group analysesperformed on the expanded digit span test showedany significant differences between patients withand without in-hospital delirium (data not shown).
A preoperative to follow-up comparison of GDSbetween patients with and without in-hospitaldelirium was significant (Table 4), with patientswho experienced in-hospital delirium showing an
Neuropsychological sequelae of delirium 7
increase of depressive symptoms (t(17) =−3.7,p = 0.002) while no change was observed amongcontrols (t(24) =−0.6, p = 0.55).
Exploratory subgroup analysesAmong patients who were free of any deliriumsymptoms at follow-up (i.e. CAM score of null),patients with in-hospital delirium still performedpoorer on the total and delayed recall measure ofthe Fifteen Words Test than non-delirious controls.
Among patients with few to no symptomsof depression at follow-up (i.e. GDS < 4),patients with in-hospital delirium performed pooreron tests of global cognition, episodic memory,attention, and constructional praxis than non-delirious controls.
Finally, patients who previously experienced in-hospital delirium and who did not show any signsof cognitive impairment at baseline (i.e. MMSE >
23 and IQCODE-N < 3.6) performed significantlyworse on all measures of the Fifteen WordsTest than patients without previous cognitiveimpairment and delirium.
Discussion
This study evaluated the impact of in-hospitaldelirium on neuropsychological function threemonths after hospital discharge in a group of elderlyhip fracture patients. In-hospital delirium was foundto be independently associated with impairments ontests of global cognition and episodic memory atfollow-up.
Strengths of the current study include thesystematic and simultaneous assessment of de-lirium, cognitive impairment, and depressionat follow-up using standardized and validatedinstruments. A limitation of this study is thesmall patient number. Although this study wouldideally have been performed in a larger and purelyobservational cohort, our multivariate models showhighly significant associations between in-hospitaldelirium and poorer cognitive performance atfollow-up. Nevertheless, future studies of largercohorts would be better able to exclude potentialtype II errors and provide more robust and definitiveconclusions. Such studies would also be betterable to take into account the interactions betweendelirium and numerous other determinants ofcognitive impairment.
Interestingly, patients with in-hospital deliriumwere more often labeled as “inattentive” accordingto the CAM than controls at follow-up whereas nodifference in attention performance was seen onthe more objective neuropsychological tests. Thisdiscrepancy may be explained by a tendency of Ta
ble
3.
Mul
tipl
elin
ear
regr
essi
on
mo
dels
ofn
euro
psyc
holo
gica
ltes
tsc
ore
ssi
gnifi
cant
lyas
soci
ated
wit
hin
-hos
pita
ldel
iriu
min
univ
aria
tean
alys
es
MM
SE
FIF
TE
EN
WO
RD
ST
ES
TT
OT
AL
RE
CA
LL
FIF
TE
EN
WO
RD
ST
ES
TD
EL
AY
ED
RE
CA
LL
FIF
TE
EN
WO
RD
ST
ES
TR
EC
OG
NIT
ION
RE
AC
TIO
NT
IME
ME
AN
RE
AC
TIO
NT
IME
ST
AN
DA
RD
DE
VIA
TIO
NT
HR
EE
MO
NT
HS
FO
LL
OW
-UP
βp
VA
LU
ER
2β
pV
AL
UE
R2
βp
VA
LU
ER
2β
pV
AL
UE
R2
βp
VA
LU
ER
2β
pV
AL
UE
R2
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
......
.....
Age
(yea
rs)
−0.1
40.
23−0
.15
0.25
−0.1
20.
36−0
.14
0.26
0.37
0.01
0.30
0.06
Gen
der
0.04
0.72
0.31
0.01
0.29
0.02
0.58
<0.
001
0.13
0.36
0.10
0.50
MM
SE
base
line
0.54
<0.
001
0.35
0.00
80.
370.
006
0.20
0.10
−0.2
70.
06−0
.29
0.07
Del
iriu
m−0
.29
0.02
−0.4
00.
003
−0.4
40.
001
−0.4
10.
001
0.26
0.07
0.09
0.57
Tre
atm
ent
grou
p0.
010.
91−0
.14
0.25
0.01
0.93
−0.0
030.
98−0
.13
0.35
0.16
0.28
0.56
0.56
0.59
0.65
0.43
0.29

8 J. Witlox et al.
Table 3. Continued.
