Embed Size (px)
Citation preview
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP
GOVERNING BODY TUESDAY 10TH FEBRUARY 2015 AT 1PM
BOARDROOM ARTHOUSE SQUARE (lunch to be provided at 12.30pm)
A G E N D A Part 1: Introductions and Apologies 1.1 Declarations of Interest All 1.2 Minutes and action points from the meeting Attached
held on 13th January 2015 All 1.3 Matters Arising All Part 2: Updates 2.1 Feedback from Committees: Report no: GB 09-15
Healthy Liverpool Programme Leads Board – Dr Nadim Fazlani 13th January 2015
Finance Procurement & Contracting Committee Tom Jackson - 27th January 2015
Primary Care Committee - 27th January 2015 Dr Rosie Kaur Committees in Common - 7th January 2015 Dr Nadim Fazlani
2.2 Feedback from CCG Network – 4th February 2015 Report no: GB 10-15 Katherine Sheerin 2.3 Feedback from Joint Commissioning Group – Report no: GB 11-15
12th January 2015 Katherine Sheerin 2.4 Chief Officer’s Update Verbal Katherine Sheerin 2.5 NHS England Update Verbal Clare Duggan 2.6 Update from Health & Wellbeing Board Verbal Dr Nadim Fazlani
Page 1 of 2 111

2.7 Public Health Update Verbal Dr Sandra Davies Part 3: Strategy & Commissioning
3.1 Mental Health Transformation Programme – Report no: GB 12-15
Strategic Outline Case Dr Nadim Fazlani Part 4: Governance
4.1 Conflict of Interest Policy 2015 Report no: GB 13-15 Prof Maureen Williams 4.2 Variations to NHS Liverpool CCG Constitution Report no: GB 14-15 Katherine Sheerin 4.3 Personal Health Budgets Policy Report no: GB 15-15 Tom Jackson
Part 5: Performance 5.1 CCG Performance Report Report no: GB 16-15 Jane Lunt/Dr Rosie Kaur 6. Questions from the Public
7. Date and time of next meeting: Tuesday 10th March 2015 at 1pm - Boardroom, Arthouse Square For Noting:
Committees in Common – 5th November 2014 Primary Care Committee – 25th November 2014 Healthy Liverpool Programme Leads Board – 9th December 2014 Finance Procurement & Contracting Committee – 16th December 2014
Exclusion of Press and Public: that in view of the confidential nature of the business to be transacted, members of the public, press and non voting members be excluded from the
meeting at this point.
Page 2 of 2 222
Report no: GB 09-15 NHS LIVERPOOL CLINICAL COMMISSIONING GROUP
GOVERNING BODY TUESDAY 10TH FEBRUARY 2015
Title of Report Feedback from Committees
Lead Governor Dr Jude Mahadanaarachchi Dr Nadim Fazlani Dr Simon Bowers
Senior Management Team Lead
Cheryl Mould, Head of Primary Care Quality & Improvement Tom Jackson, Chief Finance Officer
Report Author(s)
Cheryl Mould, Head of Primary Care Quality & Improvement Tom Jackson, Chief Finance Officer
Summary The purpose of this paper is to present the key issues discussed, risks identified and mitigating actions agreed at the following committees: Healthy Liverpool Programme Leads Board – 13th
January 2015 Finance Procurement & Contracting Committee -
27th January 2015 Primary Care Committee - 27th January 2015 Committees in Common- 7th January 2015 This will ensure that the Governing Body is fully engaged with the work of committees, and reflects sound governance and decision making arrangements for the CCG.
Recommendation That Liverpool CCG Governing Body: Considers the report and recommendations from the
committees Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
As per each Committee’s Terms of Reference
Relevant Standards or targets
Standards of Good Governance NHS Operating Framework 2013/14
Page 1 of 11
333
Healthy Liverpool Programme Leads Board
Tuesday 13th January 2015
(Immediately after the Governing Body meeting Approx 3:30pm – 5:30pm)
Boardroom – Arthouse Square
AGENDA
1. Welcome and Introductions All
2. Minutes / Actions from the 9th December 2014 Meeting All
3.
HLP Investment Approvals (Papers attached) a) MASH/Early Help b) CAMHS c) Neuro
S Bowers/J Lunt
4. Programme Diagnostic Final Feedback (Papers attached) T Jackson
5. Phase 3 Update (presentation) T Jackson
6. Any Other Business All
7. Date of Next Meeting - Tuesday 10th February 2015 (approx. 3:30pm–5:30pm immediately after the Governing Body) 4th Floor Boardroom, Arthouse Square
Page 2 of 11
444
LIVERPOOL CCG CORPORATE GOVERNANCE TEMPLATE – COMMITTEE MINUTES Committee: Programme Leads Meeting Date: 13.01.15 Chair: Nadim Fazlani
Key issues:
Risks Identified: Mitigating Actions:
1. Investment proposals for Children’s Programme
• MASH • CAMHS • Neuro
• All three proposals approved in principle but need to be further developed.
• Proposals to be reconsidered and further detail added prior to submission to Finance, Procurement and Contracting committee
• Paper submitted outlining key tasks for Phase 3 of the programme including the conclusions from the PA diagnostic.
• Scope, Governance, Support and Timelines to be clearly defined during January.
• Governing body session planned for 28th January will cover these areas.
Recommendations to NHS Liverpool CCG Governing Body:
1. Note the approval in principle of the investment proposals
2. Note the key tasks for the next phase of the HLP Programme
Page 3 of 11
555
FINANCE, PROCUREMENT AND CONTRACTING COMMITTEE TUESDAY 27 JANUARY 2015 AT 10:00AM – 12:30PM
ROOM 2 – ARTHOUSE SQUARE AGENDA
1. Welcome and Introductions All
2. Declaration of Interests (form available) All
3. Minutes and action notes of previous meeting a. held on 16 December 2014 Chair
4. Conflict of Interest Policy Report no:FPCC01-15
Ian Davies/Cheryl Mould 5. Finance & Contracts Performance Month 8 Report no: FPCC02-15
Alison Ormrod
6. Recurrent Budgets Report no: FPCC03-15 Alison Ormrod
7. Financial Planning Timetable Report no: FPCC04-15 Alison Ormrod
8. Finance KPI Report Report no: FPCC05-15
Alison Ormrod
9. Contract Update Month 8 Report no: FPCC06-15 Derek Rothwell
10. Schedule Contract Meetings Report no: FPCC07-15
Derek Rothwell
11. Procurement Waivers 2014 Report no: FPCC08-15 Derek Rothwell
12. Personal Health Budgets Information Report no: FPCC09-15 Alison Ormrod
13. Any Other Business All
Page 4 of 11
666

Date of next meeting(s): REVISED DATE Tuesday 24 February 2015 9am – 11:30pm
Room 2– Arthouse Square
Tuesday 24 March 2015 10am – 12:30pm Room 2 - Arthouse Square
2015 monthly meetings: 4th Tuesday of the month 10am – 12:30pm
Room 2 – Arthouse Square
Page 5 of 11
777
LIVERPOOL CCG CORPORATE GOVERNANCE TEMPLATE – COMMITTEE MINUTES Committee: Finance, Procurement & Contracting Committee
Meeting Date: 27 January 2015 Chair: Dr Nadim Fazlani
Key issues:
Risks Identified: Mitigating Actions:
1. Conflicts of Interest Policy The CCG needs adequate arrangements to protect itself from conflicts of interest
Review of the policy. Finance Procurement and Contracting Committee(FPCC) has suggested amendments and proposed a Q&Q session with Governing Body Members.
2. Recurrent Budget Sound financial management The FPCC reviewed the recurrent budgets that were agreed for a 2 year period in April 2014.
3. Personal Health Budgets Policy The CCG required a policy to discharge this duty.
Reviewed and endorsed at FPCC and advised to take to the Governing Body for ratification/approval
Recommendations to NHS Liverpool CCG Governing Body: 1. Note the above 2. Note the above 3. Approve the Personal Health Budgets Policy.
Page 6 of 11
888
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP PRIMARY CARE COMMITTEE
TUESDAY 27TH JANUARY 2015 AT 1PM – 3PM BOARDROOM – ARTHOUSE SQUARE
A G E N D A
Part 1: Introductions and Apologies 1.1 Declarations of Interest All 1.2 Minutes and action points from the last meeting Attached
held on 25th November 2014 All 1.3 Matters Arising: All 1.3.1 Primary Care Winter Pressures/ Verbal
Healthy Ageing Update Michelle Urwin/ Colette Morris
1.3.2 Medicines Management Validation Peter Johnstone
Part 2: Updates 2.1 Feedback from Workstreams December 2014/ Report no: PCC 01-15 January 2015
a) Localities PCC 01a-15
North, Central & Matchworks
b) Medicines Management Sub-Committee PCC 01b-15 Shamim Rose
c) Patient Engagement & Experience PCC 01c-15 Dave Antrobus
Page 7 of 11
999
2.2 Update from NHS England Verbal – Tom Knight/ Rose Gorman
Part 3: Service Development/Implementation 3.1 Liverpool Quality Improvement Scheme PCC 02-15
(GP Specification) Rosie Kaur Part 4: Quality & Performance
4.1 Validation Process – PCC 03-15 end of year GP Specification 14/15 Cheryl Mould
4.2 Primary Care Quality Performance PCC 04-15 Rosie Kaur 4.3 IM&T Update PCC 05-15 Simon Bowers/ Kate Warriner
5. Any Other Business ALL 6. Date and time of next meeting:
24th February 2015 1pm to 3pm, Boardroom, Arthouse Square
Page 8 of 11
101010
LIVERPOOL CCG CORPORATE GOVERNANCE TEMPLATE – COMMITTEE MINUTES Committee: Primary Care Committee
Meeting Date: 27th January 2015 Chair: Dr Nadim Fazlani Vice Chair: Dr Rosie Kaur
Key issues:
Risks Identified: Mitigating Actions:
1. Uptake of Over 75’s initiatives for 2014/15 was approved.
• Current underspend against plan. • Unable to complete full evaluation and
realized impact of initiative.
• Issue with estates and smaller practices
not having room for additional clinic
• Programme Manager to work with Primary Care Team to support practices.
• Communication to be sent out to offer
support to increase uptake where possible.
• Utilising EMIS Web to enable clinics to
be held in Neighbourhood Centres.
2. Local Quality Improvement Scheme (GP Specification 2015/16)
• New Key Performance Indicators required.
• Practice sign up to deliver quality
scheme.
• Member practice engagement event arranged to discuss new indicators.
• Local Quality Improvement Scheme
presented to Local Medical Committee.
• Specification sent to all practices for comments.
3. Primary Care quality Performance.
• Reporting on QOF indicators mid year presents little value.
• Areas for improvement highlighted
being address at Locality Level.
• Compare quarter 4 data and decide on future reporting.
• Supporting documentation to be
provided for Localities to help address the improvements required.
Recommendations to NHS Liverpool CCG Governing Body:
1. To note key actions. 2. To note validation process for 2014/15 was approved.
Page 9 of 11 111111
HEALTHY LIVERPOOL PROGRAMME RE-ALIGNING HOSPITAL BASED CARE
COMMITTEE(S) IN COMMON (CIC)
KNOWSLEY, LIVERPOOL AND SOUTH SEFTON CCGS
4pm, Wednesday 7th January 2015, Merton House, Bootle, Liverpool L20 3DL
1. Welcome and introductions
2. Minutes of meeting held 5.11.2015 (attached)
3. Terms of Reference (attached - KS)
4. Update from Hospital Based Services Work Stream (FL / DO’D / ID)
5. Update from NHSE Specialist Commissioners (AT)
6. Feedback from PA Consulting Diagnostic (attached – KS)
7. Draft Hospital Options Development Process (attached – ID)
8. Key Milestones and Next Steps
9. Any other business
10. Date and time of next meeting 4th February 2015 – 4:00pm – 5:30pm – Conference Room, Merton House, Bootle, L20 3DL
Page 10 of 11
121212
LIVERPOOL CCG CORPORATE GOVERNANCE TEMPLATE – COMMITTEE MINUTES Committee: Committees in Common
Meeting Date: 7th January 2015 Chair: Katherine Sheerin
Key issues:
Risks Identified: Mitigating Actions:
1. Decision making regarding options for future models for hospital services.
• Trust decision making is not robust in terms of the statutory requirements of each commissioning organisation .
• Clear process debated and agreed with amendments, reflecting statutory responsibilities of each CCG and NHS England.
Recommendations to NHS Liverpool CCG Governing Body:
1. To note the actions from the Committees in Common..
Page 11 of 11
131313

141414
Report no: GB 10-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report Feedback from Merseyside Clinical Commissioning Groups Network
Lead Governor Dr Nadim Fazlani, Chair
Senior Management Team Lead
Katherine Sheerin, Chief Officer
Report Author
Katherine Sheerin, Chief Officer
Summary The purpose of this paper is to present the key issues discussed, risks identified and mitigating actions agreed at the Merseyside CCG Network on 4th
February 2015. This will ensure that the Governing Body is fully engaged with the work of the Merseyside CCG Network and reflects sound governance and decision making arrangements for the CCG.
That Liverpool CCG Governing Body: Considers the reports and recommendations
from Merseyside CCG Network
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
By working collaboratively with CCGs across Merseyside we will ensure that opportunities are maximised for Liverpool patients and the consequence of commissioning services understood and managed.
Relevant Standards or targets
Standards of Good Governance NHS Operating Framework 2012/13
Page 1 of 3 151515
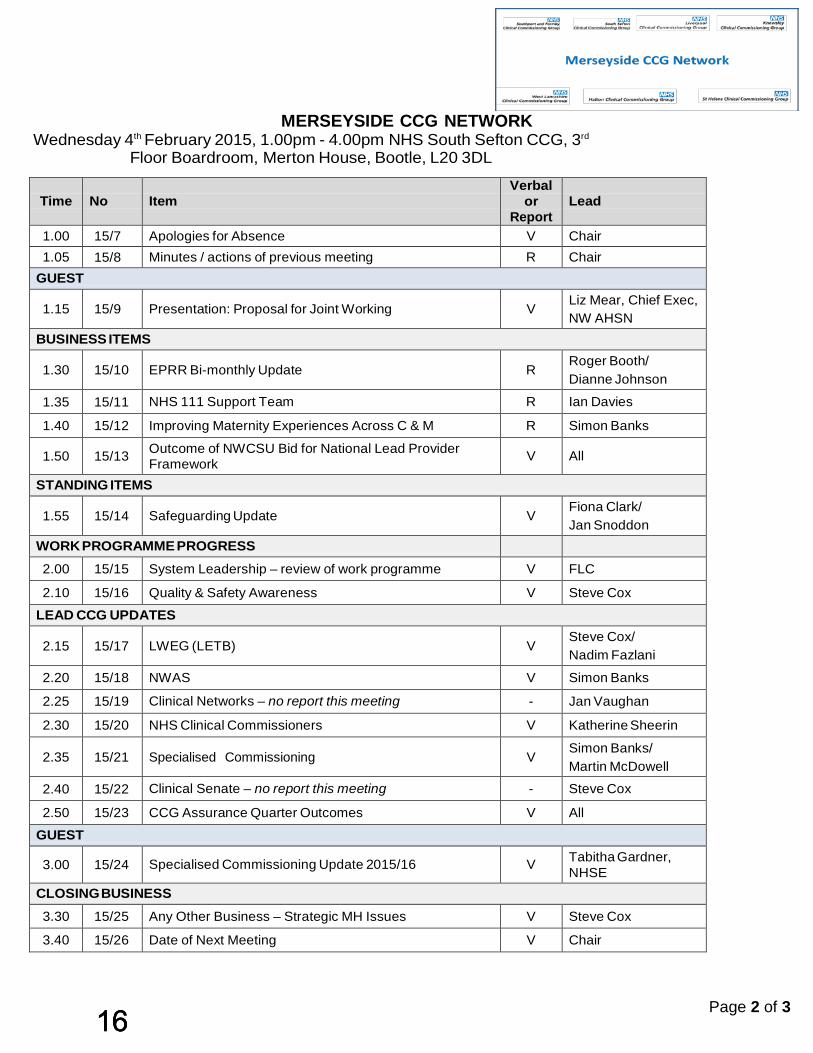
MERSEYSIDE CCG NETWORK
Wednesday 4th February 2015, 1.00pm - 4.00pm NHS South Sefton CCG, 3rd
Floor Boardroom, Merton House, Bootle, L20 3DL
Time No
Item
Verbal or
Report
Lead
1.00 15/7 Apologies for Absence V Chair 1.05 15/8 Minutes / actions of previous meeting R Chair
GUEST
1.15
15/9 Presentation: Proposal for Joint Working
V
Liz Mear, Chief Exec, NW AHSN
BUSINESS ITEMS
1.30
15/10 EPRR Bi-monthly Update
R
Roger Booth/ Dianne Johnson
1.35 15/11 NHS 111 Support Team R Ian Davies
1.40 15/12 Improving Maternity Experiences Across C & M R Simon Banks
1.50
15/13 Outcome of NWCSU Bid for National Lead Provider Framework
V
All
STANDING ITEMS
1.55
15/14 Safeguarding Update
V
Fiona Clark/ Jan Snoddon
WORK PROGRAMME PROGRESS 2.00 15/15 System Leadership – review of work programme V FLC
2.10 15/16 Quality & Safety Awareness V Steve Cox
LEAD CCG UPDATES
2.15
15/17 LWEG (LETB)
V
Steve Cox/ Nadim Fazlani
2.20 15/18 NWAS V Simon Banks
2.25 15/19 Clinical Networks – no report this meeting - Jan Vaughan
2.30 15/20 NHS Clinical Commissioners V Katherine Sheerin
2.35
15/21 Specialised Commissioning
V
Simon Banks/ Martin McDowell
2.40 15/22 Clinical Senate – no report this meeting - Steve Cox
2.50 15/23 CCG Assurance Quarter Outcomes V All
GUEST
3.00
15/24 Specialised Commissioning Update 2015/16
V Tabitha Gardner,
NHSE CLOSING BUSINESS
3.30 15/25 Any Other Business – Strategic MH Issues V Steve Cox
3.40 15/26 Date of Next Meeting V Chair
Page 2 of 3 161616
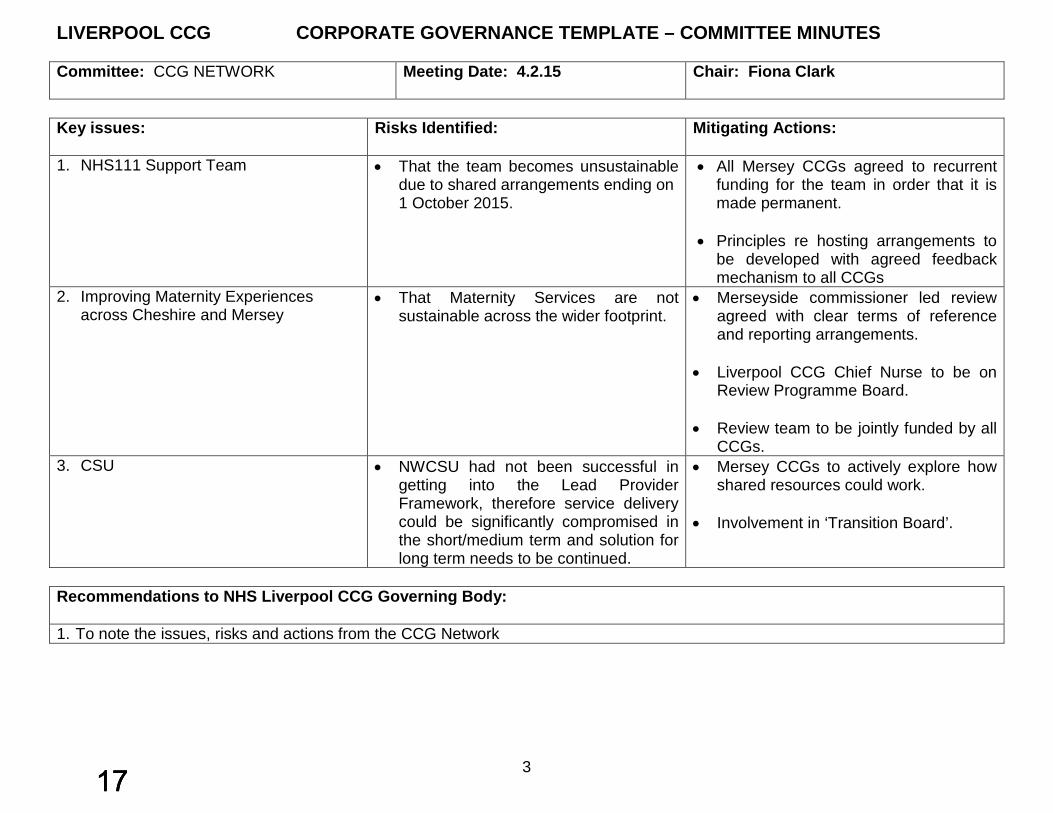
LIVERPOOL CCG CORPORATE GOVERNANCE TEMPLATE – COMMITTEE MINUTES Committee: CCG NETWORK
Meeting Date: 4.2.15 Chair: Fiona Clark
Key issues:
Risks Identified: Mitigating Actions:
1. NHS111 Support Team
• That the team becomes unsustainable due to shared arrangements ending on 1 October 2015.
• All Mersey CCGs agreed to recurrent funding for the team in order that it is made permanent.
• Principles re hosting arrangements to
be developed with agreed feedback mechanism to all CCGs
2. Improving Maternity Experiences across Cheshire and Mersey
• That Maternity Services are not sustainable across the wider footprint.
• Merseyside commissioner led review agreed with clear terms of reference and reporting arrangements.
• Liverpool CCG Chief Nurse to be on
Review Programme Board.
• Review team to be jointly funded by all CCGs.
3. CSU • NWCSU had not been successful in getting into the Lead Provider Framework, therefore service delivery could be significantly compromised in the short/medium term and solution for long term needs to be continued.
• Mersey CCGs to actively explore how shared resources could work.
• Involvement in ‘Transition Board’.
Recommendations to NHS Liverpool CCG Governing Body: 1. To note the issues, risks and actions from the CCG Network
3 171717

181818
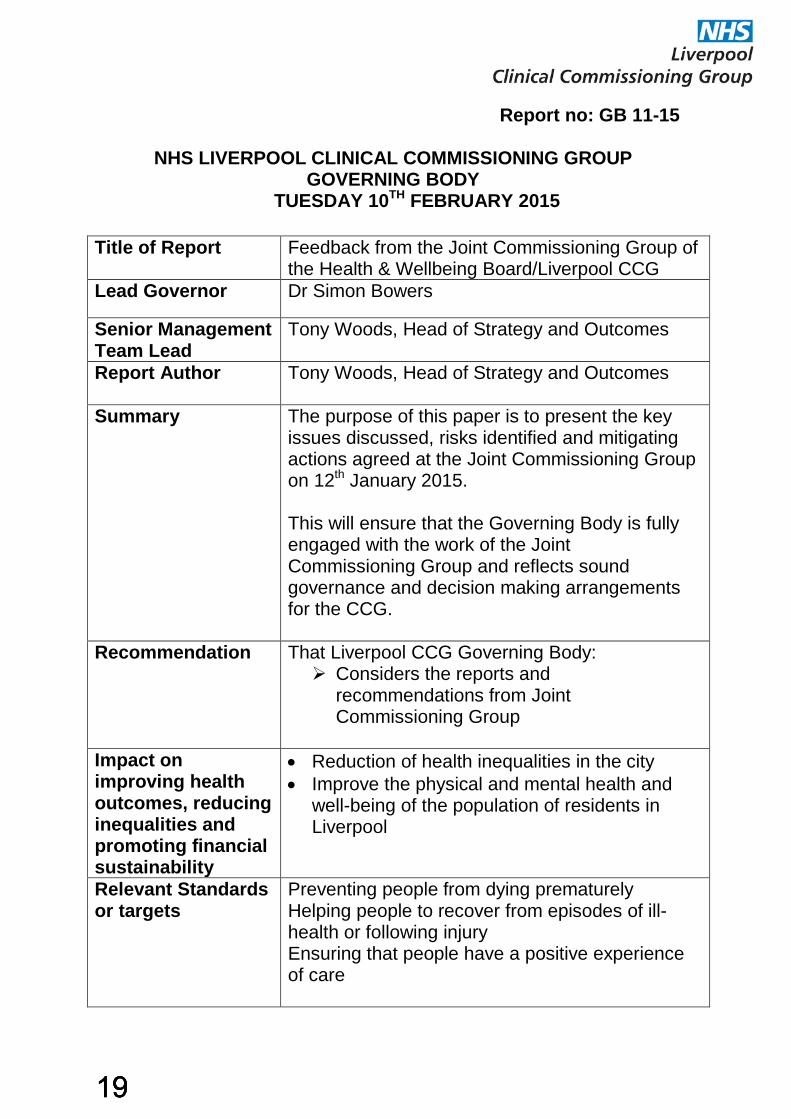
Report no: GB 11-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report Feedback from the Joint Commissioning Group of the Health & Wellbeing Board/Liverpool CCG
Lead Governor Dr Simon Bowers
Senior Management Team Lead
Tony Woods, Head of Strategy and Outcomes
Report Author
Tony Woods, Head of Strategy and Outcomes
Summary The purpose of this paper is to present the key issues discussed, risks identified and mitigating actions agreed at the Joint Commissioning Group on 12th January 2015. This will ensure that the Governing Body is fully engaged with the work of the Joint Commissioning Group and reflects sound governance and decision making arrangements for the CCG.
Recommendation That Liverpool CCG Governing Body: Considers the reports and
recommendations from Joint Commissioning Group
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
• Reduction of health inequalities in the city • Improve the physical and mental health and
well-being of the population of residents in Liverpool
Relevant Standards or targets
Preventing people from dying prematurely Helping people to recover from episodes of ill-health or following injury Ensuring that people have a positive experience of care
191919
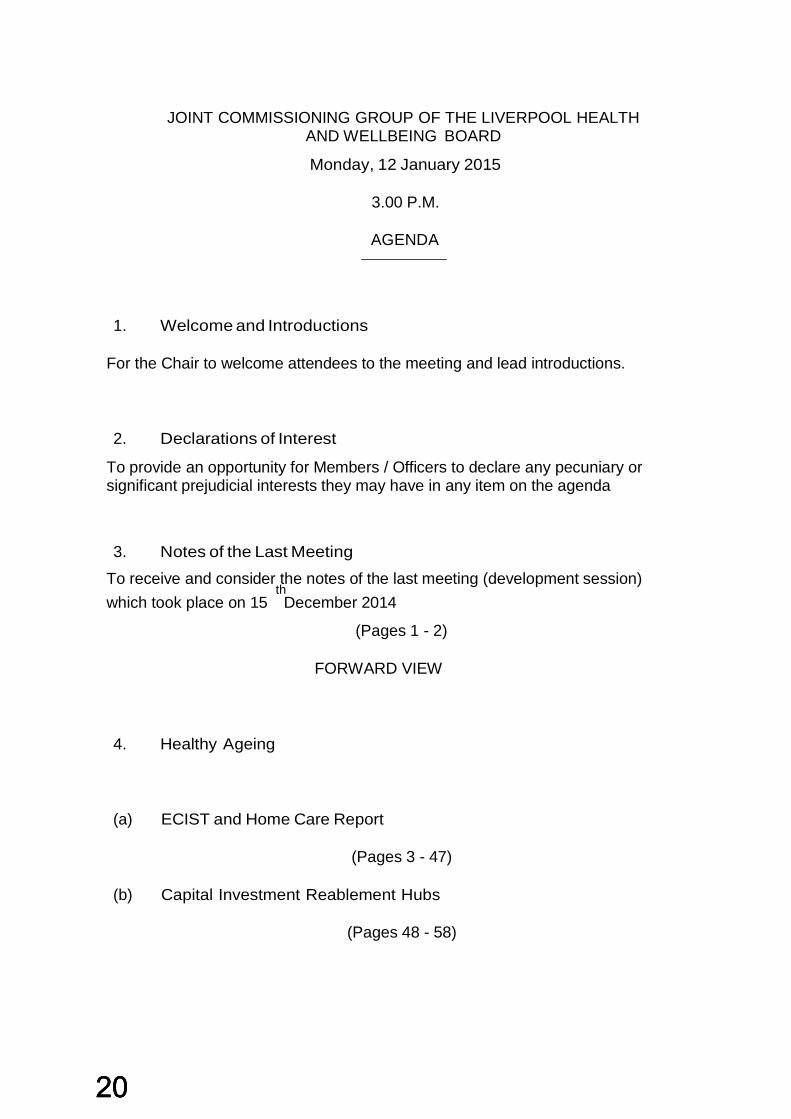
JOINT COMMISSIONING GROUP OF THE LIVERPOOL HEALTH AND WELLBEING BOARD
Monday, 12 January 2015
3.00 P.M.
AGENDA
1. Welcome and Introductions
For the Chair to welcome attendees to the meeting and lead introductions. 2. Declarations of Interest
To provide an opportunity for Members / Officers to declare any pecuniary or significant prejudicial interests they may have in any item on the agenda 3. Notes of the Last Meeting
To receive and consider the notes of the last meeting (development session)
th which took place on 15 December 2014
(Pages 1 - 2)
FORWARD VIEW
4. Healthy Ageing
(a) ECIST and Home Care Report
(Pages 3 - 47)
(b) Capital Investment Reablement Hubs
(Pages 48 - 58)
202020
5. Mental Health 6. Learning Disability
(Pages 59 - 61)
7. Substance Misuse
8. Children and Young People
(a) Joint Commissioning Priorities for Children and Young People
(Pages 62 - 64)
9. Living Well
(a) Integrated Behavioural Insight and Change Health Improvement Strategy Rationale
(Pages 65 - 71) 10. Opportunities for Joint Working
11. Date and Time of the Next Meeting
Next meeting will take place on Monday 9th February 2015 at 3pm at Liverpool CCG Arthouse Square
Page 3 of 4
212121
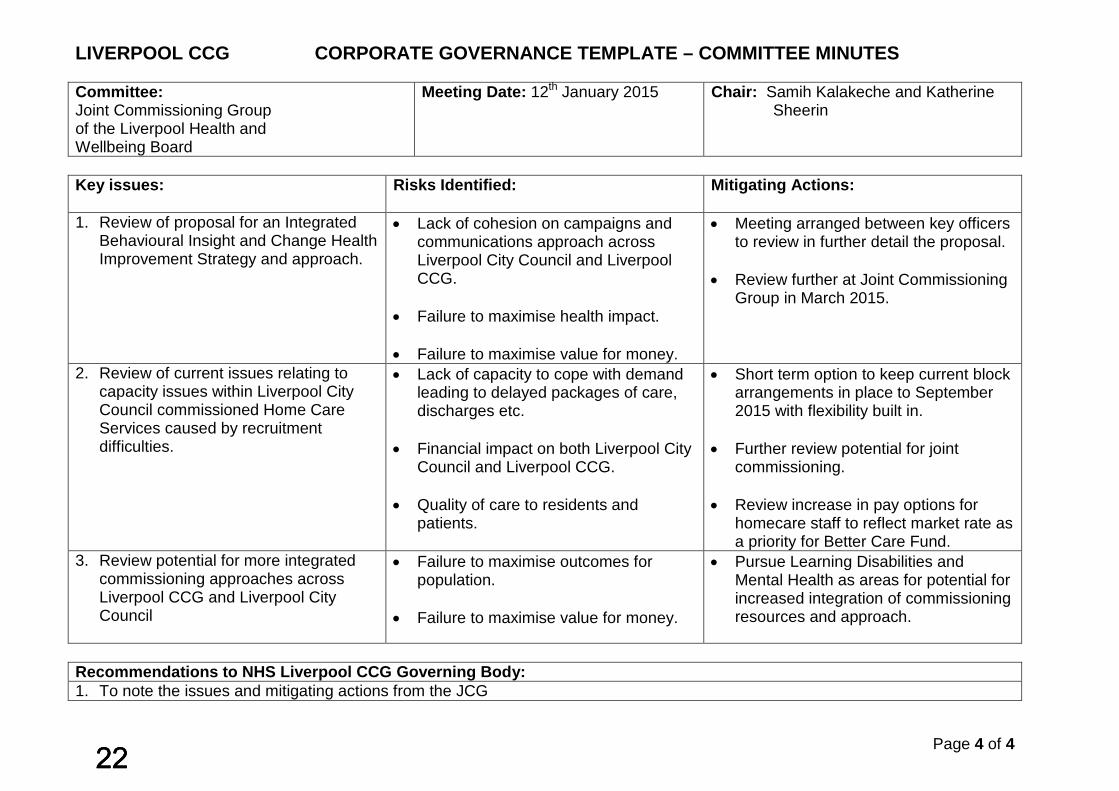
LIVERPOOL CCG CORPORATE GOVERNANCE TEMPLATE – COMMITTEE MINUTES Committee: Joint Commissioning Group of the Liverpool Health and Wellbeing Board
Meeting Date: 12th January 2015 Chair: Samih Kalakeche and Katherine Sheerin
Key issues:
Risks Identified: Mitigating Actions:
1. Review of proposal for an Integrated Behavioural Insight and Change Health Improvement Strategy and approach.
• Lack of cohesion on campaigns and communications approach across Liverpool City Council and Liverpool CCG.
• Failure to maximise health impact.
• Failure to maximise value for money.
• Meeting arranged between key officers to review in further detail the proposal.
• Review further at Joint Commissioning
Group in March 2015.
2. Review of current issues relating to capacity issues within Liverpool City Council commissioned Home Care Services caused by recruitment difficulties.
• Lack of capacity to cope with demand leading to delayed packages of care, discharges etc.
• Financial impact on both Liverpool City
Council and Liverpool CCG.
• Quality of care to residents and patients.
• Short term option to keep current block arrangements in place to September 2015 with flexibility built in.
• Further review potential for joint
commissioning.
• Review increase in pay options for homecare staff to reflect market rate as a priority for Better Care Fund.
3. Review potential for more integrated commissioning approaches across Liverpool CCG and Liverpool City Council
• Failure to maximise outcomes for population.
• Failure to maximise value for money.
• Pursue Learning Disabilities and Mental Health as areas for potential for increased integration of commissioning resources and approach.
Recommendations to NHS Liverpool CCG Governing Body: 1. To note the issues and mitigating actions from the JCG
Page 4 of 4
222222

