Embed Size (px)
Citation preview

The "cap" technique: Nonmicrosurgicalreattachment of fingertip amputations
With the exception of children, amputations at the level of the lunula survive poorly by directreattachment. Microsurgical replantation is costly and often fails because of poor venous drainage. In a series of seven adult patients the severed tip was filleted and replaced as a "cap" overthe skeletonized distal phalanx of the stump. A 2 mm remnant of germinal matrix was preservedfor nail regrowth. The reconstructed digits, although shortened by an average of 6 mm, givethe ''illusion'' of a normal finger. All were successful with small areas of tip necrosis in two,healing by secondary reepithelialization. Mean static two-point discrimination was 6.5 mm(range, 3 to 10 mm) and pulp pinch was 67% of normal. The "cap" technique of nonmicrosurgicalreattachment is a simple, reliable method of functional preservation of pulp tissue, as well asnormal esthetic appearance of the nail complex. (J HAND SURG 1989;14A:513-18.)
Elliott H. Rose, MD, and Michael S. Norris, MD, Stanford, Calif.,Thomas A. Kowalski, OTR, Burlingame, Calif., and Armand Lucas, MD, andEarl J. Fleegler, MD, Cleveland, Ohio
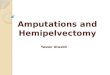
Fig. 1. Palmar schematic view of microarterial anatomy ofdistal phalanx (see text).
In an effort to overcome these problems, we haveapplied the "cap" technique for nonmicrosurgical reattachment of fingertip amputations, The procedure isquick and amenable to outpatient treatment under local
Fingertip amputations at the lunula of thenail are a dilemma to the reconstructive hand surgeon.At this level, survival by direct attachment is poor except in children.' Direct closure of the stump or conventional skin grafting fail to provide an adequate bonyplatform for nail regeneration and may result in a "beak"deformity or residual dysplastic nail remnants. The esthetic appearance of the stump devoid of nail complexis less than optimal.
Microsurgical replantation of the amputated distaldigit is feasible," but is time-consuming, costly, andoften requires adjunctive therapy for treatment of inadequate distal venous drainage (leeches or nail avulsion with topical heparin). 3 Blood loss requiring transfusion is untenable in an acquired immunodeficiencysyndrome (AIDS)-conscious society. Lengthy hospitalization for monitoring of the distal replant is oftenquestioned by third-party insurance reviewers.
From the Division of Plastic Surgery, Stanford University School ofMedicine, Stanford, Calif.; the Occupational Therapy Services,Peninsula Hospital and Medical Center, Burlingame, Calif.; andthe Section Hand Surgery, Department of Plastic and Reconstructive Surgery, Cleveland Clinic Foundation, Cleveland, Ohio.
Received for publication Dec. 4, 1987; accepted in revised form May23, 1988.
No benefits in any form have been received or will be received froma commercial party related directly or indirectly to the subject ofthis article.
Reprint requests: Elliott H. Rose, MD, 1828 EI Camino Real, Suite602, Burlingame, CA 94010.
PROXIMALARTERIAL ARCH
LYING ADJACENTTO BONE
DISTAL
ARTERIESWRAPPINGAROUND
r' ........... TOWARD........... DORSUM OF
DISTALPHALANX
FINE
.:a~.-a-"'iIll.- CAPI LLARYCOMMUNICATIONS
RADIALDIGITALARTERY
PROXIMAL
THE JOURNAL OF HAND SURGERY 513

514 Rose et al,The Journal of
HAND SURGERY
PROX IMAL
DISTAL
B
A
Specimens were fixed in 10% formalin for 3 weeksand dehydrated in increasing concentrations of alcoholfor 24 hours. They were immersed in as: I ratio ofacetone and plastic for 48 hours (SPURR method) andcured at 65 degrees for 72 hours. Chosen block cutsare refined on the diamond cutter before mounting.
On cross-sectional analyses at 4 mm proximal toeponychium and at the lunula, large arterioles werenoted on the palmar aspect of the phalanx and multipleother branches around the periosteum surface (Fig. 3).
Fig. 3. A, Cross-section of digit 4 mrnproximal to eponychium. Pointer (,) represents nutrient vessel entering bone;large arrow (+ ), distal artery; small arrow (t), periostealvascular network; and asterisk (*), flexor tendon. Bone isindicated by X. B, Transverse section at lunula. Long thinarrow (t), is between nail plate and nail bed; small arrow(t ), dorsal periosteal plexus; pointer (1 ), large arteriole inpalmar periosteal area; X is bone.
Technique (Fig. 4)
The procedure is best applied to amputations at thelevel of the lunula where microsurgical anastomosis isdifficult (Fig. 4, A). The amputated part is prepared byremoval of the distal tuft of bone from the compositeremnant of palmar pulp and distal nail bed (Fig. 4, B).
