Embed Size (px)
Citation preview
267
Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie
Vol. XV – Nr. 2 – 2016 CLINICAL ANATOMY
THE EMBRYOLOGYCAL FEATURES OF ATRIOVENTRICULAR SEPTAL DEFECT DIAGNOSED IN THE FETAL LIFE
Raluca Tulin1, S. Oprea1, C. Pantu1, R. Stanciulescu1, B. Andrei2, R.C. Jecan3, Cezarina Voichitoiu4, A. Tulin1, A. Voichitoiu5
“Carol Davila” University of Medicine and Pharmacy, BucharestFaculty of General Medicine1. Department of Anatomy
2. Department of Orthopedics5. Department of Obstetrics and Gynecology
3. “Prof. Dr. Agrippa Ionescu” Clinical Emergency Hospital, BucharestDepartment of Plastic and Reconstructive Surgery
4. Ambulatory and Preventive Medicine, BucharestDiagnostic and Treatment Medical Center
THE EMBRYOLOGYCAL FEATURES OF ATRIOVENTRICULAR SEPTAL DEFECT DIAG-NOSED IN THE FETAL LIFE (Abstract): The term “atrioventricular septal defect” (AVSD) covers a wide spectrum of heart abnormalities characterised by a common atrioventricular junction coexisting with abnormal atrioventricular septation. In ostium primum atrial septal defect (ASD) there are separate atrioventricular orifices despite a common valvar junction, while in complete AVSD the valve itself is also common. This paper focuses on the anatomy, embryology, and imag-ing of common atrioventricular (AV) canal using imagines from a case of complete atrioventricu-lar canal. Common AV canal may be non-syndromic or syndromic. The syndromic including Down syndrome and the heterotaxy syndromes associated with asplenia and polysplenia. There are sta-tistically highly significant differences between Down and non-Down canals, and between as-plenic and polysplenic canals. In humans, the anterior (anterior) and dorsal (inferior) endocardial cushions of the AV canal normally fuse during 34–36 days of fetal life (5th week of fetal life). An understanding of the fusion of endocardial cushions of the AV canal relative to the ventricular and atrial septums helps to explain normal and abnormal development and the classification of AVSD. This malformation is diagnosed in the fetal life but it becomes symptomatic in infancy due to congestive heart failure and failure to develop normally. Diagnosis of AVSD can be suspected from electrocardiographic and chest X-ray findings. Echocardiography confirms it and gives anatomical details. Over time, pulmonary hypertension becomes irreversible, thus precluding the surgical therapy. Medical treatment (digitalis, diuretics and dilators) plays a role only until the moment of surgery, usually performed between the 3rd and 6th month of life. Key-words: ATRIOVENTRIC-ULAR SEPTAL DEFECT, ATRIOVENTRICULAR CANAL, ATRIOVENTRICULAR VALVES
INTRODUCTION
AVSD is a complex cardiac abnormalities characterised by a variable deficiency of the atrioventricular area (crux cordis) in the devel-oping heart. The malformations involve the atrial, ventricular and atrioventricular septum and both atrioventricular valves (mitral/bicus-pid and tricuspid).
AVSD is an uncommon congenital heart dis-ease, accounting for about only 3% of cardiac
malformations. It occurs in two out of every 10,000 live births. Both sexes are equally af-fected but there is a strong association with Down’s syndrome.
Echocardiography is the key tool for the diagnosis and anatomic classification of this mal-formation. It shows the ostium primum atrial septal defect (ASD), with the underlying com-mon atrioventricular valve, and the defect of the ventricular septal inflow.
268
Raluca Tulin et al.
EMBRYOLOGYSeptation of the atrioventricular junction is
brought about by downgrowth of the atrial sep-tum primum, fusion of the endocardial cushions and forward expansion of the vestibular spine between atrial septum and cushions (1).
Thus, atrioventricular canal can result from arrest or interruption of the normal endocar-dial cushion development (2, 3).
The experimental studies showed that tera-togenic factors or even endogenous metabolic factors can result in abnormal development of the atrioventricular region, which may be due to altered apoptosis (4, 5, 6).
The previous studies showed that AVSD tends to be associated with chromosomal abnormali-ties, mainly Down syndrome, del (8p) syndrome, trisomy 9, trisomy 18 (Edwards syndrome) (7, 8).
AVSD with Down syndrome has been less frequently associated with left cardiac anoma-lies than the isolated form (9, 10).