Report no: GB 12-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report Mental Health Transformation Programme – Strategic
Outline Case
Lead Governor Dr Nadim Fazlani, Chair
Senior Management Team Lead
Tony Woods, Head of Strategy and Outcomes
Report Author
Kerry Harvey, Mental Health Transformation Programme Manager
Summary Members of the Mental Health Transformation Board with input from key stakeholders have identified six priority areas that require transformational change. These priorities form the basis of the draft Mental Health Strategic Outline Case and set the direction of the Mental Health Transformation Programme. The draft Mental Health Strategic Outline Case is attached here for review and comment (Appendix 1).
Recommendation That Liverpool CCG Governing Body: Note the content of the report Endorse the priorities identified
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
Reduction in the inequality in life expectancy between people with severe mental illnesses and the general population
Improved physical health outcomes for people diagnosed with a mental illness
Financial sustainability through quality improvement, increased focused on personal resilience and recovery and integrated service delivery
Relevant Standards or targets
IAPT access proportion IAPT recovery rate IAPT waiting times Early Intervention in Psychosis Liaison Psychiatry
Page 1 of 2 232323
New transforming care targets
MENTAL HEALTH TRANFORMATION PROGRAMME – STRATEGIC OUTLINE CASE
1. PURPOSE
To inform the Governing Body of the plans to transform mental health support and services for the people of Liverpool
2. RECOMMENDATIONS
That the Governing Body note the content of the draft Mental Health Strategic Outline Case and endorse the priorities identified
3. BACKGROUND
The Mental Health Transformation Board provides a strategic forum for the development and implementation of the Mental Health Transformation Programme. Over the preceding months members of the Board have engaged with key stakeholders to collectively identify and establish transformation priorities. The culmination of this is contained in the draft Mental Health Strategic Outline Case which signifies a joint commitment to review, redesign and deliver key elements of the mental health system. The draft Mental Health Strategic Outline Case was presented at the Health and Wellbeing Board on 15th January 2015 generating wide discussion and receiving positive feedback.
4. NEXT STEPS
Refinement of the draft Mental Health Strategic Outline Case Further exploration of the evidence base relating to proposals under
each transformation priority More clearly defined benefits Further analysis of affordability and financial impact
Tony Woods Head of Strategy and Outcomes 02 February 2015 ENDS
Page 2 of 2 242424
Version 1.0 09/01/2015
Mental Health: Strategic Outline Case
Introduction
Comparatively high levels of mental illness, compounded by the highest level of deprivation in England, represents a substantial challenge for the people of Liverpool and organisations charged with improving health outcomes and addressing inequality.
The Mental Health Transformation Programme signifies a joint commitment to review, redesign and deliver key elements of the mental health system bringing about positive change and transformational improvement. The Programme has strong clinical and managerial leadership from across the whole system; its members include service user representatives, GPs, Psychiatrists, an elected member of Liverpool City Council, mental health service providers and commissioners.
Over the preceding months members of the Board and stakeholders have come together at two innovative workshops collectively identifying and establishing priorities. The case for change and the results of the workshops are presented here in this Mental Health Strategic Outline Case.
The Vision for Mental Health Services and Support in Liverpool
Mental health services will operate as a seamless system of health and social care across the spectrum of severity, offering care which is holistic, timely and equitable, shifting the balance towards community based prevention and recovery.
Case for Change
Liverpool Joint Strategic Needs Assessment1
• Mental health needs in Liverpool are high. The Merseyside Lifestyle Survey (2012/13) reveals that around 1 and 5 people in Liverpool report low levels of wellbeing, with a similar proportion of residents reporting high levels of wellbeing. Adults in Liverpool with below average levels of wellbeing are twice as likely to say they were moderately anxious or depressed when compared to people with average mental wellbeing.
1 http://liverpool.gov.uk/media/688728/adultsolderpeoplementalhealth.pdf
Page 1 of 10
252525

Version 1.0 09/01/2015
• Common mental health problems (CMHP) are estimated to affect a
quarter of Liverpool’s population at any one time. Estimates produced by the Mental Health Observatory in 2008 suggest Liverpool has the second highest prevalence of mixed anxiety and depressive disorders among the eight core cities in England, only slightly behind Manchester. The prevalence of Severe Mental Illness (SMI) is the highest among the eight core cities in England, and is significantly above both regional and national levels.
• Data from the Community Mental Health Profiles 2013 show that
compared to the eight core cities in England, between 2009-10 and 2011-12, Liverpool had the highest rate of hospital admissions for mental health conditions. Rates of admission in the city were significantly above both regional and national levels over that period.
National Mental Health Profiles Data from the national Public Health Mental Health Profiles database demonstrates the high levels of mental health need within the city in comparison to similar populations elsewhere in the country. This includes:
• QOF reported prevalence for depression is 6.59%, the 5th highest amongst CCGs in the core cities
• % of people reporting a long term mental health problem through the GP patient survey is 6.65%, the 2nd highest CCG amongst the core cities
• Number of people in contact with mental health services is 4181 per 100,000, the fourth highest core city CCG
• Liverpool rates per 100,000 for AED attendances for a psychiatric disorder is 824.6 which is significantly higher than the England average and the third highest core city CCG
• The % of adults on a Care Programme Approach (CPA) in employment is 2.6% which is significantly lower than the national average and the second lowest core city CCG
Mental health and poverty
• The English Indices of Deprivation 2010 (ID 2010) show that Liverpool remains the most deprived local authority in the country.
Page 2 of 10
262626
Version 1.0 09/01/2015
Low income and poverty are significant public health issues, impacting on both physical and mental health2. People in low-income groups are most likely and people in higher income groups least likely to have CMHPs. The poorest 20% of the populations are twice as likely as those on average incomes to develop CMHPs. People are thought to live in relative poverty when their household income is less than 60% of contemporary median household income i.e. £17,2793.
• Data suggests that almost 40% of Liverpool households can be considered to be living at or close to the poverty line, with an income of less than £17,2794. Local evidence demonstrates a positive correlation between deprivation and mental health prevalence; as deprivation increases mental health prevalence also increases. Findings from a local pilot suggest that anti-poverty strategies targeted at vulnerable people need to be a key component of an effective and integrated primary mental health care system5.
Mental Health and Comorbidities
• Evidence suggests patients and practitioners tend to focus on physical symptoms during consultations. There are studies that show at least 30 per cent of all people with a long term condition also have a mental health problem and that the majority of cases of depression among people with physical illnesses go undetected and untreated. In addition people with two or more long-term conditions are seven times more likely to experience depression than those without a long-term condition6.
• Having a mental health problem increases the risk of physical ill health. Depression increases the risk of mortality by 50% and doubles the risk of coronary heart disease in adults. People with mental health problems such as schizophrenia or bipolar disorder die on average 16–25 years sooner than the general population7.
The high levels of mild mental health conditions suggests we need to ensure primary mental health care is of a consistently high quality; and
2 http://liverpool.gov.uk/media/688728/adultsolderpeoplementalhealth.pdf 3 http://liverpool.gov.uk/media/688728/adultsolderpeoplementalhealth.pdf 4 http://liverpool.gov.uk/media/688728/adultsolderpeoplementalhealth.pdf 5 Lloyd, K., Liverpool Healthcare Public Health Team Welfare Advice in General Practice, July 2013 6 http://www.kingsfund.org.uk/publications/long-term-conditions-and-mental-health 7 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213761/dh_124058.pdf
Page 3 of 10
272727
Version 1.0 09/01/2015
the high levels of psychosis prevalence demonstrate a need for adequate high-quality hospital capacity for when people are acutely unwell.
The New Model of Care for Mental Health
The new model will see resource and effort focused ‘upstream’, empowering people to maintain and restore their mental wellbeing. There will be much greater attention on early identification and the promotion of self-management, with emphasis on routes to recovery that allow for co-production and increased self-determination.
Most people, with mental health problems will be safely and effectively managed in a primary care setting by an integrated team of primary health professionals and mental health specialists. Non-clinical interventions will be more widely available with colleagues from the third sector working ‘hand in glove’ alongside clinical teams.
For those who need more intensive support and possibly inpatient care our aim is to provide services of the highest quality, with local services commissioned to meet local need, reducing the need for out of area treatments.
Overall, this approach is designed to address the wider determinants of health, avoid hospital admission (where appropriate) and support individuals to retain their independence.
Transformation Priorities
Two half-day workshops were held on the 16th October and 27th November 2014 involving key stakeholders from across the Liverpool mental health system. The first session focused on what excellence in mental health care would look like and identified a long list of areas to improve the current system.
At the second workshop these areas were reviewed further and refined to a clear set of six priority areas for the Transformation Programme to address;
1) Promotion of mental wellbeing and prevention of mental ill health
The World Health Organisation define mental health as “a state of well-being in which the individual realises his or her own abilities, can cope with the normal stresses of life and can work productively and fruitfully, and is able to make a contribution to his or her community”. We see a
Page 4 of 10
282828

Version 1.0 09/01/2015
future where all Liverpool residents, whether diagnosed with a mental illness or not, will value and understand how to protect and promote their own and others’ mental wellbeing.
The workstreams of the broader Healthy Liverpool Living Well strand will contribute substantially by encouraging physical activity, reducing alcohol misuse, reducing smoking levels and advocating for better self-care. In addition the Mental Health Transformation Programme will raise awareness of the risk factors to maintaining good mental health and signpost to supportive agencies and activities via the Wellbeing Liverpool service directory and the ‘LiveWell Liverpool’ online database.
Our priorities here are to:
• Ensure activities that promote wellbeing are accessible to all; providing targeted assistance to people diagnosed with a mental health illness and to those groups in society more susceptible to experiencing mental distress
• Ensure messages and information about maintaining and restoring mental wellbeing reach a broader audience including hospitals and schools
To achieve this we will:
• Engage locally with the Time to Change initiative to address the stigma that surrounds mental health
• Use local data to inform the best approach to influencing and encouraging positive health behaviours
• Remove barriers that prevent people with mental health issues accessing mainstream services
• Ensure a wide range of “recovery” opportunities are made available which are coproduced with people who have lived experience of mental distress
• Extend and embed preventative approaches in all settings of care • Enable organisations from the third sector that contribute to
wellbeing to come together with larger statutory providers, sharing what work wells and build capacity
• Empower carers with the skills and information they need to help the person they care for become engaged in ‘Living Well’ activities
Page 5 of 10
292929
Version 1.0 09/01/2015
2) Development of Integrated Community Services
The majority of support for mental health is received it the community, away from hospitals, mainly in primary care and often complemented by third sector organisations. Our aspiration is to build community services that reflect how people use and access support.
Primary care will become a hub of multi-disciplinary mental healthcare with professionals from secondary mental health care, social care and general practice co-located. Integration will enable increased peer support and ensure people receive personalised care, with even the most complex cases receiving care closer home.
The role of a vibrant third sector in providing holistic care cannot be underestimated; initiatives that facilitate and enable social inclusion and recovery through non-clinical intervention will be integrated into mainstream delivery.
Recognising the physical health needs of people with SMI and ensuring they receive appropriate screening and intervention is crucial, as is the integration of psychological support into long term condition care pathways. We have begun work to this end with dedicated liaison practitioners and a schedule of education events for GPs and their teams.
By promoting self-determination and recovery this new approach will establish holistic services based on the needs of people, rather than the location of professionals avoiding unnecessary medicalisation and dependence on specialist services.
Our priorities here are to
• integrate mental health into the wider community services transformation
• achieve parity of esteem between physical and mental health • provide a variety of non-medical initiatives and interventions that
aid social inclusion and recovery
To achieve this we will:
• Continue with to work as a whole system paying attention to the evidence base and thinking creatively about the design and delivery of community services
Page 6 of 10
303030

Version 1.0 09/01/2015
• Integrate mental health and social care professionals into primary care teams and community settings with colocation of third sector colleagues and services
• Run targeted initiatives focused on improving physical health outcomes for people with SMI
• Educate GPs and Practice Nurses on the benefits of considering psychological interventions for people with long term conditions
• Integrate psychological support into long term condition management
• Provide funding opportunities for third sector organisations that facilitate and enable social inclusion and recovery
3) High Quality Hospital Based Services
We will continue to strive to be a centre of excellence for acute mental health care through the innovative ‘Perfect Care’ programme within Mersey Care NHS Trust with investment in first class inpatient facilities and provision of evidence based care. The transformed service will deliver:
• Single access to all local services 24/7 that will significantly improve the management of referrals, offer help and support and consultation to service users, families and primary care colleagues
• Senior clinicians leading multidisciplinary assessment and
consultation
• Clear, evidence-based care pathways that adhere to key quality standards
• Fit for purpose acute inpatient an rehabilitation bed capacity that
compares favourably to acute inpatient facilities developed for acute physical healthcare. This will include the new Clock View facility due to open in March 2015, will be the Trust Centre of Excellence in relation to adult, acute and intensive care
• Anew assessment suite at Clock View, offering a safe and
comfortable alternative to A&E, a new and expanded PICU and Section 136 suite and new adult assessment and recovery wards that will further reduce length of stay
Page 7 of 10
313131
Version 1.0 09/01/2015
4) Liaison Psychiatry Input into Acute Hospitals Co-morbid mental health problems are known to be highly prevalent in hospital settings. Liaison psychiatry services are essential in identifying mental health problems and supporting people’s mental health needs while in hospital, including for people with long term conditions experiencing acute exacerbations. Liaison psychiatry will be a key part in our efforts to overcome the divide between mental and physical health care8,9.
Our priority here is to ensure there are adequate and effective levels of psychiatric services in acute settings. To achieve this we will work closely with the appropriate providers to establish a robust service delivery improvement plan. Areas already identified for improvement include;
o ensuring liaison teams are better integrated with the hospital teams they support
o identifying and addressing barriers that impede the effectiveness of liaison teams
o addressing communication and coordination that can be compromised by IT systems that are not inter-operable
5) Crisis Care
The core principles and outcomes outlined in the national Mental Health Crisis Care Concordat form the basis to our approach in caring for people presenting in crisis. A zero suicide approach will be taken across the Liverpool mental health and wellbeing system, focusing on people most at risk of suicide and ensuring that those at risk do not ‘fall through the cracks’ at the interfaces between primary and specialist care, between mental health and acute NHS care, and between the NHS and the criminal justice system. The principles we will adhere to are as follows:
• Access to support before crisis point • Urgent and emergency access to crisis care • The right quality of treatment and care when in crisis • Recovery and staying well, and prevention future crisis
8 http://www.kingsfund.org.uk/publications/long-term-conditions-and-mental-health 9 http://www.england.nhs.uk/wp-content/uploads/2014/12/forward-view-plning.pdf
Page 8 of 10
323232

Version 1.0 09/01/2015
Liverpool CCG is working with partners on a Merseyside footprint to provide a whole system crisis care response. A Merseyside self-assessment and action plan, guided by national policy, is being devised jointly and will be made available in the near future.
6) Youth Mental Health Transitions
A number of developments have taken place during the past three years to support young people facing the transition from child to adult mental health services. This has included the development of new teams and services in addition to better partnership working in order to develop smoother transition which best meets the needs of young people and their families. However, we are committed to doing more for our young people and improving how they experience transition into adult services10.
To ensure continuous improvement we will:
• Continue further development of the transition CQUIN (Commissioning for Quality and Innovation) between Alder Hey Children and Adolescent Mental Health Services (CAMHS) and Mersey Care
• Further strengthen and develop tier 3 and 4 pathways for children and young people in partnership with NHS England
• Work within the remit of the Healthy Liverpool Programme regarding transition ensuring a patient centred health approach.
Patient and Public Engagement
Between March and May 2013 Liverpool CCG engaged with local stakeholders on its plans to transform primary care mental health. Methods of engagement included six focus groups targeted at specific sections of the community (i.e. BME, older people), an online questionnaire to which 159 people responded and an Open Space event attended by a cross section of 70 stakeholders. To inform the Local Care Division Strategy 2014-18/19 Merseycare have engaged with over 400 clinicians, managers, other mental health organisations, service users and carers in developing their plans for the future. The results of these consultations have informed the transformational priorities.
10 http://www.liverpoolccg.nhs.uk/Library/Health_and_Services/Mental_Health/CYP%20Mental%20Health%20Strategy_Final.pdf
Page 9 of 10
333333

Version 1.0 09/01/2015
How we will manage this programme of change
The Liverpool Mental Health Transformation Programme Board continues to oversee and steer this major development. The Board has representation from across the whole system including service user representatives. Clinically led working groups, with project management support have been established to take forward delivery of the six priority areas detailed.
Next Steps
By March 2015 progress will have been made to define the six priority areas and commence implementation at pace. Additional investment requirements will be identified with business cases developed to access Healthy Liverpool Programme transformation funds.
Page 10 of 10
343434
Report no: GB 13-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report Conflicts of Interest Policy 2015
Lead Governor Dr Nadim Fazlani
Senior Management Team Lead
Ian Davies, Head of Operations & Corporate Performance
Report Author
Stephen Hendry, Senior Corporate Services Manager (Performance & Operations)
Summary The purpose of this paper is to provide an overview/summary to the Governing Body regarding the new CCG Conflicts of Interest Policy 2015.
Recommendation That Liverpool CCG Finance, Procurement & Contracting Committee: Notes the contents of the report and
accompanying policy document; Approve the Conflicts of Interest Policy as a
Corporate Policy
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
The Conflicts of Interest Policy (2015) is designed to ensure that health inequalities in access and outcomes of healthcare services in Liverpool are reduced through the continued application of a fair, transparent and open clinically led commissioning process. The policy aims to safeguard objective investment decisions of the CCG and provide a clear governance framework by which the confidence of the public, providers and regulators in the probity and integrity of commissioners’ decisions is maintained.
Page 1 of 4 353535
Relevant Standards or targets
Health & Social Care Act 2012; NHS England: Managing Conflicts of Interest: Statutory Guidance for CCGs (December 2014); NHS England: Code of Conduct: Managing conflicts of interest where GP practices are potential providers of CCG-commissioned services (July 2012); The National Health Service (Procurement, Patient Choice and Competition) Regulations 2013; Seven Principles of Public Life, as set out by the Committee on Standards in Public Life (The Nolan Principles)
NHS LIVERPOOL CCG CONFLICTS OF INTEREST POLICY 2015 1. PURPOSE The purpose of this paper is to inform the Governing Body of the new Liverpool CCG Conflicts of Interest Policy and to provide a summary of the key organisational responsibilities and requirements for the embedding of a transparent, robust policy and procedure for the management of conflicts of interest throughout the CCG. 2. RECOMMENDATIONS Governing Body is asked to note the contents of the report and approve the Liverpool CCG Conflicts of Interest Policy as a corporate policy. 3. BACKGROUND NHS Liverpool CCG’s Governing Body has overall responsibility for all actions carried out by its staff and committees. This responsibility incorporates the stewardship of significant public funds for the commissioning of healthcare services for the people of Liverpool. The CCG also has a statutory duty under the Health and Social Care Act (2012) to make arrangements for the management of conflicts of interest/potential conflicts of interest; ensuring that the integrity of the CCG’s decision making process (and membership) is not undermined by suggestions of impropriety or bias and that public trust in the CCG is maintained. These arrangements are summarised in the CCG’s Constitution (as amended 2015). As Liverpool CCG progresses towards delegated commissioning responsibility for primary medical care services, the organisation is exposed to an even
Page 2 of 4 363636
greater risk of conflicts of interest which, if not managed effectively and decisively could adversely affect public confidence in the local commissioning system and result in costly challenges to procurement decisions. In anticipation of this responsibility, Liverpool CCG’s Conflicts of Interest Policy 2015 clearly sets out how the organisation will assure the transparency of decision making in its committee structures; how conflicts of interest will be declared, managed, recorded and publicised and what steps will be taken where GPs (or other member practice representatives) included in a decision making group have a potential pecuniary or non-pecuniary interest in the outcome. 4. OVERVIEW OF THE POLICY The policy applies to all individuals involved in the CCG’s commissioning, contracting, procurement and decision making processes including (but not limited to);
• Members of the CCG acting in a formal capacity for the CCG as a member of a committee, decision making group or involved in any service design/procurement activity (including consultations);
• Governing Body Members (clinical, executive and lay members); • Committees and sub-committees of the CCG; • Committees and sub-committees of the Governing Body; • CCG employees; • Locality, neighbourhood and other relevant local commissioning
structures, and; • Contractors
It is the responsibility of all individuals to declare and update details of any personal business interests which may (or could be perceived to) influence their judgement when making commissioning or procurement decisions. The policy and associated procedures enables the CCG and clinical commissioners to demonstrate that they are acting fairly and transparently and in the best interests of the patients and local population of Liverpool. The policy document also sets out how the CCG will maintain and publicise a Register of Interests, which will record where and when interests are declared (including the nature and persons holding the interest), and describes the process by which declarations will be managed in the context of committee decision making and relevant monitoring arrangements for any contracts
Page 3 of 4 373737
awarded. The process for Dispute Resolution in relation to Conflicts of Interest is included in the policy as Appendix 6. Arrangements for the management of procurement decisions in relation to the commissioning of primary care medical service (in anticipation of the CCG’s delegated responsibility) are also covered in Section 12 of the policy. The CCG will ensure that all Governing Body members, committee/sub-committee members and CCG staff undertake mandatory training in relation to the policy once every two years (or sooner if there is a change in legislation or national guidance). This requirement will be stated in the CCG’s Organisational Development Plan. All employees and decision-makers will be made aware of the existence of this policy through established dissemination methods; this will include an introduction to the policy and related documents in induction packs for new staff. 5. SUMMARY The Conflicts of Interest Policy sets out the CCG’s commitment to acting fairly and transparently when making commissioning decisions in line with NHS England statutory guidance and in respect of the Seven Principles of Public Life (the Nolan Principles). The policy also defines the operational framework by which declarations of interest are managed at committee level, recorded in the Register of Interests and made available to the public. It establishes how policy statements will be enacted to protect both the CCG and individuals involved in decision making from any appearance of impropriety, undue bias or external influence.
Stephen Hendry Senior Corporate Services Manager
(Performance & Operations) 2nd February 2015
ENDS
Page 4 of 4 383838
NHS LIVERPOOL CCG
CONFLICTS OF INTEREST POLICY
VERSION 1.1 – February 2015
0
39
Version:
1.1
Ratified by:
Governing Body
Date ratified:
TBC
Name of originator/author:
Stephen Hendry, Senior Corporate Services Manager (Performance & Operations)
Name of lead:
Ian Davies, Head of Operations & Corporate Performance
Date issued/published:
February 2015
Review date:
February 2017
Target audience:
Organisational wide policy
Any changes to this policy should be outlined and recorded in the version control table below. In the event of any changes to relevant legislation or statutory procedures or duty this policy will be automatically updated to ensure compliance without approvals being necessary.
Version nos Type of change Date Description of change 1.0 Revision of policy
content 27/01/2015 Revisions made following recommendations
by Finance, Procurement & Contracts Committee
1
40

Contents
Page 1. Introduction 3 2. Scope 3 3. Associated Documentation 4 4. Principles of this Policy 4 5. Conflicts of Interest Covered by this Policy 5 6. Responsibilities 7 7. Management of Conflicts of Interest 9 8. Transparency in Procurement 13 9. Conflicts of Interest where GPs are Potential Providers 14
10. Decision Making for Commissioning Primary Medical Care 15 11. Register of Interests, Gifts and Hospitalities 16 12. Data Protection 17 13. Monitoring Compliance & Effectiveness of this Policy 17 14. Training 18 15 Review and Revision Arrangements 18 16. Equality & Diversity Statement 18
Appendices Appendix 1 - Declaration of Financial & Other Interests for Members/Employees 19-21 Appendix 2 - Declaration of Financial & Other Interests for Bidders/Contractors 22-24 Appendix 3 – Procurement Template for Commissioning Services from GP
Practices 25-26
Appendix 4 – Approvals Committee Terms of Reference 27-29 Appendix 5 – Primary Care Committee Terms of Reference 30-34 Appendix 6 – Dispute Resolution Process 35-37 Appendix 7– Guidance & Frequently Asked Questions 38-42
2
41
1. INTRODUCTION
Liverpool Clinical Commissioning Group (hereafter referred to as ‘the CCG) is committed to ensuring public funds are used appropriately and efficiently and recognises that it is placed in a significant position of trust in relation to responsibilities for the commissioning of healthcare services. In order to inspire and retain patient and public confidence in the CCG’s decision making the highest standards of probity, transparency and accountability will be applied when commissioning services for the population of Liverpool and when dealing with stakeholders, partners and suppliers.
Conflicts of interest may arise when an individual’s personal, or a connected person’s interests and/or loyalties conflict with those of the CCG. Identifying and managing conflicts of interest (real or perceived) is therefore essential in the promotion of transparency and maintaining public trust, demonstrating integrity and avoiding any potential or real situations of undue bias or influence in the CCG’s decision-making process.
For a GP or any other individual involved in commissioning, a conflict of interest may arise when their own judgment as an NHS commissioner could be, or be perceived to be, influenced and impaired by their own concerns and obligations as a healthcare or related provider; or as a member of a particular peer, professional or special interest group or as a friend or family member.
This policy is an expansion on Section 8 of the CCG’s Constitution and sets out Liverpool CCG’s arrangements for the management of conflicts of interest and potential conflicts of interest arising from the operation of the CCG’s commissioning activities and decisions. 2. SCOPE
The CCG’s Governing Body has a legal obligation to act in the best interests of Liverpool CCG and in accordance with its Constitution, and this policy applies to all CCG employees regardless of whether they are directly employed, in a seconded post or whether their remit is clinical or corporate. This includes:
• Members of the CCG acting in a formal capacity for the CCG as a member of a committee, decision making group or involved in any service design/procurement activity (including consultations);
• Governing Body Members (clinical, executive and lay members); • Committees and sub-committees of the CCG; • Committees and sub-committees of the Governing Body; • CCG employees; • Locality, neighbourhood and other relevant local commissioning structures,
and; • Contractors
3
42