DORSALBRANCH,DIGITAL
ARTERY
DORSALVEIN
DORSALCAPILLARY
NETWORK
DORSAL
PULP FAT(HIGHL Y VASCULAR IZED)
RADIALDIGITALARTERY
PALMAR
ARTERY LY INGADJACENT TO
BONE
ARTERY LYINGIN PULP--';"'IiiTd:.CT'A
Fig. 2. Lateral schematic view from radial side of digestedspecimen (see text).
anesthesia. The reconstructed digit, although shortened, gives the "illusion" of a normal finger by preservation of the nail complex.
Anatomy
The vascular anatomy of the distal phalanx, nail bed,and particularly the periosteum, was studied in 14 freshcadaver specimens that were injected with Batson's No.17 compound via the ulnar artery and partially corrodedwith 30% potassium hydroxide (KOH). Dissections under magnification showed a fairly consistent arterialvascular pattern. The digital vessels cross the distalinterphalangeal (DIP) joint lateral or slightly palmar tothe profundus insertion and sheath and provide a vastnetwork of collaterals beginning at the base of the phalanx. On the palmar aspect (Fig. I) at about the proximal one third the radial and ulnar digital vessels forma delicate arch lying adjacent to bone from which multiple branches arise to envelop the waist and neck ofthe phalanx and pass dorsally to provide another vast,fine reticular network on the periosteum and nail bed.The more distal vessels wrap around the tuft to form afine arch (dorsal "tuft" arch) from which a myriad offine vessels arise to supply the distal tuft and dorsalperiosteum (Fig. 2). Multiple recognizable venulesarise from the area of the nail bed and drain longitudinally into a confluence of two larger veins at the levelof the eponychium.

Vol. 14A, No.3May 1989 Nonmicrosurgical reattachment offingertip amputations 515
B
EPONYCHIUM
GERMINAL MATRIX
A -- ~ r_
,f,iJiJ" AREA EXCISED
LUNULA
NAIL WALL
Fig. 4. A, Amputation through fingertip lunula. B, Distal tuft of bone filleted from palmar pulpand distal nail bed. Shaft of phalanx trimmed circumferentially, leaving 2 mm of germinal matrixon the dorsal surface. C, Composite tip reapplied as a "cap" over skeletalized bone peg.
Fig. 5. A, Case I. Amputation through lunula of small finger. B, Nail growth with minor irregularities after "cap" replantation.
The proximal stump is trimmed circumferentially ofapproximately 6 mm soft tissue sparing at least theproximal 2 mm of the germinal nail matrix on the dorsalsurface (Fig. 4, B). A thin cuff of periosteum andadjacent tissues are preserved to retain the periostealvascular network (Figs. 1 and 2). The distal portion or"cap" is then inset over the skeletonized bone peg as a
"cap" (Fig. 1, C). Under loupe magnification the skinis coapted with 5.0 nylon and the nail matrix with 6.0vicryl. The "male-female union" adds additional boneand periosteal circulation to augment flow to the composite replant.
The procedure is done in the emergency room, withthe patient under digital block anesthesia for treatment

516 Rose et at.
Fig. 6. A, Case 2. Multidigit amputation of long, ring, andsmall fingertips.
of isolated finger injuries. A I /2-inch Penrose wrap isused to maintain a bloodless field and 4.5-power loupemagnification facilitates approximation of "like" tissue.No internal fixation, such as Kirschner wire, is needed.The completed digit is dressed with neomycin ointment(Neosporin), petrolatum gauze (Xeroform), and sterilegauze dressing. A metallic "clamshell" tip splint is applied for moderate compression.
Case reports
Case 1. A l ti-year-old girl severed her right small fingerthrough the nail fold level. The adjacent ring finger was injured less severely (Fig. 5, A). The "cap" procedure restoredher fingertip and returned her to full preinjury employmentwithin 8 weeks. Finger length was 4.6 em compared with 5.1em of the left small finger. DIP motion ranged from 0 to 70degrees. Two-point discrimination was 6 mm. Nail growthhas been good with minor irregularities (Fig. 5, B).
Case 2. A 60-year-old male machinist suffered amputations of the distal left long, ring, and small fingers(Fig. 6, A). The ring and long fingers were replanted microsurgically; the small finger amputation through the lunulawas replaced as a "cap." The long finger replant failed. Thelength of the injured left small finger was 5.2 em comparedwith the right small finger of 5.8 em. The patient returnedto his preinjury job in 6 months. DIP motion was 0 to 50degrees and two-point discrimination was 3 mm. The esthetic appearance of the "cap" digit was favorable comparedwith the microsurgical replanted ring finger (Fig. 6, B). Thedistal phalanx served as a flat platform for nail growth(Fig. 6, C).