GDS I QCODE-NTHREE M ONTHSFOLLOW-UP β p VALUE R 2 β p VALUE R 2
....................................................................................................................................................................................................................................................................................................................
Age (years) 0.20 0.15 Age (years) 0.13 0.06Gender 0.17 0.19 Gender 0.04 0.58GDS baseline 0.46 0.001 IQCODE-N baseline 0.83 <0.001Delirium 0.39 0.006 Delirium 0.14 0.10Treatment group 0.009 0.94 Treatment group −0.04 0.54
0.42 0.84
MMSE = Mini-Mental State Examination; IQCODE-N = Informant Questionnaire on Cognitive Decline in the Elderly–Short Form;GDS = Geriatric Depression Scale.
Table 4. Degree of change between baseline and three months follow-up for patientswith and without in-hospital delirium
DELIRIUM NO DELIRIUM p VALUE...........................................................................................................................................................................................................................................................
MMSE � 0.1 (4.2) 1.6 (1.8) 0.13IQCODE-N � −0.23 (0.29) −0.02 (0.27) 0.02Expanded Digit Span forward � −1.0 (3.1) −0.4 (2.2) 0.47Expanded Digit Span backward � −0.7 (2.1) −0.4 (2.1) 0.62GDS � 2.7 (3.1) 0.2 (1.7) 0.005
Values are expressed as means ± SD.MMSE = Mini-Mental State Examination; IQCODE-N = Informant Questionnaire on Cognitive Decline inthe Elderly–Short Form; GDS = Geriatric Depression Scale.
raters to label the observed cognitive impairments ashaving an attentional component when the cognitivedeficits are more severe, as they are for patients withprevious delirium.
Several hypotheses have been proposed toexplain the association between delirium andcognitive impairment. One of these explanationssuggests that the high prevalence of cognitiveimpairment at follow-up among patients withprevious delirium may reflect persistence ofdelirium instead (Cole et al., 2009). Indeed,according to the CAM, elderly hip fracture patientswho earlier experienced in-hospital delirium weremost likely to show signs of inattention – thecardinal and required symptom of (persistent)delirium (World Health Organization, 1993;American Psychiatric Association, 2000) – atfollow-up. However, when important baselinecharacteristics were taken into account, differencesbetween both groups in attentional performancecould not be observed on the more objectiveneuropsychological tests. This may imply that thepoorer cognitive performance at the follow-up ofpatients who earlier experienced delirium cannot befully explained by the persistence of a key symptomof delirium. This suggestion is substantiated by oursubgroup analyses that showed that patients with in-hospital delirium, but without delirium symptomsat follow-up (i.e. CAM score of null), performed
poorer on an episodic memory test than controlswho never experienced delirium.
On the contrary, our study also clearlydemonstrates that the persistence of delirium canaffect cognitive outcome at follow-up in somepatients, as almost 20% of our patients within-hospital delirium were excluded because ofpersistent (or recurrent) delirium three months afterhospital discharge.
When explaining the association betweendelirium and cognitive impairment at follow-up, the interrelationship between delirium anddepression may also be of relevance. Depressionis a known risk factor for delirium in elderlyhip fracture patients (Olofsson et al., 2005). Inturn, delirium has been associated with higherdepressive symptom levels months after hip fracture(Lenze et al., 2007), and importantly, depressioncan markedly affect cognitive function (Herrmannet al., 2007). To date, few, if any, studieshave examined the association between deliriumand cognitive impairment at follow-up whilesimultaneously documenting the presence of mooddisturbances. Contrary to previous investigations(Olofsson et al., 2005), depression was not arisk factor for in-hospital delirium in our study.However, patients with in-hospital delirium didshow an increase in depressive symptoms atfollow-up that may (partially) explain their poorer

Neuropsychological sequelae of delirium 9
performance on neuropsychological tests. Yet, theneuropsychological profile of depression in late lifeis typically characterized by diminished processingspeed and impaired executive function (Herrmannet al., 2007). In contrast, our delirium patientsshowed disproportionate memory disturbances. Inaddition, in patients with few or no depressivesymptoms present at follow-up, in-hospital deliriumremained associated with poorer performanceon a range of neuropsychological tests. Theseresults suggest that an increase of depressivesymptoms at follow-up among patients withprevious delirium cannot fully explain their poorercognitive functioning.