Collectively, and for the purpose of this policy the above will generally be referred to as ‘CCG members and staff’ throughout the document. Where specific clarification is required, this will be appropriately referenced.
This policy does not replace or supersede the CCG’s Standing Orders or Prime Financial Policies contained within the CCG’s Constitution, which will always take primacy.
3. ASSOCIATED DOCUMENTATION
This policy should be read in conjunction with the following documents, which also set out generic guidelines and responsibilities for NHS organisations and General Practitioners in relation to conflicts of interests:
• Liverpool CCG’s Constitution and Standing Orders (SO), Scheme of Delegation (SD) and Standing Financial Instructions (SFI)
• Liverpool CCG Standards of Business Conduct Policy (January 2015)
• NHS England: Managing Conflicts of Interest: Statutory Guidance for CCGs (December 2014)
• NHS England: Code of Conduct: Managing conflicts of interest where GP practices are potential providers of CCG-commissioned services (July 2012)
• NHS England: Managing Conflicts of Interests: Guidance for Clinical
Commissioning Groups (2013)
• The Healthy NHS Board: Principles for Good Governance
• General Medical Council: Good Medical Practice 2006
• The National Health Service (Procurement, Patient Choice and Competition) Regulations 2013
4. PRINCIPLES OF THIS POLICY The main principle of this policy is to protect both the CCG and individuals involved in decision making from any appearance of impropriety and demonstrate transparency to the public and external interested parties. It is not intended to dilute or subvert the responsibility of the Governing Body to take strategic decisions on investment. The general processes and safeguards contained within will equally apply across the planning, decision making and monitoring stages of the commissioning process.
4
43
All employees of the CCG, Governing Body and Patient Representatives, including persons serving on CCG committees and other decision-making groups, are required to:
• Ensure that the interests of patients remain paramount at all times;
• Be impartial and honest in the conduct of their official business;
• Use public funds entrusted to them to the best advantage of the service, always ensuring value for money;
• Ensure that they do not abuse their official position for personal gain or to the
benefit of their family or friends;
• Ensure that they do not seek to advantage or further, private or other interests, in the course of their official duties, and;
• Use public funds entrusted to them to the best advantage of the service,
always ensuring value for money. The CCG is committed to conducting all of its business and functions in line with the Seven Principles of Public Life, as set out by the Committee on Standards in Public Life (The Nolan Principles) of:
• Selflessness; • Integrity; • Objectivity; • Accountability; • Openness; • Honesty, and; • Leadership;
In addition to these principles and values, the CCG embraces and includes the following standards of conduct expected in public service (as promoted by the Scottish Executive and Good Governance Institute):
• Public Service: Holders of public office have a duty to act in the interests of the public body of which they are a Board member and to act in accordance of the core tasks of the body, and;
• Respect: Holders of public office must respect fellow members of the public
body and employees of the body and the role they play, treating them with courtesy at all times
The CCG will ensure that all employees and decision-makers are aware of the existence of this policy, and will include an introduction to the policy and related documents in induction packs for new staff. A six-monthly reminder to review and update declarations of interest will be sent to all Governing Body members by the
5
44
Chief Finance Officer. This is does not replace the requirement for all CCG members and staff to notify the Chief Finance Officer of any changes within 28 days.
The CCG will view any instances where this policy is not followed as serious and may take disciplinary action against individuals, which may ultimately result in dismissal. In the case of members of the Governing Body or its Committees and Sub-Committees this could result in removal from office.
5. CONFLICTS OF INTEREST COVERED BY THIS POLICY
A conflict of interest could be defined as any situation where a CCG Governing Body member, committee member or member of staff’s personal interests or responsibilities may, or appear to influence the CCG’s decision making. The most common types of conflicts of interest include:
• A direct financial interest - where an individual may financially benefit from the consequence of a decision made;
• An indirect financial interest – where an individual is a member, partner or shareholder in an organisation which will benefit financially from a commissioning or other decision;
• Non-financial interest – where an individual holds a not-for-profit/non-remunerative interest in an organisation that will benefit from a commissioning or other decision (for example a Trustee of a charity that is bidding for a contract);
• Non-financial personal benefit. These occur where Governing Body members,
committee members or CCG staff receive no financial benefit, but are influenced by other external factors which could mean gaining status or wider recognition (for example, awarding contracts to friends or personal business contacts), and;
• Where an individual is closely related to, or in a close relationship/friendship with an individual in the above categories.
The NHS Model Standing Orders, Reservation and Delegation of Powers and Standing Financial Instructions, page 23 Department of Health (2006) defines relevant and material interests as:
• Directorships, including non-executive directorships held in private
companies or PLCs (with the exception of those of dormant companies);
• Ownership or part-ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the NHS;
6
45
• Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS;
• A position of authority in a charity or voluntary organisation in the field of health and social care;
• Any connection with a voluntary or other organisation contracting for NHS services;
• Research funding/grants that may be received by an individual or their
department;
• Interests in pooled funds that are under separate management, and;
• Clause 7.15 of the Model Standing Orders, Reservation and Delegation of Powers and Standing Financial Instructions states that such directorships should be included in the organisation’s Annual Report.
Statutory guidance states that interests “...must not exceed £5,000 in nominal value or one per cent of the total issued share capital of the company or of the relevant class of such capital, whichever is the less.” Conflicts can arise from an indirect financial interest such as payment to a spouse or a non-financial interest (for example kudos or reputation). Conflicts of loyalty may arise in respect of an organisation of which the individual is a member or has an affiliation (for example, a trustee of a charity). Conflicts can also arise from personal or professional relationships with others; for example where the role or interest of a family member, friend or acquaintance may influence an individual’s judgement or actions or could be perceived to do so. It is not possible to define or describe all instances in which an interest may be real or perceived as a conflict as they are greatly dependent on the circumstances and the context in which a conflict is applied. It is, however the responsibility of each individual involved in decision making to exercise their judgement in deciding whether to register any interests that may be construed as a conflict. When in doubt, individuals should seek guidance from the Chief Finance Officer but are advised to declare if there is any doubt as to whether a conflict exists or not. A guidance document (which includes a table of Frequently Asked Questions) attached as Appendix 7.
6. RESPONSIBILITIES The duties of Governing Body members are equivalent to those of a company director, in that there is a legal duty to avoid conflicts of interest under Section 175 of the Companies Act 2006 and which sets out how some conflicts should be managed.
It is the responsibility of all individual Governing Body members, committee members and all CCG staff serving in a formal capacity to declare and keep up-to-
7
46

date details of any personal or business interests which may influence (or be perceived to influence) their judgement and therefore place them in a position which creates a potential conflict of interest between their private interests and their CCG duties.
The CCG is to be made aware of all situations where a member of staff, Governing Body or committee member have an interest outside of their NHS Contract of Employment (or other involvement with the CCG) where that interest can, or has the potential to be perceived as a conflict of interest.
All staff, Governing Body and committee members (including patient representatives) and other decision makers must therefore declare all relevant and material interests in the following circumstances:
• On appointment (see 7.1);
• Annually;
• At every meeting before the agenda is discussed (new and existing);
• On changing role or responsibility (see 7.2);
• On any other change of circumstances and (see 7.2);
• On becoming aware that the CCG has entered into (or proposes entering into) a contract with a provider/company which they, or any person connected with them has a direct or indirect financial interest in.
The Chair (or nominated deputy) of every decision making group will ensure that declarations of interest, and subsequent decisions made concerning on-going participation are clearly recorded in the minutes and on an individual basis. Where the Chair/nominated deputy is concerned about the declaration of interest and/or decision made about an individual’s on-going participation in an agenda item, the declaration will be referred to the Audit, Risk and Scrutiny Committee for further consideration.
Where a decision relating to a conflict of interest is challenged or is perceived to be inappropriate, the Dispute Resolution Process detailed in Appendix 6 will be followed.
6.1 Deputy Chair of the Governing Body/Lay Member for Governance
The Deputy Chair/Lay Member for Governance will provide guidance and an external view of the working of the CCG with a strategic and impartial focus, and will take the Governing Body Chair’s role for discussion and decisions where the Chair has made a declaration of interest.
8
47

6.2 The Chief Finance Officer
The Chief Finance Officer will act as the designated responsible officer for the CCG’s Register of Interests and on-going compliance with this policy. The Chief Finance Officer will also ensure that for every interest declared (either in writing or orally) appropriate arrangements are put in place to manage the conflict of interest or potential conflict of interest. The Chief Finance Officer will confirm these arrangements, in writing to the relevant individual within 7 days of the declaration.
Where necessary, the Chief Finance Officer will seek advice on the management of the conflicts of interest (or potential conflicts of interest) from one or more of the following:
• The Chief Officer; • The CCG Chair; • The Deputy Chair of the Governing Body/Lay Member for Governance; • The Head of Operations & Corporate Performance
6.3 The CCG Approvals Committee
The Approvals Committee, which is accountable to the CCG’s Governing Body will provide neutrality in the evaluation and decision making processes and is responsible for ensuring that the CCG applies conflicts of interest principles and policies rigorously; providing the Governing Body with non conflicted advice and judgement where there is any doubt about how these should be applied to individual or group cases involving clinical services. The Committee will judge where risks of conflicts of interest exist or may arise and confirm the appropriateness (or otherwise) of their handling of the matter in terms of the best way to manage such risks appropriate to the matter under consideration (see Appendix 4).
The Committee will also manage other conflicts of interest which may arise and which are not specifically related to the commissioning of services.
The Approvals Committee will prepare an annual report for the Audit, Scrutiny and Risk Committee on all conflicts of interest referred to the Committee in the period 1st April to 31st March inclusive of the relevant financial year; describing how they have been managed and what lessons have been learned so as to inform future policy or governance arrangements. The review by the Audit, Risk & Scrutiny Committee will provide external assurance and oversight through internal and external audit presence on the Committee.
The Terms of Reference for the Approvals Committee can be found in Appendix 4.
7. MANAGEMENT OF CONFLICTS OF INTEREST
The CCG will proactively manage conflicts of interest by:
9
48
• Maintaining and reviewing a Declarations of Interest Register (held by the Chief Finance Officer);
• Managing membership of all formal committees and decision making bodies supporting the CCG;
• Working within the CCG Constitution, Standing Orders (SO) and Scheme of
Reservations and Delegations, and;
• Ensuring robust mechanisms are in place for committee members to declare interests and withdraw from decision making where appropriate.
All Governing Body members will be required to complete a Declaration of Interests pro-forma (see Appendix 1) upon appointment to their position/role. Where there are no interests to declare a ‘nil return’ will be recorded. Any subsequent interests acquired or changes to existing interests, role or circumstances will be declared to the Chief Finance Officer as and when they arise on the pro-forma, within 28 days of the change.
Governing Body members and CCG staff will also be asked to review and update the Declarations of Interest Register every six months, and will be required to respond, including ‘nil returns’ within 28 days of the request.
Prior to attending any meeting, individuals should consider whether they have a conflict of interest pertaining to the meeting’s agenda. All CCG committee meetings will include a standing agenda item at the beginning of each meeting for members to declare any interests relating specifically to business being considered. In cases where an interest previously undeclared is identified during the course of a meeting, the declaration will be noted in the minutes (which will detail all declarations made). The chair of the meeting will determine how such interests will be managed and inform the member of their decision. Declarations will be treated as relevant for both decision making and any on-going monitoring.
Any suspicion that a relevant personal interest may not have been declared should be reported to the Chief Finance Officer immediately.
7.1 Declarations on Appointment or Nomination
Individuals applying for appointment for any position in the CCG will be required, at the point of application to declare any relevant interests. This includes:
• Lay Member appointments to the Governing Body; • Other appointments of external individuals to the Governing Body, its
committees, sub-committees and/or other working or project groups; • Medical Practitioners standing for election to the Governing Body.
10
49
The purpose of such declarations will be to enable the Chief Finance Officer (seeking guidance where applicable from the Lay Member for Governance, the CCG Chair or relevant external sources) to assess on a case-by-case basis whether any of the declared interests are such that they could not be managed under this policy and would prevent the individual from making a full and proper contribution to the CCG; thus prohibiting the individual from appointment or election to the CCG.
In doing so, the Chief Finance Officer will consider the materiality of the declared interest and the extent to which the individual could benefit from any decision of the CCG (e.g. an individual who has a material interest in an organisation which undertakes, or is likely to undertake substantial business with the CCG as a provider of healthcare or as a commissioning support service).
7.2 Declarations on changing role/responsibility or other changes in circumstances
Where an individual changes role or responsibility (either within the CCG or its Governing Body) any changes to that individual’s interests should be declared immediately. Similarly, where an individual’s circumstances change to an extent that it affects the individual’s interests (for example where an individual takes on a new role outside of the CCG, sets up a new business or enters into a new relationship) a further declaration should be made to reflect the change in circumstances; preferably as soon as possible and no later than 28 days of the change occurring. This applies equally to where a conflict of interest ceases to exist or a new one emerges.
7.3. Governance of Committee and Decision Making Meetings
Where attendees/members have declared a material interest, they should either be excluded from relevant parts of meetings, or join in the discussion but not participate in the decision-making itself (i.e. withdraw from the vote and any subsequent monitoring arrangements). The Chair/nominated deputy of the meeting will decide if a member is to be excluded from the relevant part of the meeting. The conflict and the action taken will be recorded in the minutes of the meeting and the register of interests updated accordingly. It is the responsibility of the Chair of the meeting (or Deputy Chair) to monitor quorum to ensure it is maintained throughout the discussion and decision of the agenda item. Should the withdrawal of the individual member(s) result in the loss of quorum, the item should not be concluded at that meeting. Once a conflict of interest is declared, the Chief Finance Officer, under delegated authority from the Chief Officer will determine and notify, in writing, any individual arrangements for managing the conflict of interests or potential conflicts of interests within seven days of declaration. These arrangements should confirm the following:
• When an individual should withdraw from a specified activity, on a temporary
or permanent basis;
11
50
• Monitoring of the specified activity undertaken by the individual, either by a line manager, colleague or other designated individual.
7.4 Decisions Where a Governing Body Member Has Declared an Interest
In situations where the Governing Body has to make a decision in which a member has declared an interest, all decisions will be made by vote, with a simple majority required. A quorum must be maintained for the discussion and decision and interested parties will not be counted when deciding whether the meeting meets quorum. Interested members must not vote on matters affecting their own interests. The Vice Chair will assume the Chair’s role for any discussions and decisions where the Chair has a conflict of interest. All decisions under a conflict of interest will be reported and recorded at the meeting of the Governing Body in the minutes. The minutes will record:
• The nature and extent of the conflict; • An outline of the discussion, and; • The actions taken to manage the conflict (including arrangements for
monitoring of contracts awarded). 7.5 Use of ‘Waivers’ In some cases the Governing Body may execute the use of a ‘waiver’ to allow the conflicted person to participate in a meeting. For example, the Governing Body may grant a waiver if the member's expertise is considered essential to the discussions and/or where certain policies and criteria are met. If a ‘waiver’ is granted and the conflicted member is allowed to participate in the meeting, the minutes will reflect that the circumstances of granting the waiver are sufficiently exceptional to justify a departure from guidance. Where a Governing Body member does benefit from a decision, the matter will be reported in the CCG Annual Report and Accounts. All payments (or benefits in kind) to Governing Body members will be reported in the CCG’s accounts and annual report, with amounts for each member listed for the year in question. Independent external mediation will be sought where conflicts cannot be resolved through the usual procedures. 7.6 CCG Dispute Resolution Process The CCG will endeavour to ensure that all disputes in relation to conflicts of interest are resolved informally and effectively through negotiation, mediation and local resolution. Where disputes cannot be resolved informally, the CCG operates a Dispute Resolution Process based on the principles of effective arbitration and natural justice. This process aims to resolve disputes transparently, fairly and consistently. If concerns cannot be resolved through mediation a formal complaint should be submitted, in writing, to the Chair of the CCG who will then communicate the process, decision making criteria and relevant timescales to the complainant in advance of the commencement. The Dispute Resolution Process can be found in Appendix 6 of this policy document.
12
51
8. TRANSPARENCY IN PROCUREMENT The CCG will procure services in a manner that is open, transparent, non-discriminatory and fair to all potential providers and is compliant with the NHS (Procurement, Patient Choice and Competition) Regulations 2013 by ensuring:
• All relevant clinicians (not limited to members of the CCG), potential providers and members of the public are fully engaged in the decision-making process;
• Offers for tender or procurement are not shaped in such a way that it provides advantages or disadvantages for an organisation that might bid for a service;
• The prohibiting of the award of a contract where the integrity of the award has been, or appears to have been affected by a conflict of interests, and;
• Maintaining appropriate records of how conflicts of interest have been managed in individual cases.
It is essential that the CCG balances an inclusive approach to partnership working; gaining the best technical advice whilst being mindful of acting in a fair manner and complying with competition law. This is particularly complex in cases where the CCG wishes to involve potential providers in shaping strategies or specifications and commercially sensitive information could potentially be discussed. Where one potential provider has access to information during the course of giving technical advice to the CCG, this will be openly shared with all other potential providers/suppliers should a tender or procurement be issued at a later date.
Where an individual has a conflict of interest they will not be involved in the procuring, managing or monitoring a contract in which they have declared an interest. Individuals must declare an interest where they, or organisations in which they have an interest, may be proposing to bid for a planned service by competitive tender, any qualified provider, or single tender routes.
Exceptions to this provision are in circumstances where the contribution of a professional with specific subject matter/clinical expertise or research knowledge in a field is necessary in supporting the commissioning process (see 9.1). In these situations full disclosure will be made and monitoring arrangements will include robust provisions for an independent challenge of bills and invoices and termination of the contract if the relationship is determined as unsatisfactory.
All potential bidders, contractors and service providers, including sub-contractors, members of consortia, advisors or other associated parties will be required to identify any potential conflicts of interest that could arise if they were to take part in any procurement process and /or provide services under or otherwise enter into any contract with the CCG, using the template attached as Appendix 2.
The interests that must be declared are that the organisation or any person employed or engaged by or otherwise connected with it:
13
52

• Has provided or is providing services or other work for the CCG; • Is providing services or other work for any potential bidder in respect of this
project or procurement process; • Has any other connection with the CCG, whether personal or professional,
which the public could perceive may impair or otherwise influence the CCG’s or any of its members or employees judgements, decisions or actions.
In addition to the above, the CCG will comply with the Procurement Guide for Commissioners of NHS Funded Services (2010) by:
• Widely advertising that a service design/re-design is taking place and inviting comments from all potential providers (ensuring that a record is kept of all interactions);
• Continued engagement with a wide range of providers as the service design develops;
• Obtaining the advice of an independent clinical advisor in relation to the design of the service (where appropriate), and;
• Specifying desired outcomes (clinical or otherwise) as opposed to specific inputs or activity.
9. CONFLICTS OF INTEREST WHERE GP PRACTICES ARE POTENTIAL PROVIDERS OF SERVICES
There may be circumstances where the CCG could reasonably commission services from member GP practices on a single tender basis (i.e. where they are the only capable providers or where the service is of minimal value). The general safeguards that the CCG will adopt when commissioning services for which GP practices could be potential providers of services, or where it is appropriate to commission community-based services through competitive tender or an Any Qualified Provider (AQP) approach are the same as those described in Sections 8 and 9 above. Essentially, the CCG has a responsibility to evidence that the service(s) clearly meet local need, have been planned properly and that the appropriate procurement approach has been used. AQP contracts will require GP Practices involved in the delivery of contracts to apply the latest GMC and BMA guidance regarding conflicts of interest to ensure that GP practices have offered fully informed choice at the point of referral. Any decisions to commission services from GP practices on a single tender basis will be taken in accordance with the CCG’s Procurement Strategy, after verifying that such services should not be provided under the GP contract. Where a limited number of GPs have an interest, it should be straightforward for relevant individuals to be excluded from decision-making. It is feasible that a situation could arise where a majority of members of the Governing Body who are GPs (or other healthcare professionals from a Member Practice) might share a material conflict of interest in a specific agenda item, which would prevent their participation in the decision making process. Where all of the
14
53
GPs (or other practice representatives) on a decision making body could have a material interest in a decision, particularly where the CCG is proposing to commission services on a single tender basis from all GP practices in the area, or where it is likely that all or most practices would wish to be qualified providers for a service under AQP, and as a result a quorum cannot be convened, the Chair of the meeting will consult with the Chief Officer on the action to be taken. This may include:
a) requiring another of the CCG’s committees or sub-committees, the CCG Governing Body or the Governing Body’s committees or sub-committees (as appropriate) which can be quorate to progress the item of business, or if this is not possible;
b) inviting on a temporary basis one or more of the following to make up the
quorum (where these are permitted members of the Governing Body or committee / sub-committee in question) so that the group can progress the item of business:
i) an individual appointed by a member to act on its behalf in the
dealings between it and the clinical commissioning group; ii) a member of a relevant Health and Wellbeing Board; iii) a member of a governing body of another clinical commissioning
group. Where any of the above are applied the arrangements will be recorded in the minutes. In general, commissioning through competitive tender or AQP should introduce greater transparency and help reduce the scope for conflicts. Depending on the nature of the conflict, GPs or other practice representatives could be permitted to participate in the Governing Body’s discussion about the proposed decision, but should not take part in any vote on the decision. The CCG will consistently adopt the specific additional safeguards set out in NHS England’s ‘Managing Conflicts of Interest: Statutory Guidance for CCGs (December 2014) which are designed to:
• Maintain the confidence and trust between patients and GPs; • Enable the CCG and Member Practices to demonstrate that they are acting
fairly and transparently; • That all Members will put their duty to patients before any financial interest,
and; • Ensure that the CCG operates within the legal framework and refrains from
engaging in anti-competitive behaviour.
A template document is attached at Appendix 3 which sets out the factors will provide evidential assurance to the Approvals Panel, the Audit, Scrutiny and Risk Committee and any other interested parties that services have been commissioned
15
54
in an open and transparent manner and with an absolute focus on meeting local health needs and priorities.
The CCG will ensure that details of all contracts, including the value of the contracts are published on the corporate website http://www.liverpoolccg.nhs.uk/ as soon as they are agreed. Where the CCG commissions services through AQP, the type of service commissioned and the agreed price of the service will be made available publicly as will information about those providers who qualify to provide the service.
10. DECISION-MAKING FOR THE COMMISSIONING PRIMARY MEDICAL CARE
Whilst the arrangements for primary medical care decision making do not preclude GP participation in strategic discussion on primary care issues, delegated commissioning responsibility from NHS England for primary medical care services exposes the CCG to an even greater risk of conflicts of interest which, if not managed effectively and decisively could adversely affect public confidence in the local commissioning system.
The CCG has established the Primary Care Commissioning Committee (as a committee of the CCG Governing Body) to enable the members to make collective decisions on the review, planning and procurement of primary care services in Liverpool under delegated authority from NHS England.
To ensure transparency, meetings of the Primary Care Commissioning Committee (including decision making and deliberations leading up to decision making) will generally be held in public unless the CCG considers it is appropriate to exclude the public due to the confidential nature of the business to be considered. Where any member of any meeting of the Primary Care Commissioning Committee has a personal interest in relation to the scheduled or likely business of the meeting (previously declared or otherwise) they must make a declaration which will be recorded in the minutes and managed as described in Sections 8 and 9 above. Where arrangements have been confirmed for the management of the conflict of interests or potential conflicts of interests in relation to the Chair, the Deputy Chair will act as Chair for the relevant part of the meeting and will ensure these arrangements are followed. Where no arrangements have been confirmed, the Deputy Chair may require the Chair to withdraw from the meeting (or part of it). Where there is no Deputy Chair, the members of the meeting will select one.
The Lay Member (Governance) of the Governing Body will take such steps as deemed appropriate and will request information considered relevant from individuals to ensure that all conflicts of interest and potential conflicts of interest are declared.
The Committee will present its minutes to Cheshire and Merseyside Sub-Regional Area Team (NHS England) and the Governing Body of Liverpool CCG each month for information, including the minutes of any sub-committees.
16
55
As set out throughout this policy, the CCG will endeavour to ensure that clear records of any conflicts of interests are maintained and made available for public inspection on request.
The Terms of Reference and membership for the Primary Care Commissioning Committee are attached as Appendix 5.
11. REGISTER OF INTERESTS, GIFTS, HOSPITALITIES AND SPONSORSHIP
Interests, gifts, hospitality and sponsorship will be recorded on the CCG’s Register of Interests and Hospitality, which will be maintained by the Chief Finance Officer on behalf of the Chief Officer. The register will be accessible by the public by postal application (or for inspection on request) at the CCG Headquarters, 1 Arthouse Square, Seel Street, Liverpool L1 7AZ. An electronic version of the Register of Interests and Hospitality Register can be accessed at http://www.liverpoolccg.nhs.uk/
All declarations of interest made by Governing Body members will be published in the CCG’s Annual Report.
12. DATA PROTECTION
The information provided will be processed in accordance with data protection principles as set out in the Data Protection Act 1998. Data will be processed only to ensure that the board members and employees act in the best interests of the CCG and the public and patients the group was established to serve. The information provided will not be used for any other purpose. Signing the declaration form will also signify consent to personal data being processed for the purposes set out in this policy.
13. MONITORING COMPLIANCE AND EFFECTIVENESS OF THIS POLICY
Decision-makers will be reminded of the policy and register of interests at least annually. The Chief Finance Officer will review register entries on a quarterly basis and take any action necessary as highlighted by the review. Regular and continued engagement will also take place between the CCG and its Member Practices to ensure that the principles contained within this policy are applied as best practice. Evidence of any deviation from this policy will be reported as an incident to the Chief Finance Officer and reviewed by the Audit, Risk & Scrutiny Committee.
14. TRAINING
All Governing Body members, committee/sub-committee members and CCG staff will be required to undertake mandatory training in relation to this policy once every two years (or sooner if there is a change in legislation or national guidance). This requirement will be stated in the CCG’s Organisational Development Plan. In this respect Liverpool CCG does not differentiate between permanent or temporary staff.
17
56
Details of training programmes and attendance sheets will be retained centrally by Liverpool CCG for audit and compliance monitoring.
15. REVIEW AND REVISION ARRANGEMENTS
This policy and associated procedures will be reviewed annually (or earlier if appropriate) by the CCG’s Approvals Committee to take account of any relevant changes in legislation or guidance, organisational change or other exceptional circumstances. Where significant revisions are made to this policy consultation will take place with the Governing Body and other stakeholders as appropriate for ratification and adoption by the CCG.
16. EQUALITY & DIVERSITY STATEMENT
Liverpool CCG is committed to ensuring that it treats its employees fairly, equitably and reasonably and that it does not discriminate against individuals or groups on the basis of their ethnic origin, physical or mental abilities, gender, age, religious beliefs or sexual orientation.
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP
Declaration of Financial and Other Interests for Members/Employees April 2015 – March 2016
Please complete in block capitals and return (including nil returns) to:
Appendix 1
18
57
Chief Finance Officer, Liverpool CCG, 3rd Floor, Arthouse Square, Seel Street, Liverpool L1 4AZ
Name (print)
Position or role within Liverpool CCG
Member / Employee/ Governing Body Member / Committee or Sub-Committee Member (including Committees and Sub-Committees of the Governing Body) [delete as appropriate]
Date Appointed
This is a new declaration This is a revised declaration
This form is required to be completed in accordance with the CCG’s Constitution and the Code of Accountability
Before completing this form, please note:
• Each CCG must make arrangements to ensure that the persons mentioned above declare any interest which may lead to a conflict with the interests of the CCG and the public for whom they commission services in relation to a decision to be made by the CCG.
• A declaration must be made of any interest likely to lead to a conflict or potential conflict as soon as the individual becomes aware of it, and within 28 days.
• If any assistance is required in order to complete this form, then the individual should contact Lynne Hill, Liverpool CCG by telephoning 0151 296 7195 or via email at [email protected]
• The completed form should be sent by both email and signed hard copy to the Chief Finance Officer, Liverpool CCG, 3rd Floor, Arthouse Square, Seel Street, Liverpool L1 4AZ
• Any changes to interests declared must also be registered within 28 days by completing and submitting a new declaration form.
• The register will be published as part of the CCG’s Governing Body meeting papers and will be available for the public on the CCG website www.liverpoolccg.nhs.uk or by postal application to the address given above.
• Any individual – and in particular members and employees of the CCG - must provide sufficient detail of the interest, and the potential for conflict with the interests of the CCG and the public for whom they commission services, to enable a lay person to understand the implications and why the interest needs to be registered.
• If there is any doubt as to whether or not a conflict of interests could arise, a declaration of the interest must be made. Interests that must be declared (whether such interests are those of the individual themselves or of a family member, close friend or other acquaintance of the individual) include:
o Roles and responsibilities held within member practices; o Directorships, including non-executive directorships, held in private
companies or PLCs;
19
58

o Ownership or part-ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG;
o Shareholdings (more than 5%) of companies in the field of health and social care;
o A position of authority in an organisation (e.g. charity or voluntary organisation) in the field of health and social care;
o Any connection with a voluntary or other organisation contracting for NHS services;
o Research funding/grants that may be received by the individual or any organisation in which they have an interest or role, and;
o Any other role or relationship which the public could perceive would impair or otherwise influence the individual’s judgement or actions in their role within the CCG.
If there is any doubt as to whether or not an interest is relevant, a declaration of the interest must be made. In the event of no interests to be declared, the form below should be completed with ‘nil return’ recorded and duly signed/dated.
Declaration
In accordance with the Code of Accountability I wish to declare the following interests that fall within the outlined within the Corporate Governance Framework to NHS Liverpool Clinical Commissioning Group:
Type of Interest Details Is this a personal interest or that of a family member, close friend or other acquaintance?
Roles and responsibilities held within member practices
Directorships, including non-executive directorships, held in private companies or PLCs
Ownership or part-ownership of private companies, businesses or consultancies likely or possibly seeking to do business with the CCG
Shareholdings (more than 5%) of companies in the field of health and social care
Positions of authority in an organisation (e.g. charity or voluntary organisation) in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that
20
59

