Embed Size (px)
Citation preview

THE BURDEN OF FUNGALKERATITIS IN INDIA
Philip A. ThomasPhilip A. Thomas MD, PhDMD, PhD
Associate Director (Research) &Associate Director (Research) &Professor of MicrobiologyProfessor of Microbiology
Institute of OphthalmologyInstitute of OphthalmologyJoseph Eye HospitalJoseph Eye HospitalTiruchirapalli 620001Tiruchirapalli 620001Tamilnadu, INDIATamilnadu, INDIA
Philip A. ThomasPhilip A. Thomas MD, PhDMD, PhD
Associate Director (Research) &Associate Director (Research) &Professor of MicrobiologyProfessor of Microbiology
Institute of OphthalmologyInstitute of OphthalmologyJoseph Eye HospitalJoseph Eye HospitalTiruchirapalli 620001Tiruchirapalli 620001Tamilnadu, INDIATamilnadu, INDIA

THE BURDEN OF FUNGAL KERATITIS IN INDIA
KERATITIS•Cornea is the outermostprojecting part of eyeball
•Transparent
•Break in corneal epithelium
•Inflammation of theunderlying corneal stroma
ENDOPHTHALMITIS•Infection of posteriorsegment of eyeball
•Vitreous humour is infected
•Retina & choroid alsoinfected
KERATITIS•Cornea is the outermostprojecting part of eyeball
•Transparent
•Break in corneal epithelium
•Inflammation of theunderlying corneal stroma
ENDOPHTHALMITIS•Infection of posteriorsegment of eyeball
•Vitreous humour is infected
•Retina & choroid alsoinfected
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Medical emergencyMedical emergency
Patients suffer fromPatients suffer fromsignificant pain &significant pain &distressdistress
Rapid initiation ofRapid initiation ofaggressive treatmentaggressive treatment
is needed to halt theis needed to halt the disease processdisease process
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
FUNGAL KERATITIS
Medical emergencyMedical emergency
Patients suffer fromPatients suffer fromsignificant pain &significant pain &distressdistress
Rapid initiation ofRapid initiation ofaggressive treatmentaggressive treatment
is needed to halt theis needed to halt the disease processdisease process
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
FUNGAL KERATITIS

THE BURDEN OF FUNGAL KERATITIS IN INDIASong et al.Song et al. A multiA multi--center, crosscenter, cross--sectional study on the burden of infectioussectional study on the burden of infectious
keratitis in China.keratitis in China. PLoS OnePLoS One. 2014 1;9:e113843. 2014 1;9:e113843
Multi-center, population-based cross-sectional study 8 months 2010; 168,673 individuals of all age groups
participated. Prevalence of past and active infectious keratitis= 0.19 % Prevalence of viral, bacterial, & fungal keratitis= 0.11%,
0.075%, and 0.007%, respectively. 138 cases of infectious corneal blindness in at least one
eye in the study population (prevalence of 0.082% Risk factors identified for infectious corneal blindness
(based on statistical analysis):---ocular trauma---alcoholic consumption---low socioeconomic levels---advanced age & poor education
Song et al.Song et al. A multiA multi--center, crosscenter, cross--sectional study on the burden of infectioussectional study on the burden of infectiouskeratitis in China.keratitis in China. PLoS OnePLoS One. 2014 1;9:e113843. 2014 1;9:e113843
Multi-center, population-based cross-sectional study 8 months 2010; 168,673 individuals of all age groups
participated. Prevalence of past and active infectious keratitis= 0.19 % Prevalence of viral, bacterial, & fungal keratitis= 0.11%,
0.075%, and 0.007%, respectively. 138 cases of infectious corneal blindness in at least one
eye in the study population (prevalence of 0.082% Risk factors identified for infectious corneal blindness
(based on statistical analysis):---ocular trauma---alcoholic consumption---low socioeconomic levels---advanced age & poor education
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIAIn Andhra Pradesh, India Dandona et al. Invest Ophthalmol Vis Sci 2001; 42: 908--Preventable corneal disease, glaucoma, complications of cataractsurgery & amblyopia caused 19% of overall blindness
In Andhra Pradesh Dandona & Dandona, Br J Ophthalmol 2003; 87: 133-- Corneal blindness if an an eye had v/a < 20/200 due to a corneal disease-- Corneal blindness in at least one eye in 86 of 10, 293 (prevalence 0.66%
[0.1% bilateral; 0.56% unilateral])-- Major causes of keratitis during childhood (36.7%), trauma (28.6%) &
keratitis during adulthood (17.7%)--Nearly 95% of all corneal blindness was avoidable-- prevalence significantly higher with ↓ socioeconomic status and ↑ age
In India(2000 through 2020) Dandona et al. Nat Med J India 2001; 14: 327--Success of strategies to prevent 90% of preventable blindness due tocorneal disease & glaucoma by 2020 would prevent 3.6 million blindpersons in 2020 & 29 million blind person-years.
In Andhra Pradesh, India Dandona et al. Invest Ophthalmol Vis Sci 2001; 42: 908--Preventable corneal disease, glaucoma, complications of cataractsurgery & amblyopia caused 19% of overall blindness
In Andhra Pradesh Dandona & Dandona, Br J Ophthalmol 2003; 87: 133-- Corneal blindness if an an eye had v/a < 20/200 due to a corneal disease-- Corneal blindness in at least one eye in 86 of 10, 293 (prevalence 0.66%
[0.1% bilateral; 0.56% unilateral])-- Major causes of keratitis during childhood (36.7%), trauma (28.6%) &
keratitis during adulthood (17.7%)--Nearly 95% of all corneal blindness was avoidable-- prevalence significantly higher with ↓ socioeconomic status and ↑ age
In India(2000 through 2020) Dandona et al. Nat Med J India 2001; 14: 327--Success of strategies to prevent 90% of preventable blindness due tocorneal disease & glaucoma by 2020 would prevent 3.6 million blindpersons in 2020 & 29 million blind person-years.
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Gonzales et al.Gonzales et al. Ophthalmic Epidemiol 1996 ; 3:159Ophthalmic Epidemiol 1996 ; 3:159Retrospective, incidence, general communityRetrospective, incidence, general community--basedbased
study in 1993 in Madurai districtstudy in 1993 in Madurai district
·· 1148 episodes of corneal ulceration noted in medical1148 episodes of corneal ulceration noted in medicalrecords = Incidence of 34 / 100,000 / yearrecords = Incidence of 34 / 100,000 / year
·· Episodes of corneal ulceration seen but not recorded =Episodes of corneal ulceration seen but not recorded =Corrected incidence of 113 / 100,000 / yearCorrected incidence of 113 / 100,000 / year..
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
Gonzales et al.Gonzales et al. Ophthalmic Epidemiol 1996 ; 3:159Ophthalmic Epidemiol 1996 ; 3:159Retrospective, incidence, general communityRetrospective, incidence, general community--basedbased
study in 1993 in Madurai districtstudy in 1993 in Madurai district
·· 1148 episodes of corneal ulceration noted in medical1148 episodes of corneal ulceration noted in medicalrecords = Incidence of 34 / 100,000 / yearrecords = Incidence of 34 / 100,000 / year
·· Episodes of corneal ulceration seen but not recorded =Episodes of corneal ulceration seen but not recorded =Corrected incidence of 113 / 100,000 / yearCorrected incidence of 113 / 100,000 / year..

