Embed Size (px)
Citation preview
POSTGRAD. MED. J. (196 I), 37, 646
THE PERSISTENT OSTIUM PRIMUMATRIAL SEPTAL DEFECT
(Partial Persistent Common Atrioventricular Canal)T. HOLMES SELLORS, D.M., M.CH., F.R.C.S.
Thoracic Surgeon, Middlesex Hospital; Surgeon, National Heart Hospital, London Chest Hospital,Harefield Hospital
WALTER SOMERVILLE, M.D., F.R.C.P.Physician, Department of Cardiology, Middlesex Hospital; Cardiologist, Harefield Hospital
AnatomyTHE embryological development of the mitraland tricuspid valves is intimately related to theformation of the adjacent portions of the atrialand ventricular septa. The clinical conditionknown as the complete form of the persistentcommon atrioventricular canal represents an arrestin development of these four structures, the twovalves and the two septa. When a heart with thiscondition is laid open, a continuous defect can beseen involving the lowermost portion of the atrialseptum and the uppermost part of the ventricularseptum. A single atrioventricular valve lies acrossthis defect representing the mitral and tricuspidvalves whose development ceased before theywere evolved into two separate structures eachattached to its own individual valve ring. Thevalve is composed of two large leaflets, anteriorand posterior with smaller lateral leaflets. Twolateral leaflets lie on the right side, the anteriorand posterior leaflets of the tricuspid valve, and asingle lateral leaflet on the left, the posterior cuspof the mitral valve. This, the complete form ofthe persistent common atrioventricular canal, isrelatively rare.
Partial forms of the condition are more commonand the best known of these is the persistentostium primum about which this paper is con-cerned. Apart from its interest to anatomists, itsimportance lies in the fact that it offers a hopefulprospect for surgical correction.The lower boundary of the persistent ostium
primum is the atrioventricular valves, in contrastto the ostium secundum defect which has a lowerrim, however narrow, separating it from the valves.This is the single most important distinguishinganatomical feature between these two types ofatrial septal defect. The mitral valve is almostinvariably deformed by a cleft in the anteriorleaflet. Accessory chordae tendinea attached tothe cleft leaflet may contribute to the incom-
petence of the valve (Edwards, I960). The tri-cuspid valve is usually normal, but uncommonlyits septal leaflet is cleft too. When both mitral andtricuspid valves are malformed in this way, acareful search will usually disclose a small ven-tricular septal defect of the appropriate typedesignating the condition as a complete ratherthan a partial common atrioventricular canal.Ostium primum defects of all sizes have beenseen from a few millimetres across to the situationwhen no trace of an atrial septum exists, the cortriloculare biventriculare or common atrium (Ellis,Kirklin, Swan, DuShane and Edwards, 1959).
In addition to the persistent ostium primumand the common atrium, a wide variety exists ofpartial forms of the common atrioventricular canaldepending on the degree of development of eachof the four components of the canal. Some ofthese are very uncommon and might be classedas collectors' pieces, for instance an isolated cleftmitral or tricuspid valve or both, an isolatedostium primum with normal valves (Blount,Balchum and Gensini, 1956), an isolated defectof the upper part of the ventricular septum orpermutations of these anomalies (Kiely, Adams,Anderson and Lester, I958). In the isolated cleftmitral valve, the anterior or aortic cusp is cleft,the posterior cusp and the tricuspid valve arenormal and the septa intact (Edwards, Dry,Parker, Burchell, Wood and Bulbulian, 1954).The anatomical, electrocardiographic and vector-cardiographic distinction between the isolatedventricular septal defect forming part of thecommon atrioventricular canal and the usual typeof ventricular septal defect have been defined bythe Mayo Clinic workers (Neufeld, Titus,DuShane, Burchell and Edwards, I96I). Theremainder of this paper deals with the ostiumprimum defect with which is implied a cleftmitral valve.
copyright. on M
ay 22, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.433.646 on 1 N
ovember 1961. D
ownloaded from

November I96I SELLORS and SOMERVILLE: Persistent Ostium Primum Atrial Septal Defect
DiagnosisIt has been our practice to repair all atrial
septal defects (ASD) under direct vision by open-heart surgery, the ostium secundum defects underhypothermia and the ostium primum defects usingextra-corporeal circulation. The pre-operativerecognition of the type of defect present is there-fore essential. The operable ostium primumdefect in our experience is about seven times lesscommon than the operable ostium secundumdefect. Each of.the following six diagnostic pro-cedures contributes something to the identificationof the persistent ostium primum, but experiencehas whittled down their number to two crucialtests-auscultation, and the electrocardiogram andvectorcardiogram considered together. The otherfour, the chest radiogram, cardiac catheterization,dye dilution curves and angiocardiography areless specific and less reliable.