Type of Interest Details Is this a personal interest or that of a family member, close friend or other acquaintance?
may be received by the individual or any organisation in which they have an interest or role
Any other specific interests?
Any other role or relationship which the public could perceive would impair or otherwise influence the individual’s judgement or actions in their role within the CCG
I understand that I have a responsibility at future meetings to declare my interest in any specific items on the agenda or as part of any project at the point of commencement. This will include any personal or immediate family interest which may impinge or might reasonably be deemed by others on my impartiality in any matter relevant to my duties as a member of NHS Liverpool Clinical Commissioning Group.
I confirm that to the best of my knowledge and belief, the above information is complete and correct and I have declared all interests of which I am aware might affect or be seen to affect my impartiality or judgement. I undertake to update as necessary and to review the accuracy of the information provided regularly and no longer than annually. I give my consent for the information to be used for the purposes described in the CCG’s Constitution and published accordingly.
Signature Date
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP
Declaration of Financial and Other Interests for Bidders/Contractors April 2015 – March 2016
Appendix 2
21
60
This form is required to be completed in accordance with the CCG’s Constitution and s140 of the NHS Act 2006 (as amended by the Health & Social Care Act 2012) and the NHS (Procurement, Patient Choice and Competition) (No2) Regulations 2013 and related guidance.
Notes:
• All potential bidders/contractors/service providers, including sub-contractors, members of a consortium, advisers or other associated parties (Relevant Organisation) are required to identify any potential conflicts of interest that could arise if the Relevant Organisation were to take part in any procurement process and/or provide services under, or otherwise enter into any contract with, the CCG, or with NHS England in circumstances where the CCG is jointly commissioning the service with, or acting under a delegation from, NHS England. If any assistance is required in order to complete this form, then the Relevant Organisation should contact Lynne Hill, Liverpool CCG by telephoning 0151 296 7195 or via email at [email protected];
• The completed form should be sent by both email (to the address above) and signed hard copy to the Chief Finance Officer, Liverpool CCG, 3rd Floor, Arthouse Square, Seel Street, Liverpool L1 4AZ
• Any changes to interests declared either during the procurement process or during the term of any contract subsequently entered into by the Relevant Organisation and the CCG must notified to the CCG by completing a new declaration form and submitting it to [specify].
• Relevant Organisations completing this declaration form must provide sufficient detail of each interest so that the CCG, NHS England and also a member of the public would be able to understand clearly the sort of financial or other interest the person concerned has and the circumstances in which a conflict of interest with the business or running of the CCG or NHS England (including the award of a contract) might arise.
• If in doubt as to whether a conflict of interests could arise, a declaration of the interest should be made.
Interests that must be declared (whether such interests are those of the Relevant Person themselves or of a family member, close friend or other acquaintance of the Relevant Person), include the following:
• the Relevant Organisation or any person employed or engaged by or otherwise connected with a Relevant Organisation (Relevant Person) has provided or is providing services or other work for the CCG or NHS England;
• the Relevant Organisation or Relevant Person is providing services or other work for any other potential bidder in respect of this project or procurement process;
• the Relevant Organisation or any Relevant Person has any other connection with the CCG or NHS England, whether personal or professional, which the public could perceive may impair or otherwise influence the CCG’s or any of its members’ or employees’ judgements, decisions or actions.
Declarations
22
61
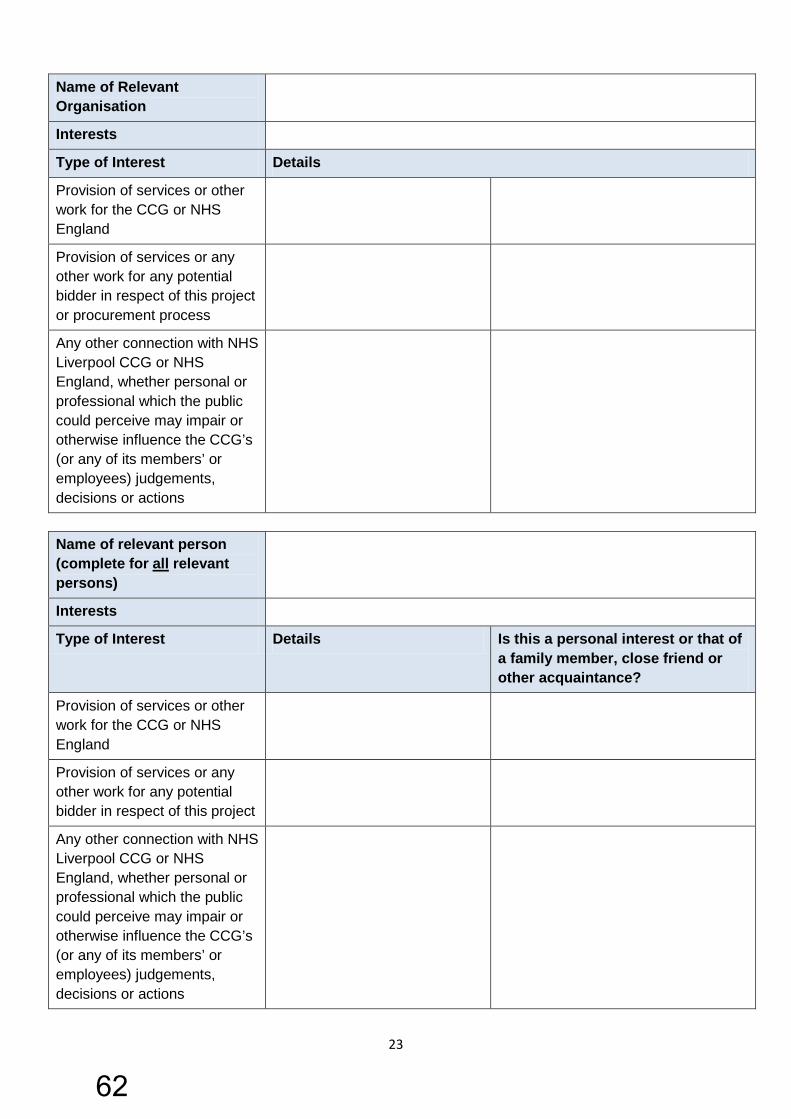
Name of Relevant Organisation
Interests
Type of Interest Details
Provision of services or other work for the CCG or NHS England
Provision of services or any other work for any potential bidder in respect of this project or procurement process
Any other connection with NHS Liverpool CCG or NHS England, whether personal or professional which the public could perceive may impair or otherwise influence the CCG’s (or any of its members’ or employees) judgements, decisions or actions
Name of relevant person (complete for all relevant persons)
Interests
Type of Interest Details Is this a personal interest or that of a family member, close friend or other acquaintance?
Provision of services or other work for the CCG or NHS England
Provision of services or any other work for any potential bidder in respect of this project
Any other connection with NHS Liverpool CCG or NHS England, whether personal or professional which the public could perceive may impair or otherwise influence the CCG’s (or any of its members’ or employees) judgements, decisions or actions
23
62
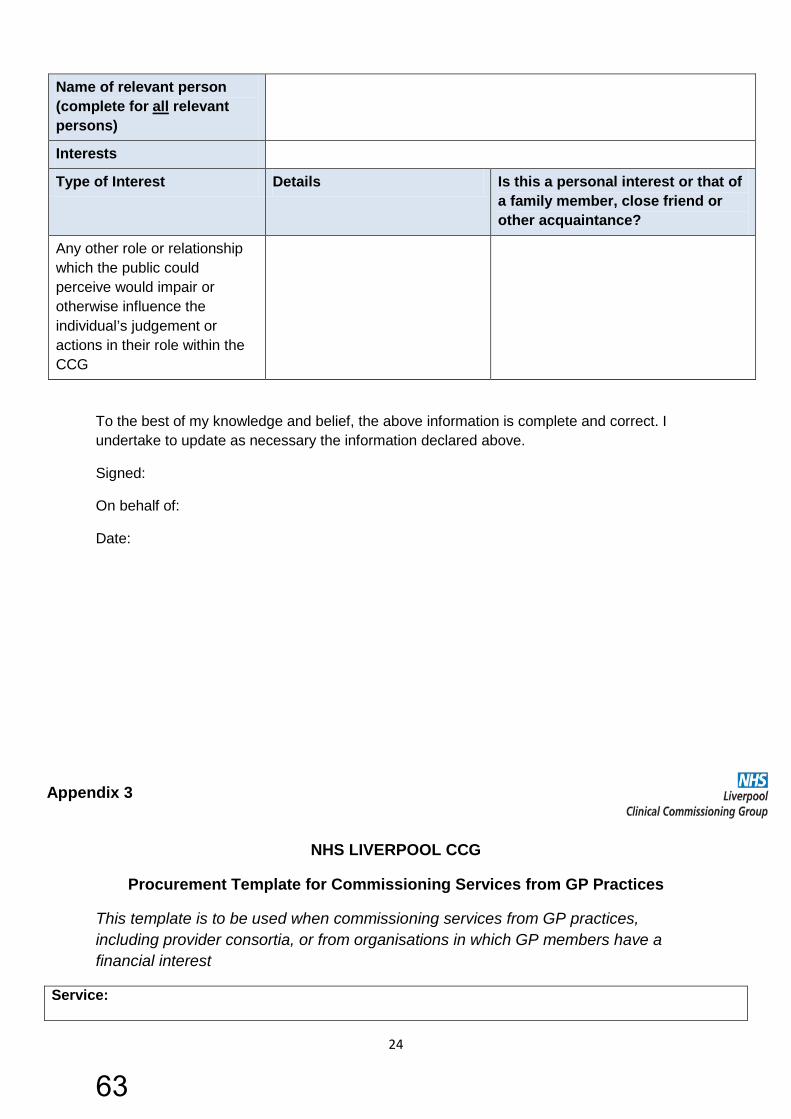
Name of relevant person (complete for all relevant persons)
Interests
Type of Interest Details Is this a personal interest or that of a family member, close friend or other acquaintance?
Any other role or relationship which the public could perceive would impair or otherwise influence the individual’s judgement or actions in their role within the CCG
To the best of my knowledge and belief, the above information is complete and correct. I undertake to update as necessary the information declared above.
Signed:
On behalf of:
Date:
NHS LIVERPOOL CCG
Procurement Template for Commissioning Services from GP Practices
This template is to be used when commissioning services from GP practices, including provider consortia, or from organisations in which GP members have a financial interest
Service:
Appendix 3
24
63
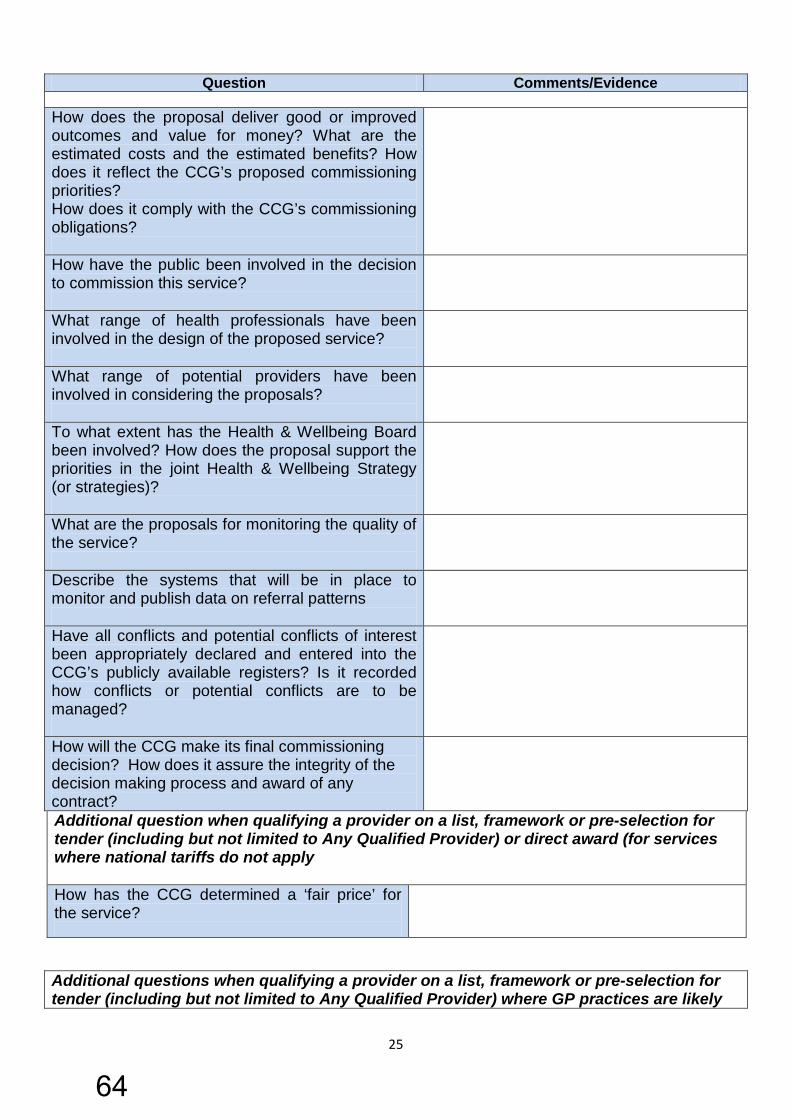
Question Comments/Evidence How does the proposal deliver good or improved outcomes and value for money? What are the estimated costs and the estimated benefits? How does it reflect the CCG’s proposed commissioning priorities? How does it comply with the CCG’s commissioning obligations?
How have the public been involved in the decision to commission this service?
What range of health professionals have been involved in the design of the proposed service?
What range of potential providers have been involved in considering the proposals?
To what extent has the Health & Wellbeing Board been involved? How does the proposal support the priorities in the joint Health & Wellbeing Strategy (or strategies)?
What are the proposals for monitoring the quality of the service?
Describe the systems that will be in place to monitor and publish data on referral patterns
Have all conflicts and potential conflicts of interest been appropriately declared and entered into the CCG’s publicly available registers? Is it recorded how conflicts or potential conflicts are to be managed?
How will the CCG make its final commissioning decision? How does it assure the integrity of the decision making process and award of any contract?
Additional question when qualifying a provider on a list, framework or pre-selection for tender (including but not limited to Any Qualified Provider) or direct award (for services where national tariffs do not apply How has the CCG determined a ‘fair price’ for the service?
Additional questions when qualifying a provider on a list, framework or pre-selection for tender (including but not limited to Any Qualified Provider) where GP practices are likely
25
64

to be qualified providers How will it be ensured that patients are aware of the full range of qualified providers from whom they can choose?
Additional questions for direct proposed awards to GP providers What steps have been taken to demonstrate that the services to which the contract relates are capable of being delivered by one provider?
In what ways does the proposed service go above and beyond what GP practices should be expected to provide under the GP contract?
What assurances will there be that the GP practice is providing high quality services under the GP contract before it has the opportunity to provide any new services?
APPROVALS COMMITTEE TERMS OF REFERENCE The Approvals Committee (the Committee) is established in accordance with NHS Liverpool Clinical Commissioning Group’s (the CCG) Constitution, Standing Orders and Scheme of Delegation. These terms of reference set out the membership, remit, responsibilities and reporting arrangements of the Committee.
1. Membership
Appendix 4
26
65
The Approvals Panel will have the following membership:
• Deputy Chair (Lay member) • Chief Officer • Chief Finance Officer • Chief Nurse • Secondary Care Clinician • Lay member Stakeholder engagement
Other representatives will be invited to attend to provide clinical or procurement expertise as necessary, at the discretion of the Chief Officer.
2. Remit and responsibilities of the Committee
The role of the Committee will be to provide neutrality in the evaluation and decision making processes. It will be made up of non-conflicted members of the Governing Body and its decisions will be noted by the Governing Body.
The Approvals Committee is responsible for ensuring that the CCG applies conflict of interest principles and policies rigorously and provides the CCG with independent advice and judgment where there is any doubt about how to apply them to individual or group cases involving commissioning clinical services.
The Approval Committee’s responsibilities are to:
• Judge whether or not there is a risk of a conflict of interest existing or arising;
• Confirm the appropriateness or otherwise of their handling of the matter as the best way to manage the risks, and;
• Provide advice to the CCG Governing Body as to any other course of action which may be desirable or more appropriate on the matter under consideration
The Committee will operate:
• Reactively, when the Chair of a meeting, individual Governing Body member, or Liverpool CCG as a whole seeks advice on a specific issue involving the commissioning of any clinical services,
• Proactively, when such a potential Conflict of Interest risk is identified and acts on it.
In either mode, the Approvals Committee will discuss the issue with those involved (and any other relevant party) and issue its written decision, advice or judgement for the Governing Body. The members of the Governing Body, its committees and sub-committees will agree that they will accept the decision advice or judgement of the Committee in such cases.
27
66

The existence of the Committee does not preclude the GB Board / or committee from discussing the appropriateness of certain clinical services or the desirability of significant investment in clinical services. The Committee would assume such informed discussion had taken place prior to items being submitted to it. The Committee does not replace the Governing Body and its committees but works with appropriate information to take the formal decision.
It should be noted that other conflicts of interest may arise that are not around the commissioning of clinical services and such conflicts are not currently proposed to be managed by this Committee.
3. Administration
The Committee Chair and Panel will be provided with appropriate support in the management of the Committee’s business. The Secretary will take minutes. 4. Quorum
The Committee Chair or Vice Chair and at least 3 voting members. If exceptionally, any of the members are conflicted, an additional member will be substituted.
5. Frequency and notice of meetings
The Committee will meet monthly or as necessary (virtually where applicable). Members shall be notified at least 10 days in advance that a meeting is due to take place. Agendas and reports shall be distributed to members at least 5 working days in advance of the meeting date.
6. Reporting
The Governing Body will receive and note the Panel’s conclusions and ratified minutes of the Approvals Committee.
7. Conduct
All members are required to make open and honest declarations of their interests at the commencement of each meeting or to notify the Committee Chair of any actual, potential or perceived conflict in advance of the meeting.
All members are required to uphold the Nolan Principles and all other relevant NHS Code of Conduct requirements.
Date and Review
These Terms of Reference were approved by the NHS Liverpool CCG Governing Body on 18 October 2013
28
67
To be reviewed on 18th October 2015
Liverpool Clinical Commissioning Group
Governing Body Primary Care Commissioning Committee
Terms of Reference
Role of the Committee
1. The Committee has been established to enable the members to make collective decisions on the review, planning and procurement of primary care
Appendix 5
29
68

services in Liverpool under delegated authority from NHS England. 2. In performing its role the Committee will exercise its management of the
functions in accordance with the agreement entered into between NHS England and Liverpool CCG, which will sit alongside the delegation and terms of reference.
3. The functions of the Committee are undertaken in the context of a desire to
promote increased co-commissioning to increase quality, efficiency, productivity and value for money and to remove administrative barriers.
4. The role of the Committee shall be to carry out the functions relating to the
commissioning of primary medical services under section 83 of The NHS Act.
5. This includes the following:
• GMS, PMS and APMS contracts (including the design of PMS and APMS
contracts, monitoring of contracts, taking contractual action such as issuing breach/remedial notices, and removing a contract);
• Newly designed enhanced services (“Local Enhanced Services” and “Directed Enhanced Services”);
• Consideration of local incentive schemes as an alternative to the Quality
Outcomes Framework (QOF);
• Decision making on whether to establish new GP practices in an area;
• Approving practice mergers; and
• Making decisions on ‘discretionary’ payment (e.g., returner/retainer schemes).
6. The CCG will also carry out the following activities:
a) To plan, including needs assessment, primary medical care services in
Liverpool;
b) To undertake reviews of primary [medical] care services in Liverpool;
c) To co-ordinate a common approach to the commissioning of primary care services generally;
d) To manage the budget for commissioning of primary [medical] care
services in Liverpool;
e) To drive the continuous improvement of primary care in order to deliver the ambitions of the Healthy Liverpool Programme.
30
69

Geographical Coverage
7. The Committee will comprise the Liverpool CCG area only.
Membership 8. The Committee shall consist of:
Chair - Lay Member (patient engagement) Lay member (Vice-Chair) Chief Officer Chief Finance Officer Chief Nurse 4 GPs (chair of existing Primary Care Quality Committee and 3 Locality Chairs) Co-opted non-voting members: HealthWatch Health and Wellbeing Board Governing Body Practice Nurse Governing Body Practice Manager LMC representative GP Advisor Advisory non-voting members: Head of Primary Care Quality and Improvement Head of Contracting and Procurement Deputy Chief Finance Officer
Meetings and Voting
9. The Committee will operate in accordance with the CCG’s Standing Orders. The Secretary to the Committee will be responsible for giving notice of meetings. This will be accompanied by an agenda and supporting papers and sent to each member representative no later than 5 days before the date of the meeting. When the Chair of the Committee deems it necessary in light of the urgent circumstances to call a meeting at short notice, the notice period shall be such as s/he shall specify.
10. Each member of the Committee shall have one vote. The Committee shall
reach decisions by a simple majority of members present, but with the Chair having a second and deciding vote, if necessary. However, the aim of the Committee will be to achieve consensus decision-making wherever possible.
Quorum
11. 5 voting members the majority of which must be lay/executive members
and including 2 GPs
31
70

12. Where the chair or any member of any meeting of the Primary Care Commissioning Committee has a personal interest, previously declared or otherwise, in relation to the scheduled or likely business of the meeting, they must make a declaration and the deputy chair will act as chair for the relevant part of the meeting. Where arrangements have been confirmed for the management of the conflict of interests or potential conflicts of interests in relation to the chair, the meeting must ensure these are followed. Where no arrangements have been confirmed, the deputy chair may require the chair to withdraw from the meeting or part of it. Where there is no deputy chair, the members of the meeting will select one.
13. Any declarations of interests, and arrangements agreed in any meeting of
the Primary Care Commissioning Committee will be recorded in the minutes.
14. Where more than 50% of the members of a meeting are required to
withdraw from a meeting or part of it, owing to the arrangements agreed for the management of conflicts of interests or potential conflicts of interests, the chair (or deputy) will determine whether or not the discussion can proceed.
15. In making this decision the chair will consider whether the meeting is
quorate, in accordance with the number and balance of membership set out in the CCG’s standing orders. Where the meeting is not quorate, owing to the absence of certain members, the discussion will be deferred until such time as a quorum can be convened. Where a quorum cannot be convened from the membership of the meeting, owing to the arrangements for managing conflicts of interest or potential conflicts of interests, the chair of the meeting shall consult with Lay Member (Governance) of the Governing Body on the action to be taken.
16. This may include:
a) requiring another of the CCG’s committees or sub-committees,
the CCG’s Governing Body or the Governing Body’s committees or sub-committees (as appropriate) which can be quorate to progress the item of business, or if this is not possible,
b) inviting on a temporary basis one or more of the following to
make up the quorum (where these are permitted members of the Primary Care Commissioning Committee) so that the CCG can progress the item of business:
i) a member (s) of a Governing Body of another Clinical
Commissioning Group.
These arrangements must be recorded in the minutes.
17. In any transaction undertaken in support of the Clinical Commissioning Group’s exercise of its commissioning functions (including conversations
32
71

between two or more individuals, e-mails, correspondence and other communications), individuals must ensure, where they are aware of an interest, that they conform to the arrangements confirmed for the management of that interest. Where an individual has not had confirmation of arrangements for managing the interest, they must declare their interest at the earliest possible opportunity in the course of that transaction, and declare that interest as soon as possible thereafter. The individual must also inform either their line manager (in the case of employees), or the Lay Member (Governance) on the Governing body of the transaction.
18. The Lay Member (Governance) of the Governing Body will take such
steps as deemed appropriate, and request information deemed appropriate from individuals, to ensure that all conflicts of interest and potential conflicts of interest are declared
Frequency of meetings
19. The Committee shall meet monthly in the first instance and frequency of meetings will be agreed thereafter.
20. Meetings of the Committee shall:
a) be held in public, subject to the application of 23(b);
b) the Committee may resolve to exclude the public from a meeting that is open to the public (whether during the whole or part of the proceedings) whenever publicity would be prejudicial to the public interest by reason of the confidential nature of the business to be transacted or for other special reasons stated in the resolution and arising from the nature of that business or of the proceedings or for any other reason permitted by The Public Bodies (Admission to Meetings) Act 1960 as amended or succeeded from time to time.
21. Members of the Committee have a collective responsibility for the
operation of the Committee. They will participate in discussion, review evidence and provide objective expert input to the best of their knowledge and ability, and endeavour to reach a collective view.
22. The Committee may delegate tasks to such individuals, sub-committees or
individual members as it shall see fit, provided that any such delegations are consistent with the parties’ relevant governance arrangements, are recorded in a scheme of delegation, are governed by terms of reference as appropriate and reflect appropriate arrangements for the management of conflicts of interest.
23. The Committee may call additional experts to attend meetings on an ad
hoc basis to inform discussions.
24. Members of the Committee shall respect confidentiality requirements as set out in the CCG’s Constitution.
33
72

25. The Committee will present its minutes to Cheshire and Merseyside Team (NHS England) and the governing body of Liverpool CCG each month for information, including the minutes of any sub-committees.
26. The CCG will also comply with any reporting requirements set out
in its constitution.
27. It is envisaged that these Terms of Reference will be reviewed periodically, reflecting experience of the Committee in fulfilling its functions. NHS England may also issue revised model terms of reference from time to time.
Accountability of the Committee
28. The Committee will at all times act in accordance with the CCG Standing Orders and scheme of delegation and ultimately accountable to the Governing Body.
Decisions
29. The Committee will make decisions within the bounds of its remit.
30. The decisions of the Committee shall be binding on NHS England and Liverpool CCG.
31. The Committee will produce an executive summary report which will be
presented to Cheshire and Merseyside Team (NHS England) and the governing body of Liverpool CCG each month [or longer] for information.
Date and Review
These Terms of Reference were approved by the NHS Liverpool CCG Governing Body on 13th January 2015.
Review date: January 2017
NHS LIVERPOOL CCG
DISPUTE RESOLUTION PROCESS FOR CONFLICTS OF INTEREST
1. Aim of this Procedure
Appendix 6
34
73
The aim of this procedure is based on the principles that disputes should be resolved informally and at the most local level possible. In the first instance the dispute should be raised with Liverpool CCG’s Deputy Chair/Lay Member for Governance who will provide mediation and appropriate guidance. If the dispute is not successfully resolved at this level, a complaint should be made following the steps set out in this document.
2. Objectives of this Procedure The objectives of this procedure are to:
a) Provide Liverpool CCG with an appropriate mechanism for dealing with disputes concerning conflicts of interest;
b) Resolve disputes transparently, fairly and consistently – assuring bidders and service providers of the CCG’s commitment to natural justice and procedural fairness;
c) To mitigate risks, protect the reputation of Liverpool CCG and prevent possible
legal challenges and costly external reference processes by maintaining an appropriate audit trail of cases considered.
When handling disputes Liverpool CCG will engage with all relevant stakeholders and publish the findings/outcomes of complaints within and across the CCG to ensure consistency. Proactively, the CCG will communicate the process and decision making criteria widely and in advance;
3. The Procedure for Dispute Resolution The following stages represent Liverpool CCG’s dispute resolution process in relation to conflicts of interest: 3.1 Stage One – Making the Complaint All complaints must be made in writing and submitted to the CCG Chair at the address below:
The Chair, Liverpool CCG 1 Arthouse Square Seel Street Liverpool L1 4AZ Email: [email protected]
35
74
Complaints will be acknowledged within five working days from the date of receipt and a copy of this process included. 3.2 Stage Two – Initial Assessment Following receipt of the complaint, the CCG Chair will review the details of the complaint and may contact the complainant to seek further clarification or information. If the complaint is not deemed to warrant further progress the complainant will be notified in writing and of the reasons behind the decision not to proceed. Where the complaint falls within the remit of this procedure it will proceed to the next stage, with confirmation made in writing to the complainant within 5 working days of the decision being made and an outline of the next steps. 3.3. Stage Three – Chair Review Following progression to Stage Three, the CCG Chair will review the complaint to determine whether a swift resolution could be achieved without the need to involve the Governing Body. The Chair may call a meeting of the parties concerned to discuss the matter informally and without prejudice. If the Chair is unavailable (or if the complaint involves the Chair) the Chief Officer will review the complaint and act in accordance with this procedure as appropriate. The Deputy Chair/Lay Member for Governance will be made aware of the complaint and will provide advice and guidance where necessary. If the matter cannot be resolved at this level, the Chair will progress the complaint to Stage Four, notifying the complainant in writing of the decision. 3.4 Stage Four - Referral to the Approvals Committee of the Governing Body Where complaints cannot be resolved at Stage Three, the Governing Body Approvals Committee (Chaired by the Deputy Chair/Lay Member for Governance) will formally review the complaint, using external advice as appropriate and as per the Committee’s Terms of Reference. The Approvals Committee may refer the matter to the Audit, Scrutiny and Risk Committee to advise on the appropriate of the procedures followed. 3.5 Stage Five – The Decision Once the Approvals Committee of the Governing Body has made a decision, it will write to the complainant notifying them of the outcome; explaining the rationale and necessary course of action to be taken. The Committee will also inform NHS England of the dispute and of the outcome. Timescales for the conclusion of each stage will be determined depending on the complexity of the complaint and on a case-by-case basis. However, the CCG will endeavour to ensure that the process as a whole will take no longer than three months from the date of receipt of the complaint.
36
75
It is expected that most complaints will be successfully resolved under this process. However, where complainants are unhappy with the outcome or are dissatisfied with how their case has been handled by the CCG, they may complain to NHS England’s sub-regional area team (Cheshire & Merseyside) within three months of receipt of Liverpool CCG’s final decision by writing to:
NHS England (Cheshire & Merseyside Sub-Regional Area Team) Regatta Place Brunswick Business Park Summers Road Liverpool. L3 4BL
Conflicts of Interest – Guidance & Frequently Asked Questions
Why is this guidance document needed?
Appendix 7
37
76