THE BURDEN OF FUNGAL KERATITISIN INDIA
Whitcher & SrinivasanWhitcher & Srinivasan Br J OphthalmolBr J Ophthalmol 1997 ; 81: 6221997 ; 81: 622
•• Corneal ulceration in the developing world : a silentCorneal ulceration in the developing world : a silentepidemicepidemic
More frequent in developing countries than previouslyMore frequent in developing countries than previouslyrecognisedrecognised ------ EPIDEMIC PROPORTIONSEPIDEMIC PROPORTIONS
New Cases / YearNew Cases / Year Madurai DistrictMadurai District == 50,00050,000 Whole of IndiaWhole of India == 840,000840,000 Developing world =Developing world = > 1,500,000> 1,500,000 U.S.A.U.S.A. == 27,00027,000
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
Whitcher & SrinivasanWhitcher & Srinivasan Br J OphthalmolBr J Ophthalmol 1997 ; 81: 6221997 ; 81: 622
•• Corneal ulceration in the developing world : a silentCorneal ulceration in the developing world : a silentepidemicepidemic
More frequent in developing countries than previouslyMore frequent in developing countries than previouslyrecognisedrecognised ------ EPIDEMIC PROPORTIONSEPIDEMIC PROPORTIONS
New Cases / YearNew Cases / Year Madurai DistrictMadurai District == 50,00050,000 Whole of IndiaWhole of India == 840,000840,000 Developing world =Developing world = > 1,500,000> 1,500,000 U.S.A.U.S.A. == 27,00027,000

THE BURDEN OF FUNGAL KERATITIS IN INDIA
Prevalence: unknownPrevalence: unknownIncidenceIncidence
Tuft andTuft and TulloTullo,, Eye (Eye (LondLond.).) 2009; 23: 13082009; 23: 1308---- O.32 cases per million population/yearO.32 cases per million population/year---- 39 cases over 3 years39 cases over 3 years
Incidence of infectiousIncidence of infectious keratitiskeratitis (per 100,000 /year)(per 100,000 /year)-------- Hong Kong : 6.3Hong Kong : 6.3 Lam et al.,Lam et al., EyeEye 2002; 16 : 6082002; 16 : 608-------- USA : 11.0USA : 11.0 Erie et al.,Erie et al., ArchArch OphthalmolOphthalmol 1993; 111:1993; 111:
11651165------ Bhutan : 339.0Bhutan : 339.0 WHO, SEAWHO, SEA OphthalOphthal, 126 ,2004; 1, 126 ,2004; 1------ Myanmar : 710.0Myanmar : 710.0 WHO, SEAWHO, SEA OphthalOphthal, 126, 2004; 1, 126, 2004; 1
Prevalence: unknownPrevalence: unknownIncidenceIncidence
Tuft andTuft and TulloTullo,, Eye (Eye (LondLond.).) 2009; 23: 13082009; 23: 1308---- O.32 cases per million population/yearO.32 cases per million population/year---- 39 cases over 3 years39 cases over 3 years
Incidence of infectiousIncidence of infectious keratitiskeratitis (per 100,000 /year)(per 100,000 /year)-------- Hong Kong : 6.3Hong Kong : 6.3 Lam et al.,Lam et al., EyeEye 2002; 16 : 6082002; 16 : 608-------- USA : 11.0USA : 11.0 Erie et al.,Erie et al., ArchArch OphthalmolOphthalmol 1993; 111:1993; 111:
11651165------ Bhutan : 339.0Bhutan : 339.0 WHO, SEAWHO, SEA OphthalOphthal, 126 ,2004; 1, 126 ,2004; 1------ Myanmar : 710.0Myanmar : 710.0 WHO, SEAWHO, SEA OphthalOphthal, 126, 2004; 1, 126, 2004; 1
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

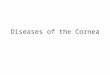
Suppurative keratitis due to fungi as a proportion of total number of cases, by latitude.THE BURDEN OF FUNGAL KERATITIS IN INDIA
Institute of Ophthalmology, Joseph EyeHospital, Tiruchirappalli
Leck A K et al. Br J Ophthalmol 2002;86:1211-1215©2002 by BMJ Publishing Group Ltd.
Institute of Ophthalmology, Joseph EyeHospital, Tiruchirappalli
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Leck et al.,Leck et al., Br J OphthalmolBr J Ophthalmol 2002; 86: 12112002; 86: 1211
39 studies (1976 to 2001)39 studies (1976 to 2001)
23 from Asia (23 from Asia (India 12, Bangladesh 4, Nepal 3, Sri Lanka, Thailand, Hong Kong,India 12, Bangladesh 4, Nepal 3, Sri Lanka, Thailand, Hong Kong,
Singapore)Singapore)
7 from North America (7 from North America (all USAall USA))6 from Africa & Mid East6 from Africa & Mid East ((South Africa (2), Nigeria, Tanzania, Ghana, KSASouth Africa (2), Nigeria, Tanzania, Ghana, KSA))2 from Europe (2 from Europe (LondonLondon) 1 from South America () 1 from South America (ParaguayParaguay))
2% to 58 %2% to 58 % Principal fungal isolatesPrincipal fungal isolatesAspergillusAspergillus spp.spp.---- 17 ;17 ; FusariumFusarium spp.spp.---- 12 ;12 ; CandidaCandida sppspp.. ---- 55
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
Leck et al.,Leck et al., Br J OphthalmolBr J Ophthalmol 2002; 86: 12112002; 86: 1211
39 studies (1976 to 2001)39 studies (1976 to 2001)
23 from Asia (23 from Asia (India 12, Bangladesh 4, Nepal 3, Sri Lanka, Thailand, Hong Kong,India 12, Bangladesh 4, Nepal 3, Sri Lanka, Thailand, Hong Kong,
Singapore)Singapore)
7 from North America (7 from North America (all USAall USA))6 from Africa & Mid East6 from Africa & Mid East ((South Africa (2), Nigeria, Tanzania, Ghana, KSASouth Africa (2), Nigeria, Tanzania, Ghana, KSA))2 from Europe (2 from Europe (LondonLondon) 1 from South America () 1 from South America (ParaguayParaguay))
2% to 58 %2% to 58 % Principal fungal isolatesPrincipal fungal isolatesAspergillusAspergillus spp.spp.---- 17 ;17 ; FusariumFusarium spp.spp.---- 12 ;12 ; CandidaCandida sppspp.. ---- 55
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Shah et al.,Shah et al., Br J OphthalmolBr J Ophthalmol 2011; 95: 7622011; 95: 762
Highest % of bacterial corneal ulcersHighest % of bacterial corneal ulcers ---- from North America, Australia,from North America, Australia,Netherlands, SingaporeNetherlands, Singapore
Highest % of fungal corneal ulcersHighest % of fungal corneal ulcers –– India, NepalIndia, Nepal
statistically significant coefficient correlations between gross nationalstatistically significant coefficient correlations between gross nationalincome and percentages of :income and percentages of :
----bacterial K (0.85 [95%CI 0.68 to 0.91) &bacterial K (0.85 [95%CI 0.68 to 0.91) &---- FUNGAL KERATITISFUNGAL KERATITIS ((--0.81 [95% CI0.81 [95% CI --0.9 to0.9 to --0.66)0.66)