Auscultation. An ejection-type systolic murmurfollowed by clear splitting of the second sound isheard in the pulmonary area. By splitting of thesecond sound is meant the audible closure of theaortic valve (A2), followed by closure of the pul-monary valve (P2). The interval between thesetwo elements of the second sound may be constantin inspiration and expiration-' fixed splitting '-or it may be longer during inspiration and shorterduring expiration. This pair of signs, the murmurand the splitting of the second sound, is commonto both types of atrial septal defect. In the ostiumprimum defect, a separate mitral systolic murmuris usually heard at the apex, different in pitchand occupying the whole of systole (pan-systolic).These murmurs are illustrated in Fig. i. Themurmur at the pulmonary area is produced bythe ejection of blood from the right ventricle intothe pulmonary artery. The mitral pan-systolicmurmur is caused by regurgitation of blood fromthe left ventricle to the left atrium through thedeformed and incompetent mitral valve. A similartype of pan-systolic murmur is sometimes heardat the tricuspid area denoting tricuspid regurgita-tion. Identification of the two different pan-systolic murmurs is not always possible by stetho-scope or phonocardiogram. Loudening of themurmur during inspiration and waning duringexpiration used to be thought typical of tricuspidmurmurs, but has not stood the test of experience;many systolic murmurs which behaved in thisway were found at operation to come from themitral valve, the tricuspid valve being normal.A tricuspid diastolic murmur becoming louder ininspiration is heard when a large shunt existsbetween the left and right atria. Occasionally aseparate mitral diastolic murmur is produced bya turbulent blood flow across the deformed mitralvalve. Generally, the same difficulty in precise
i%A 4L?k t .1
SMM
FIG. I.-Phonocardiogram of patient with ostiumprimum defect. At the pulmonary area (PA) anejection-type i,ystolic murmur (SM) is followed bythe two components of the second heart sound(A2 and P2). At the mitral area (MA) the systolicmurmur (SM) begins at the first heart sound andcontinues throughout systole. The diastolic murmur(DM) is recorded at both MA and PA; in thispatient it was loudest at the tricuspid area (notshown). ECG lead II and a venous tracing (VEN.)are recorded above.
identification exists for the diastolic as well as thesystolic murmurs.
These auscultatory findings hold good for themajority of operable ostium primum defects.Naturally they are modified when the defect issmall or the valve nearly normal, but then theclinical diagnosis is not critical from the viewpointof surgical treatment.
Electrocardiogram and Vectorcardiogram. Thereare two features of the electrocardiogram (ECG)which together identify an ostium primum defectwith near certainty in a person having the auscul-tatory pattern described above. They are leftaxis deviation (LAD) and in the chest leads thepattern of right ventricular diastolic overload,sometimes called ' incomplete right bundle branchblock '. This pair of signs is shown in Fig. 2and contrasted with the usual pattern of theostium secundum defect. Two other ECG signssufficiently common to have diagnostic value area notched S wave in lead II (Somerville, I960)and a PR interval of 0.22 sec. or longer.
647
copyright. on M
ay 22, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.433.646 on 1 N
ovember 1961. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
FIG. 2.-ECG of ostium primumASD (above) and ostiumsecundum ASD (below). Inboth, right ventricular dia-stolic overload pattern (incom-plete right bundle branchblock) is shown in VI-2. Theostium primum graph isdistinguished by left axisdeviation, prolonged P-R (0.22sec.) and a notched S wave inlead II. Time marking: o.Isec.