GP members actively involved in commissioning decisions can often have a wide range of interests in healthcare businesses which provide services such as diagnostics, pharmacy (including internet pharmacies), minor surgery and out of hours primary care services to name but a few. Involvement can range from local directorships to shareholdings in much larger private sector companies which provide medical care. The presence of numerous different professions and professionals in any health economy means that conflicts of interest cannot always be avoided, but by identifying them early and assessing where they may influence decision making, the CCG will be able to shape an appropriate response. Apart from our legal obligation to continually demonstrate the transparency of decision making and ability to manage conflicts of interest, the CCG’s Constitution is reflective of our commitment to ensure appropriate management of public money, effective public engagement and of course, the best outcomes for our patients. Managing conflicts of interest effectively and maintaining public confidence in the integrity of our decision making requires a balanced and proportionate approach; ensuring arrangements are robust enough to withstand scrutiny but not so restrictive that it makes the decision making process overly complex and slow. Therefore this guidance is intended to protect and empower members by making conflicts of interest easier to identify, manage and avoid in advance, rather than waiting for them to arise. As individuals, GPs make commissioning decisions every day when they refer a patient for further care, diagnosis and/or treatment. If the referring GP is a service provider, then it is incumbent on them to ensure that the patient is aware of all the facts and promote alternative choices so that they can then make an informed decision in relation to their treatment. The same principals apply for the CCG, albeit on a much larger scale. Commissioning decisions for a service transformation/reconfiguration could be considered flawed if any CCG members involved in the consultation process could directly benefit from the proposed changes. What are the risks for the CCG? Conflicts can often inhibit free discussion and could result in decisions or actions being perceived as based on external influences; implying that the CCG has not acted in the best interests of the patients and public. As well as the potential to significantly damage the reputation of the CCG (to an extent where public trust has been lost) regulatory and/or criminal action could be taken against the CCG as a whole or any individuals found to have acted improperly. It is near impossible to describe all instances where an interest may be a real or perceived conflict, and it is essentially about exercise of judgement when deciding to register any interests that may be interpreted as a conflict. Individuals can seek guidance from the Chief Finance Officer, but the general rule of thumb is that if there is even a minor doubt, it should be declared. The scenarios below give some common examples of where conflicts of interest may occur:
38
77
Q - I am a GP Governing Body member and am also a board member of a healthcare business tendering for a contract with the CCG. Do I have to declare this as a conflict? A - This is probably the most recognisable form of ‘direct financial interest’ and could be considered as giving the healthcare business an unfair competitive advantage, particularly if the GP in the scenario were to be involved in any consultation process which could (or be seen to) influence the eventual decision. The procurement process needs to be right from the outset, and any conflicts of this nature should be declared.
Q - I am GP Governing Body member and I have a close relative who is a shareholder in a company that has just submitted a tender to provide services. Do I have to declare an interest?
A - An ‘indirect financial interest’ can arise when a close relative of a CCG member benefits from the decisions of the Clinical Commissioning Group. The GP member could be seen to benefit indirectly, particularly if their financial affairs are tied with their spouse or partner’s through the legal concept of “joint purse”. Whether this would create a serious concern would depend greatly on the circumstances and, more importantly, what measures are in place (or have been taken) to reduce or eliminate the risk. The GP member could simply declare it and exclude themselves from any decision making or consultation process, with the CCG responsible for ensuring the action is evidenced and that the conflicted GP Member is not involved in any subsequent contract monitoring arrangements.
Q - I am a GP and a member of a committee that approves the specification for a locally commissioned service that my practice is hoping to provide. Is this a conflict of interest?
A - Any situation in which a committee member’s personal interests or responsibilities may, or may appear to, influence the decision-making process could be regarded as a conflict. In this scenario, the GP could materially benefit from providing a Locally Enhanced Service and as they are involved in the approval of the specification it would be regarded as a direct financial interest. In this case the GP should either exclude themselves from relevant parts of meetings (including discussions focused on the specification) or not participate in the decision-making itself (i.e. not have a vote). Q - Is there a conflict of interest if I am a GP on the Committee that approves Prescribing Quality Schemes; a scheme that I may benefit from personally if approved?
A - The CCG will inevitably make decisions which will affect all our member practices. This situation cannot be avoided but if managed appropriately, should
39
78
safeguard against conflicts. This could include, for example ensuring decision makers are non-GP members of the Governing Body and therefore not in a position to benefit from the distribution of practice incentive scheme payments or other quality related rewards drawn from CCG allocated monies. Q - If I sit on panel that votes to approve payments to GPs for attendance at locality meetings, is this a conflict of interest?
A - If the GP in this case will receive a payment then the key point to recognise here is that a decision maker will be able to benefit from the decisions they take and a conflict of interest is therefore present. This situation must be managed appropriately if it cannot be avoided and where possible, the panel member should declare their interest and remove themselves from the decision making process. If this affects quorum the CCG’s Standing Orders can provide for a review of the decision made by another panel, committee or external partner organisation; although the likely outcome may be that the item cannot be decided upon at that meeting. Whether there are actual or perceived conflicts of interest the consequences can be very much visible and highly publicised. Q - If I have to withdraw from a meeting where I have declared a conflict of interest what should I expect? A - Members who withdraw due to a conflict are entitled to receive edited minutes which should reflect that the individual concerned has not unduly influenced the debate and related decision.
Q - What are non-financial or personal conflicts? A - These occur where CCG Governing Body members receive no financial benefit, but are influenced by other external factors such as:
• To gain some other intangible benefit such as gaining status or wider recognition from the decision made, and;
• Awarding contracts to friends or personal business contacts (favouritism) It is also possible for conflicts of interest to arise as part of the recruitment process and the promotion/performance management of staff. Transparency in relation to appointments to the Governing Body and associated committees avoids any accusations of favouritism (real or perceived). This includes passing on CVs of friends, family or acquaintances for consideration. Q - What is a conflict of loyalties? A - Conflicts of loyalty arise when a Governing Body member’s decision making could be influenced by their other interests or affiliations with other organisations. Although the member may not gain any benefit, Governing Body members may frequently experience competing loyalties between the Clinical Commissioning
40
79

Group and another person or entity (including their own GP practice and patients). For healthcare professionals, this could also extend to membership of a particular professional body, society, special interest group or charities. Conflicts of loyalties are often difficult to determine and depend greatly on the circumstances and the nature of the decision being made, and to where the primary duty of the individual lies. Conflicting loyalties could arise where Governing Body members owe or may feel loyalty towards family, friends, other people or organisations that are part of the member’s network. A conflict of loyalty could also be perceived where the religious, political or personal views of a Governing Body member or staff could potentially be perceived as interfering with their ability to make decisions in the best interests of the CCG (e.g. active membership of a political party campaigning against the de-commissioning of a service). Q – How can a close friendship or relationship cause a conflict of interest? A - This greatly depends on context and whether the close friendship/relationship could be construed as a conflict of interests in a particular given situation. For example, a Governing Body member has a close friend who is a Director at a healthcare provider in a neighbouring borough with whom they often meet socially for meals and drinks. The CCG does not currently have a contract with the healthcare provider but the Governing Body member registers this as a potential conflict. The healthcare provider subsequently bids for CCG business following a procurement process. In this scenario, when the Governing Body member originally registered the close friendship there was no actual conflict of interest; however, as soon as the provider submitted a bid the conflict became ‘live’ as the context of the relationship with the close friend in question could be construed as being influential in the decision making. As the Governing Body member has proactively declared this as a potential conflict of interest, the management of the situation is much easier and the member simply withdraws from the decision making process. It is important to note from this example that although a conflict is declared, it doesn’t necessarily means one exists at that particular point in time, but could should the circumstances change. A declaration is a proactive approach to safeguard both parties AND the CCG from any suggestion of bias or flawed decision making. Q - Can I accept gifts and hospitalities? A - CCG members, staff and directors are advised to simply refuse gifts or hospitality rather than declare after the event. There is some flexibility in relation to gifts of low value (less than £30) such as promotional pens and diaries but gifts or hospitality of high value (i.e. more than £30, including accrual of individual gifts above that value) should always be refused and reported to the Chief Finance Officer. Again, the test applied should always consider whether the acceptance of a gift could, or could be seen to exploit the influence of the individual’s position in the CCG and question their integrity. Q - Is it acceptable for drug companies to pay for or develop training for practices or the CCG?
41
80

A – Whilst this is usually acceptable for member practices, for the CCG there could be a very high potential for this to be perceived at worst as preferential treatment, or at best a way for the drug company to gain access to key people in the CCG. That said, the CCG also has a finite running cost allowance and has to explore ways in which to work leaner, smarter and be more efficient. The key consideration here is whether it falls under ‘sponsorship’ or ‘joint working’. In sponsorship arrangements, pharmaceutical companies will provide funding for a specific event (or training programme) whereas ‘joint working’ involves the CCG jointly agreeing goals with a private company (e.g. a pharmaceutical company) with the focus on improved patient outcomes, effective packages of care etc. In joint working the management arrangements are conducted with participation from both parties in an open and transparent manner, and would therefore stand up to scrutiny. Where can I get further advice or information?
Further advice and information is available from the Chief Finance Officer, Liverpool CCG by telephoning 0151 296 7195 or via email at [email protected]
Further reading
NHS England – Managing conflicts of interest: Statutory Guidance for CCGs http://www.england.nhs.uk/wp-content/uploads/2014/12/man-confl-int-guid-1214.pdf NHS England - Managing conflicts of interests: Guidance for clinical commissioning groups (March 2013) http://www.england.nhs.uk/wp-content/uploads/2013/03/manage-con-int.pdf NHS England - Procurement of healthcare (clinical) services (2012) http://www.england.nhs.uk/wp-content/uploads/2012/09/procure-intro.pdf NHS England - Code of Conduct: Managing conflicts of interest where GP practices are potential providers of CCG-commissioned services (2012) http://www.england.nhs.uk/wp-content/uploads/2012/09/c-of-c-conflicts-of-interest.pdf NHS Confederation/RCGP - Managing conflicts of interest in clinical commissioning groups http://www.nhsconfed.org/Publications/Documents/Managing_conflicts_of_interest_in_CCGs.pdf Co-operation and Competition Panel: www.ccpanel.org.uk
42
81

828282

Report no: GB 14-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report Variations to NHS Liverpool CCG Constitution
Lead Governor Dr Nadim Fazlani
Senior Management Team Lead
Katherine Sheerin Chief Officer
Report Author
Stephen Hendry, Senior Corporate Services Manager (Performance & Operations)
Summary The purpose of this paper is to bring to the Governing Body’s attention the further revisions made to the CCG’s Constitution as a result recommendations made by NHS England following the CCG’s application for approval of variation.
Recommendation That the Governing Body Notes the revisions made as an amended
submission to NHS England for approval of variation.
Formally adopt (and explicitly minute) the statement at paragraph 9.9 of the Constitution which clarifies and strengthens the CCG’s commitment to ensuring that all Governing Body members of the CCG, committee members and all staff can raise concerns in an environment that is safe and which values openness and transparency.
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
The variations are intended to further strengthen the Constitution and reaffirm the CCG’s commitment to improving health outcomes, maximising value from financial resources and the overall effective discharge of its role, functions and statutory duties.
Page 1 of 10
838383
Relevant Standards or targets
Health & Social Care Act 2012 (section 14E); Legislative Reform Order 2014; The Seven Principles of Public Life (The Nolan Principles).
NHS LIVERPOOL CCG VARIATION TO CONSTITUTION 1. PURPOSE The paper is to advise the Governing Body of the further revisions made to the CCG Constitution and provide assurances that the Constitution continues to be ‘fit for purpose’; reflecting current NHS England guidance and legislative changes that have taken effect in 2014. 2. RECOMMENDATIONS The Governing Body is asked to note the revisions made which reflect the amended Constitution submission to NHS England in January 2015 for approval and to formally adopt (and explicitly minute) the statement at paragraph 9.9 of the Constitution which clarifies and strengthens the CCG’s commitment to ensuring that all members of the Governing Body, its committees and individuals employed by the CCG feel that they are protected and can raise concerns in an environment that is safe and which values openness and transparency. 3. BACKGROUND The CCG’s Constitution has recently undergone a number of changes to reflect the strengthening of the CCG’s governance structures, revised arrangements for decision making and updated committee structures. The Governing Body will be aware that NHS Liverpool CCG submitted its revised Constitution to NHS England for approval in January 2015 after consultation with all member practices, the Local Medical Committee and other key stakeholders. The CCG received detailed feedback from NHS England regarding its application on 13th January 2015, which subsequently highlighted that further amendments to the CCG Constitution were necessary in order to meet the requirements of the Act. The Governing Body’s attention is therefore drawn to the following areas of the Constitution which have been inserted or amended:
• The effective date of approval on the cover sheet has been left blank as the date on which NHS England formally endorse the application will be inserted once confirmation has been received;
Page 2 of 10
848484

• Removal of all references to ‘co-opted’ members in paragraph 6.8.2 (i) in favour of NHS England model wording to describe ‘non-voting’ members and their participation;
• Insertion of paragraphs 6.8.3 (a) to (h) identifying all eight committees of the Governing Body and summarising their functions;
• Insertion of paragraphs 7.8 to 7.11 describing the statutory roles of Lay Member (Governance, Financial Management and Audit), Lay Member (Patient and Public Involvement), Secondary Care Doctor and Registered Nurse as per CCG Regulations 2012, and;
• Insertion of NHS England model wording to reflect the rights of Governing Body members, committee members and all CCG staff to make protected disclosures in Section 9, paragraph 9.9 (p45).
Member practices and the Local Medical Committee were consulted on 21st January 2015 and no representations had been received by the response deadline of 30th January 2015, indicating members’ (and Local Medical Committee) agreement with the revisions. The attached relevant ‘annotated’ extracts of the variations to the CCG Constitution are included as Appendix 1. The revised Constitution document has been re-submitted to NHS England pending the Governing Body’s formal adoption of the variations highlighted in this report. 4. SUMMARY The revisions to the Constitution have been made to ensure that the CCG continues to meet the requirements of the Act and comply with specific guidance from NHS England to support NHS Liverpool CCG’s application for variation. The changes have been thoroughly assessed and have been determined as non-detrimental to the discharge of the CCG’s statutory duties and responsibilities, or to the discharge of its functions.
Stephen Hendry Senior Corporate Services Manager
(Performance & Operations) 28th January 2015
ENDS
Page 3 of 10
858585
Appendix 1
NHS LIVERPOOL CCG CONSTITUTION VARIATION EXTRACTS
1. Extract from Section 6 - Decision Making: The Governance Structure The following paragraphs have been amended to reflect model wording from NHS England in relation to Governing Body Membership and non-voting members. The references to ‘co-opted members’ in 6.8.2 (i) have been replaced by wording which clarifies participation in meetings for non-voting members:
6.8.2. Composition of the Governing Body - the Governing Body shall not
have less than 16 Governing Body Members and comprises of:
a) 9 GP Representatives, one of whom shall be elected as the Chair, to be elected in respect of the Localities as follows:-
i) Liverpool Central Locality – 4 GP Representatives ii) Matchworks Locality – 3 GP Representatives iii) North Locality – 2 GP Representatives
b) 1 Nurse Representative
c) 1 Lay Person (Governance)
d) 1 Lay Person (Engagement) e) 1 Registered Nurse Member;
f) 1 Secondary Care Specialist;
g) the Accountable Officer;
h) the Chief Finance Officer;
i) The Governing Body may invite such other person(s) to attend all or any
of its meetings or part(s) of a meeting, in order to assist in its decision –making and discharge of its functions as it sees fit. Any such person may speak and participate in debate, but may not vote.
j) The Governing Body will invite the following individuals to attend any or
all of its meetings and participate in the way as described in in 6.8.2 (i) above:
k) The Director of Public Health for Liverpool;
Page 4 of 10
868686
l) Representative(s)from Liverpool Local Authority, Social Care;
m) A representative from each of the three Localities (which shall be the
Locality Chair if this person is not an elected member of the Governing Body);
n) A representative from the Local Medical Committee (LMC);
o) A Practice Manager working in one of the Member Practices
1.1 Extract from Section 6 - Decision Making: The Governance Structure (6.8.3 -
committees of the Governing Body)
The following paragraphs have been inserted to summarise and describe the functions of the committees/sub-committees of the Governing Body (as per NHS England recommendations, January 2015):
6.9. Committees of the Governing Body - the Governing Body has
appointed the following committees and sub-committees:
a) Audit Committee – the Audit Committee, which is accountable to the CCG’s Governing Body, provides the Governing Body with an independent and objective view of the CCG’s financial systems, financial information and compliance with laws, regulations and directions governing the CCG in so far as they relate to finance. The Audit Committee will also have a role to scrutinise internal decision making within the CCG. The Governing Body has approved and keeps under review the terms of reference for the audit committee, which includes information on the membership of the audit committee.
b) Remuneration Committee – the Remuneration Committee, which is accountable to the CCG’s Governing Body makes recommendations to the Governing Body on determinations about the remuneration, fees and other allowances for employees and for people who provide services to the CCG and on determinations about allowances under any pension scheme that the CCG may establish as an alternative to the NHS pension scheme. The Governing Body has approved and keeps under review the terms of reference for the remuneration committee, which includes information on the membership of the remuneration committee.
c) Primary Care Commissioning Committee – the Primary Care Committee which is accountable to the CCG’s Governing Body, makes collective decisions on the review, planning and procurement of primary care medical services in Liverpool under delegated authority from NHS England. In performing this role the Committee exercises its management of the functions in accordance with the agreement entered into between NHS England and Liverpool CCG which is undertaken in the context of the promotion of increased co-commissioning to increase quality, efficiency,
Page 5 of 10
878787
productivity and value for money. The Governing Body has approved and keeps under review the terms of reference for the Primary Care Committee, which includes information on the membership of the committee**.
d) Finance, Procurement and Contracting Committee - The Finance, Procurement and Contracting Committee, which is accountable to the CCG’s Governing Body, is responsible to assure delivery of the QIPP programme and agree corrective action (if required) on behalf of the Governing Body. The Committee will also assure delivery of statutory financial duties and financial reporting arrangements; processes for procurement and contracts (in line with prevailing strategies); processes for Information Governance and assure processes for enabling choice on behalf of the on behalf of the Governing Body. The Governing Body has approved and keeps under review the Terms of Reference for the Finance, Procurement and Contracting Committee, which includes information on the membership of the committee.*
e) Quality, Safety & Outcomes Committee - the Quality, Safety and Outcomes Committee, which is accountable to the CCG’s Governing Body will make recommendations to the Governing Body on quality and safety processes across all commissioned services, ensuring alignment with delivery of the NHS Outcomes Framework, and for assuring the CCG Governing Body that quality and patient safety activity is coordinated and transparent ensuring a coherent and systematic review of the system. The Governing Body has approved and keeps under review the terms of reference for the Quality, Safety and Outcomes Committee, which includes information on the membership of the committee.*
f) Approvals Committee – the Approvals Committee, which is accountable to the CCG’s Governing Body will provide neutrality in the evaluation and decision making processes and is responsible for ensuring that the CCG applies conflicts of interest principles and policies rigorously; providing the Governing Body with independent advice and judgement where there is any doubt about how these should be applied to individual or group cases involving clinical services. The Committee will judge where risks of conflicts of interest exist or may arise and confirm the appropriateness (or otherwise) of their handling of the matter in terms of the best way to manage such risks appropriate to the matter under consideration. The Governing Body has approved and keeps under review the terms of reference for the Approvals Committee, which includes information on the membership of the committee.*
g) Healthy Liverpool Programme Leads Board – the Healthy Liverpool Programme Leads Board is accountable to the CCG’s Governing Body and will act as a forum for development and partnership working. It is not a decision making body which can commit members to any course of action (including expenditure) but will be expected to make recommendations to appropriate bodies as appropriate to Liverpool CCG and other key organisations to ensure alignment between the Healthy Liverpool Programme and the plans for each organisation included in the programme. The Governing Body has approved and keeps under review
Page 6 of 10
888888

the terms of reference for the Healthy Liverpool Programme Leads Board, which includes information on the membership of the committee.*
h) Human Resources Committee - the Human Resources Committee is accountable to the Governing Body and will determine HR policies and salary frameworks for employees and other persons working on behalf of the CCG. The Committee will monitor organisational performance on corporate workforce indicators including the Annual Staff Survey, Equality & Diversity and Sickness Absence; providing assurance to the Governing Body that performance is managed. The Governing Body has approved and keeps under review the terms of reference for the Human Resources Committee, which includes information on the membership of the committee.*
6.8.4 The Governing Body may change the number of committees, their terms of reference and membership as required in order to meet the needs of the organisation and in line with the principles of good governance.
*Copies of the Terms of Reference and membership of these committees can be found on the Liverpool CCG website www.liverpoolccg.nhs.uk
** New ToR Dec 2014 to reflect co-commissioning arrangements of Primary Care Medical Services under Section 83 of the NHS Act.
2. Extract from Section 7 – Roles and Responsibilities The following paragraphs have been inserted to comply with the National Health Service (Clinical Commissioning Groups) Regulations 2012. These insertions summarise the roles of the Lay Member (Governance, Financial Management and Audit; Lay Member (Patient and Public Involvement); Secondary Care Doctor and Chief Nurse:
7.8. Role of the Lay Member (governance, financial management and audit)
7.8.1. The Lay Member with a lead role in overseeing key elements of governance, financial management and audit is a member of the Governing Body and is responsible for bringing specific expertise and experience to the work of the Governing Body.
7.8.2. This role of the Lay Member has been summarised in a national
document as:
a) acting as Chair of the Audit Committee; overseeing key elements of governance including audit, remuneration and managing conflicts of interest;
Page 7 of 10
898989

b) ensuring that the Governing Body and the wider CCG behaves
with the utmost probity at all times;
c) ensuring that appropriate and effective whistle blowing and anti-fraud systems are in place. overseeing robust audit and governance arrangements leading to propriety in the use of the CCG’s resources;
d) as Chair of the Audit Committee the Lay Member will also act as
Deputy Chair of the CCG Governing Body.
7.9. Role of the Lay Member (patient and public involvement)
7.9.1. The Lay Member with a lead role in championing patient and public involvement is a member of the Governing Body and is responsible for bringing specific expertise and experience to the work of the Governing Body as well as knowledge of the local community.
7.9.2. This role of the Lay Member has been summarised in a national
document as:
a) ensuring public and patients’ views are heard and their expectations met and understood as appropriate;
b) ensuring that the CCG builds and maintains an effective relationship with Healthwatch Liverpool and draws on existing patient and public engagement and involvement expertise, and;
c) ensuring that the CCG has appropriate arrangements in place to
secure public and patient involvement and responds in an effective and timely way to feedback recommendations from patients, carers and public;
7.10. Role of the Governing Body Clinical Member – Secondary Care Doctor
7.10.1. The Secondary Care Doctor is a clinical member of the Governing Body and has responsibility for bringing a broader view on health and care issues which underpin the work of the CCG.
7.10.2. The role of the Clinical Member - Secondary Care Doctor has been
summarised in a national document as:
a) bringing to the Governing Body a high level of understanding of patient care in a secondary care setting;
Page 8 of 10
909090
b) giving an independent strategic clinical view on all aspects of CCG
business;
c) ensuring that the Governing Body and wider CCG acts in the best interests of the health of the population at all times, and;
d) ensuring that the CCG commissions the highest quality services
with a view to securing the best possible outcomes for patients within allocated resources whilst maintaining a focus on quality, integration and innovation.
7.11. Role of the Governing Body Clinical Member – Registered Nurse
7.11.1. The Registered Nurse is a clinical member of the Governing Body and has responsibility for bringing a broader view from their perspective as a registered nurse on health and care issues which underpin the work of the CCG; especially in regard to the contribution of nursing to patient care.
7.11.2. This role of the Clinical Member - Registered Nurse has been
summarised in a national document as:
a) giving an independent strategic clinical view on all aspects of CCG business;
b) ensuring that the Governing Body and wider CCG acts in the best
interests of the health of the population at all times, and;
c) ensuring that the CCG commissions the highest quality services with a view to securing the best possible outcomes for patients within allocated resources whilst maintaining a focus on quality, integration and innovation.
3. Extract from Section 9 – The Clinical Commissioning Group as an Employer This revision is in response to NHS England ‘Update & Advice for CCGs on the process and approval of severance payments and wording in constitutions on whistleblowing’ (Sir David Nicholson, May 2013, Gateway ref: 0053). This document references NHS England’s Model Constitution Framework for CCGs paragraph 9.9 “The group will adopt a code of conduct for staff and will maintain and promote effective whistleblowing procedures to ensure that concerned staff have means through which their concerns can be voiced.” and requests that CCG Governing Bodies to formally adopt (and explicitly minute) the following statement, which has been inserted in Section 9 (paragraph 9.9) in the January 2015 CCG Constitution;
Page 9 of 10
919191
9.9. The CCG recognises and confirms that nothing in or referred to in this
constitution (including in relation to the issues of any press release or other public statement or disclosure) will prevent or inhibit the making of any protected disclosure (as defined by the Employment Rights Act 1996, as amended by the Public Interest Disclosure Act 1998) by any member of the CCG, any member of its Governing Body, any member of its committees or sub-committees or the committees or sub-committees of the Governing Body, or any employee of the CCG or any of its members, nor will it affect the rights of any worker (as defined in that Act) under that Act.
Ends
Page 10 of 10
929292
Report no: GB 15-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report Personal Health Budgets -
Personalisation & Personal Budgets Policy - Liverpool City Council/ Liverpool CCG
Lead Governor Jane Lunt Chief Nurse
Senior Management Team Lead
Kim McNaught Deputy Chief Finance Officer
Report Author
Alison Ormrod Chief Accountant
Summary The purpose of this paper is to inform the Governing Body of joint policy arrangements developed between the CCG and Liverpool City Council to meet the requirements of the introduction of Personal Health Budgets for children and young people with special education needs and disability.
Recommendation That Liverpool CCG Governing Body: Notes that the policy was endorsed by the Finance,
Procurement and Contracting Committee at the meeting on 27th January 2015.
Approves the content of the policy as applicable to the CCG.
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
The policy demonstrates the processes required to support the implementation of the requirements of the Children and Families Act 2014. Evidence from the evaluation of pilot sites for personal health budgets indicated that personal health budgets led to:
• Improved quality of life Page 1 of 5
939393
• Reduction in the use of unplanned care • Benefits were particularly evident for people with
high levels of need. Relevant Standards or targets
NHS Outcomes • Ensuring that people have a positive experience of
care. • Enhancing quality of life for people with long term
conditions.
Page 2 of 5 949494

Personal Health Budgets - Personalisation & Personal Budgets Policy - Liverpool City Council/
Liverpool CCG
1. PURPOSE During 2014 Liverpool City Council worked with the CCG around the development of arrangements to support the requirements of the Children and Families Act 2014 - Special Educational Needs and Disability (SEND) including systems for the operation of personal budgets. The attached paper summaries the approach developed by the Council and the CCG, as appropriate, into a Personalisation - Personal Health Budget policy. 2. RECOMMENDATIONS The policy was taken to the Liverpool City Council Cabinet for ratification and formal adoption on 26th January 2015. Following endorsement by the Finance, Procurement and Contracting Committee on 27th January 2015, the Governing Body is asked to approve the policy and its application to the CCG. 3. BACKGROUND Personal Health Budgets were piloted across England between 2009 and 2012. In response to findings from the evaluation of the pilot schemes the Government announced a phased approach to introducing personal health budgets. As a first step from April 2014, people eligible for NHS Continuing Health Care or Continuing Care have had the “right to ask” for a personal health budget, including a direct payment. From October 2014 this became a “right to have” a personal health budget. The CCG has legal obligations relating to personal health budgets. These include duties to:
• publicise and promote their availability; • to provide information and advice; • consider requests for personal health budgets; • develop systems and process to be able to make this provision.
Page 3 of 5 959595