Mycotic cause in 1.2 % to 62 % of Inf. keratitisMycotic cause in 1.2 % to 62 % of Inf. keratitisRitterband et al.,Ritterband et al., CorneaCornea 2006; 25: 2642006; 25: 264Xie et al.,Xie et al., OphthalmologyOphthalmology 2006; 113: 19432006; 113: 1943Nath et al.,Nath et al., Indian J OphthalmolIndian J Ophthalmol 2011; 59:2672011; 59:267
Shah et al.,Shah et al., Br J OphthalmolBr J Ophthalmol 2011; 95: 7622011; 95: 762
Highest % of bacterial corneal ulcersHighest % of bacterial corneal ulcers ---- from North America, Australia,from North America, Australia,Netherlands, SingaporeNetherlands, Singapore
Highest % of fungal corneal ulcersHighest % of fungal corneal ulcers –– India, NepalIndia, Nepal
statistically significant coefficient correlations between gross nationalstatistically significant coefficient correlations between gross nationalincome and percentages of :income and percentages of :
----bacterial K (0.85 [95%CI 0.68 to 0.91) &bacterial K (0.85 [95%CI 0.68 to 0.91) &---- FUNGAL KERATITISFUNGAL KERATITIS ((--0.81 [95% CI0.81 [95% CI --0.9 to0.9 to --0.66)0.66)
Mycotic cause in 1.2 % to 62 % of Inf. keratitisMycotic cause in 1.2 % to 62 % of Inf. keratitisRitterband et al.,Ritterband et al., CorneaCornea 2006; 25: 2642006; 25: 264Xie et al.,Xie et al., OphthalmologyOphthalmology 2006; 113: 19432006; 113: 1943Nath et al.,Nath et al., Indian J OphthalmolIndian J Ophthalmol 2011; 59:2672011; 59:267
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA
Ibrahim et al.Ibrahim et al. PLoS One.PLoS One. 2012; 7:e33775.2012; 7:e33775. retrospective study of antifungal eye drops
sales from only authorised pharmaceuticalophthalmologic laboratory in Brazil (6 years)
26,087 antifungal eye drop units sold (mean= 2.3 / patient).
Significant variation in antifungal sales duringthe year.
By linear regression a significant associationbetween reduced relative humidity &antifungal drug sales (R2 = 0.17,p<0.01).
Ibrahim et al.Ibrahim et al. PLoS One.PLoS One. 2012; 7:e33775.2012; 7:e33775. retrospective study of antifungal eye drops
sales from only authorised pharmaceuticalophthalmologic laboratory in Brazil (6 years)
26,087 antifungal eye drop units sold (mean= 2.3 / patient).
Significant variation in antifungal sales duringthe year.
By linear regression a significant associationbetween reduced relative humidity &antifungal drug sales (R2 = 0.17,p<0.01).Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIAAbsolute numbersAbsolute numbers
---- ~~ 340 cases/year340 cases/year –– single centre (southern India)single centre (southern India)Bharathi et al.Bharathi et al. OphthalmolOphthalmol EpidemiolEpidemiol 2007; 14:612007; 14:61
---- ~~ 200 cases/year200 cases/year –– single centre (central China)single centre (central China)Wang et al.Wang et al. Clin Experiment OphthalmolClin Experiment Ophthalmol 2009; 37:7632009; 37:763
---- ~~ 100 cases/year100 cases/year –– single centresingle centreXie et al.,Xie et al., OphthalmologyOphthalmology 2006; 113: 19432006; 113: 1943Nath et al.,Nath et al., Indian J OphthalmolIndian J Ophthalmol 2011; 59:2672011; 59:267Sengupta et al.,Sengupta et al., Indian J OphthalmolIndian J Ophthalmol 2011; 59:2912011; 59:291
---- ~~ 100 cases/year100 cases/year –– 11 centres (USA)11 centres (USA)Keay et al.Keay et al. OphthalmologyOphthalmology 2011; 118; 9202011; 118; 920
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
Absolute numbersAbsolute numbers
---- ~~ 340 cases/year340 cases/year –– single centre (southern India)single centre (southern India)Bharathi et al.Bharathi et al. OphthalmolOphthalmol EpidemiolEpidemiol 2007; 14:612007; 14:61
---- ~~ 200 cases/year200 cases/year –– single centre (central China)single centre (central China)Wang et al.Wang et al. Clin Experiment OphthalmolClin Experiment Ophthalmol 2009; 37:7632009; 37:763
---- ~~ 100 cases/year100 cases/year –– single centresingle centreXie et al.,Xie et al., OphthalmologyOphthalmology 2006; 113: 19432006; 113: 1943Nath et al.,Nath et al., Indian J OphthalmolIndian J Ophthalmol 2011; 59:2672011; 59:267Sengupta et al.,Sengupta et al., Indian J OphthalmolIndian J Ophthalmol 2011; 59:2912011; 59:291
---- ~~ 100 cases/year100 cases/year –– 11 centres (USA)11 centres (USA)Keay et al.Keay et al. OphthalmologyOphthalmology 2011; 118; 9202011; 118; 920
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
>50 % of oculomycoses>50 % of oculomycoses Srinivasan et al.,Srinivasan et al., ActaActaOphthalmolOphthalmol 1991; 69: 7441991; 69: 744
2 distinct forms due to:2 distinct forms due to:----filamentous fungifilamentous fungi----yeasts & yeastyeasts & yeast--likelike
fungifungi
THE BURDEN OF FUNGAL KERATITISIN INDIA
>50 % of oculomycoses>50 % of oculomycoses Srinivasan et al.,Srinivasan et al., ActaActaOphthalmolOphthalmol 1991; 69: 7441991; 69: 744
2 distinct forms due to:2 distinct forms due to:----filamentous fungifilamentous fungi----yeasts & yeastyeasts & yeast--likelike
fungifungi
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

Scedosporium
THE BURDEN OF FUNGAL KERATITIS IN INDIAAetiological Agents of Filamentous FUNGAL KERATITIS
Fusarium LasiodiplodiaBipolaris
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIAAetiological Agents of Filamentous FUNGAL KERATITIS
Auerswaldia lignicola
Colletotrichum dematium
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
Auerswaldia lignicola

THE BURDEN OF FUNGAL KERATITISIN INDIA
Filamentous FUNGAL KERATITISFilamentous FUNGAL KERATITIS IncreasedIncreased frequency towards tropical latitudes (wind,frequency towards tropical latitudes (wind,temperature, rainfall)temperature, rainfall)Leck et al.,Leck et al., Br J OphthalmoBr J Ophthalmol 2002; 86: 1211l 2002; 86: 1211
IncreasedIncreased CurvulariaCurvularia keratitis during hot moisterkeratitis during hot moistersummer months along Gulf of Mexicosummer months along Gulf of MexicoWilhelmus,Wilhelmus, Am J OphthalmolAm J Ophthalmol 2005; 140: 11562005; 140: 1156
Tends to occur more frequently in adults & elderly thanTends to occur more frequently in adults & elderly thanin children (in children (<< 16 yr)16 yr) Parmar et al.,Parmar et al., CorneaCornea 2006; 25: 2642006; 25: 264