As a consequence, studies that include patientswith reversible causes of cognitive impairment,such as persistent delirium and depression, maysystematically overestimate the strength of therelationship between delirium and newly acquiredlong-term cognitive impairment or dementia.
If the presence of delirium symptoms orworsening of depressive symptomatology at follow-up cannot fully explain poor cognitive outcomeof individuals with previous delirium, what otherexplanations can be considered? Delirium mayunmask early or subclinical dementia or may initiateor accelerate a process of cognitive decline. In mostdementias, there is a disproportionate disturbanceon tests of global cognition and episodic memorywith relatively preserved attentional capacities.Thus, the neuropsychological profile of our patientswith previous delirium may seem consistent with thepresence or development of a dementia syndrome.However, to test the hypothesis that deliriumactually initiates neurodegeneration requires a(seemingly) population without dementia atbaseline. Because pre-existent cognitive impairmentis an important predisposing risk factor for deliriumin elderly individuals (Dasgupta and Dumbrell,2006), our findings of poor cognitive performanceat follow-up among patients with in-hospitaldelirium may merely reflect the presence (oracceleration) of baseline cognitive impairment.Indeed, many of our patients who did developdelirium showed signs of pre-fracture cognitivedecline. Therefore, we adjusted our multivariatemodels for baseline cognitive impairment and alsorepeated our analyses in a subgroup of patientsthat did not show any sign of cognitive impairmentat baseline. The results of these analyses suggestthat delirium may be more than a marker ofpre-existent cognitive decline, although the exactmechanism through which delirium is associatedwith later cognitive deterioration remains unclear.Factors that precipitate delirium may incite asequence of events in the brain which maycontribute to the development or acceleration of
cognitive impairment. Microglia and aberrant stressresponses have been suggested to play a role inthis detrimental process (MacLullich et al., 2008;Cunningham et al., 2009; van Gool et al., 2010).
In conclusion, the current investigation providesevidence of the poor cognitive and affectiveprognosis of elderly people after delirium andadds to a growing body of evidence that suggeststhat delirium is associated with various forms ofpoor long-term outcomes (Witlox et al., 2010).Future studies with multiple and longer follow-up periods will be needed to draw definitiveconclusions as to whether cognitive dysfunctionat follow-up after delirium follows a static,fluctuating, gradually resolving or progressivecourse. Moreover, intervention studies are neededto investigate whether the sequelae associated withdelirium can be averted.
Conflict of interest
Funding sources: Dr. van Gool is supported by aZonMw-TOP grant 40-00812-98-10017.
Description of authors’ roles
Joost Witlox contributed to the conceptionand design, acquisition of data, analysis andinterpretation of data, drafting the paper, finalapproval for publication. Chantal J. Slor andRené W.W.M. Jansen undertook analysis andinterpretation of data, critical revision of themanuscript for intellectual content, and finalapproval for publication. Kees J. Kalisvaart, PietEikelenboom, Willem A. van Gool, and Jos F.M.de Jonghe contributed to the conception anddesign, analysis and interpretation of data, criticalrevision of the manuscript for intellectual content,and final approval for publication. Mireille F.M.van Stijn and Alexander P.J. Houdijk contributedto the acquisition of data, critical revision ofthe manuscript for intellectual content, and finalapproval for publication.
Acknowledgments
We would like to thank Gisela Dekker, RN(data acquisition), Ralph Vreeswijk, RN (dataacquisition), Milko van Langen (data acquisition),Tjerk Schoemaker, MSc (data acquisition), EllenSlijkerman, MSc (data acquisition), and Tjeerdvan der Ploeg, MSc (data analysis) for their workon the study. Dr. van Gool is supported by aZonMw-TOP grant 40-00812-98-10017.
Sponsor’s role. None.

10 J. Witlox et al.
Trial name. The Effect of Taurine on Morbidityand Mortality in the Elderly Hip Fracture Patient.Registration number: NCT00497978. URL: http://clinicaltrials.gov/ct2/show/NCT00497978?term=taurine+hip+fracture&rank=1
References
American Psychiatric Association (2000). Diagnostic andStatistical Manual of Mental Health Disorders, 4th edn,TextRev. Washington, DC: American PsychiatricAssociation.