A personal health budget is an amount of money to support a person’s identified health and well-being needs. Application of the funds identified is planned and agreed between the individual, their representative or in the case of children, their families and carers. The funds are not new monies; NHS funding that would have been spent on a person’s care will be spent more flexibly to meet individual identified need. The Children and Families Act 2014 reforms earlier Special Educational Needs provisions. The Act imposes a duty on local authorities to prepare and maintain, where necessary, an Education, Health and Care Plan (EHC) for children and young people who have SEND. The Council is required to publish a Local Offer, which sets out available provision across health, education and social care for children and young people (18 to 25) with SEND. Personalisation is central to the SEND reforms. The Act specifies that a young person or their family can request a personal budget or direct payment if they have a qualifying health, social care or education need. The expectation is that the local authority, school or health organisation will develop the Liverpool offer over time to identify how money can be spent to ensure the achievement of agreed outcomes. An EHC plan results from a co-ordinated assessment which specifies the outcomes sought for a child or young person with SEND across education social care and where appropriate health. A Personal Budget is an allocation of funding identified to provide support to meet all or some of the outcomes in the EHC plan. A Personal Health Budget will apply to children and young people who receive or are assessed as meeting the eligibility criteria. It is anticipated that the provision will apply to a limited number of children and young people. 4. NEXT STEPS
• The Personalisation & Personal Budgets Policy describes the approach between Liverpool City Council and, where applicable, Liverpool CCG to personalisation and personal budgets across education, health and social care. The policy was developed by a multi-disciplinary group during 2014 including representatives from education, social care, health commissioners, school representatives and parents.
Page 4 of 5 969696

• The CCG have engaged the North West Commissioning Support Unit to manage and develop systems and processes around the SEND agenda and personal health budgets in general. The CCG continues to engage with the Council around joint working arrangements to fulfil the requirements of this agenda.
• In addition the draft policy has been reviewed by the CCG legal advisor, Hill Dickinson. Amendments have been incorporated into the policy to reflect their feedback.
• To date there has been limited take up of personal health budgets; nonetheless the CCG will continue to ensure that appropriate arrangements are developed and available as required.
Alison Ormrod Chief Accountant 03.02.15
Page 5 of 5 979797

989898
Personalisation & Personal Budgets Policy Special Educational Needs and Disability (SEND)
1
999999

Version Author Date Description 1.0 Angela Quane 15.07.2014 First draft of policy to reflect new
provisions Children & Families Act 1.1 Andrew Buck 31.07.2014 Second draft following review by
Resources Sub Group of the 0-25 Strategy Group
1.2 Angela Quane 16.08.2014 Third draft following feedback from SEND Commissioner and AD Early Help and further additions/amendments from Angela Quane
1.3 Angela Quane 22.8.2014 Forth draft following further review by Resources Sub Group of the 0-25 Strategy Group and feedback from Liverpool CCG
1.4 Angela Quane 1.9.2014 Fifth draft following review by David Steel, Legal Services and additions to Direct Payments guidance (A Quane)- now includes recruitment of staff and purchasing of services
1.5 Angela Quane 12.9.2014 Sixth draft following review by In Control (charity working with SEND Pathfinders and LAs to implement personal budgets and review by the Disabled Children’s Team Manager
1.6 Angela Quane 20.11.2014 Seventh draft following review by Andrew Laing Solicitor SEN and CCG Legal Advisors Dicks Hill / Alison Ormrod Chief Accountant LCCG / LCC Audit
1.7 Angela Quane 3.11.2014 Eighth draft following amendments by Angela Quane, Andrew Laing Solicitor SEN and Alison Ormrod / Chief Account LCCG
1.8 Angela Quane 5.11.2014 Nineth draft following additions by Angela Quane Finance Manager
1.9 Angela Quane 8.1.2015 Tenth draft following final review by Resources Sub Group of 0-25 Strategy Group
2
100100100

Contents 1. About this Policy 2. Personalisation 3. Personal Budgets 3.1 Requesting a Personal Budget 3.2 A Personal Education Budget 3.3 A Personal Social Care Budget 3.4 A Personal Health Budget
3.5 A system for determining a Personal Budget 3.6 Mechanisms for delivery of a Personal Budget 3.7 Exclusions 3.8 Reviewing a Personal Budget 3.9 Withdrawing or Reducing a Personal Budget 4. Direct Payments 5. Personal Budget Pathway 6. Advice and Guidance 7. Complaints and Appeals Annexe A References
3
101101101
1 About this Policy This document provides details of Liverpool City Council’s and Liverpool Clinical Commissioning Group’s approach to personalisation and personal budgets across education, health and social care. It has been developed by a group including parents, school representatives, health commissioners, social care and education. The designated Lead Professional and/or Plan Co-ordinator will work with families to discuss personalised opportunities and the option of a personal budget and the support available to them to manage a personal budget. 2 Personalisation – the legal framework The Children and Families Act 2014 (“The Act”) reforms the earlier Special Educational Needs (SEN) provisions1. The Government published the Green Paper “Support and Aspiration” (2011), followed by the Children and Families Bill (2013) which received Royal Assent in March 2014 with an implementation date of September 2014. The Act imposes a duty on local authorities to prepare and maintain, where necessary, an Education, Health and Care Plan (“EHC Plan”) for children and young people who have SEN. In addition to the revised legislative framework, the government published a Code of Practice in July 2014 to support the new arrangements: Special educational needs and disability code of practice: 0 to 25 years https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/342440/SEND_Code_of_Practice_approved_by_Parliament_29.07.14.pdf. The Code is statutory guidance for organisations who work with and support children and young people with special educational needs and disabilities. In carrying out their respective functions in relation to children and young people who have SEN, the City Council and Liverpool Clinical Commissioning Group (“Liverpool CCG”) must have regard to the Code of Practice with effect from 1st September 2014. The City Council is required to publish a Local Offer, setting out in one place information about provision they expect to be available across education, health and social care for children and young people in their area who have SEN or are disabled, including those who do not have an EHC Plan.
1 Predominantly laid out within the Education Act 1996
4
102102102

The City Council and the CCG must work together to plan and commission education, health and social care services jointly for children and young people with SEN and disabilities. Personalisation is at the heart of the Special Educational Needs and Disability (“SEND”) reforms and seeks to put children, young people and their families at the centre of the Education, Health and Care planning process. The Act specifies that a young person or their family can request a personal budget or direct payment if they have a qualifying health, social care, or education need; and that they can do so either during the assessment or at the point of review of the EHC Plan. The expectation is on the local authority, health organisations and schools to develop Liverpool’s offer over a period of time as requests for personalised support identify where and how money could be spent differently to achieve agreed outcomes. In Liverpool, we encourage the use of the social model of disability which says that disability is created by barriers in society. The barriers generally fall into 3 categories:
the environment – including inaccessible buildings and services
people’s attitudes – stereotyping, discrimination and prejudice
organisations – inflexible policies, practices and procedures This means we perceive the disability to originate in the environment not the individual’s impairment. The barriers that prevent a ‘normal’ life disable us, not the physical characteristics of the individual. Personal Budgets are just one way in which Liverpool City Council supports children with disability when they have a need for higher levels of support. Set out below is a description of the range of supports that are available across a range of children’s needs. Community Wealth and Social Capital Community wealth or Social Capital is about the support that people can offer each other from outside the traditional statutory services. Communities and groups of people coming together with shared interests to support a family; this can include friends and neighbours as well as wider community networks. All families and communities have ‘real wealth’ and a community can be made up of everyone’s real wealth, all the skills and knowledge, formal and informal networks and the wider society. Social capital can also include volunteering. Universal Services Children and young people can access many activities and services that are available locally to everyone in the community (community groups, leisure, cinemas, schools and their GPs). Universal and Mainstream Services are the first place for children and young people to be with their peers.
5
103103103
Targeted Support Sometimes it is identified that children and young people have additional needs which require some targeted support to help with education and accessing the community. Targeted education support may be delivered in schools and colleges by specialist teachers and care in the home and help with accessing community activities. Where a child may have some health needs they may have support from nurses or other health professionals. Choice and Control The reforms seek to ensure that the child/young person and their family are involved in personalising those additional support needs identified which cannot be met from within the other three areas, and one of the choices could be the option of a personal budget. Personalisation in Liverpool is about:-
• adopting person-centred approaches where children with SEND and their families are put at the centre of processes, enabling them to express their views, wishes and feelings and participate in decision making.
• personalising the support that families receive by working holistically in partnership with services across education, health and social care
• the option of a personal budgets where appropriate, and. • providing advice and support, when families need additional help with
exercising choice and control to meet the agreed outcomes 3 Personal Budgets An EHC Plan is the product of a co-ordinated assessment which specifies the outcomes sought for a child or young person 0-25 years old with SEND across education and, where appropriate, health and social care. A Personal Budget is an allocation of funding identified by the Local Authority (and, if appropriate, the CCG) to provide support to meet all or some of the outcomes identified in an EHC Plan. A Personal Budget will be provided in circumstances where it is assessed that the child or young person is eligible for additional funding and it is agreed that the parent or young person is to be involved in securing that provision, taking into account the legal duties on the City Council and the CCG to ensure that the funding is spent appropriately. The scope of the Personal Budget will vary depending on the needs of the individual and local eligibility criteria, the EHC Plan will clearly state which outcomes can be met by a Personal Budget. Some services cannot be purchased using a Personal Budget and these are discussed in more detail below.
6
104104104
3.1 Requesting a Personal Budget The child’s parent or the young person has the option of requesting a Personal Budget when the local authority has completed an EHC assessment and has confirmed that it will prepare a draft EHC Plan. They also have the option of requesting a Personal Budget during the period of any statutory review of an existing EHC Plan or any re-assessment of the educational, health care and social care needs of a child or young person for whom it maintains an EHC plan. A Personal Budget may consist of elements of funding from education, health and social care. In the main this will be:-
• For education – High Needs Funding (part of element 3 top-up funding) (1) • For children’s social care – Funding for specialist provision as assessed
by the Disabled Children’s Team (DCT): http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/family.page?familychannel=10-5-1
• For adult’s social care – Funding assessed by: http://liverpool.gov.uk/health-and-social-care/adults-and-older-people/fair-access-to-care-services
• For children’s health – Continuing Care (CC) funding http://www.nhs.uk/CarersDirect/guide/practicalsupport/Documents/National-framework-for-continuing-care-england.pdf
• For adult’s health – Continuing Health Care (CHC) funding https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213137/National-Framework-for-NHS-CHC-NHS-FNC-Nov-2012.pdf
3.2 A Personal Education Budget: Children and young people with special educational needs and or a disability will attend a school or college where their needs can usually be met by the resources that the school or college have available as part of their “Local Offer” http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/family.page?familychannel=10-1 However additional funding over and above the school or college place could be made available if an assessment has identified that the learning support needs cannot be met within the school/college place funding; a costed provision map will be submitted by the school/college and used for determining any additional High Needs (element 3) education funding that could be made available. (1) Schools and colleges receive base funding (element 1) for all children and young people to provide a
school place as part of universal services and this funding cannot be used as a personal budget. Schools and colleges also receive an amount of element 2 funding to support children and young people with SEN, this funding is only available as part of a personal budget when the school or college agrees to this. Element 3 top up funding is also used to fund special schools and colleges as part of the core specialist integrated provision (Local Offer) this funding is only available for a personal budget when the school or college agrees to this.
7
105105105
3.3 A Personal Social Care Budget: Funding will be made available if a child or young person has been assessed and is eligible for additional specialist individual support in the home or in the wider community as part of the Care Act 2014 (over 18 years old) or under section 17 of the Children Act 1989 (children 0-18 years old). The assessment information will be used to determine the level of funding available. 3.4 A Personal Health Budget: There will be a small number of children and young people who have complex needs and require support services which cannot be met by universal and targeted health services (all of which are part of the Local Offer). Those children and young people who receive, or are assessed as meeting the eligibility criteria for NHS Continuing Healthcare, (including children's continuing care) have the right to ask for a Personal Health Budget, including a direct payment. From October 2014 this group will benefit from 'a right to have' a Personal Health Budget. The eligibility process for Continuing Care and Continuing Health Care can be accessed through the Local Offer. http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/advice.page?id=T0rp0MDZh40&category=10-4 http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/advice.page?id=OyyZdjuqR7I&category=10-4 The assessment will be used to determine the level of funding available. 3.5 Calculating a Personal Budget The Local Authority and, where appropriate, Liverpool CCG will determine the amount of a Personal Budget to be included within an EHC plan. This will be informed by the provision needed to meet the child or young person’s identified needs. A system is being explored which will help to inform decisions about funding levels for Personal Budgets; this includes the use of a Resource Allocation System (RAS), which will be completed as part of the EHC assessment. The RAS will provide indicative levels of resources required to help in the planning of support outcomes in education, health and social care. This is a complex area and any system requires rigorous testing before it can be adopted to ensure that it is fit for purpose. 3.6 Mechanisms for delivery of a Personal Budget Personal Budgets can be offered in a number of different ways:-
• Direct payments - where individuals receive the cash to contract, purchase and manage services themselves (1)
• An organised arrangement (sometimes referred to as a notional budget) where Liverpool City Council, Liverpool CCG, or the school or college holds the funding and commissions the support
8
106106106
• Third party arrangements/nominees – where funds (direct payments) are paid to and managed by an individual or another organisation on behalf of the parent/young person
• A combination of the above
(1) A personal budget and in particular a direct payment cannot be made in respect of provision which will take place in a school, post 16 institution or early years setting (maintained schools and maintained nursery schools, early years providers, further education institutions or the proprietor of academies as well as non-maintained and independent special schools and colleges) without the written consent of the head teacher, principal or the person occupying an equivalent position.
Local authorities and, where appropriate, CCGs must consider each request for a Personal Budget on its own individual merits. If a local authority and/or a CCG are unable to identify a sum of money, they should inform the child's parent or young person of the reasons. For example, the local authority might agree that the provision in respect of which a Personal Budget has been requested by the young person or their family is needed but may be unable, at that point in time, to disaggregate funding that is currently supporting provision of services to a number of children and young people. In these circumstances, the local authority may refuse to prepare a Personal Budget on the basis that doing so would have an adverse impact on the services which it provides or arranges for children and young people with an EHC Plan or would not be an efficient use of its resources.2 Where the child or young person’s EHC Plan includes healthcare provision, the CCG may consider a Personal Budget to be an impracticable or inappropriate way of securing the specified provision. This could be due to the specialised clinical care required or because a Personal Health Budget would not represent value for money as any additional benefits to the child or young person would not outweigh the extra cost to the NHS. Again, this might include cases where the CCG is unable, at that point in time, to disaggregate funding that is currently supporting provision of healthcare services to a number of children and young people. The funding currently available for Personal Budgets will reflect local circumstances, commissioning arrangements and the school/college preference. The scope of Personal Budgets should increase over time as local joint commissioning arrangements between Liverpool City Council and Liverpool CCG provide greater opportunity for choice and control over local provision (Code of Practice 9.110). 3.7 Exclusions Personal Budgets will not be appropriate for all aspects of Education, Health or Care, for example, those Universal Services that are available to all children/young people are exempt, such as a school place or Post 16 institution (element 1 base funding) and primary medical services provided by GPs.
2 Regulation 4A of the Special Educational Needs (Personal Budgets) Regulations 2014.
9
107107107
Looked After Children placements are not available as a Personal Budget. Where provision is already available through a block contract it is unlikely that that a direct payment (as part of a Personal Budget) would be available to access alternative services as this would be determined to be double funding and therefore an inefficient use of resources. This will, however, change over time as parents and young people inform future commissioning of new services. Using a direct payment to employ a family member who lives in the same household will not be possible except in very exceptional circumstances. 3.8 Reviewing a Personal Budget It is essential to check at appropriate intervals how a Personal Budget is working, and, whether the EHC Plan is achieving the agreed outcomes. It is also important that Personal Budget holders know who to contact to discuss changes to their Personal Budget should their needs change. To this end, the local authority and, where appropriate, the CCG will periodically audit and review the use of a Personal Budget, normally at the point at which the local authority carries out its annual review of the child or young person’s EHC Plan. Depending on the outcome of the audit / review, changes can be made to the resources, support or controls described in the EHC Plan. The ultimate aim of the audit / review is to strengthen the person’s ability to achieve the outcomes they want in a timely fashion. Where some or all of a Personal Budget is made available by way of direct payments, this arrangement, too, will be periodically audited and reviewed by the local authority and, where appropriate, the CCG. Further information on this process can be found in the separate document, ‘A Guide to Direct Payments’. 3.9 Withdrawing or reducing a Personal Budget Before making a decision to withdraw or reduce a Personal Budget, wherever possible, Liverpool City Council and, where appropriate, Liverpool CCG will consult all relevant parties as well as the family or young person. Whenever a Personal Budget is withdrawn or reduced, Liverpool City Council, and where appropriate, Liverpool CCG will ensure that the person is given written notice of the reasons for the decision. 4 Direct Payments Liverpool City Council and, where appropriate, Liverpool CCG will only agree to make direct payments in respect of educational, social care and/or healthcare provision where a valid request has been made for a Personal Budget, including a request for direct payments, and they are satisfied that:
• the person receiving the direct payments will act in the best interests of the child or young person when securing the agreed provision
• and, they will use them in the appropriate way
10
108108108
. Direct Payments are discussed in more detail in the separate document, ‘A Guide to Direct Payments’. Liverpool City Council and, where appropriate, Liverpool CCG will have regard to the following regulations in relation to all requests for Direct Payments: The Community Care, services for Carers and Children’s Services (Direct Payments) (England) Regulations 2009 The National Health Service (Direct Payments) Regulations 2013 (as amended by the National Health Service (Direct Payments) (Amendment) Regulations 2013) The Special Educational Needs (Personal Budgets) Regulations 2014 (as amended by the Special Educational Needs (Miscellaneous Amendments) Regulations 2014)
11
109109109
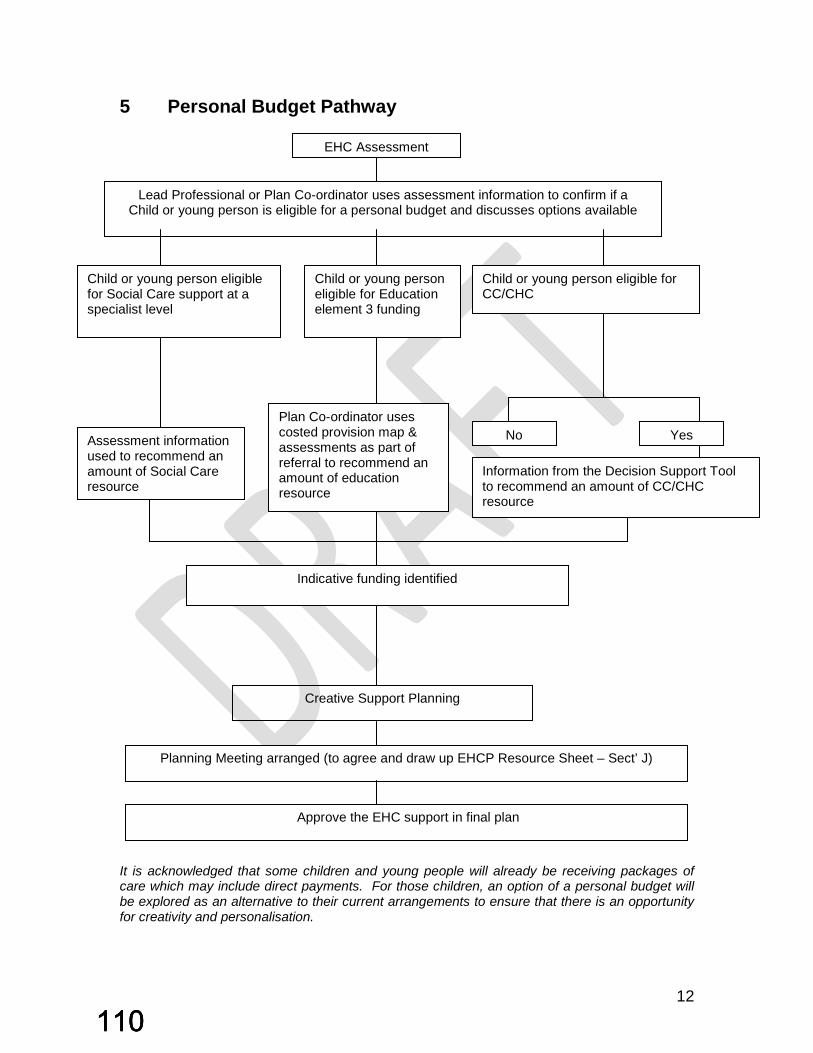
5 Personal Budget Pathway It is acknowledged that some children and young people will already be receiving packages of care which may include direct payments. For those children, an option of a personal budget will be explored as an alternative to their current arrangements to ensure that there is an opportunity for creativity and personalisation.
EHC Assessment
Child or young person eligible for Social Care support at a specialist level
Child or young person eligible for CC/CHC
Information from the Decision Support Tool to recommend an amount of CC/CHC resource
Assessment information used to recommend an amount of Social Care resource
Indicative funding identified
Planning Meeting arranged (to agree and draw up EHCP Resource Sheet – Sect’ J)
No Yes
Approve the EHC support in final plan
Lead Professional or Plan Co-ordinator uses assessment information to confirm if a Child or young person is eligible for a personal budget and discusses options available
Child or young person eligible for Education element 3 funding
Plan Co-ordinator uses costed provision map & assessments as part of referral to recommend an amount of education resource
Creative Support Planning
12
110110110
6 Information, Advice and Support The Plan Co-ordinator or the Lead Professional will have a detailed discussion with the family to discuss if they would like to explore the option of a personal budget and they will provide advice on the process. In addition advice will be available from Parent Partnership http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/service.page?id=mj3W9YG68yM&familychannel=10-9-5 and Liverpool’s Independent Supporters http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/service.page?id=E34wpiaJoU4&familychannel=10-9-5 7 Complaints and Appeals An appeal can occur under the following circumstances:
• An aspect of provision listed in the Education, Health and Care Plan has not been offered in a Personal Budget, which is requested by the parent or young person;
• A Personal Budget has not been offered or the request has been refused; • The amount of the Personal Budget is felt not to be sufficient to meet the
needs of the young person. An appeal would in the first instance be dealt with through the Disagreement Resolution procedures http://fsd.liverpool.gov.uk/kb5/liverpool/fsd/advice.page?id=gzJom0NmGrI&familychannel=10-9 http://liverpool.gov.uk/council/complaints-and-feedback/make-a-complaint-about-a-council-service/ https://www.gov.uk/special-educational-needs-disability-tribunal/overview http://www.liverpoolccg.nhs.uk/Contact_Us/Complaints_and_Comments.aspx http://www.ombudsman.org.uk/make-a-complaint/complaints-about-continuing-healthcare-funding
13
111111111
Annexe A References Special Educational Needs and Disability Code of Practice: 0 to 25 years July 2014 The Community Care, services for Carers and Children’s Services (Direct Payments) (England) Regulations 2009 The National Health Service (Direct Payments) Regulations 2013 (as amended by the National Health Service (Direct Payments) (Amendment) Regulations 2013) The Special Educational Needs (Personal Budgets) Regulations 2014 (as amended by the Special Educational Needs (Miscellaneous Amendments) Regulations 2014)
14
112112112

Report no: GB 16-15
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP
GOVERNING BODY
TUESDAY 10TH FEBRUARY 2015
Title of Report CCG Corporate Performance report
Lead Governor Dr Nadim Fazlani
Senior Management Team Lead
Ian Davies, Head of Operations & Corporate Performance
Report Author
Stephen Hendry, Senior Corporate Services Manager (Performance & Operations)
Summary The purpose of this paper is to report to the Governing Body key aspects of the CCG’s performance in delivery of quality, performance and financial targets for 2014/15.
Recommendation That Liverpool CCG Governing Body: Notes the performance of the CCG in delivery
of key national performance indicators and the recovery actions taken to improve performance
Impact on improving health outcomes, reducing inequalities and promoting financial sustainability
The report provides evidence of the progress being made across the organisation at both an organisational and individual service provider level.
Relevant Standards or targets
Everyone Counts: Planning for Patients 2014/15
Page 1 of 41
113113113

LIVERPOOL CCG PERFORMANCE REPORT 1. PURPOSE The purpose of this paper is to report to the Governing Body key aspects of the CCG’s performance in delivery of quality, performance and financial targets for the year 2014/15. 2. RECOMMENDATIONS That Liverpool CCG Governing Body: Notes the performance of the CCG in delivery of key national performance
indicators and the recovery actions taken to improve performance, if required. 3. BACKGROUND The CCG is held to account by NHS England for corporate performance against delivery of key indicators within the CCG Outcome Indicator Set of the NHS Outcomes Framework 2014/15 and operational standards expected from the NHS Constitution. In addition, the CCG has to be assured that the services we commission are delivering the required quality standards and that any risks and issues relating to service quality and patient safety are identified and positive action taken to rectify. The CCG has established robust governance processes and committee structures in order to monitor performance and provide assurance to the Governing Body that key risks to the organisation are being identified and effectively managed. For example, the Quality, Safety and Outcomes Committee has responsibility for quality and performance issues within its commissioned services, whereas the Finance, Procurement and Contracting Committee has responsibility for financial monitoring and contract activity. Whilst the February 2015 Performance Report provides a summary of CCG performance in relation to the NHS Outcomes Framework/Everyone Counts (which has been the primary focus of previous reports) the revised format allows for performance analysis against key Public Health/local outcomes; providing the Governing Body with a much more integrated report structure which maps progress against statutory
Page 2 of 41
114114114
reporting requirements and measurement across the priority programme areas of Mental Health; Healthy Ageing; Long Term Conditions; Children; Learning Disabilities and Cancer. Due to the way in which these indicators are measured, the majority of these elements will be reported upon on a quarterly and annual basis. The quality and accuracy of some data flows continue to present issues for the CCG, although it should be emphasised that any specific problem areas are generally dealt with swiftly between NHS Liverpool CCG and North West Commissioning Support Unit (NWCSU). The report is based on the published and validated data available as at 31st January 2015. As a consequence of the timing of submissions to meet NHS Liverpool CCG’s governance reporting and data schedules, this report updates the Governing Body with a combination of data up to the end of November and/or December 2014. 4. NATIONAL PERFORMANCE MEASURES NHS Liverpool CCG is committed to ensuring that patient rights under the NHS Constitution are consistently upheld. National Performance Measures are reflective of the key priority areas detailed in Everyone Counts: Planning for Patients 2014/15 and encompass measurements against Quality (including Safety, Effectiveness and Patient Experience) and Resources (including Finance, Capability and Capacity). In addition to analysing local performance against these indicators, CCGs are expected to achieve improvements against indicators across the five domains detailed in the NHS Outcomes Framework 2014/15 and the high-level national outcomes the NHS is expected to be aiming to improve. Headline commentary is provided below to draw the Governing Body’s attention to specific areas of performance which represent risks to delivery, and to the relevant assurances on internal control measures in place to mitigate those risks.
Page 3 of 41
115115115