OccupationOccupation--relatedrelated Gopinathan et al.,Gopinathan et al., CorneaCornea 2002;2002; 21: 55521: 555
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
THE BURDEN OF FUNGAL KERATITISIN INDIA
Filamentous FUNGAL KERATITISFilamentous FUNGAL KERATITIS IncreasedIncreased frequency towards tropical latitudes (wind,frequency towards tropical latitudes (wind,temperature, rainfall)temperature, rainfall)Leck et al.,Leck et al., Br J OphthalmoBr J Ophthalmol 2002; 86: 1211l 2002; 86: 1211
IncreasedIncreased CurvulariaCurvularia keratitis during hot moisterkeratitis during hot moistersummer months along Gulf of Mexicosummer months along Gulf of MexicoWilhelmus,Wilhelmus, Am J OphthalmolAm J Ophthalmol 2005; 140: 11562005; 140: 1156
Tends to occur more frequently in adults & elderly thanTends to occur more frequently in adults & elderly thanin children (in children (<< 16 yr)16 yr) Parmar et al.,Parmar et al., CorneaCornea 2006; 25: 2642006; 25: 264
OccupationOccupation--relatedrelated Gopinathan et al.,Gopinathan et al., CorneaCornea 2002;2002; 21: 55521: 555
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA
SaadSaad--Hussein et al.,Hussein et al., East Mediterr Health JEast Mediterr Health J 2011; 17: 4682011; 17: 468
Statistically significantStatistically significant ↑↑ in relative frequencyin relative frequencyof FK (1997of FK (1997--2007) in greater Cairo area2007) in greater Cairo area
Rise correlated significantly withRise correlated significantly with---- ↑↑ minimum temperatureminimum temperature---- ↑↑ maximum atmospheric humiditymaximum atmospheric humidity
↑↑ in COin CO22 emissions & surface temperatureemissions & surface temperature
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
SaadSaad--Hussein et al.,Hussein et al., East Mediterr Health JEast Mediterr Health J 2011; 17: 4682011; 17: 468
Statistically significantStatistically significant ↑↑ in relative frequencyin relative frequencyof FK (1997of FK (1997--2007) in greater Cairo area2007) in greater Cairo area
Rise correlated significantly withRise correlated significantly with---- ↑↑ minimum temperatureminimum temperature---- ↑↑ maximum atmospheric humiditymaximum atmospheric humidity
↑↑ in COin CO22 emissions & surface temperatureemissions & surface temperature
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIAFilamentous FUNGAL KERATITISFilamentous FUNGAL KERATITIS
Seasonal occurrenceSeasonal occurrence
During paddy harvesting in Assam (Jan & Feb)During paddy harvesting in Assam (Jan & Feb) Nath et al. 2011Nath et al. 2011
Higher between September to December (central China)Higher between September to December (central China)Wang et al.Wang et al. Clin Experiment OphthalmolClin Experiment Ophthalmol 2009; 37: 7632009; 37: 763
Fungi cultured significantly more frequently duringFungi cultured significantly more frequently duringsummer months (Australia)summer months (Australia) Green et al.Green et al. CorneaCornea 2008; 27:332008; 27:33
Incidence ofIncidence of FUNGAL KERATITISFUNGAL KERATITIS higher between June & Sept (southern India).higher between June & Sept (southern India). Bharathi etBharathi etal.al. Ophthalmic EpidemiolOphthalmic Epidemiol 2007; 14:612007; 14:61
Highest during harvest seasons, including summer and autumn (northern China)Highest during harvest seasons, including summer and autumn (northern China). Xie et al.. Xie et al.OphthalmologyOphthalmology 2006; 113: 19432006; 113: 1943
Highest sales of antifungal eye drops during 3Highest sales of antifungal eye drops during 3rdrd quarter of year (climate drier, agricultural activityquarter of year (climate drier, agricultural activitymore intense in Brazil during this period) ? a correlation with amore intense in Brazil during this period) ? a correlation with a ↑ed↑ed incidence of fungal keratitis.incidence of fungal keratitis.Ibrahim et al.Ibrahim et al. PLoS One.PLoS One. 2012; 7:e33775.2012; 7:e33775.
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
THE BURDEN OF FUNGAL KERATITIS IN INDIAFilamentous FUNGAL KERATITISFilamentous FUNGAL KERATITIS
Seasonal occurrenceSeasonal occurrence
During paddy harvesting in Assam (Jan & Feb)During paddy harvesting in Assam (Jan & Feb) Nath et al. 2011Nath et al. 2011
Higher between September to December (central China)Higher between September to December (central China)Wang et al.Wang et al. Clin Experiment OphthalmolClin Experiment Ophthalmol 2009; 37: 7632009; 37: 763
Fungi cultured significantly more frequently duringFungi cultured significantly more frequently duringsummer months (Australia)summer months (Australia) Green et al.Green et al. CorneaCornea 2008; 27:332008; 27:33
Incidence ofIncidence of FUNGAL KERATITISFUNGAL KERATITIS higher between June & Sept (southern India).higher between June & Sept (southern India). Bharathi etBharathi etal.al. Ophthalmic EpidemiolOphthalmic Epidemiol 2007; 14:612007; 14:61
Highest during harvest seasons, including summer and autumn (northern China)Highest during harvest seasons, including summer and autumn (northern China). Xie et al.. Xie et al.OphthalmologyOphthalmology 2006; 113: 19432006; 113: 1943
Highest sales of antifungal eye drops during 3Highest sales of antifungal eye drops during 3rdrd quarter of year (climate drier, agricultural activityquarter of year (climate drier, agricultural activitymore intense in Brazil during this period) ? a correlation with amore intense in Brazil during this period) ? a correlation with a ↑ed↑ed incidence of fungal keratitis.incidence of fungal keratitis.Ibrahim et al.Ibrahim et al. PLoS One.PLoS One. 2012; 7:e33775.2012; 7:e33775.
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Risk factors for filamentous FUNGAL KERATITISRisk factors for filamentous FUNGAL KERATITIS TraumaTrauma --Bharathi et al 2007; Wong et al 1997; Leck et alBharathi et al 2007; Wong et al 1997; Leck et al
2002; Xie et al 2006; Gopinathan et al 2002).2002; Xie et al 2006; Gopinathan et al 2002).