The frontal vectorcardiogram (VCG) as wouldbe expected from the ECG has a characteristicform in ostium primum defects which distin-guishes the primum from the secundum defects(Fig. 3). In ostium primum defects, the loop liesabove the isoelectric point and rotates counter-clockwise, whereas in ostium secundum defects itlies below the isoelectric point and rotates in aclockwise direction (Toscano-Barbosa, Branden-burg and Burchell, 1956).We feel justified in relying strongly on the ECG
and VCG to identify an ostium primum defectwhen an ASD is present. Diagnostic patternswere present in both ECG and VCG in over go%of our surgically-treated cases of ostium primumdefects already reported (Bedford and Sellors,
i96o) and in z8 patients operated on since then.A like degree of confidence in these tests has beenstated by the Mayo Clinic workers (DuShane,Weidman, Brandenburg and Kirklin, I960). Asexperience of these lesions widened, exceptions tothe usual ECG and VCG patterns were noted(Somerville, I96I), but it is unlikely that thesewill be common enough to take from the diag-nostic value of the tests.
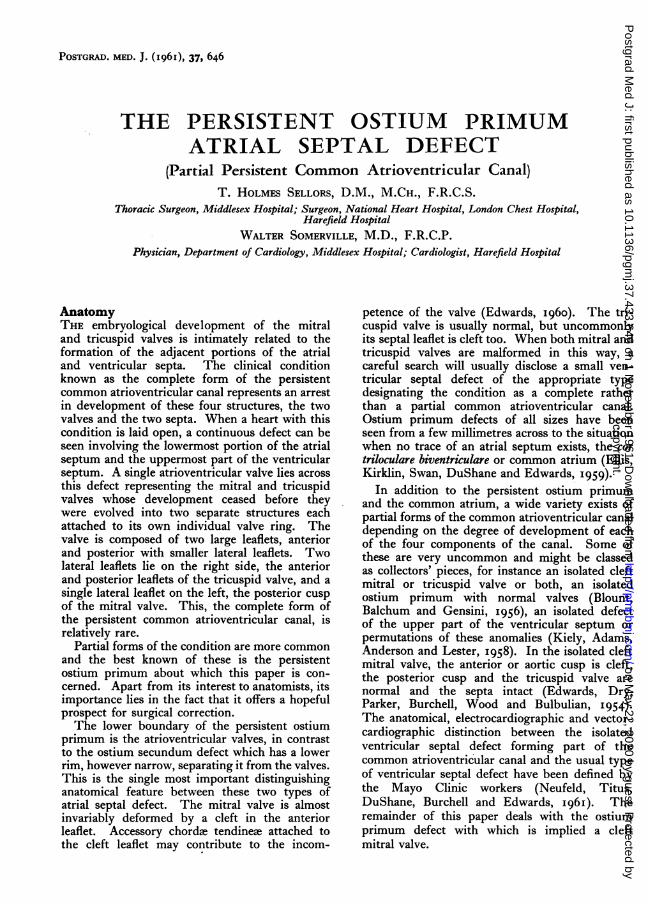
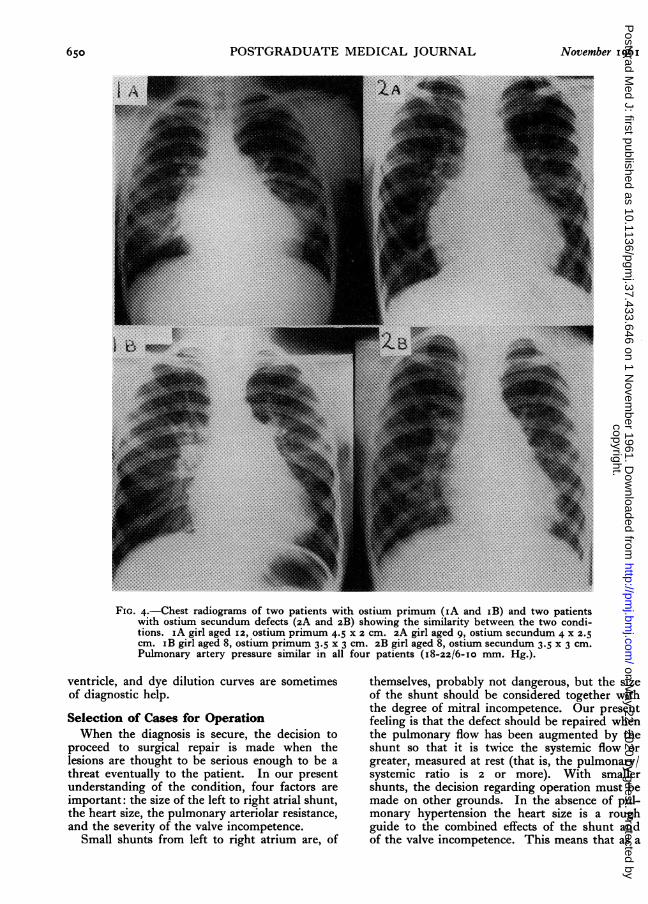
Chest Radiogram. The chest radiogram is indis-pensable for the diagnosis of ASD, but there areno consistent diagnostic features distinguishingostium primum from ostium secundum defects(Fig. 4).