Case 3. A 46-year-old man severed the right index, long,and ring fingers on a punch press. The index finger wasreplanted microsurgically. The long finger stump was closed,and the distal part of the long finger placed as a "cap" on the
The Journal ofHAND SURGERY
Fig. 6 Cont'd B-C, Ring finger replanted microsurgicallyand small finger reapplied as nonmicrosurgical "cap." Smalldigit, although shortened, gives illusion of normal finger because of appearance of nail complex.
ring finger. A 0.5 em portion of tip skin necrosed, healingby secondary intention within 8 weeks. He returned to limitedduty 10 weeks after injury. When examined 18 months later,the capped ring finger had a two-point discrimination of7 mm, pulp pinch was 68% of the contralateral ring finger,and DIP motion was 0 to 45 degrees. The right ring fingerwas 6.6 em in length, compared with the left ring finger of7.3 em.
Results
In adult patients seven amputations through the lunulalevel were replanted by the "cap" technique during the

Vol. 14A, No .3May 1989
last 3 years . Follow-up ranged from 6 months to 3 years.Two-point discriminations ranged from 3 mm to 10mm, with an average of 6 .5 mm . Mean shortening ofthe digit , compared with the contralateral uninjured finger was 6 mm. Pulp pinches averaged 67% of the noninjured finger. Hat nail growth has returned in all digits.
Two reattached fingertips had small areas of necrosis,healed by secondary intention, prolonging disability 7to 10 days . None required further surgery. In all patients, the replanted tissue was pale during the first fewdays. In several, a superficial eschar developed, whichseparated spontaneously to reveal epithelialized tissuebeneath. Infections did not develop in any of thepatients.
Discussion
Severed fingertips are often recovered at the sceneof injury and accompany the patient to the emergencydepartment. The hand surgeon must decide whether toreplant the tip or to discard it and resurface the stumpby another method ..~
Local flaps have been described to cover thewound." ? but these often entail bone shortening to permit closure. Grafts of split-thickness or full-thicknessskin not infrequently yield cold intolerance and dysesthesia ." Pedicle flaps from adjacent fingers?or the thenarregion 10. II require staged procedures and may result instiffness and poor sensory return .": 12 although Flatt lJ
suggests this is due to poor design rather than an inherent defect of the thenar flap .
Direct reattachment of the severed tip is the idealreconstruction to preserve length and normal anatomyof the nail complex. Before the microvascular surgeryera, Douglas" meticulously replanted 17 amputationsat various levels with excellent results. Others havebeen unable to duplicate this success. Elsahy' demonstrated 80% viable replantation of distal pulp amputations, but only 20% of amputations through the lunulawere successfully reattached (including two children inthis series).
The physiological objective of the "cap" techniqueis to enhance blood flow to composite tissue of thereattached tip. The area of the "raw" surface of thetransverse amputation stump is 1Tr/ if it is assumed toapproach a circular shape (r, = radius of the finger).After "skeletonizing" bone, the surface area equal s1Tr/ + 2 1Tr21 where 1is the length of the bone exposed(average 6 mm ) and rz the radius of the bone peg (average 3 mm) (Fig. 7). The area for capillary ingrowthis augmented by the circumference of the bone pegmultiplied by its length (net increase approximately45%).
Nonmicros urgical reattachment ojfin gertip amputations 517
AREA EXCISED
__-?>_~~:;;;;::.../ EXPOSED BONE
Fig, 7. Schematic drawing of geometry of soft tissue exci sion .The surface for capillary ingrowth is augmented by the cir cumference of the bone peg multiplied by its length (netincrease approximately 45%). See text for detail s.
Brent " applied the "pocket principle" to enhanceblood flow in distal replants. Severed tips at the lunulawere deepithelialized and buried in a subcutaneouspocket for 11 to 21 days . Only 50% of such replantssurvived compared with 100% in other series.
Yamano? has reported the largest ser ies of distal phalangeal microvascular replantations . His 95% survivalis impressive. "Good daily usc" is reported in 81%.Microvascular replantation , however, is costly in timeand resources. Average operating time in our hands was5.0 hours. 16
The functional results of the nonmicrosurgical "cap"reattachments compare favorably with those achievedmicrosurgically. In our previously-reported series , twopoint discrimination of distal microsurgical replants averaged 9.8 mm and pulp pinches 65% of normal. 16
The "cap" procedure is particularly applicable to amputations at the lunula or distally. The germinal matrixextends 6.0 to 8.0 mm proximal to the eponychium andis responsible for the majority of nail plate growth. "In our experience, preservation of the most proximal2 mm is sufficient for normal nail regeneration. The6 mm bony peg of distal phalanx acts as a platform forflat nail growth. The excised nail wall of the proximalstump contracts to stimulate a new eponychial fold .