American Society of Anesthesiologists. (2010). ASAPhysical Status Classification System. Available at:http://www.asahq.org/clinical/physicalstatus.html; lastaccessed January 2012.
Benoit, A. G. et al. (2005). Risk factors and prevalence ofperioperative cognitive dysfunction in abdominal aneurysmpatients. Journal of Vascular Surgery, 42, 884–890.
Brand, N. and Jolles, J. (1985). Learning and retrieval rateof words presented auditorily and visually. Journal ofGeneral Psychology, 112, 201–210.
Cole, M. G., Ciampi, A., Belzile, E. and Zhong, L.(2009). Persistent delirium in older hospital patients: asystematic review of frequency and prognosis. Age andAgeing, 38, 19–26.
Cunningham, C. et al. (2009). Systemic inflammationinduces acute behavioral and cognitive changes andaccelerates neurodegenerative disease. Biological Psychiatry,65, 304–312.
Dasgupta, M. and Dumbrell, A. C. (2006). Preoperativerisk assessment for delirium after noncardiac surgery: asystematic review. Journal of the American Geriatrics Society,54, 1578–1589.
de Jonghe, J. F., Schmand, B., Ooms, M. E. and Ribbe,M. W. (1997). Abbreviated form of the informantquestionnaire on cognitive decline in the elderly. Tijdschriftvoor Gerontologie en Geriatrie, 28, 224–229.
Folstein, M. F., Folstein, S. E. and McHugh, P. R.(1975). “Mini-mental state”. A practical method forgrading the cognitive state of patients for the clinician.Journal of Psychiatric Research, 12, 189–198.
Herrmann, L. L., Goodwin, G. M. and Ebmeier, K. P.(2007). The cognitive neuropsychology of depression in theelderly. Psychological Medicine, 37, 1693–1702.
Hetherington, R. (1954). The Snellen chart as a test of visualacuity. Psychologische Forschung, 24, 349–357.
Inouye, S. K., van Dyck, C. H., Alessi, C. A., Balkin, S.,Siegal, A. P. and Horwitz, R. I. (1990). Clarifyingconfusion: the confusion assessment method. A newmethod for detection of delirium. Annals of InternalMedicine, 113, 941–948.
Jackson, J. C., Gordon, S. M., Hart, R. P., Hopkins, R.O. and Ely, E. W. (2004). The association betweendelirium and cognitive decline: a review of the empiricalliterature. Neuropsychology Review, 14, 87–98.
Jankowski, C. J. et al. (2011). Cognitive and functionalpredictors and sequelae of postoperative delirium in elderlypatients undergoing elective joint arthroplasty. Anesthesiaand Analgesia, 112, 1186–1193.
Jorm, A. F. and Jacomb, P. A. (1989). The InformantQuestionnaire on Cognitive Decline in the Elderly(IQCODE): socio-demographic correlates, reliability,validity and some norms. Psychological Medicine, 19,1015–1022.
Kalisvaart, K. J. et al. (2005). Haloperidol prophylaxis forelderly hip-surgery patients at risk for delirium: arandomized placebo-controlled study. Journal of theAmerican Geriatrics Society, 53, 1658–1666.
Katz, I. R., Curyto, K. J., TenHave, T., Mossey, J.,Sands, L. and Kallan, M. J. (2001). Validating thediagnosis of delirium and evaluating its association withdeterioration over a one-year period. American Journal ofGeriatric Psychiatry, 9, 148–159.
Knaus, W. A., Draper, E. A., Wagner, D. P. andZimmerman, J. E. (1985). APACHE II: a severity ofdisease classification system. Critical Care Medicine, 13,818–829.
Krogseth, M., Wyller, T. B., Engedal, K. and Juliebo, V.(2011). Delirium is an important predictor of incidentdementia among elderly hip fracture patients. Dementia andGeriatric Cognitive Disorders, 31, 63–70.
Lawton, M. P. and Brody, E. M. (1969). Assessment ofolder people: self-maintaining and instrumental activities ofdaily living. Gerontologist, 9, 179–186.
Lenze, E. J. et al. (2007). Onset of depression in elderlypersons after hip fracture: implications for prevention andearly intervention of late-life depression. Journal of theAmerican Geriatrics Society, 55, 81–86.