In isolated form the analysis of potential risk factors showed a strong association with mater-nal diabetes and antitussive drugs (11).
In patients with Down syndrome and AVSD there is a strong association with maternal age. In the asplenia syndrome, the AVSD is always present, while it occurs in about 25% of pa-tients with polisplenia (12).
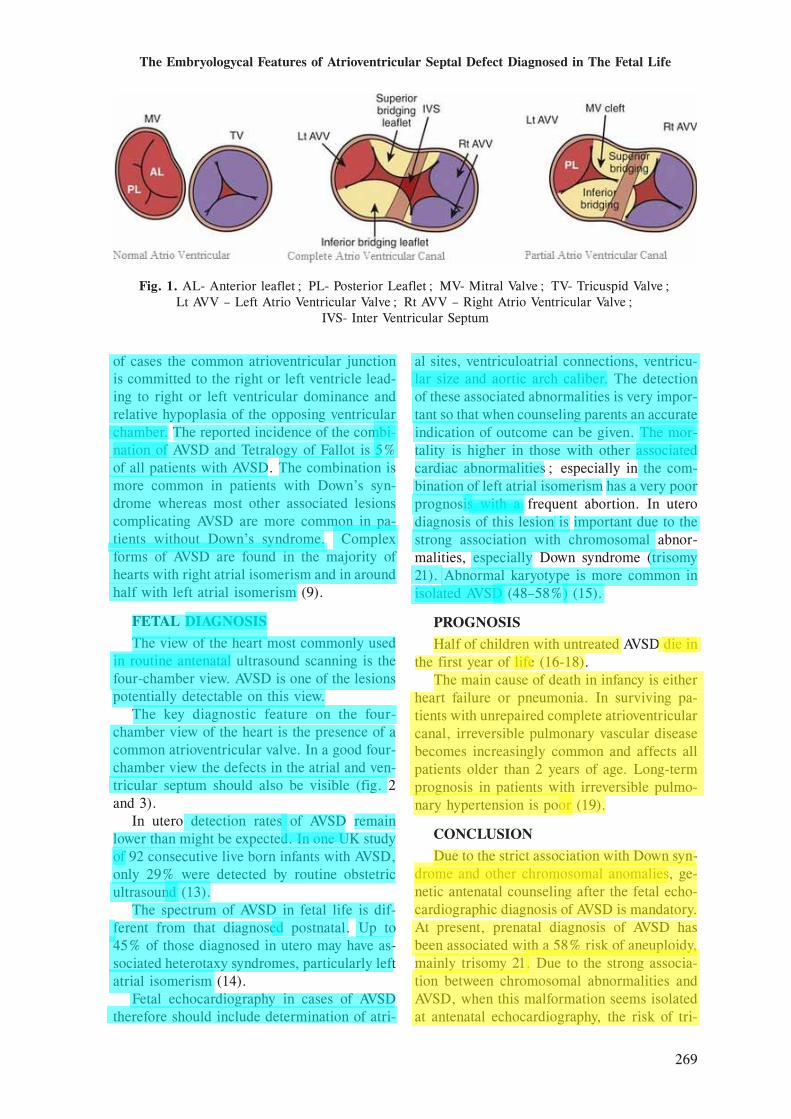
Defects of AVSD can be either complete or partial (fig. 1).1. A Complete Atrio Ventricular Canal (CAVC)
consists of a ventricular septal defect (VSD), an ostium primum atrial septal defect (ASD), and a single AV valve (AVV).
2. Partial Atrio Ventricular Canal (PAVC) has an ostium primum ASD, two separate AVV orifices, and cleft present in the anterior left-sided AVV.The complete form is sub classified as Ras-
telli types A, B, and C. Rastelli anatomical classification was based
on the relationships of the anterior bridging leaflets to the crest of the ventricular septum or right ventricle (RV) papillary muscles.
Type A: the superior bridging leaflet is almost completely adherent to the left ventricle and is firmly attached on the ventricular septum by multiple chordal insertions
Type B: the superior bridging leaflet is at-tached over the ventricular septum by an anom-alous papillary muscle of the right ventricle
Type C: the superior bridging leaflet is not
attached to the ventricular septum (free-floating leaflet)
An echocardiographic examination shows the degree of dysfunction of the common atrioven-tricular valve, as well as the presence of associ-ated cardiac malformations. To date, cardiac catheterisation is not considered as mandatory for the diagnosis, but can be indicated in pa-tients older than 6 months (postnatal) with sus-pected irreversible pulmonary hypertension. Cardiac catheterisation allows accurate quanti-fication of the left-to-right shunt as well as assessment of the degree of pulmonary hyper-tension and the reversibility of the pulmonary artery resistances.