4.1 NHS Constitution – Access & Waiting 4.1.1 Good Performance
Indicator Narrative Ambulance Response Times. GREEN (with alert)
Cumulatively up to the end of December 2014 the CCG met all targets relating to ambulance calls (Cat A Red 1, Red 2 and Red Category 19). However, at Trust level the Ambulance Service has not achieved any of these targets with ‘Red 1’ recording 69.99% against a plan of 75%; ‘Red 2’ performance at 70.8% against a target of 75% and ‘Category 19’ marginally failing to meet the target of 95% at 93.8%, little changed from the previous month. Trust performance continues to be significantly challenged at a North West and in part at a Merseyside level.
Assurance on CCG control measures The Ambulance Service has continued to experience a sustained and unparalleled volume of emergency ‘999’ calls during December 2014, which is reflective of the system pressures prevalent in the wider health economy during the same period. Inevitably, these winter pressures have impacted quite severely on response times and continue to delay responses to less urgent calls. Commissioners continue to work with the Trust and the impact of the current demand. The latest data highlights that during December 2015, the service responded to 95,063 incidents across the North West, an increase in Red activity of 19.8% per cent.
Page 4 of 41
116116116
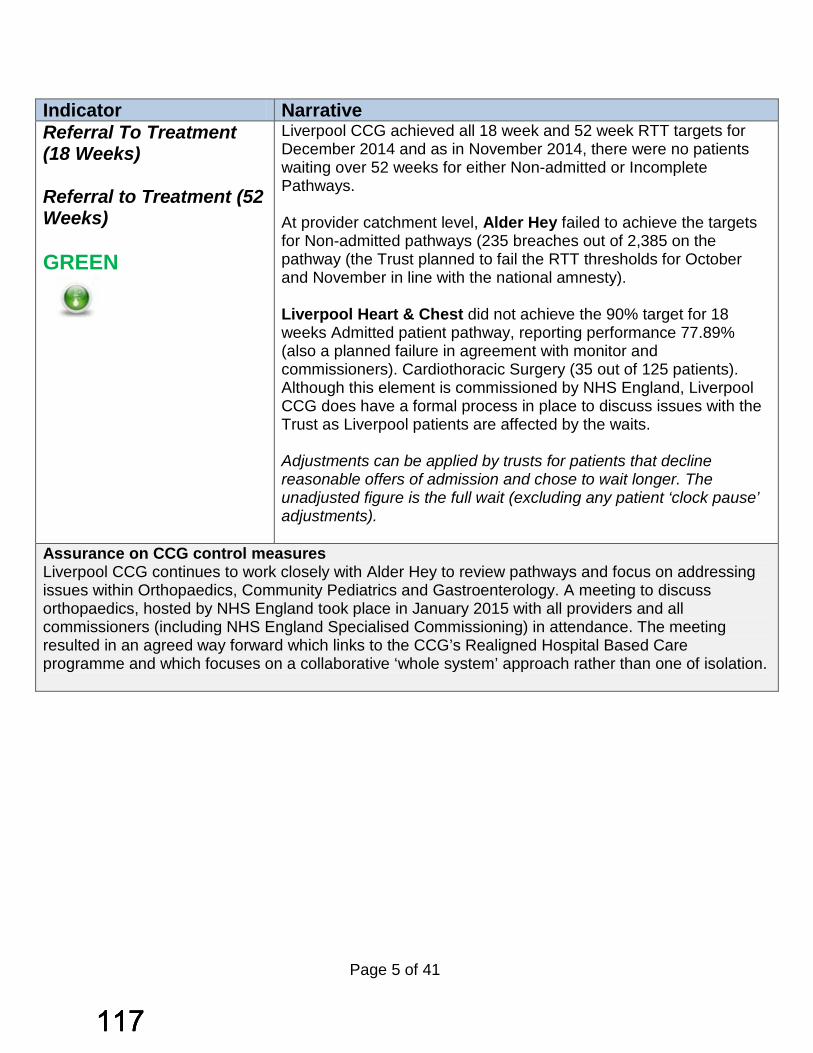
Indicator Narrative Referral To Treatment (18 Weeks) Referral to Treatment (52 Weeks) GREEN
Liverpool CCG achieved all 18 week and 52 week RTT targets for December 2014 and as in November 2014, there were no patients waiting over 52 weeks for either Non-admitted or Incomplete Pathways. At provider catchment level, Alder Hey failed to achieve the targets for Non-admitted pathways (235 breaches out of 2,385 on the pathway (the Trust planned to fail the RTT thresholds for October and November in line with the national amnesty). Liverpool Heart & Chest did not achieve the 90% target for 18 weeks Admitted patient pathway, reporting performance 77.89% (also a planned failure in agreement with monitor and commissioners). Cardiothoracic Surgery (35 out of 125 patients). Although this element is commissioned by NHS England, Liverpool CCG does have a formal process in place to discuss issues with the Trust as Liverpool patients are affected by the waits. Adjustments can be applied by trusts for patients that decline reasonable offers of admission and chose to wait longer. The unadjusted figure is the full wait (excluding any patient ‘clock pause’ adjustments).
Assurance on CCG control measures Liverpool CCG continues to work closely with Alder Hey to review pathways and focus on addressing issues within Orthopaedics, Community Pediatrics and Gastroenterology. A meeting to discuss orthopaedics, hosted by NHS England took place in January 2015 with all providers and all commissioners (including NHS England Specialised Commissioning) in attendance. The meeting resulted in an agreed way forward which links to the CCG’s Realigned Hospital Based Care programme and which focuses on a collaborative ‘whole system’ approach rather than one of isolation.
Page 5 of 41
117117117
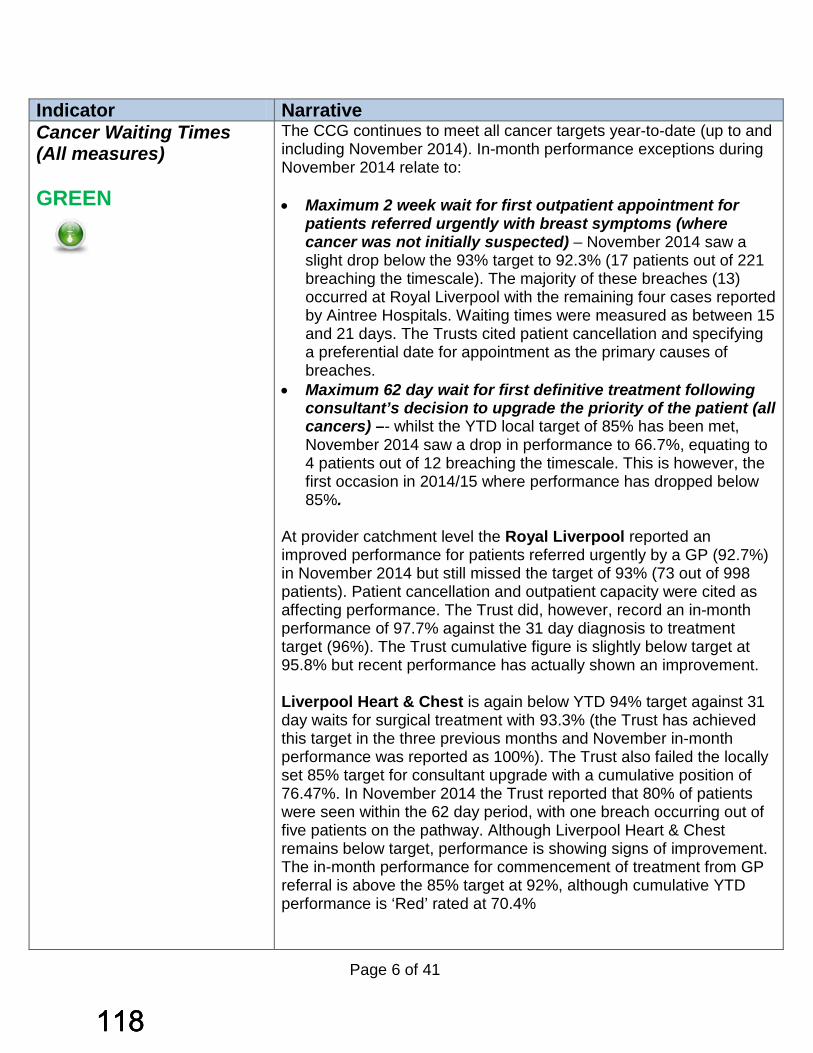
Indicator Narrative Cancer Waiting Times (All measures) GREEN
The CCG continues to meet all cancer targets year-to-date (up to and including November 2014). In-month performance exceptions during November 2014 relate to: • Maximum 2 week wait for first outpatient appointment for
patients referred urgently with breast symptoms (where cancer was not initially suspected) – November 2014 saw a slight drop below the 93% target to 92.3% (17 patients out of 221 breaching the timescale). The majority of these breaches (13) occurred at Royal Liverpool with the remaining four cases reported by Aintree Hospitals. Waiting times were measured as between 15 and 21 days. The Trusts cited patient cancellation and specifying a preferential date for appointment as the primary causes of breaches.
• Maximum 62 day wait for first definitive treatment following consultant’s decision to upgrade the priority of the patient (all cancers) –- whilst the YTD local target of 85% has been met, November 2014 saw a drop in performance to 66.7%, equating to 4 patients out of 12 breaching the timescale. This is however, the first occasion in 2014/15 where performance has dropped below 85%.
At provider catchment level the Royal Liverpool reported an improved performance for patients referred urgently by a GP (92.7%) in November 2014 but still missed the target of 93% (73 out of 998 patients). Patient cancellation and outpatient capacity were cited as affecting performance. The Trust did, however, record an in-month performance of 97.7% against the 31 day diagnosis to treatment target (96%). The Trust cumulative figure is slightly below target at 95.8% but recent performance has actually shown an improvement. Liverpool Heart & Chest is again below YTD 94% target against 31 day waits for surgical treatment with 93.3% (the Trust has achieved this target in the three previous months and November in-month performance was reported as 100%). The Trust also failed the locally set 85% target for consultant upgrade with a cumulative position of 76.47%. In November 2014 the Trust reported that 80% of patients were seen within the 62 day period, with one breach occurring out of five patients on the pathway. Although Liverpool Heart & Chest remains below target, performance is showing signs of improvement. The in-month performance for commencement of treatment from GP referral is above the 85% target at 92%, although cumulative YTD performance is ‘Red’ rated at 70.4%
Page 6 of 41
118118118

Indicator Narrative Cancer Waiting Times (all measures, continued from page 5) GREEN
Aintree Hospitals recorded a measure of 86.8% YTD against a plan of 90% for 62 Day Waits for referral to treatment from a screening service. The Trust also under-performed for November 2014, achieving 75% (1.5 patients breaching out of 6). The Trust has cited patient choice as influencing performance in this area; particularly in the early (pre-diagnosis phase).
Assurance on CCG control measures Whilst the CCG has achieved all cancer targets, provider performance against specific measures at a local level highlights some challenges. For the Royal Liverpool, 2 week wait performance in November 2014 is reflective of the recovery from the previously reported Dermatology issues (peak of referrals in July 2014, reduced capacity due to sickness and vacancies), whilst Liverpool Heart & Chest continues to be affected by delayed referral processes for consultant upgrades. However, in-month performance for both Trusts evidences an improvement which will continue to be monitored via established CCG contract, quality and transformational change mechanisms.
Page 7 of 41
119119119
4.1.2 Areas for improvement
Indicator Narrative Diagnostics - Percentage of Patients waiting for more than 6 weeks for a diagnostic test. RED
The CCG failed to remain below the 1% threshold in December 2014, achieving 1.41%. This equates to 82 patients out of 5,808 waiting for more than 6 weeks for a diagnostic test and is largely driven by performance at Aintree Hospital (4.08%) and Alder Hey (3.5%). In the case of Aintree, the 4.08% equated to 67 patients out of 1,642 waiting in excess of 6 weeks; the majority of breaches (47) occurred in Cardiology (ECG) and were attributed to significant staff sickness. Alder Hey’s performance of 3.45% equates to 4 patients out of 116 waiting for more than 6 weeks; all 4 cases concerned waits for magnetic resonance imaging with waiting times reported as being 6-7 weeks.
Assurance on CCG control measures Provider performance against this measure continues to be closely monitored at CCG level. The contract query in place for LCH in relation to this standard has now been lifted as the Trust has achieved a sustained level of performance below 1% for three consecutive months. South Sefton CCG has been in discussions with Aintree Hospitals in relation to December 2014 performance against this measure and any resulting actions agreed will be in the March 2015 Performance Report.
Page 8 of 41
120120120
Indicator Narrative A&E Waits - % of patients who spend 4 hours or less in A&E (cumulative) 95% threshold AMBER
The CCG failed to achieve the 95% target both in-month (December 2014 – 89.73%) and Year to Date (94.07%). Performance has also dropped from November 2014. The CCG is yet to achieve the 95% cumulatively in 2014/15 (although this was achieved in individual months, namely August and September 2014). The Royal Liverpool failed the Year to Date up to December 2014 recording 93.66% and has not seen a further deterioration of in-month performance at 88.7%. Assuming the Trust continues activity at the current weekly rate there is a significant risk of non-achievement at year end. Aintree Hospitals A&E in-month performance for December 2014 has decreased to the lowest in the financial year at 86.87%. The Trust has failed to achieve the target in any month in 2014/15 with Year to Date performance at 90.98%. Given the current trajectory it is now highly likely that Aintree will fail the year end four hour operating standard. Quarter 3 performance for Type 1 and Type 2 attendances was 88%; failing the 90% target agreed with Monitor. The causes continue to be multi-faceted with flow into the assessment areas and throughput to wards affected by delayed discharges and capacity.
Assurance on CCG control measures The CCG continues to work closely with both Trusts through the System Resilience Group. Contract queries remain in place for both the Royal Liverpool and Aintree whilst active remedial action plans are closely monitored to address the required improvements in performance. For the Royal Liverpool, the most significant development to date is the running of a scaled down version of ‘Operation Fresh Start’ during the week commencing 26th January 2015 (this was previously run in November 2013). Key changes to the working week during the initial exercise included daily board rounds and daily consultant start times of 08:00hrs. The success of this initiative during 2013 was evident by performance above 95% on a daily basis. Aintree Hospital’s action plan demonstrated progress in key areas, but overall this is not providing sufficient evidential assurances of improvement against the operating standard. External factors are influencing the challenges the Trust faces such as access to Intermediate Care Level 1 beds and extensive assessment processes. Delayed transfers of care remain fairly high and are arising frequently due to issues such as patient choice. A Merseyside-wide NHS Patient Choice & Transfer of Care policy has recently been circulated to all Trusts for dissemination and integration into internal governance processes.
Page 9 of 41
121121121

4.2 NHS Outcomes Framework - Helping People to Recover from Episodes of Ill Health or following Injury 4.2.1 Good Performance Indicator Narrative TIA – % patients assessed and treated within 24 hours (Target 60%) GREEN
The CCG has exceeded the performance target for TIA with an achievement of 92% for December 2014. Although this represents a decrease in performance compared to 95.65% reported for November 2014, the CCG has maintained its ‘Green’ rating against this important measure.
4.2.2 Areas for improvement Indicator Narrative Stroke – (% of patients spend at least 90% of their time on a Stroke Unit (Target 80%) RED
Performance against the 80% target has further deteriorated since November 2014 with 68.9% of patients spending at least 90% of their time on a stroke ward in the month of December 2014. Performance in December 2014 is affected by Aintree Hospital’s failure to meet the target at 66.6% (Red) which represents a deterioration from November and the Royal Liverpool’s under-performance of 75.80%.
Assurance on CCG control measures Performance against this standard is discussed at individual provider Contract/Clinical Quality & Performance Group meetings. In addition, the CCG’s Long Term Conditions Group has responsibility for transformation of the stroke pathway and continues to hold joint meetings with providers to facilitate collaborative working; particularly between the Royal Liverpool and Aintree. Analysis of length of stay has revealed that this is significantly higher in Aintree than the Royal; consequently affecting capacity and accommodation of stroke patients in the specialised Stroke Ward. The Royal Liverpool has also targeted length of stay ahead of the new hospital build and has shared its’ discharge policy with Aintree as part of the improved collaborative working arrangements between the two Trusts.
Page 10 of 41
122122122

4.3 NHS Outcomes Framework – Enhancing Quality of Life for People with Long Term Conditions 4.3.1 Areas for Improvement Indicator Narrative Mental Health Measure - % of patients on Care Programme Approach (target 90%) RED
Liverpool CCG performance against this measure has dropped from 97.87% in November 2014 with 92.31% of Mersey Care patients reported as being on a CPA as at December 2014. This equates to 6 out of 72 patients not on a CPA at CCG level. At Trust level performance was reported as 91.26%, equating to 9 out of 103 patients not on a CPA.
Assurance on CCG control measures Whilst this can be considered as an exception to an otherwise continuous achievement of performance, a small number of breaches have occurred which were attributed to a combination of data quality issues (which have since been resolved although the Trust has been unable to evidence this in December 2014 data). A new reporting mechanism with greater input from services has been implemented for January 2015, which is expected to enable a more detailed commentary on breaches for analysis by commissioners. 4.4 NHS Outcomes Framework - Ensuring People Have a Positive Experience of Care 4.4.1 Areas for Improvement Indicator Narrative Mixed Sex Accommodation – zero tolerance of breaches RED
One Mixed Sex Accommodation breach relating to a Liverpool CCG patient was reported in December 2014 by the Royal Liverpool; continuing the trend of a breach occurring every month in 2014/15 and brining the YTD total to 28. The Royal Liverpool has accounted for 27 of the 28 breaches reported in the financial year
Assurance on CCG control measures Although the two units in the Royal Liverpool at the centre of the reported breaches since April 2014 were relocated on 12th December 2014, the breaches in-month have been attributed to the time that patients in critical care are deemed ‘fit for transfer’ to another ward but are subject to bed availability; a lack of appropriate sleeping accommodation for these patients has been a significant factor. The CCG continues to apply appropriate contract sanctions for breaches and will ensure that robust monitoring is maintained in regard to the ward relocations. These breaches were discussed at the Royal Liverpool CQPG meeting on 23rd Jan 2015.
Page 11 of 41
123123123

4.5 Quality Premium – National Indicators (Health Care Acquired Infection) 4.5.1 Areas for Improvement Indicator Narrative Incidence of Healthcare Acquired Infections – MRSA (Plan tolerance of 0) RED
The CCG has recorded four new cases of MRSA in December 2014; bringing the year to date total to 9 (the CCG is measured against a zero plan for the year). The cases in December consisted of two acute - one at the Royal Liverpool and one at Aintree Hospital and two community-attributed (Royal Liverpool and Liverpool Heart and Chest).
Assurance on CCG control measures Each MRSA case reported is subject to robust Post Infection Review (PIR) processes with appropriate remedial action plans put in place to address any gaps in quality or safety and prevent recurrences.
Indicator Narrative Incidence of Healthcare Acquired Infections – C.difficile (Monthly plan tolerance of 13) AMBER
The CCG has recorded 10 new cases of C.diff during December 2014, which is below the monthly plan of 13. For the year to date a total of 122 cases have been reported, exceeding the plan of 119. Of the 10 cases reported in-month three were acute acquired with the remaining 7 attributed to the community setting. The Royal Liverpool and Aintree Hospital each reported 5 cases relating to Liverpool CCG patients; The Royal Liverpool had one acute case and four community, whilst Aintree reported a split of two acute and three community acquired. Over the course of the financial year the proportionate split of cases are 54 acute and 68. The majority of cases have occurred at the Royal Liverpool (69)
Assurance on CCG control measures Liverpool CCG continues to hold C.Difficile appeals panels to review any cases where the Trust concerned considers there to be no ‘lapse in care’ episodes. Each of the providers has submitted all documentation pertinent to C.diff cases for YTD review (as per NHS England 2014 guidance). Liverpool CCG also continues to support South Sefton CCG in relation to cases submitted by Aintree. The Royal Liverpool is currently reviewing all cases where ‘no evidence of lapses of care’ which have been submitted for consideration at panel. The Trust has a comprehensive action plan in place for Health Care Acquired Infections, which includes a ‘deep dive’ into specific, high-risk areas and urgently conducted surveillance.
Page 12 of 41
124124124
4.6 NHS Outcomes Framework - Treating and Caring for People in a Safe Environment 4.6.1 Good Performance Indicator Narrative Serious Incidents – reporting within 48 hours (national target) The 48 hour national timescale is in place to ensure that providers of healthcare services alert commissioners to each event where a patient has suffered significant harm or death as a result of their care. The early detection and reporting of Serious Incidents is essential for both providers and commissioners in order to agree immediate actions to prevent further harm occurring. GREEN
In December 2014 there were 32 Serious Incidents (SIs) assigned to Liverpool CCG patients from providers (year-to-date total of 223). Of the 32 incidents in December 2014, 24 were reported on the Strategic Executive Information System (StEIS) within the national 48hr timescale. Provider level data is as follows: • The Royal Liverpool had four SIs during December
2014 with three reported within the 48hr timescale. YTD incidents for the Trust total 43;
• Alder Hey reported two SIs; both within 48hrs and therefore achieving 100% compliance for December. YTD incidents for the Trust total 33;
• Liverpool Women’s reported one SI which was within the national timescale; YTD SIs reported total 19;
• Liverpool Community Health reported 20 SIs in December 2014; 13 of which were within the 48hr timescale achieving 65% compliance (rated as ‘Amber’). YTD incidents reported by the Trust total 191;
• Mersey Care also achieved 100% compliance reporting five SIs in December 2014 all within the 48hr timescale. YTD incidents for the Trust total 61;
• Liverpool Heart & Chest reported 0 incidents in-month; YTD incidents total 5;
• Spire Hospital reported 0 incidents in December 2014. YTD total incidents is one.
Assurance on CCG control measures This new indicator is being introduced to provide the Governing Body with an assurance that all Serious Incidents are properly reported within timescales and investigated. All providers with whom Liverpool CCG commissions healthcare are robustly monitored via internal governance arrangements (primarily the Quality, Safety & Outcomes Committee).
Page 13 of 41
125125125

Indicator Narrative Serious Incidents –Submission of investigation reports within 45 days (national timescale) The 45 day national timescale is in place to ensure that providers of healthcare services conduct timely and thorough Root Cause Analysis (RCA) investigations into Serious Incidents. Within this standard is the requirement for providers to submit outcomes-based action plans to improve the quality and safety of services and to limit or eliminate recurrences of incidents. Where extensions of time have been agreed with the provider the new deadline is used as the performance measure. GREEN
A total of 40 Root Cause Analysis (RCA) reports were due for submission during the month of November 2014, 24 of which were submitted within the 45 day timescale with one extension of time granted. The Royal Liverpool submitted 4/4 RCA reports within the national timescale, achieving 100% compliance against the standard; Liverpool Women’s submitted 2/2 RCA reports within the 45 day timescale, achieving 100% compliance; Mersey Care achieved 100% compliance submitting 11 reports within the timescale and agreeing two extension of time (requests for extensions of time are also performance monitored in terms of the timing of the request and submission of the RCA against the revised timescale); Liverpool Community Health submitted 17 RCA reports out of 21 due within the 45 day timescale (Amber rating); All providers were rated as ‘Green’ for the completion of remedial improvement actions in relation to SIs for December 2014 (‘Significant’ Assurance Rating).
Assurance on CCG control measures The CCG has established robust internal performance management arrangements and clinically-led assurance systems of all Root Cause Analysis reports received for co-ordinating commissioner review. Incidents are not authorised to be ‘closed’ unless the report complies with a nationally recognised checklist and all improvement actions are completed and signed off by the relevant organisation. Joint working arrangements with CCG colleagues across Merseyside are also in place where patient flow crosses geographical and organisational boundaries.
Page 14 of 41
126126126
4.6.2 Areas for Improvement Indicator Narrative Never Events (Plan of Zero) RED
Although zero Never Events were reported during the month of December 2014 the CCG is still rated as ‘Red’ as a total of 11 Never Events have been reported year to date against a plan of zero. The breakdown of Never Events by provider for the year 2014/15 is as follows:
• Royal Liverpool – 3; • Alder Hey – 2; • Liverpool Women’s – 0; • Liverpool Heart & Chest – 2; • Mersey Care 0; • Liverpool Community Health – 4; • Spire Hospitals – 0; • Inclusion Matters (IAPT) - 0.
Assurance on CCG control measures Liverpool CCG has requested that providers who report Never Events triangulate each incident where there is evidence of non-compliance of the WHO checklist. The CCG meets with providers on a monthly basis to discuss all Serious Incidents/Never Events and the organisational learning resulting from their Root Cause Analysis. 5. INTEGRATED PERFORMANCE OUTCOMES INDICATORS Integrated CCG Outcomes Indicators have been developed from NHS Outcomes Framework and Public Health indicators and are intended to provide clear and comparative information on progress against local priorities for quality improvement and to demonstrate where the CCG is achieving gains in health outcomes for the population of Liverpool. Where possible, Liverpool is benchmarked against other ‘Core City’ CCGs and ranked against relevant NHS Outcome ambitions. The ‘Joint Performance Report Dashboard’ is included as Appendix 5 and summarises all relevant indicators in this area. It should be noted that this section of the performance report remains somewhat under development and will be further refined over the remainder of the financial year.
Page 15 of 41
127127127
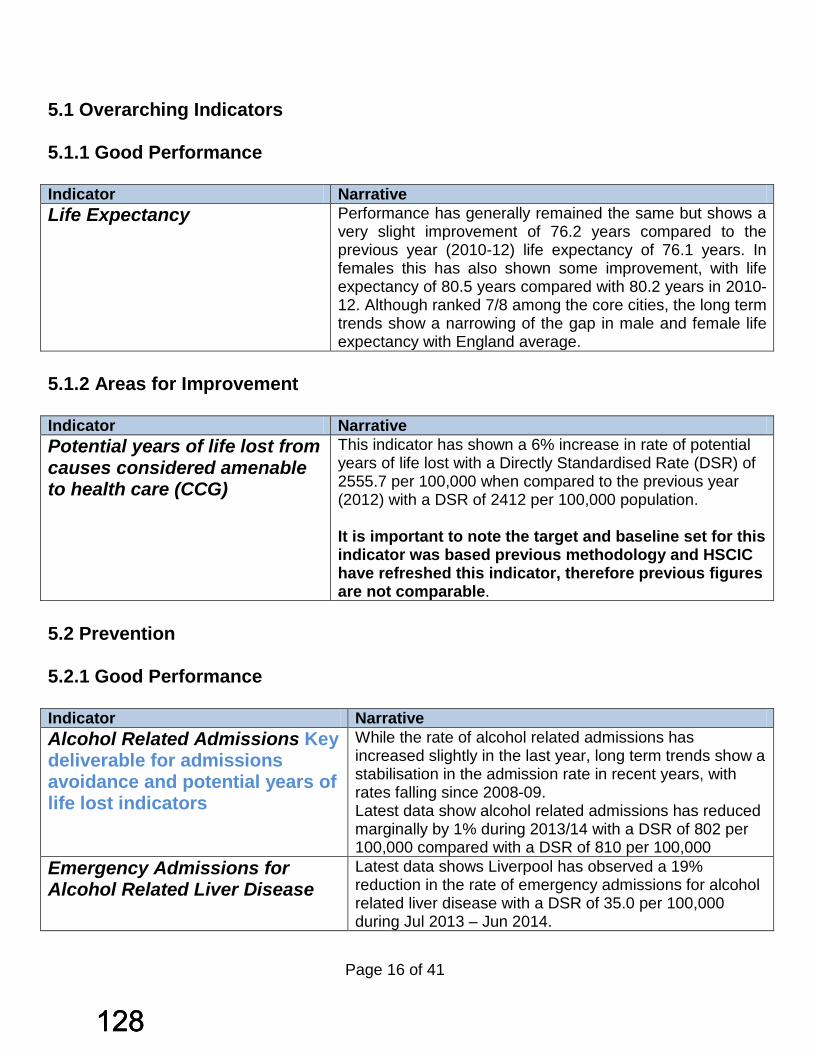
5.1 Overarching Indicators 5.1.1 Good Performance Indicator Narrative Life Expectancy Performance has generally remained the same but shows a
very slight improvement of 76.2 years compared to the previous year (2010-12) life expectancy of 76.1 years. In females this has also shown some improvement, with life expectancy of 80.5 years compared with 80.2 years in 2010-12. Although ranked 7/8 among the core cities, the long term trends show a narrowing of the gap in male and female life expectancy with England average.
5.1.2 Areas for Improvement Indicator Narrative Potential years of life lost from causes considered amenable to health care (CCG)
This indicator has shown a 6% increase in rate of potential years of life lost with a Directly Standardised Rate (DSR) of 2555.7 per 100,000 when compared to the previous year (2012) with a DSR of 2412 per 100,000 population. It is important to note the target and baseline set for this indicator was based previous methodology and HSCIC have refreshed this indicator, therefore previous figures are not comparable.
5.2 Prevention 5.2.1 Good Performance Indicator Narrative Alcohol Related Admissions Key deliverable for admissions avoidance and potential years of life lost indicators
While the rate of alcohol related admissions has increased slightly in the last year, long term trends show a stabilisation in the admission rate in recent years, with rates falling since 2008-09. Latest data show alcohol related admissions has reduced marginally by 1% during 2013/14 with a DSR of 802 per 100,000 compared with a DSR of 810 per 100,000
Emergency Admissions for Alcohol Related Liver Disease
Latest data shows Liverpool has observed a 19% reduction in the rate of emergency admissions for alcohol related liver disease with a DSR of 35.0 per 100,000 during Jul 2013 – Jun 2014.
Page 16 of 41
128128128
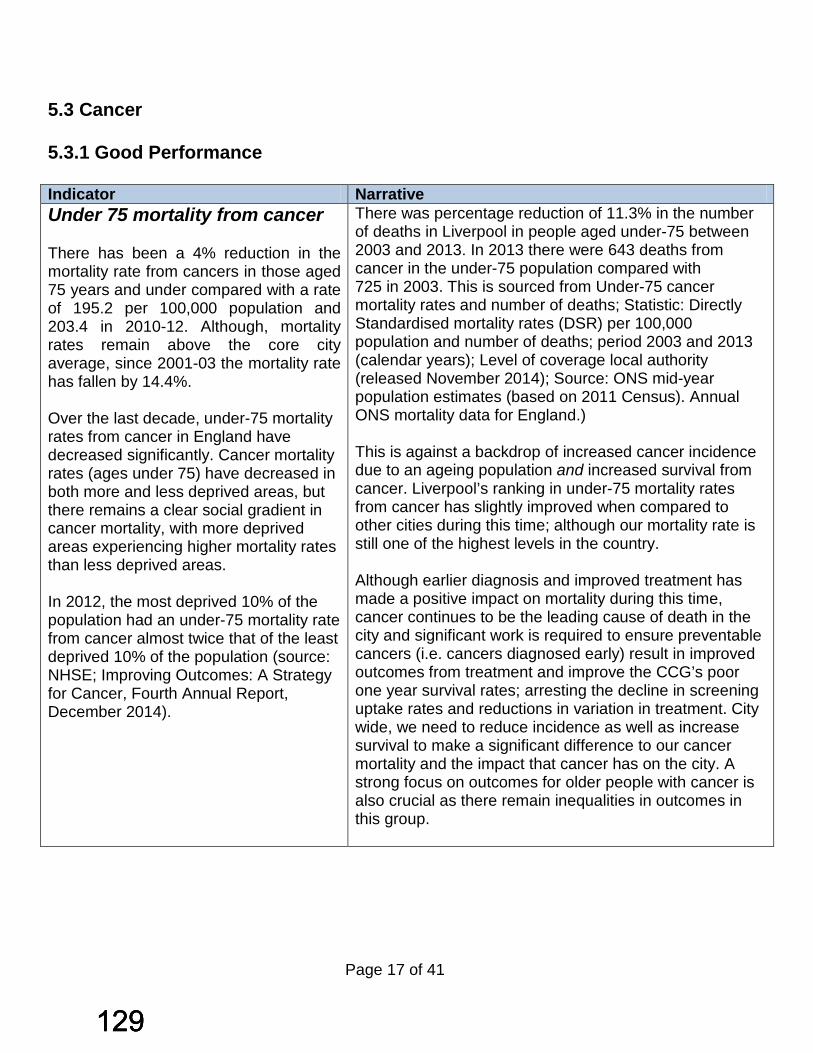
5.3 Cancer 5.3.1 Good Performance Indicator Narrative Under 75 mortality from cancer There has been a 4% reduction in the mortality rate from cancers in those aged 75 years and under compared with a rate of 195.2 per 100,000 population and 203.4 in 2010-12. Although, mortality rates remain above the core city average, since 2001-03 the mortality rate has fallen by 14.4%. Over the last decade, under-75 mortality rates from cancer in England have decreased significantly. Cancer mortality rates (ages under 75) have decreased in both more and less deprived areas, but there remains a clear social gradient in cancer mortality, with more deprived areas experiencing higher mortality rates than less deprived areas. In 2012, the most deprived 10% of the population had an under-75 mortality rate from cancer almost twice that of the least deprived 10% of the population (source: NHSE; Improving Outcomes: A Strategy for Cancer, Fourth Annual Report, December 2014).
There was percentage reduction of 11.3% in the number of deaths in Liverpool in people aged under-75 between 2003 and 2013. In 2013 there were 643 deaths from cancer in the under-75 population compared with 725 in 2003. This is sourced from Under-75 cancer mortality rates and number of deaths; Statistic: Directly Standardised mortality rates (DSR) per 100,000 population and number of deaths; period 2003 and 2013 (calendar years); Level of coverage local authority (released November 2014); Source: ONS mid-year population estimates (based on 2011 Census). Annual ONS mortality data for England.) This is against a backdrop of increased cancer incidence due to an ageing population and increased survival from cancer. Liverpool’s ranking in under-75 mortality rates from cancer has slightly improved when compared to other cities during this time; although our mortality rate is still one of the highest levels in the country. Although earlier diagnosis and improved treatment has made a positive impact on mortality during this time, cancer continues to be the leading cause of death in the city and significant work is required to ensure preventable cancers (i.e. cancers diagnosed early) result in improved outcomes from treatment and improve the CCG’s poor one year survival rates; arresting the decline in screening uptake rates and reductions in variation in treatment. City wide, we need to reduce incidence as well as increase survival to make a significant difference to our cancer mortality and the impact that cancer has on the city. A strong focus on outcomes for older people with cancer is also crucial as there remain inequalities in outcomes in this group.
Page 17 of 41
129129129