Lezak, M. D., Howieson, D. B. and Loring, D. W. (2004).Orientation and attention. In M. D. Lezak, D. B.Howieson and D. W. Loring (eds.), NeuropsychologicalAssessment (pp. 337–374). New York: Oxford UniversityPress.
Lindeboom, J., Koene, T. and Matto, D. (1993). Thediagnostic value of tests for mental control. Tijdschrift voorGerontologie en Geriatrie, 24, 105–109.
Lindeboom, J. and Matto, D. (1994). Digit series and Knoxcubes as concentration tests for elderly subjects. Tijdschriftvoor Gerontologie en Geriatrie, 25, 63–68.
MacLullich, A. M., Beaglehole, A., Hall, R. J. andMeagher, D. J. (2009). Delirium and long-term cognitiveimpairment. International Review of Psychiatry, 21, 30–42.
MacLullich, A. M., Ferguson, K. J., Miller, T., de Rooij,S. E. and Cunningham, C. (2008). Unravelling thepathophysiology of delirium: a focus on the role of aberrantstress responses. Journal of Psychosomatic Research, 65,229–238.
Mahoney, F. I. and Barthel, D. W. (1965). Functionalevaluation: the Barthel Index. Maryland State MedicalJournal, 14, 61–65.
Meagher, D. J., Leonard, M., Donnelly, S., Conroy, M.,Saunders, J. and Trzepacz, P. T. (2010). A comparisonof neuropsychiatric and cognitive profiles in delirium,dementia, comorbid delirium-dementia and cognitivelyintact controls. Journal of Neurology, Neurosurgery andPsychiatry, 81, 876–881.
Nelson, H. E. (1991). The Revised National Adult ReadingTest: Test Manual. Windsor: NFER-Nelson.
Olofsson, B., Lundstrom, M., Borssen, B., Nyberg, L.and Gustafson, Y. (2005). Delirium is associated withpoor rehabilitation outcome in elderly patients treated for

Neuropsychological sequelae of delirium 11
femoral neck fractures. Scandinivian Journal CaringSciences, 19, 119–127.
Pinto, E. and Peters, R. (2009). Literature review of theClock Drawing Test as a tool for cognitive screening.Dementia and Geriatric Cognitive Disorders, 27,201–213.
Schmand, B., Lindeboom, J. and van Harskamp, F.(1992). De Nederlandse Leestest voor Volwassenen [The DutchAdult Reading Test]. Lisse, the Netherlands: Swets andZeitlinger.
Schmand, B., Groenink, S. C. and van den Dungen, M.(2008). Letter fluency: psychometric properties and Dutchnormative data. Tijdschrift voor Gerontologie en Geriatrie, 39,64–76.
Sheikh, J. I. and Yesavage, J. A. (1986). GeriatricDepression Scale (GDS): recent evidence and developmentof a shorter version. Clinical Gerontologist, 5, 165–173.
Stek, M. L., Gussekloo, J., Beekman, A. T., van Tilburg,W. and Westendorp, R. G. (2004). Prevalence, correlatesand recognition of depression in the oldest old: the Leiden
85-plus study. Journal of Affective Disorders, 78, 193–200.
van der Elst, E. W., Van Boxtel, M. P., Van Breukelen,G. J. and Jolles, J. (2005). Rey’s verbal learning test:normative data for 1855 healthy participants aged 24–81years and the influence of age, sex, education, and mode ofpresentation. Journal of the International NeuropsychologicalSociety, 11, 290–302.
van Gool, W. A., van de Beek, D. and Eikelenboom, P.(2010). Systemic infection and delirium: when cytokinesand acetylcholine collide. Lancet, 375, 773–775.
Witlox, J., Eurelings, L. S., de Jonghe, J. F., Kalisvaart,K. J., Eikelenboom, P. and van Gool, W. A. (2010).Delirium in elderly patients and the risk of postdischargemortality, institutionalization, and dementia: ameta-analysis. Journal of the American Medical Association,304, 443–451.
World Health Organization (1993). International StatisticalClassification of Diseases and Related Health Problems.Geneva: World Health Organization.





