Injury caused by plants show a 3.8 fold greater chance ofInjury caused by plants show a 3.8 fold greater chance ofpositive fungal culture.positive fungal culture. Cariello et al.Cariello et al. Int OphthalmolInt Ophthalmol 2011; 31: 1972011; 31: 197
CorticosteroidsCorticosteroids(Stern & Buttross,(Stern & Buttross, OphthalmologyOphthalmology 1991; 98:847)1991; 98:847)
‘allergic’ conjunctivitis‘allergic’ conjunctivitis
? traditional eye medicines? traditional eye medicines
Institute of Ophthalmology,Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology,Joseph Eye Hospital, Tiruchirappalli
TraumaTrauma --Bharathi et al 2007; Wong et al 1997; Leck et alBharathi et al 2007; Wong et al 1997; Leck et al2002; Xie et al 2006; Gopinathan et al 2002).2002; Xie et al 2006; Gopinathan et al 2002).
Injury caused by plants show a 3.8 fold greater chance ofInjury caused by plants show a 3.8 fold greater chance ofpositive fungal culture.positive fungal culture. Cariello et al.Cariello et al. Int OphthalmolInt Ophthalmol 2011; 31: 1972011; 31: 197
CorticosteroidsCorticosteroids(Stern & Buttross,(Stern & Buttross, OphthalmologyOphthalmology 1991; 98:847)1991; 98:847)
‘allergic’ conjunctivitis‘allergic’ conjunctivitis
? traditional eye medicines? traditional eye medicines
Institute of Ophthalmology,Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology,Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Predisposing factorsPredisposing factors68.18
24.5
1.8
42.7
26.4
6.8
0
10
20
30
40
50
60
70
% OFPATIENTS
TRA TEM STER AB NO Rx TEM+AB
68.18
24.5
1.8
42.7
26.4
6.8
0
10
20
30
40
50
60
70
% OFPATIENTS
TRA TEM STER AB NO Rx TEM+ABTOTAL NO. OF CASES = 515.
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
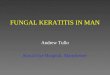
Risk factors for filamentous FUNGAL KERATITISRisk factors for filamentous FUNGAL KERATITIS
28 28
47
15
05
101520253035404550
Fungal Bacterial
Fungal 28 47Bacterial 28 15
Veg.Matter Mud
P<0.02P>0.05
28 28
47
15
05
101520253035404550
Fungal Bacterial
Fungal 28 47Bacterial 28 15
Veg.Matter Mud
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGALKERATITIS IN INDIA
Injury by needleInjury by needle
Courtesy J. KALIAMURTHY
foreign body in the corneaforeign body in the cornea
Welding sparkWelding sparkInstitute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA
Courtesy J. KALIAMURTHY
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

Hydrophilic contact lensesHydrophilic contact lensesLiesegang,Liesegang, CorneaCornea 1997; 16: 125, 2651997; 16: 125, 265
Contact lens cleaning solutionContact lens cleaning solution((ReNu with MoistureLoc -Bausch & Lomb, Rochester, NY)------ Singapore, Hong Kong, USA, West IndiesSingapore, Hong Kong, USA, West Indies
------ withdrawal controlled the outbreakwithdrawal controlled the outbreakKhor et al.,Khor et al., JAMAJAMA 2006; 295: 28672006; 295: 2867
Chang et al.,Chang et al., JAMAJAMA 2006; 296: 9532006; 296: 953
THE BURDEN OFFUNGAL KERATITIS
IN INDIAHydrophilic contact lensesHydrophilic contact lenses
Liesegang,Liesegang, CorneaCornea 1997; 16: 125, 2651997; 16: 125, 265
Contact lens cleaning solutionContact lens cleaning solution((ReNu with MoistureLoc -Bausch & Lomb, Rochester, NY)------ Singapore, Hong Kong, USA, West IndiesSingapore, Hong Kong, USA, West Indies
------ withdrawal controlled the outbreakwithdrawal controlled the outbreakKhor et al.,Khor et al., JAMAJAMA 2006; 295: 28672006; 295: 2867
Chang et al.,Chang et al., JAMAJAMA 2006; 296: 9532006; 296: 953
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
KeratitisKeratitis due to yeasts and yeast like fungidue to yeasts and yeast like fungi
CandidaCandida albicansalbicans
No geographic localization, exogenousNo geographic localization, exogenous
Ocular ( tears, eyelid closure)Ocular ( tears, eyelid closure) Systemic (diabetes mellitus,Systemic (diabetes mellitus, immunosuppressionimmunosuppression))
PrePre--existing corneal lesionsexisting corneal lesions
HerpesHerpes keratitiskeratitis, contact lens, contact lens--associatedassociated keratitiskeratitis
KeratitisKeratitis due to yeasts and yeast like fungidue to yeasts and yeast like fungi
CandidaCandida albicansalbicans
No geographic localization, exogenousNo geographic localization, exogenous
Ocular ( tears, eyelid closure)Ocular ( tears, eyelid closure) Systemic (diabetes mellitus,Systemic (diabetes mellitus, immunosuppressionimmunosuppression))
PrePre--existing corneal lesionsexisting corneal lesions
HerpesHerpes keratitiskeratitis, contact lens, contact lens--associatedassociated keratitiskeratitis
Institute of Ophthalmology, Joseph Eye Hospital, TiruchirappalliInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIAAgarwal et al.Agarwal et al. CorneaCornea. 2015; 34: 355. 2015; 34: 355--7.7.
Tried to detect fungal hyphae in corneal scraping material by aTried to detect fungal hyphae in corneal scraping material by acostcost--effective assembly of smartphone & pocket magnifier.effective assembly of smartphone & pocket magnifier.
A tissue sample was obtained by conventional corneal scrapingA tissue sample was obtained by conventional corneal scrapingfrom a clinically suspicious case of fungal keratitis.from a clinically suspicious case of fungal keratitis.
Smear stained by Gram stain; a 10% potassium hydroxide mountSmear stained by Gram stain; a 10% potassium hydroxide mountalso prepared.also prepared.
Slides imaged ny a smartphone coupled with a compact pocketSlides imaged ny a smartphone coupled with a compact pocketmagnifier & integrated lightmagnifier & integrated light--emitting diode assembly at pointemitting diode assembly at point--ofof--care.care.
Photographs of multiple sections of slides were viewed usingPhotographs of multiple sections of slides were viewed usingsmartphone screen & pinchsmartphone screen & pinch--toto--zoom function. Same slideszoom function. Same slidessubsequently screened under a light microscope by experiencedsubsequently screened under a light microscope by experiencedmicrobiologist.microbiologist.
The scraping from the ulcer also culturedThe scraping from the ulcer also cultured SmartphoneSmartphone--based digital imaging revealed grambased digital imaging revealed gram--positivepositive
organisms with hyphae.Examination under a light microscopeorganisms with hyphae.Examination under a light microscopealso yielded similar findings.also yielded similar findings.
Fusarium cultured from the corneal scraping, confirming theFusarium cultured from the corneal scraping, confirming thediagnosis of fungal keratitis.diagnosis of fungal keratitis.
Agarwal et al.Agarwal et al. CorneaCornea. 2015; 34: 355. 2015; 34: 355--7.7.