Cardiac Catheterization. A cardiac catheter canbe passed from right to left atrium in the great
648 ATrovember I 96 I
copyright. on M
ay 22, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.433.646 on 1 N
ovember 1961. D
ownloaded from

November I96I SELLORS and SOMERVILLE: Persistent Ostium Primum Atrial Septal Defect
A B
majority of cases of ASD. When the cathetertraverses the ostium primum it lies in close rela-tion to the tricuspid valve or it can be manceuvredinto this position. It can pass directly into theleft ventricle from the right atrium when thetricuspid valve is cleft. The position of thecatheter as it lies in the left ventricle havingpassed through the cleft mitral valve is fairlycharacteristic but unfortunately not diagnosticbecause in certain low ostium secundum defectsthe catheter can take a similar course.A pressure tracing in the left atrium may show
mitral regurgitation if the catheter tip can beplaced in a suitable position. However, theabsence of such a pressure pattern has no diag-nostic value.Dye Dilution Curves. In the ostium secundum
defect, blood returning from the right lung isshunted preferentially into the right atrium be-cause of the proximity of the right pulmonaryvein orifices to the septal defect. Dye dilutioncurves after injections into left and right pulmonaryarteries respectively have characteristically dif-ferent shapes. In certain ostium primum defectsthe curves are similar because, as a rule prefer-ential shunting from the right lung does not occur,the orifices of the right pulmonary veins beingremote from the defect (Wakai, Swan and Wood,1956). Naturally this distinction ceases to existwhen the ostium primum defect is very large, forinstance in its ultimate form, the common atrium,or when a separate ostium secundum defect ispresent.
In the common atrium or cor triloculare biven-triculare, no remnant of atrial septum is present,or it may be represented by a small fringe on aportion of the circumference of a large commonatrial chamber. The atrioventricular valves areabnormal as described earlier; one or both maybe cleft or a common valve may lie across theatrioventricular space. The diagnostic features
FIG. 3.-Frontal vectorcardiograms(diagrammatic) in ASD. Inthe ostium secundum defect(A) the loop lies mainly belowthe isoelectric point and rotatesclockwise. In the ostium pri-mum defect (B) it lies mainlyabove the isoelectric point androtates counter-clockwise.
of this condition are shown by cardiac catheteriza-tion: a shunt from left to right atrium, oxygensaturation in the pulmonary artery equal to or inexcess of that in a systemic artery, and dye dilu-tion curves showing a left-to-right shunt acrossthe ASD when the injection is made in the pul-monary artery, and a right-to-left shunt whenmade in right atrium or superior vena cava (Ellis,Kirklin, Swan, DuShane and Edwards, 1959).
Angiocardiography. Angiocardiograms obtainedfrom injection of contrast medium into rightatrium, right ventricle, pulmonary arteries or leftatrium have no diagnostic value beyond con-firming a shunt from left to right atrium. Leftventricular injection through a catheter passedvia a systemic artery may show mitral regurgitationfollowed by passage of the medium from left toright atrium. In this way an ostium primumdefect may be suspected. These findings are notconclusive, however, because they also occur whenan ostium secundum defect is associated withorganic mitral incompetence, congenital or ac-quired. A further limitation to this technique isthe fact that the cleft mitral valve found withostium primum defects-and indeed the commonatrioventricular valve in complete persistent com-mon atrioventricular canal-cannot always beshown to be incompetent even when the injectionand angiocardiographic techniques are flawless.