The main characteristic of an AVSD is the presence of a common atrioventricular junc-tion as compared to the separate right and left atrioventricular junction in the normal heart.
Other morphological features include:1. Defects of the muscular and membranous
atrioventricular septum and 2. An ovoid shape of the common atrioven-
tricular junction with moving of the left ven-tricular outflow tract from the place between the tricuspid and bicuspid valve. There is disproportion of outlet and inlet
dimensions of the left ventricle, with the outlet greater than the inlet as compared to the normal heart where both dimensions are similar.
The valve leaflet morphology in AVSD bears little resemblance to the arrangement of the leaflets of normal mitral and tricuspid valves. There are essentially five leaflets, two of which are bridging across the crest of the interven-tricular septum. In complete AVSD there is a space between the bridging leaflets and the atrioventricular valvar orifice is common.
Over the past fifty years the management of the complete form has evolved to primary re-pair in early infancy to prevent the development of pulmonary hypertension. The improved prog-nosis for patients with Down’s syndrome and AVSD has implications for the management of patients diagnosed in the fetal life. The postna-tal and long term outcomes are influenced by the presence of associated defects (usually ven-tricular hypoplasia).
In most patients with AVSD the right and left components of the common atrioventricular junction are comparable and the ventricles are similarly sized (balanced AVSD). In a minority
269
The Embryologycal Features of Atrioventricular Septal Defect Diagnosed in The Fetal Life
of cases the common atrioventricular junction is committed to the right or left ventricle lead-ing to right or left ventricular dominance and relative hypoplasia of the opposing ventricular chamber. The reported incidence of the combi-nation of AVSD and Tetralogy of Fallot is 5% of all patients with AVSD. The combination is more common in patients with Down’s syn-drome whereas most other associated lesions complicating AVSD are more common in pa-tients without Down’s syndrome. Complex forms of AVSD are found in the majority of hearts with right atrial isomerism and in around half with left atrial isomerism (9).
FETAL DIAGNOSISThe view of the heart most commonly used
in routine antenatal ultrasound scanning is the four-chamber view. AVSD is one of the lesions potentially detectable on this view.
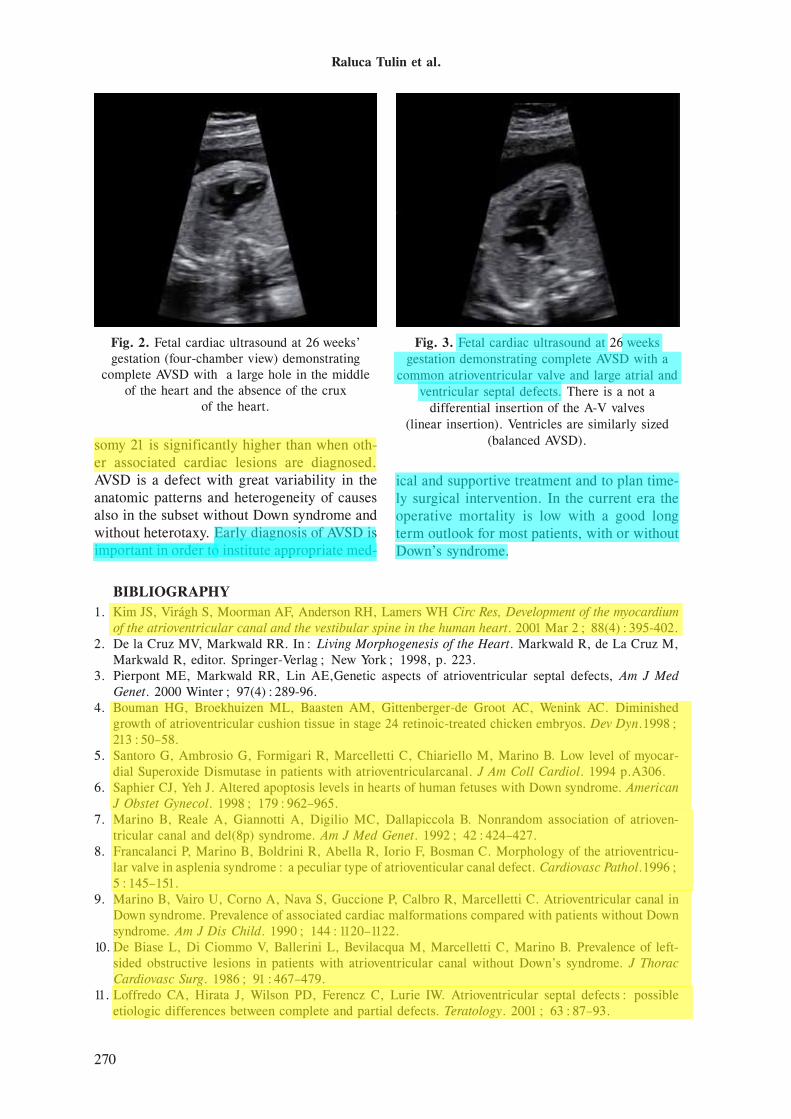
The key diagnostic feature on the four-chamber view of the heart is the presence of a common atrioventricular valve. In a good four-chamber view the defects in the atrial and ven-tricular septum should also be visible (fig. 2 and 3).