Tried to detect fungal hyphae in corneal scraping material by aTried to detect fungal hyphae in corneal scraping material by acostcost--effective assembly of smartphone & pocket magnifier.effective assembly of smartphone & pocket magnifier.
A tissue sample was obtained by conventional corneal scrapingA tissue sample was obtained by conventional corneal scrapingfrom a clinically suspicious case of fungal keratitis.from a clinically suspicious case of fungal keratitis.
Smear stained by Gram stain; a 10% potassium hydroxide mountSmear stained by Gram stain; a 10% potassium hydroxide mountalso prepared.also prepared.
Slides imaged ny a smartphone coupled with a compact pocketSlides imaged ny a smartphone coupled with a compact pocketmagnifier & integrated lightmagnifier & integrated light--emitting diode assembly at pointemitting diode assembly at point--ofof--care.care.
Photographs of multiple sections of slides were viewed usingPhotographs of multiple sections of slides were viewed usingsmartphone screen & pinchsmartphone screen & pinch--toto--zoom function. Same slideszoom function. Same slidessubsequently screened under a light microscope by experiencedsubsequently screened under a light microscope by experiencedmicrobiologist.microbiologist.
The scraping from the ulcer also culturedThe scraping from the ulcer also cultured SmartphoneSmartphone--based digital imaging revealed grambased digital imaging revealed gram--positivepositive
organisms with hyphae.Examination under a light microscopeorganisms with hyphae.Examination under a light microscopealso yielded similar findings.also yielded similar findings.
Fusarium cultured from the corneal scraping, confirming theFusarium cultured from the corneal scraping, confirming thediagnosis of fungal keratitis.diagnosis of fungal keratitis.
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Corneal scrapesCorneal scrapesEdgesEdgesBaseBase
Corneal biopsyCorneal biopsyLamellarLamellarFormalFormal
Anterior chamberAnterior chamber
Laboratory Diagnosis of FUNGAL KERATITIS
Corneal scrapesCorneal scrapesEdgesEdgesBaseBase
Corneal biopsyCorneal biopsyLamellarLamellarFormalFormal
Anterior chamberAnterior chamber
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Wet MountsWet Mounts KOH, ink KOH, KOHKOH, ink KOH, KOH--DMSO+AODMSO+AO Gopinathan et al.,Gopinathan et al., CorneaCornea 2002;2002;
21: 55521: 555 LPCBLPCB Thomas et al.,Thomas et al., Diagn Microbiol Infect DisDiagn Microbiol Infect Dis 1991; 14:2191991; 14:219
Stained smearsStained smears GramGram Gopinathan et al.,Gopinathan et al., CorneaCornea 2002; 21: 5552002; 21: 555 GiemsaGiemsa
Special stainsSpecial stains GMS, PASGMS, PAS Gopinathan et al.,Gopinathan et al., CorneaCornea 2002; 21: 5552002; 21: 555 AO, CFWAO, CFW
LectinsLectins FC, ECFC, EC Robin et al.,Robin et al., Am J OphthalmolAm J Ophthalmol 1986; 102: 7971986; 102: 797
Garcia et al.,Garcia et al., Mol VisMol Vis 2002; 8: 102002; 8: 10
Laboratory Diagnosis: Direct Microscopy Wet MountsWet Mounts
KOH, ink KOH, KOHKOH, ink KOH, KOH--DMSO+AODMSO+AO Gopinathan et al.,Gopinathan et al., CorneaCornea 2002;2002;21: 55521: 555
LPCBLPCB Thomas et al.,Thomas et al., Diagn Microbiol Infect DisDiagn Microbiol Infect Dis 1991; 14:2191991; 14:219
Stained smearsStained smears GramGram Gopinathan et al.,Gopinathan et al., CorneaCornea 2002; 21: 5552002; 21: 555 GiemsaGiemsa
Special stainsSpecial stains GMS, PASGMS, PAS Gopinathan et al.,Gopinathan et al., CorneaCornea 2002; 21: 5552002; 21: 555 AO, CFWAO, CFW
LectinsLectins FC, ECFC, EC Robin et al.,Robin et al., Am J OphthalmolAm J Ophthalmol 1986; 102: 7971986; 102: 797
Garcia et al.,Garcia et al., Mol VisMol Vis 2002; 8: 102002; 8: 10
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA : LABORATORY DIAGNOSIS
Calcofluor white
Lactophenol cotton blue
Gram stain Methenamine silver stain
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA :CULTURE
Solid mediaSolid media
••Sheep blood agarSheep blood agar••Cystine tryptone agarCystine tryptone agar••Sabouraud agarSabouraud agar••Rose Bengal agarRose Bengal agar
Antibacterial added to mediaAntibacterial added to media
Liquid mediaLiquid media•Brain heart infusion broth•Thioglycollate
Incubation Temperature : 22°C, 30-35°C
Duration of Incubation
Controls
Solid mediaSolid media
••Sheep blood agarSheep blood agar••Cystine tryptone agarCystine tryptone agar••Sabouraud agarSabouraud agar••Rose Bengal agarRose Bengal agar
Antibacterial added to mediaAntibacterial added to media
Liquid mediaLiquid media•Brain heart infusion broth•Thioglycollate
Incubation Temperature : 22°C, 30-35°C
Duration of Incubation
Controls Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
DIAGNOSIS ESTABLISHED BY :DIAGNOSIS ESTABLISHED BY :
Fungal hyphae or yeast cells in directFungal hyphae or yeast cells in directmicroscopy of LPCB wet films, Grammicroscopy of LPCB wet films, Gram-- ororCFWCFW--stained smearsstained smears
Growth of fungi in `C’ streaks of at least 2Growth of fungi in `C’ streaks of at least 2solid culture media inoculated with cornealsolid culture media inoculated with cornealscrapes.scrapes.
DIAGNOSIS ESTABLISHED BY :DIAGNOSIS ESTABLISHED BY :
Fungal hyphae or yeast cells in directFungal hyphae or yeast cells in directmicroscopy of LPCB wet films, Grammicroscopy of LPCB wet films, Gram-- ororCFWCFW--stained smearsstained smears
Growth of fungi in `C’ streaks of at least 2Growth of fungi in `C’ streaks of at least 2solid culture media inoculated with cornealsolid culture media inoculated with cornealscrapes.scrapes.
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA
Fungal Keratitis: Direct microscopic examination
Advantages
•Rapid, relatively inexpensive, relatively easy
•Good sensitivity and specificity for some methods
Disadvantages
Can detect fungi but very difficult toidentify the genus and species involved
Fungal Keratitis: Direct microscopic examination
Advantages
•Rapid, relatively inexpensive, relatively easy
•Good sensitivity and specificity for some methods
Disadvantages
Can detect fungi but very difficult toidentify the genus and species involved
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIACulture
Advantages: a) More sensitive than direct microscopy
b) May sometimes exceed molecular techniques in sensitivity andspecificity
c) Organism can be identified & susceptibility testing can be done.