In summary, the diagnosis of ostium primumdefects is made mainly on the following points:(i) By auscultation, when a pan-systolic mitralmurmur is present in addition to the usualauscultatory signs of ASD, and (2) from theECG which shows left axis deviation as well asthe pattern of right ventricular diastolic overload(incomplete right bundle branch block) and fromthe VCG when the frontal loop is mainly abovethe isoelectric point and rotates counterclockwise.The position of the cardiac catheter as it passesfrom the right atrium to the left atrium and left
649copyright.
on May 22, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.37.433.646 on 1 Novem
ber 1961. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
FIG. 4.-Chest radiograms of two patients with ostium primum (iA and iB) and two patientswith ostium secundum defects (2A and 2B) showing the similarity between the two condi-tions. sA girl aged I2, ostium primum 4.5 X 2 cm. 2A girl aged 9, ostium secundum 4 X 2.5cm. iB girl aged 8, ostium primum 3.5 x 3 cm. 2B girl aged 8, ostium secundum 3.5 x 3 cm.Pulmonary artery pressure similar in all four patients (i8-22/6-Io mm. Hg.).
ventricle, and dye dilution curves are sometimesof diagnostic help.
Selection of Cases for OperationWhen the diagnosis is secure, the decision to
proceed to surgical repair is made when thelesions are thought to be serious enough to be athreat eventually to the patient. In our presentunderstanding of the condition, four factors areimportant: the size of the left to right atrial shunt,the heart size, the pulmonary arteriolar resistance,and the severity of the valve incompetence.
Small shunts from left to right atrium are, of
themselves, probably not dangerous, but the sizeof the shunt should be considered together withthe degree of mitral incompetence. Our presentfeeling is that the defect should be repaired whenthe pulmonary flow has been augmented by theshunt so that it is twice the systemic flow orgreater, measured at rest (that is, the pulmonary/systemic ratio is 2 or more). With smallershunts, the decision regarding operation must bemade on other grounds. In the absence of pul-monary hypertension the heart size is a roughguide to the combined effects of the shunt andof the valve incompetence. This means that as a
650 November I 96 I
copyright. on M
ay 22, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.433.646 on 1 N
ovember 1961. D
ownloaded from

November I96I SELLORS and SOMERVILLE: Persistent Ostium Primum Atrial Septal Defect
rule operation is not needed when the heart sizeis normal (cardiothoracic ratio 45 or less). A highresistance means obstructive pulmonary arteriolardisease and it carries a heavy operative risk. Thehighest resistance in our series has been 4 units(320 dynes/sec./cm.-5) and we feel that thisfigureshould be taken as the upper limit of safety.When mitral incompetence dominates the clinicalpicture, the decision to operate depends on theseverity of the mitral lesion. The surgical manage-ment of mitral incompetence is described else-where (Barnard and Schrire, I96I).
Surgical TreatmentIn correcting ostium primum defects our
custom has been to employ full body perfusion at2.4 litres/sq. metre body surface at normal bodytemperature, using the Mayo-Gibbon heart-lungmachine.The patient is anaesthetized and placed on the
operating table with a needle or cannula in theright external jugular vein. This is attached to amanometer for measuring the venous pressure.Blood pressure and ECG records are also made.The incision may be vertical, splitting the
sternum longitudinally, or transverse with de-liberate opening into one or both pleural cavities.Though the vertical incision is currently morepopular, we find no difference in the managementand after-pain between the vertical and transverseincisions. The transverse approach gives betterexposure of the atrium and is therefore preferablein atrial septal defects, whereas the vertical in-cision is better placed for ventriculotomy.The incision is enlarged by forceful retraction
and absolute haemostasis ensured before openingthe pericardium. Stay sutures to the cut edgesof the pericardium serve to act as retractors andto bring the heart towards the surface. Thevenx cave are dissected and surrounded withtapes which will later act as tourniquets. Ifpressures are required they are recorded at thisstage.