In utero detection rates of AVSD remain lower than might be expected. In one UK study of 92 consecutive live born infants with AVSD, only 29% were detected by routine obstetric ultrasound (13).
The spectrum of AVSD in fetal life is dif-ferent from that diagnosed postnatal. Up to 45% of those diagnosed in utero may have as-sociated heterotaxy syndromes, particularly left atrial isomerism (14).
Fetal echocardiography in cases of AVSD therefore should include determination of atri-
al sites, ventriculoatrial connections, ventricu-lar size and aortic arch caliber. The detection of these associated abnormalities is very impor-tant so that when counseling parents an accurate indication of outcome can be given. The mor-tality is higher in those with other associated cardiac abnormalities; especially in the com-bination of left atrial isomerism has a very poor prognosis with a frequent abortion. In utero diagnosis of this lesion is important due to the strong association with chromosomal abnor-malities, especially Down syndrome (trisomy 21). Abnormal karyotype is more common in isolated AVSD (48–58%) (15).
PROGNOSISHalf of children with untreated AVSD die in
the first year of life (16-18).The main cause of death in infancy is either
heart failure or pneumonia. In surviving pa-tients with unrepaired complete atrioventricular canal, irreversible pulmonary vascular disease becomes increasingly common and affects all patients older than 2 years of age. Long-term prognosis in patients with irreversible pulmo-nary hypertension is poor (19).
CONCLUSIONDue to the strict association with Down syn-
drome and other chromosomal anomalies, ge-netic antenatal counseling after the fetal echo-cardiographic diagnosis of AVSD is mandatory. At present, prenatal diagnosis of AVSD has been associated with a 58% risk of aneuploidy, mainly trisomy 21. Due to the strong associa-tion between chromosomal abnormalities and AVSD, when this malformation seems isolated at antenatal echocardiography, the risk of tri-
Fig. 1. AL- Anterior leaflet; PL- Posterior Leaflet; MV- Mitral Valve; TV- Tricuspid Valve; Lt AVV – Left Atrio Ventricular Valve; Rt AVV – Right Atrio Ventricular Valve;
IVS- Inter Ventricular Septum
270
Raluca Tulin et al.
somy 21 is significantly higher than when oth-er associated cardiac lesions are diagnosed. AVSD is a defect with great variability in the anatomic patterns and heterogeneity of causes also in the subset without Down syndrome and without heterotaxy. Early diagnosis of AVSD is important in order to institute appropriate med-
ical and supportive treatment and to plan time-ly surgical intervention. In the current era the operative mortality is low with a good long term outlook for most patients, with or without Down’s syndrome.
Fig. 2. Fetal cardiac ultrasound at 26 weeks’ gestation (four-chamber view) demonstrating
complete AVSD with a large hole in the middle of the heart and the absence of the crux
of the heart.
Fig. 3. Fetal cardiac ultrasound at 26 weeks gestation demonstrating complete AVSD with a
common atrioventricular valve and large atrial and ventricular septal defects. There is a not a
differential insertion of the A-V valves (linear insertion). Ventricles are similarly sized
(balanced AVSD).