Disadvantage: a) Takes time
b) There may be no growth in culture due to
c) Some amount of expertise needed for proper identification
AlfonsoAlfonso Trans Am Ophthalmol Soc 2008;Trans Am Ophthalmol Soc 2008; 106: 227106: 227--239239••IdentifiedIdentified FusariumFusarium isolates from ocular infections by morphological methods and by PCRisolates from ocular infections by morphological methods and by PCRanalysis of ITS regions (ITS 1, 5.8 S & ITS2)analysis of ITS regions (ITS 1, 5.8 S & ITS2)
••At species level, morphologic classification correlated with genotypic classification inAt species level, morphologic classification correlated with genotypic classification in25%(general ocular microbiology laboratory) and 97 %(reference mycology laboratory)25%(general ocular microbiology laboratory) and 97 %(reference mycology laboratory)
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli
THE BURDEN OF FUNGAL KERATITIS IN INDIACulture
Advantages: a) More sensitive than direct microscopy
b) May sometimes exceed molecular techniques in sensitivity andspecificity
c) Organism can be identified & susceptibility testing can be done.
Disadvantage: a) Takes time
b) There may be no growth in culture due to
c) Some amount of expertise needed for proper identification
AlfonsoAlfonso Trans Am Ophthalmol Soc 2008;Trans Am Ophthalmol Soc 2008; 106: 227106: 227--239239••IdentifiedIdentified FusariumFusarium isolates from ocular infections by morphological methods and by PCRisolates from ocular infections by morphological methods and by PCRanalysis of ITS regions (ITS 1, 5.8 S & ITS2)analysis of ITS regions (ITS 1, 5.8 S & ITS2)
••At species level, morphologic classification correlated with genotypic classification inAt species level, morphologic classification correlated with genotypic classification in25%(general ocular microbiology laboratory) and 97 %(reference mycology laboratory)25%(general ocular microbiology laboratory) and 97 %(reference mycology laboratory)
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIAPolymerase chain reaction (PCR)Polymerase chain reaction (PCR)
DNA target systemsDNA target systems
Fungal rRNA complex• Coding regions 18S, 5.8S & 28S nuclear rRNA genes evolved slowly-- are relatively conserved among fungi-- provide molecular basis of establishing phylogenetic relationships
•Non-coding regions ITS1 and ITS2 evolved more rapidly– responsible for sequence variability among fungal genera & species
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS ININDIA
Identification of pathogensIdentification of pathogensSingle strand conformation polymorphism (SSCP) analysisSingle strand conformation polymorphism (SSCP) analysis
after PCRafter PCR
Amplified products of target sequence denatured into singleAmplified products of target sequence denatured into single--stranded DNAstranded DNAfragmentsfragments
SingleSingle--stranded fragments subjected to nonstranded fragments subjected to non--denaturing PAGEdenaturing PAGE
PCRPCR--SSCP can detect > 90% of singleSSCP can detect > 90% of single--base substitutions in a 200 bpbase substitutions in a 200 bpfragmentfragment
Used to diagnoseUsed to diagnose FUNGAL KERATITISFUNGAL KERATITIS identify the fungal species involvedidentify the fungal species involved
KumarKumar et al. Am J Ophthalmolet al. Am J Ophthalmol 2005; 140: 8512005; 140: 851--857.857.Kumar and ShuklaKumar and Shukla J Clin MicrobiolJ Clin Microbiol 2005; 43: 6622005; 43: 662--668668Kumar and ShuklaKumar and Shukla Diagn Microbiol Infect DisDiagn Microbiol Infect Dis 2006; 56: 452006; 56: 45--5151
Single strand conformation polymorphism (SSCP) analysisSingle strand conformation polymorphism (SSCP) analysisafter PCRafter PCR
Amplified products of target sequence denatured into singleAmplified products of target sequence denatured into single--stranded DNAstranded DNAfragmentsfragments
SingleSingle--stranded fragments subjected to nonstranded fragments subjected to non--denaturing PAGEdenaturing PAGE
PCRPCR--SSCP can detect > 90% of singleSSCP can detect > 90% of single--base substitutions in a 200 bpbase substitutions in a 200 bpfragmentfragment
Used to diagnoseUsed to diagnose FUNGAL KERATITISFUNGAL KERATITIS identify the fungal species involvedidentify the fungal species involved
KumarKumar et al. Am J Ophthalmolet al. Am J Ophthalmol 2005; 140: 8512005; 140: 851--857.857.Kumar and ShuklaKumar and Shukla J Clin MicrobiolJ Clin Microbiol 2005; 43: 6622005; 43: 662--668668Kumar and ShuklaKumar and Shukla Diagn Microbiol Infect DisDiagn Microbiol Infect Dis 2006; 56: 452006; 56: 45--5151
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITISIN INDIA
Identification of pathogensIdentification of pathogensNucleic acid sequence analysis after PCRNucleic acid sequence analysis after PCR
Provides most information since size, nucleotideProvides most information since size, nucleotidecomposition and order of nucleotides are consideredcomposition and order of nucleotides are consideredBest method for identification of pathogens sinceBest method for identification of pathogens since
suspicion of aetiological agent is not necessarysuspicion of aetiological agent is not necessary
Used to identify the fungus causing MYCOTICUsed to identify the fungus causing MYCOTICENDOPHTHALMITIS &ENDOPHTHALMITIS & THE BURDEN OF FUNGALTHE BURDEN OF FUNGALKERATITIS IN INDIAKERATITIS IN INDIA
---- FerrerFerrer et al. J Clin Microbiolet al. J Clin Microbiol 2001; 39: 28732001; 39: 2873--28792879---- FerrerFerrer et al. J Clin Microbiolet al. J Clin Microbiol 2003; 41: 33582003; 41: 3358--33603360 AlternariaAlternaria---- FerrerFerrer et al. J Clin Microbiolet al. J Clin Microbiol 2005; 43: 53722005; 43: 5372--53755375 Fusarium proliferatumFusarium proliferatum
Nucleic acid sequence analysis after PCRNucleic acid sequence analysis after PCR
Provides most information since size, nucleotideProvides most information since size, nucleotidecomposition and order of nucleotides are consideredcomposition and order of nucleotides are consideredBest method for identification of pathogens sinceBest method for identification of pathogens since
suspicion of aetiological agent is not necessarysuspicion of aetiological agent is not necessary
Used to identify the fungus causing MYCOTICUsed to identify the fungus causing MYCOTICENDOPHTHALMITIS &ENDOPHTHALMITIS & THE BURDEN OF FUNGALTHE BURDEN OF FUNGALKERATITIS IN INDIAKERATITIS IN INDIA
---- FerrerFerrer et al. J Clin Microbiolet al. J Clin Microbiol 2001; 39: 28732001; 39: 2873--28792879---- FerrerFerrer et al. J Clin Microbiolet al. J Clin Microbiol 2003; 41: 33582003; 41: 3358--33603360 AlternariaAlternaria---- FerrerFerrer et al. J Clin Microbiolet al. J Clin Microbiol 2005; 43: 53722005; 43: 5372--53755375 Fusarium proliferatumFusarium proliferatum
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIATHE POLYMERASE CHAIN REACTION
1. Suspected ocular fungal infection where fungal1. Suspected ocular fungal infection where fungalspecies identification is not immediatelyspecies identification is not immediatelyrequiredrequired
Broad range PCR using universal fungal primersBroad range PCR using universal fungal primersto confirm a fungal aetiologyto confirm a fungal aetiology