Cannulation of a femoral or external iliac arterymay be undertaken at the start of the operation,or at this stage as soon as the patient has beengiven a dose of heparin. After the cannula hasbeen inserted, attention is given to venouscannulation.The atrial appendage is lightly clamped and
incised prior to digital exploration, after whichthe venous cannula are inserted, directed into thevenee cava and secured. The heart-lung machine,which will by this time be primed and circu-lating, is then connected to the venous and arterialcannule and perfusion is started. It is customaryto use a period of partial ' by-pass' before
tightening the venous tapes and establishing totalperfusion.When perfusion has been satisfactorily estab-
lished the atrium is incised and blood sucked outthrough the coronary sinus sucker. The atrialincision is carried up to the venous cannulawhich can then be retracted or adjusted whilethe atrial interior is inspected.The appearance of ostium primum defects is
remarkably constant. A well-defined crescenticedge marks the upper limit of the septum andbelow this are the poorly demarcated tricuspidand mitral valve cusps. The upper edge of theventricular septum is usually only recognized onpalpation. It appears as if two delicate veils ofcusp are laid over the ventricular septum and theline between them is roughened or nodular. Themitral valve is always cleft and if the tricuspid islikewise deformed, the ventricular septal edgewill be visible. The cusps themselves may notbe attached to the septum, but in all cases thereis an obvious abnormality of the chordal attach-ments and rotation of the aortic cusp of themitral.The strong probability of regurgitation makes
it imperative to close enough of the cleft mitralvalve to prevent gross reflux, but this repair orclosure must not be carried too far lest the mitralorifice be unduly narrowed. Usually four to fiveclosely placed thread stitches afford a satisfactoryrepair. Abnormal chordal attachments keepingthe valve open during systole must be identifiedand divided, and if the heart has not been sub-jected to artificial arrest, the competence of thevalve can be tested. A similar repair of the tri-cuspid valve should be carried out if this valveis cleft.
Before starting closure of the defect itself itmust be ensured that the valves are firmlyattached to the upper part of the septum.The defect extends the whole width of the
atrioventricular ring blending off at the uppermargin over the aortic sinuses and to the left ofthe coronary sinus below to join the crescenticupper margin. The average short axis of thedefect is I.5 to 2 cm., which is too great fordirect suture. In some early cases in which thedistance was less than I.5 cm. direct suture wasused, but certainly in two cases there was a partiatdisruption at a later date. In consequence, andin spite of inherent objections to buried foreignmaterial, a prosthesis has to be used. Thisoriginally consisted of compressed Ivalon, buthas been succeeded by the more fashionableTeflon felt.The first sutures are placed through the cusps
into the top of the ventricular septum deepenough to obtain a firm hold but placed in the
6Sr
copyright. on M
ay 22, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.433.646 on 1 N
ovember 1961. D
ownloaded from

652 POSTGRADUATE MEDICAL JOURNAL November i196 i
long axis to avoid possible injury to the conductingtissue. Three or four sutures will suffice to formthe base for the patch which is sewn on so as toclose the defect. At the upper border suturesmust be placed superficially to avoid damage tothe aorta, and at the lower border where the atrio-ventricular node lies between the defect and thecoronary sinus. The ECG is carefully watchedfor any sign of heart block. Should it occur wheninserting or tying a suture in this region thestitch must be removed immediately. A hmema-toma or cedema may lead to continued block, butit should not be permanent so long as the ana-tomical integrity of the node and bundle has beenmaintained. When the patch is complete theatrial incision is closed, taking care to exclude airbefore final closure round the venous cannule.Perfusion is then stopped and when the hearthas taken over with good action the cannule areremoved and the action of heparin is neutralizedby an appropriate dose of polybrene.
If there is any question of heart block, two (orthree) electrodes are sutured into the anteriorwall of the right ventricle and passed throughstab incisions in the skin. These are connectedto a pace-maker which can be used if required.The wound is closed after further attention to
haemostasis and the pericardium and pleuralcavities (if opened) are adequately drained bysuction tubes.The complications of the operation are firstly
those of perfusion. Bleeding from coagulation-failure or from the actual heart incision andelectrolyte disturbance from inadequate perfusionare possibilities. The complications referable tothe intracardiac procedures are firstly disorders
in the conduction mechanism, for example, heartblock and arrhythmias. Permanent damage tothe node or bundle is irreversible, but temporaryheart block due to a hkmatoma or traction in theregion of these delicate structures is usually con-trolled by isoprenalin or by pace-making over aperiod of two or three weeks. Bacterial endo-carditis may result from the embedding of aforeign body (patch) in the heart.The repair of the deformed valve may not
leave a perfectly functioning structure and therisk of producing mitral stenosis has been men-tioned. There may also be some measure ofresidual mitral incompetence if a perfectly closingvalve cannot be constructed.