BIBLIOGRAPHY1. Kim JS, Virágh S, Moorman AF, Anderson RH, Lamers WH Circ Res, Development of the myocardium
of the atrioventricular canal and the vestibular spine in the human heart. 2001 Mar 2; 88(4):395-402.2. De la Cruz MV, Markwald RR. In: Living Morphogenesis of the Heart. Markwald R, de La Cruz M,
Markwald R, editor. Springer-Verlag; New York; 1998, p. 223.3. Pierpont ME, Markwald RR, Lin AE,Genetic aspects of atrioventricular septal defects, Am J Med
Genet. 2000 Winter; 97(4):289-96.4. Bouman HG, Broekhuizen ML, Baasten AM, Gittenberger-de Groot AC, Wenink AC. Diminished
growth of atrioventricular cushion tissue in stage 24 retinoic-treated chicken embryos. Dev Dyn.1998; 213:50–58.
5. Santoro G, Ambrosio G, Formigari R, Marcelletti C, Chiariello M, Marino B. Low level of myocar-dial Superoxide Dismutase in patients with atrioventricularcanal. J Am Coll Cardiol. 1994 p.A306.
6. Saphier CJ, Yeh J. Altered apoptosis levels in hearts of human fetuses with Down syndrome. American J Obstet Gynecol. 1998; 179:962–965.
7. Marino B, Reale A, Giannotti A, Digilio MC, Dallapiccola B. Nonrandom association of atrioven-tricular canal and del(8p) syndrome. Am J Med Genet. 1992; 42:424–427.
8. Francalanci P, Marino B, Boldrini R, Abella R, Iorio F, Bosman C. Morphology of the atrioventricu-lar valve in asplenia syndrome: a peculiar type of atrioventicular canal defect. Cardiovasc Pathol.1996; 5:145–151.
9. Marino B, Vairo U, Corno A, Nava S, Guccione P, Calbro R, Marcelletti C. Atrioventricular canal in Down syndrome. Prevalence of associated cardiac malformations compared with patients without Down syndrome. Am J Dis Child. 1990; 144:1120–1122.
10. De Biase L, Di Ciommo V, Ballerini L, Bevilacqua M, Marcelletti C, Marino B. Prevalence of left-sided obstructive lesions in patients with atrioventricular canal without Down’s syndrome. J Thorac Cardiovasc Surg. 1986; 91:467–479.
11. Loffredo CA, Hirata J, Wilson PD, Ferencz C, Lurie IW. Atrioventricular septal defects: possible etiologic differences between complete and partial defects. Teratology. 2001; 63:87–93.

271
The Embryologycal Features of Atrioventricular Septal Defect Diagnosed in The Fetal Life
12. Rose V, Izukawa T, Moes CA. Syndromes of asplenia and polysplenia. A review of cardiac and non-cardiac malformations in 60 cases with special reference to diagnosis and prognosis. Br Heart J. 1975; 37:840–852.
13. Ter Heide H, Thompson J D R, Wharton G A. et al Poor sensitivity of routine fetal anomaly scanning ultrasound screening for antenatal detection of atrioventricular septal defect. Heart 2004; 90:916-917.
14. Delisle M F, Sandor G G, Tessier F. et al Outcome of fetuses diagnosed with atrioventricular septal defect. Obstet Gynecol 1999, p.763–767.
15. Huggon I C, Cook A C, Smeeton N C. et al Atrioventricular septal defects diagnosed in fetal life: associated cardiac and extra-cardiac abnormalities and outcome. J Am Coll Cardiol. 2000; 36(2): 593-601.
16. Flyer DC. Endocardial cushion defects. In: Fyler DC, editor. Nadas’ Pediatric Cardiology. Hanley & Belfus, Inc., Philadelphia; 1992. pp. 577–589.
17. Marsico F, Violini R, Calabrò R, et al. Atrioventricular septal defects. Natural history and clinical picture. In: Quero Jimenez M, Arteaga Martinez M, editor. Pediatric Cardiology – Atrioventricular Septal Defects. Ediciones Norma, Madrid; 1988. p194–203.
18. Santoro G, Marino B, Di Carlo D, Formigari R, Santoro G, Marcelletti C, Pasquini L. Patient selec-tion for repair of complete atrioventricular canal guided by echocardiography. Eur J Cardio-Thorac Surg. 1996; 10:439–442.
19. Berger TJ, Blackstone EH, Kirklin JW. Survival and probability of cure without and with surgery in complete atrioventricular canal. Ann Thorac Surg. 1979; 27:104–111.