1. Suspected ocular fungal infection where fungal1. Suspected ocular fungal infection where fungalspecies identification is not immediatelyspecies identification is not immediatelyrequiredrequired
Broad range PCR using universal fungal primersBroad range PCR using universal fungal primersto confirm a fungal aetiologyto confirm a fungal aetiology
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIATHE POLYMERASE CHAIN REACTION
2. Suspected ocular fungal infection where fungal2. Suspected ocular fungal infection where fungalspecies identification is a crucial needspecies identification is a crucial need
a)a) Single step or nested PCR amplification ofSingle step or nested PCR amplification of18S rRNA or 28S rRNA genes18S rRNA or 28S rRNA genesITSsITSs-- 5.8S rRNA gene5.8S rRNA geneITS2ITS2
b)b) Identification of the amplified product :Identification of the amplified product :nested PCR, DNA sequencing or SSCPnested PCR, DNA sequencing or SSCP
2. Suspected ocular fungal infection where fungal2. Suspected ocular fungal infection where fungalspecies identification is a crucial needspecies identification is a crucial need
a)a) Single step or nested PCR amplification ofSingle step or nested PCR amplification of18S rRNA or 28S rRNA genes18S rRNA or 28S rRNA genesITSsITSs-- 5.8S rRNA gene5.8S rRNA geneITS2ITS2
b)b) Identification of the amplified product :Identification of the amplified product :nested PCR, DNA sequencing or SSCPnested PCR, DNA sequencing or SSCPInstitute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIATHE POLYMERASE CHAIN REACTION
3. Identification of fungal isolate and determination3. Identification of fungal isolate and determinationof genetic relatedness to other fungal isolatesof genetic relatedness to other fungal isolates
Multilocus sequence typing (MLST)Multilocus sequence typing (MLST) Used to determine relatedness between isolatesUsed to determine relatedness between isolates
causing disease in different patients, hospitals andcausing disease in different patients, hospitals andcountriescountries
Epidemiological association ofEpidemiological association of FusariumFusarium keratitis inkeratitis in2006 performed by this method2006 performed by this methodChangChang et al.et al. JAMA 2006; 296: 953JAMA 2006; 296: 953--963.963.
ArbitrarilyArbitrarily--primed PCR (APprimed PCR (AP--PCR)PCR) useful for determining whether two isolates of theuseful for determining whether two isolates of the
same species are epidemiologically related.same species are epidemiologically related.
3. Identification of fungal isolate and determination3. Identification of fungal isolate and determinationof genetic relatedness to other fungal isolatesof genetic relatedness to other fungal isolates
Multilocus sequence typing (MLST)Multilocus sequence typing (MLST) Used to determine relatedness between isolatesUsed to determine relatedness between isolates
causing disease in different patients, hospitals andcausing disease in different patients, hospitals andcountriescountries
Epidemiological association ofEpidemiological association of FusariumFusarium keratitis inkeratitis in2006 performed by this method2006 performed by this methodChangChang et al.et al. JAMA 2006; 296: 953JAMA 2006; 296: 953--963.963.
ArbitrarilyArbitrarily--primed PCR (APprimed PCR (AP--PCR)PCR) useful for determining whether two isolates of theuseful for determining whether two isolates of the
same species are epidemiologically related.same species are epidemiologically related.Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIATHE BURDEN OF FUNGAL KERATITIS IN INDIA MedicalMedical emergencyemergency
Frequently occurs as anFrequently occurs as an acute presentationacute presentation
Patients in a state of distress due toPatients in a state of distress due to pain & loss of visionpain & loss of vision Index of suspicionIndex of suspicion based on demographics and clinical presentation of greatbased on demographics and clinical presentation of great
importanceimportance
•• Fungi may causeFungi may cause 1.2 to > 60 % of infectious keratitis1.2 to > 60 % of infectious keratitis•• Two important types:Two important types:---- due todue to filamentous fungifilamentous fungi---- due todue to yeast and yeastyeast and yeast--like fungilike fungi
•• AspergillusAspergillus andand FusariumFusarium ;; Candida albicansCandida albicans
Laboratory diagnosisLaboratory diagnosis (conventional and new modalities) required for(conventional and new modalities) required forconfirmationconfirmation
MedicalMedical emergencyemergency
Frequently occurs as anFrequently occurs as an acute presentationacute presentation
Patients in a state of distress due toPatients in a state of distress due to pain & loss of visionpain & loss of vision Index of suspicionIndex of suspicion based on demographics and clinical presentation of greatbased on demographics and clinical presentation of great
importanceimportance
•• Fungi may causeFungi may cause 1.2 to > 60 % of infectious keratitis1.2 to > 60 % of infectious keratitis•• Two important types:Two important types:---- due todue to filamentous fungifilamentous fungi---- due todue to yeast and yeastyeast and yeast--like fungilike fungi
•• AspergillusAspergillus andand FusariumFusarium ;; Candida albicansCandida albicans
Laboratory diagnosisLaboratory diagnosis (conventional and new modalities) required for(conventional and new modalities) required forconfirmationconfirmation
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli

THE BURDEN OF FUNGAL KERATITIS IN INDIA
Prompt diagnosisPrompt diagnosis & identification of the fungal& identification of the fungalpathogen is of utmost importancepathogen is of utmost importance
Direct microscopyDirect microscopy is rapid and sensitive but speciesis rapid and sensitive but speciesidentification is difficultidentification is difficult
CultureCulture allows species identification andallows species identification andsusceptibility testing but is timesusceptibility testing but is time--consumingconsuming
The polymerase chain reactionThe polymerase chain reaction permits rapidpermits rapiddetection of fungal nucleic acid in corneal scrapedetection of fungal nucleic acid in corneal scrapematerialmaterial
The polymerase chain reactionThe polymerase chain reaction permits accuratepermits accuratespecies identificationspecies identification——helps treatmenthelps treatment
Prompt diagnosisPrompt diagnosis & identification of the fungal& identification of the fungalpathogen is of utmost importancepathogen is of utmost importance
Direct microscopyDirect microscopy is rapid and sensitive but speciesis rapid and sensitive but speciesidentification is difficultidentification is difficult
CultureCulture allows species identification andallows species identification andsusceptibility testing but is timesusceptibility testing but is time--consumingconsuming
The polymerase chain reactionThe polymerase chain reaction permits rapidpermits rapiddetection of fungal nucleic acid in corneal scrapedetection of fungal nucleic acid in corneal scrapematerialmaterial
The polymerase chain reactionThe polymerase chain reaction permits accuratepermits accuratespecies identificationspecies identification——helps treatmenthelps treatment
Institute of Ophthalmology, Joseph Eye Hospital, Tiruchirappalli