SummaryThe persistent ostium primum atrial septal
defect is a defect in the lowermost portion of theatrial septum. A cleft mitral valve and abnormalchorda tendinew are usually present.When an atrial septal defect has been con-
firmed by the usual techniques, an ostium primumdefect is recognized from auscultation, the electro-cardiogram and vector cardiogram.
Selection for surgical correction is based on thesize of the shunt from left to right atrium, theheart size, the pulmonary arteriolar resistance,and the degree of valve incompetence.
Surgical correction consists of closure of thedefect by a prosthesis and repair of the deformedmitral valve under extra-corporeal circulation.We are indebted to Dr. Evan Bedford and the staff
of the Departments of Thoracic Surgery and Cardiology,Middlesex Hospital, and of the National Heart, LondonChest and Harefield Hospitals.
REFERENCESBANAR, C. N., and SCHRIRE, V. (1961): Surgery of Mitral Incompetence, Postgrad. med. J., 37, 666.BEDFORD, D. E., and SELLORS, T. H. (I960): The Atrio-Ventricular Type of Atrial Septal Defect and its Surgical
Treatment, Brit. Heart Y., 22, 300.BLOUNT, S. G., BALCHUM, 0. J., and GENSINI, G. (1956): The Persistent Ostium Primum Atrial Septal Defect,
Circulation, 13, 499.DUSHANE, J. W., WEIDMAN, W. H., BRANDENBURG, R. O., and KIRKLIN, J. W. (I960): Differentiation of Interatrial
Communications by Clinical Methods, Ibid., 21, 363.EDWARDS, J. E. (I960): The Problem of Mitral Insufficiency Caused by Accessory Chordm Tendinex in Persistent
Common Atrioventricular Canal, Proc. Mayo Clin., 35, 299., DRY, T. J., PARKmE, R. L., BURCHELL, H. B., WOOD, E. H., and BULBULIAN, A. H. (I954): ' An Atlas of CongenitalAnomalies of the Heart and Great Vessels ', p. 35. Springfield, Illinois: Charles C Thomas.
ELLIS, F. H., KIRKLIN, J. W., SWAN, H. J. C., DUSHANE, J. W., and EDWARDS, J. E. (1959): Diagnosis and SurgicalTreatment of Common Atrium (Cor Triloculare-biventriculare), Surgery, 45, I60.
KIELY, B., ADAMS, P., ANDERSON, R. C., and LESTER, R. G. (1958): The Ostium Primum Syndrome, Amer. Y. Dis.Child., 96, 38I.
NEUFELD, H. N., TITUS, J. L., DUSHANE, J. W., BURCHELL, H. B., and EDWARDS, J. E. (I96I): Isolated VentricularSeptal Defect of the Persistent Common Atrioventricular Canal Type, Circulation, 23, 685.
SOMERVILLE, J. (I960): Personal communication.(I96I): The Significance of Atypical Electrocardiograms in Atrio-ventricular and Atrial Septal Defect, Brit.
Heart J., 23, 459.TOSCANO-BARBOSA, E., BRANDENBURG, R. O., and BURCHELL, H. B. (1956): Electrocardiographic Studies of Cases
with Intracardiac Malformations of the Atrioventricular Canal, Proc. Mayo Clin., 31, 5I3.WAKAI, C. S., SWAN, H. J. C., and WOOD, E. H. (1956): Hemodynamic Data and Findings of Diagnostic Value in
Nine Proved Cases of Persistent Common Atrioventricular Canal. Ibid.. u3r. ;oo.
copyright. on M
ay 22, 2020 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.37.433.646 on 1 N
ovember 1961. D
ownloaded from





