In summary , the "cap" technique is a simple andreliable method of eponychial nonmicrosurgical replantation that preserves the specialized pulp tissue ofthe tip. Salvaging the nail complex gives the "illusion"

Rose et al,
of a normal digit, although actually shortened in comparison with the adjacent fingers.
REFERENCESI. Elsahy NI. When to replant a fingertip after its complete
amputation. Plast Reconstr Surg 1977;60: 14-21.2. Yamano Y. Replantation of the amputated distal part of
the fingers. J HAND SURG 1985;lOA:211-18.3. Gordon L, Leitner DW, Buncke HJ, Alpert BD. Partial
nail plate removal after digital replantation as an alternative method of venous drainage. J HAND SURG1985;lOA:360-4.
4. Allen MJ. Conservative treatment of fingertip injuries inadults. Hand 1980; 12:257.
5. Kutler W. A new method for fingertip amputations.JAMA 1947;133:29.
6. Moberg B. Aspects of sensation in reconstructive surgeryof the upper extremity. J Bone Joint Surg 1964;46A:817 .
7. Atasoy E, lokimiolis B, Kasdan M, et al. Reconstructionof amputated fingertip with a triangular volar flap. J BoneJoint Surg 1970;52(A):921.
8. Sturman M, Duran R. Late results of fingertip injuries.J Bone Joint Surg 1963;45(A):289.
9. Kleinert HB, McAlister CG, MacDonald CJ, et al. Acritical evaluation of cross finger flaps. J Trauma1974;14:756.
10. Flatt AE. The thenar flap. J Bone Joint Surg 1957;39(B):80.
The Journal ofHAND SURGERY
11. Beasley R. Reconstruction of amputated fingertips. PlastReconst Surg 1969;44:349.
12. Ma FY, Cheng CY, Chen Y, Leung C. Fingertipinjuries-a prospective study on seven methods oftreatment on 200 cases. Ann Acad Med Singapore1982;11:207.
13. Flatt AE. The care of minor hand injuries. 4th ed.St. Louis: The CY Mosby Co, 1979.
14. Douglas B. Successful replacement of completelyavulsed portions of fingers as composite grafts. PlastReconst Surg 1959;23:213-25.
15. Brent B. Replantation of amputated distal phalangealparts of fingers without vascular anastomoses, using subcutaneous pockets. Plast Reconstr Surg 1979;63:1-8.
16. Rose EH, Norris MS, Kowalski TA. Microsurgical management of complex fingertip injuries: comparison toconventional skin grafting. J Reconstr Microsurg 1988;4:89-98.
17. Urbaniak JR, Roth JM, Nunley JA, Goldner RD, KomanLA. The results of replantation after amputation of asingle finger. J Bone Joint Surg 1985;67A:611-19.
18. May JY, Toth BA, Gardner M. Digital replantation distalto the proximal interphalangeal joint. J HAND SURG1982;7:161-6.
19. Zook EG. Nailbed injuries. Hand Clinics 1985;1:70116.
Infection associated with a palmar skin pit inrecurrent Dupuytren's disease
A clinical case of documented hand infection, caused by a skin pit in a patient with. Dupuytren'scontracture is described. (J HAND SURG 1989;14A:518-20.)
P. Wylock, MD, and H. Vansteenland, MD, Brussels, Belgium
From the Unit of Plastic Surgery, Academic Hospital Vrije Universiteit Brussel, Brussels, Belgium.
Presented at the WinterMeetingof the Dutch Association of Plasticand Reconstructive Surgery, Utrecht,The Netherlands, November7, 1987.
Received for publication Feb. 17, 1988; accepted in revised formJuly 1, 1988.
No benefits in any form have been receivedor will be received froma commercial party related directly or indirectly to the subject ofthis article.
Reprint requests: P. Wylock, MD, Unitof PlasticSurgery, AcademicHospital Vrije Universiteit Brussel, Laarbeeklaan 101, 1090 Brossels, Belgium.
518 THE JOURNAL OF HAND SURGERY
Case report
A 55-year-old man was seen initially in October 1983 withthrobbing pain in the ulnar part of his right hand. He wasknown to have bilateral Dupuytren's disease. There are noother members of his family affected.
A regional fasciectomy had already been done 2 yearsearlier for a contracture of the small finger of his right hand.At that operation a Skoog incision in the palm and a Z-plastyover the base of the small finger was used. The extensiondeficit at the proximal interphalangeal (PIP) joint was reducedfrom 90 degrees to 40 degrees. Healing was uneventful.
The patient returned later in October 1983 with a painful