5.4 Long Term Conditions 5.4.1 Good Performance Indicator Narrative Health Related Quality Of Life for people with Long Term Conditions NHS Outcome ambition 2
Progress in this area continues to be built upon, with current performance in 2013/14 showing that two – thirds (66.2%) reported good health-related quality of life. This has exceeded the target set in 14/15 of 65.4%. However, Liverpool is currently ranked 15/16 CCG core city comparators for this indicator.
Reduction in emergency admissions – Stroke
The current 12 month rolling period (Nov 13 – Oct 14) has seen a reduction in emergency admissions fall by 14% for stroke patients This is an excellent result, and the CCG is optimistic that with the introduction of GRASP –AF (a tool used in primary care to help GPs assess the risk of Atrial Fibrillation) in all practices in 2015/16, this will continue to improve.
Reduction in emergency admissions – COPD
The current 12 month rolling period (Nov 13 – Oct 14) has seen a reduction in emergency admissions by 5% for COPD patients. This is performing above expectation and demonstrates real benefits for this cohort of patients.
Unplanned hospitalisation for chronic ambulatory care sensitive conditions: National data
This is line with national performance and so is a positive improvement for Liverpool, given its demographics. During 2013/14 Liverpool has observed a 1% reduction in the hospitalisation rate for chronic (ACS) It is important to note that this indicator cannot be compared with the local available data due to different reporting periods -national indicator is 13/14 and differing methodologies i.e. local data is crude rate level whereas the national data is age-standardised DSR. However both indicators are useful to monitor progress at a local level and compare CCG nationally
Under 75 mortality rate from cardiovascular disease
Deaths from CVD have seen a 5.3% reduction in 2011-13 with a rate of 108.8 per 100,000 population, compared with the previous year’s (2010-12) rate of 114.9 per 100,000. This reflects the efforts made within primary care to manage BP and Cholesterol more effectively and the increasing emphasis on prevention and lifestyle factors.
Page 18 of 41
130130130

5.5 Healthy Ageing 5.5.1 Good Performance Indicator Narrative Injuries due to falls (aged 65-79) During 2013/14 this indicator has shown significant signs
of improvement with a 13% reduction in the rate of injuries in persons aged 65-79. Although the number of injuries due to falls shows a reduction, Liverpool continues to benchmark poorly for falls in this age range. A key element of the redesign work for Healthy Ageing is focussed on establishing a comprehensive falls service for Liverpool, and a proposal is currently being designed by clinical leads to set out the details for this critical area.
Injuries due to falls (aged 80+) During 2013/14 this indicator has shown significant signs of improvement with a 12% reduction in the rate of injuries in persons aged 80+.
Hip Fractures in people aged 80+ The current 12 month rolling period (Oct 13 – Sep 14) has seen a reduction (3.2%) based on the previous rolling 12 months data in rate of hip fractures in people aged 80+ Due to reporting methodologies, data in this area is limited to September 2014 inclusive.
Diagnosis Rate for people with Dementia
Dementia diagnosis rates continue to increase month on month. More recent data at December 2014 shows that Liverpool has now reached the planned year end position with a diagnosis rate of 64.7%. It is anticipated that this figure will increase further over the last quarter of 2014-15 as practices undertake their record reviews for QOF purposes.
5.5.2 Areas for Improvement Indicator Narrative Hip Fractures in people aged 65-79
The current 12 month rolling period (Oct 13 – Sep14) has seen an Increase of 3.8% in the rate of Hip Fractures (310.7 per 100,000 population) compared to the previous rolling 12 months data with a rate of 299.4 per 100,000 population (due to reporting methods, data up to and including September 2014 is only reported). The recent approval of the new Fragility Fractures service will support the secondary prevention of hip fractures. It is anticipated that the new service at RLBUHT will be implemented from April 2015.
Page 19 of 41
131131131
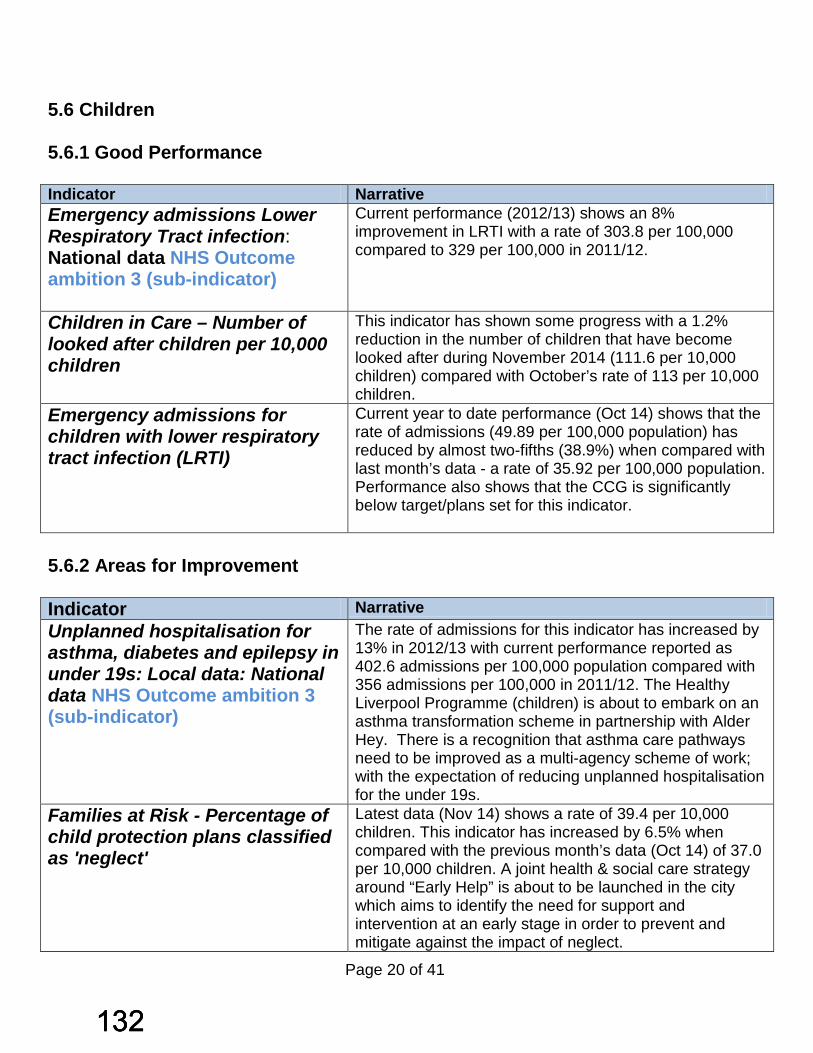
5.6 Children 5.6.1 Good Performance Indicator Narrative Emergency admissions Lower Respiratory Tract infection: National data NHS Outcome ambition 3 (sub-indicator)
Current performance (2012/13) shows an 8% improvement in LRTI with a rate of 303.8 per 100,000 compared to 329 per 100,000 in 2011/12.
Children in Care – Number of looked after children per 10,000 children
This indicator has shown some progress with a 1.2% reduction in the number of children that have become looked after during November 2014 (111.6 per 10,000 children) compared with October’s rate of 113 per 10,000 children.
Emergency admissions for children with lower respiratory tract infection (LRTI)
Current year to date performance (Oct 14) shows that the rate of admissions (49.89 per 100,000 population) has reduced by almost two-fifths (38.9%) when compared with last month’s data - a rate of 35.92 per 100,000 population. Performance also shows that the CCG is significantly below target/plans set for this indicator.
5.6.2 Areas for Improvement Indicator Narrative Unplanned hospitalisation for asthma, diabetes and epilepsy in under 19s: Local data: National data NHS Outcome ambition 3 (sub-indicator)
The rate of admissions for this indicator has increased by 13% in 2012/13 with current performance reported as 402.6 admissions per 100,000 population compared with 356 admissions per 100,000 in 2011/12. The Healthy Liverpool Programme (children) is about to embark on an asthma transformation scheme in partnership with Alder Hey. There is a recognition that asthma care pathways need to be improved as a multi-agency scheme of work; with the expectation of reducing unplanned hospitalisation for the under 19s.
Families at Risk - Percentage of child protection plans classified as 'neglect'
Latest data (Nov 14) shows a rate of 39.4 per 10,000 children. This indicator has increased by 6.5% when compared with the previous month’s data (Oct 14) of 37.0 per 10,000 children. A joint health & social care strategy around “Early Help” is about to be launched in the city which aims to identify the need for support and intervention at an early stage in order to prevent and mitigate against the impact of neglect.
Page 20 of 41
132132132
6. CCG QUALITY PREMIUMS Appendix 3 provides a summary of performance against the Quality Premium, although it should be noted that there is an overlap in a number of the items shown in this dashboard and those in the CCG Corporate and Provider Performance tables. Discussions are ongoing with between the CCG Business Intelligence Team and the CSU to amend the Corporate Performance Dashboard to reflect these changes. 7. NHS TRUST CLINICAL QUALITY AND NHS CONSTITUTIONAL RIGHTS In line with the recommendations of the National Quality Board (NQB) the Quality, Safety and Outcomes Committee have established a Quality Early Warning Dashboard. The purpose of this dashboard is to provide the CCG with a system to identify any issues and risks relating to patient quality and safety; particularly for those areas identified by the NQB as potential indicators of quality and safety issues. The dashboard covers all NHS Trusts within the Merseyside area and includes Risk Profiles for each organisation issued by the Care Quality Commission (CQC) and Monitor Risk and Financial Ratings. Where risks have been identified they will be actively managed through CCG governance arrangements overseen by the Quality, Safety and Outcomes Committee, Trust Clinical Quality and Performance Meetings and collaborative commissioning arrangements with Merseyside CCGs. 7.1 Care Quality Commission and Monitor Warning/Issue Notices & Inspections Where providers are not meeting essential standards, the CQC has a range of enforcement powers to protect the health, safety and welfare of people who use the service (and others, where appropriate). When the CQC propose to take enforcement action, the decision is open to challenge by the provider through a range of internal and external appeal processes. The following updates are provided in relation to recent CQC inspection activity locally:
Page 21 of 41
133133133
7.2 CQC Inspections of Liverpool GP Practices Under the new CQC inspection model, GP practices will be assessed against the following five key questions about the practice:
• Is it safe? • Is it effective? • Is it caring? • Is it responsive to people’s needs? • Is it well led?
All GP practices will be rated by April 2016, which enable patients and commissioners to use the CQC’s judgement in establishing the standard of care provided. The CQC has published reports in January 2015 relating to three Liverpool CCG practices, summaries of which are provided below: 7.2.1 Park Road Group Practice The overall rating for Park Road Practice was ‘Good’ and the practice also received a rating of ‘Good’ for four out of the five standards inspected. In determining whether services are ‘Safe’ the report concluded that this area required improvement. The report highlighted concerns that risk assessments and risk management procedures were not up-to-date and recommended that these elements should be reviewed and localised. The practice recruitment policy and procedures did not include a policy statement or risk assessment for undertaking Disclosure and Barring Service checks to ensure it reflected national guidance and legislation. Required information relating to staff and their suitability for their role was not available, checked or held by the practice. The CQC report for this practice also recommended follow-up audits and an undertaking to ensure that the audit cycle is complete and improvements can be demonstrated. The practice was also asked to undertake a review of actions taken as a result of patient complaints in order to demonstrate learning and improvements and conduct a review. Further concerns were raised in relation to fire risk assessments and the practice was asked to update its ‘Fire Precautions Policy and procedures’ to reflect the local situation and current guidance and ensure that fire alarms checks were recorded fully to evidence that they were undertaken appropriately.
Page 22 of 41
134134134
7.2.2 Picton Green Family Practice The overall rating for this service was ‘Good’ and the practice also received a ‘Good’ rating for four out of the five standards. In determining whether services are ‘Safe’ the report concluded that this area required improvement. The required information relating to staff and their suitability for their role was not available, checked or held by the practice. The inspection recommended that the practice improve the management of Patient Group Directives (PGDs) to ensure safe administration of relevant medicines by appropriately qualified staff. Other areas highlighted as requiring improvement included training for all staff in Infection Control and an improvement of medical emergency equipment to ensure staff can safely and appropriately respond to medical emergencies. 7.2.3 Dr S Dharmana Family & General Practice The CQC planned comprehensive inspection took place on 1st October 2014. The subsequent inspection report published on 22nd January 2015 provided an overall rating for the service as ‘Inadequate’. All five domains for Safe, Effective, Caring, Responsive and Well Led were rated as ‘Inadequate’. Key findings of the inspection report were as follows:
• Positive comments were received from patients that inspectors spoke to during the visit. Patients were complimentary about the reception staff;
• Although Dr Dharmana had not provided clinical care since November 2013 patients spoke highly of him;
• There were no systems in place to monitor the quality and safety of the service provided to patients. Evidence of analysis of significant events was not available for 2014 and there was no evidence of recent clinical audits;
• The quality of service provided by locum GPs was not monitored and systems to ensure information was shared with locum GPs (e.g. alerts for medicines and equipment) were not in place;
• Equipment to respond to medical emergencies was not accessible and when located was not adequately resources to respond to a medical emergency. Checks to monitor medicines and medical equipment held at the practice were not undertaken;
• Systems to monitor and respond appropriately to safeguarding concerns were not robust, nor were staff pre-employment checks.
Page 23 of 41
135135135
Given the level of concern and the provider’s failure to meet Regulation 10 of the Health & Social Care Act 2008 (Regulated Activities) the practice has been placed in special measures. The CCG is providing support to the practice (along with the Local Medical Committee and continues to work closely with NHS England on an agreed improvement action plan to be delivered over the next six months (performance managed by NHS England). Due to the concerns with regard to safe prescribing practices, NHS England has put in place additional medicines management support. The CCG Primary Care Team is also providing senior management support to ensure systems and processes are in place for the safe and sustainable running of the practice to address the concerns of the CQC, who will re-inspect the practice in six months’ time. 7.2.4 Great Homer Street Medical Centre The practice received an overall composite rating of ‘Requires Improvement’ following their CQC inspection, which rated three out of the five indicators as ‘Requires Improvement’. The practice is required to develop a separate improvement plan using the CQC template with support from NHS England and the CCG. The practice will then have 6 months to implement the plan. The CCG will continue to meet with the practice regularly to offer any support required in the implementation of their plan (which will be performance managed by NHS England). 7.3 CQC Hospital Monitoring Intelligence Reports The CQC developed this set of indicators through consultation and testing to replace Quality Risk Profiles. The CQC has analysed each of the indicators to identify one of the following levels for each trust:
• ‘No evidence of risk’
• ‘Risk’
• ‘Elevated risk’ Trusts that have undergone inspection at the time of producing updates of Intelligence Monitoring have not been assigned a banding; all other indicator analysis results are shown in their individual reports (“Recently Inspected” is stated for these providers). Profiles of all local acute trusts and relevant analyses will be included in the March 2015 Governing Body Performance Report.
Page 24 of 41
136136136
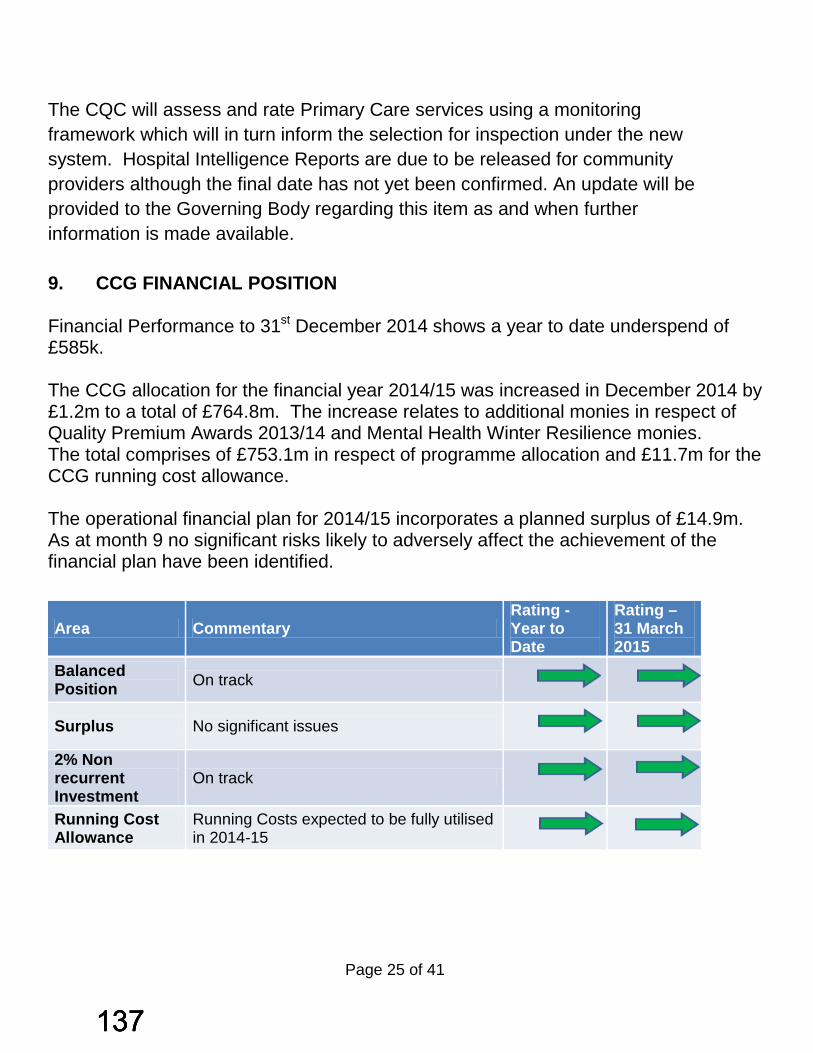
The CQC will assess and rate Primary Care services using a monitoring framework which will in turn inform the selection for inspection under the new system. Hospital Intelligence Reports are due to be released for community providers although the final date has not yet been confirmed. An update will be provided to the Governing Body regarding this item as and when further information is made available. 9. CCG FINANCIAL POSITION Financial Performance to 31st December 2014 shows a year to date underspend of £585k. The CCG allocation for the financial year 2014/15 was increased in December 2014 by £1.2m to a total of £764.8m. The increase relates to additional monies in respect of Quality Premium Awards 2013/14 and Mental Health Winter Resilience monies. The total comprises of £753.1m in respect of programme allocation and £11.7m for the CCG running cost allowance. The operational financial plan for 2014/15 incorporates a planned surplus of £14.9m. As at month 9 no significant risks likely to adversely affect the achievement of the financial plan have been identified.
Area Commentary Rating - Year to Date
Rating – 31 March 2015
Balanced Position On track
Surplus No significant issues
2% Non recurrent Investment
On track
Running Cost Allowance
Running Costs expected to be fully utilised in 2014-15
Page 25 of 41
137137137

10. SUMMARY Where performance is at variance to plan action is underway with Trusts to deliver corrective action to improve performance in 2014/15 with contractual levers utilised to support improvements. These improvements are actively led by CCG Clinicians.
Stephen Hendry Senior Corporate Services Manager
(Performance & Operations)
Ian Davies Head of Operations & Corporate Performance
3rd February 2015
Page 26 of 41
138138138
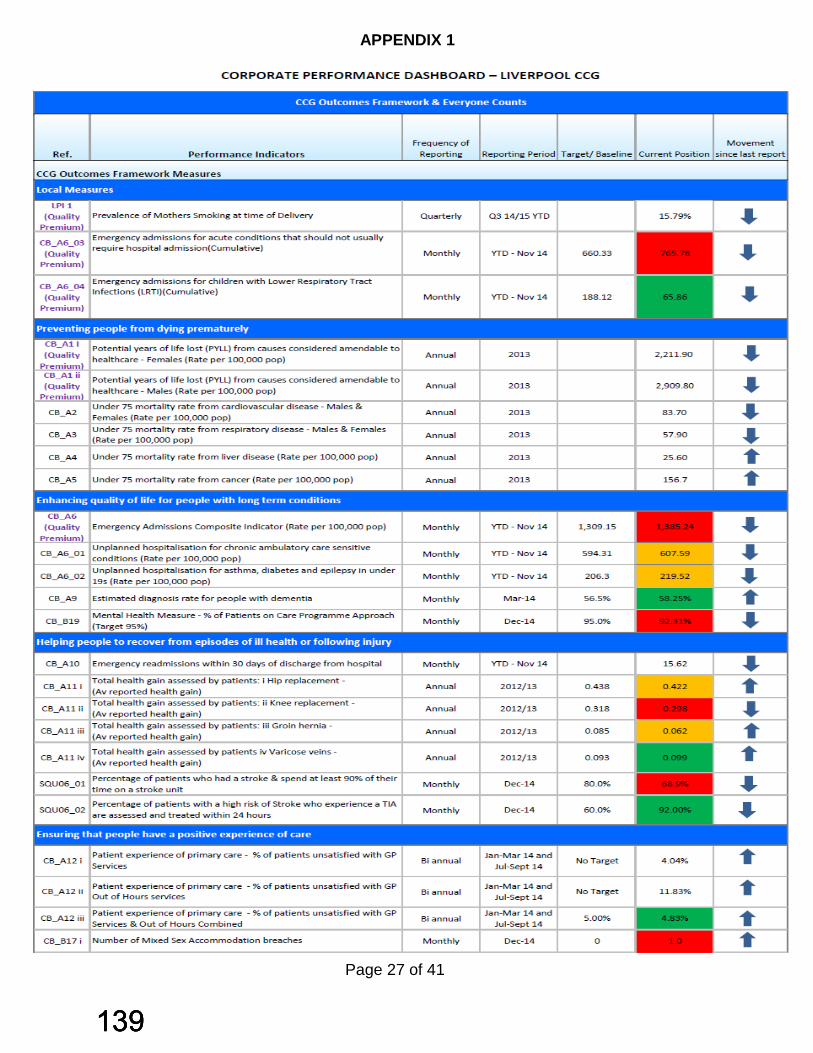
APPENDIX 1
Page 27 of 41
139139139

Page 28 of 41
140140140

Page 29 of 41
141141141

APPENDIX 2
Page 30 of 41
142142142

Page 31 of 41
143143143
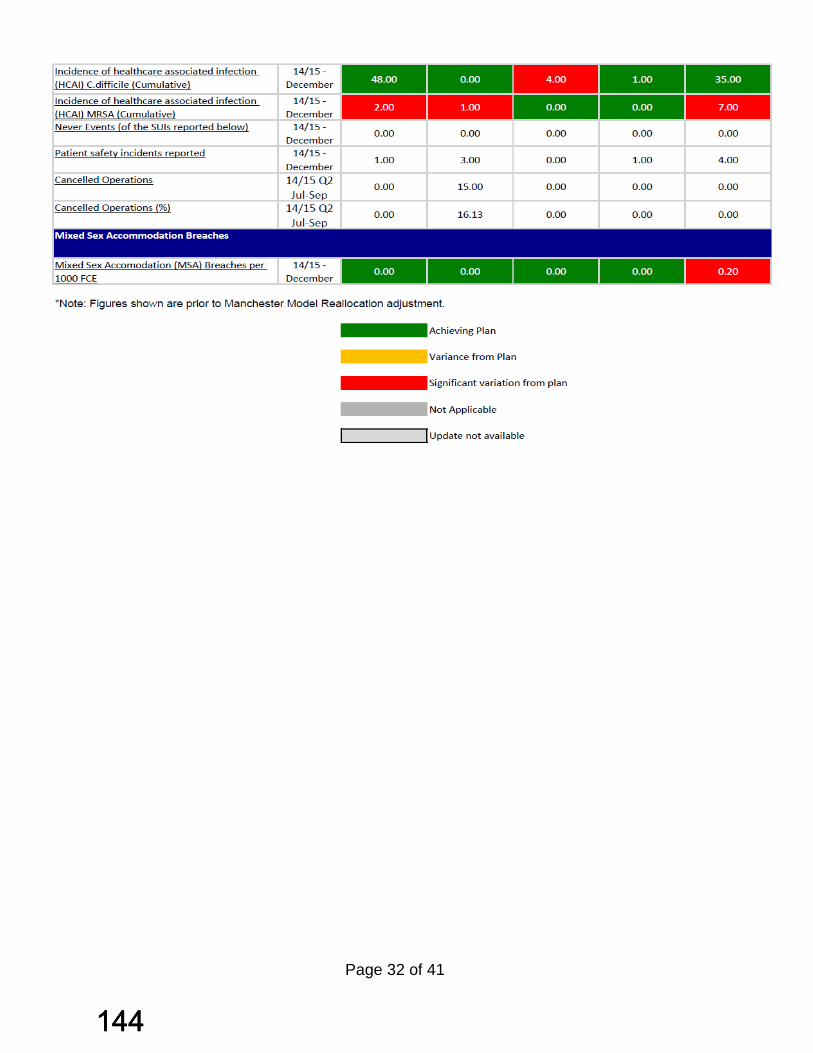
Page 32 of 41
144144144
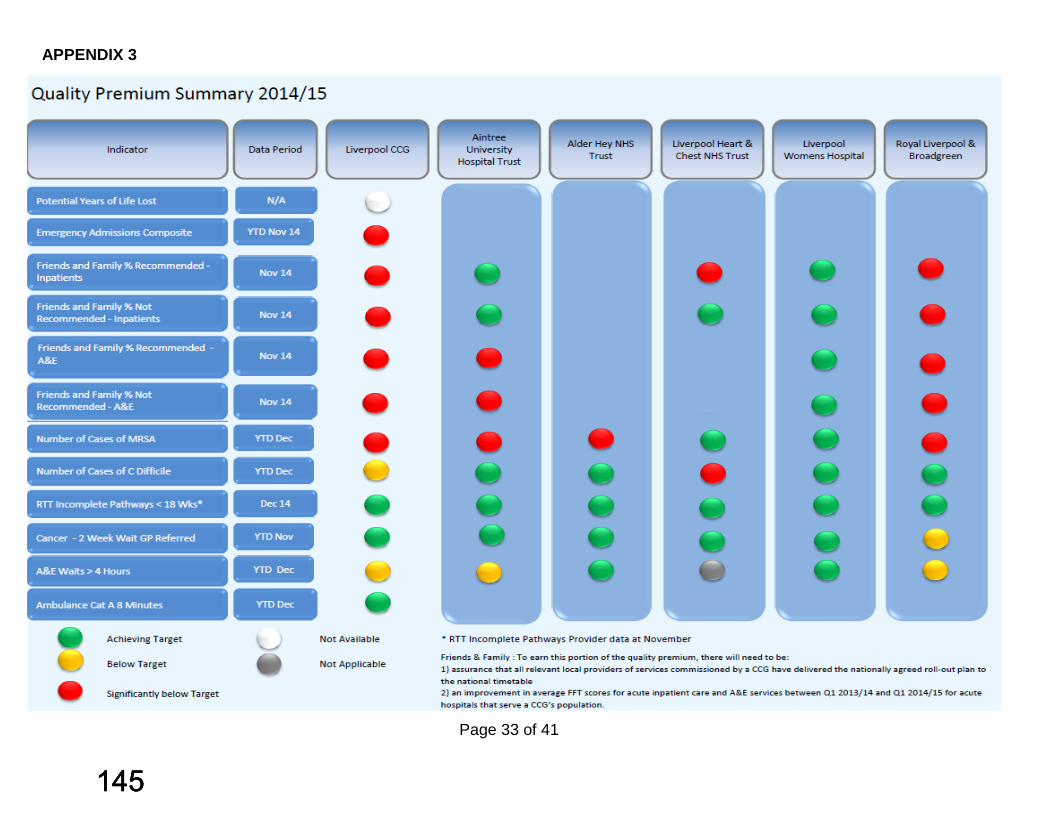
APPENDIX 3
Page 33 of 41
145145145
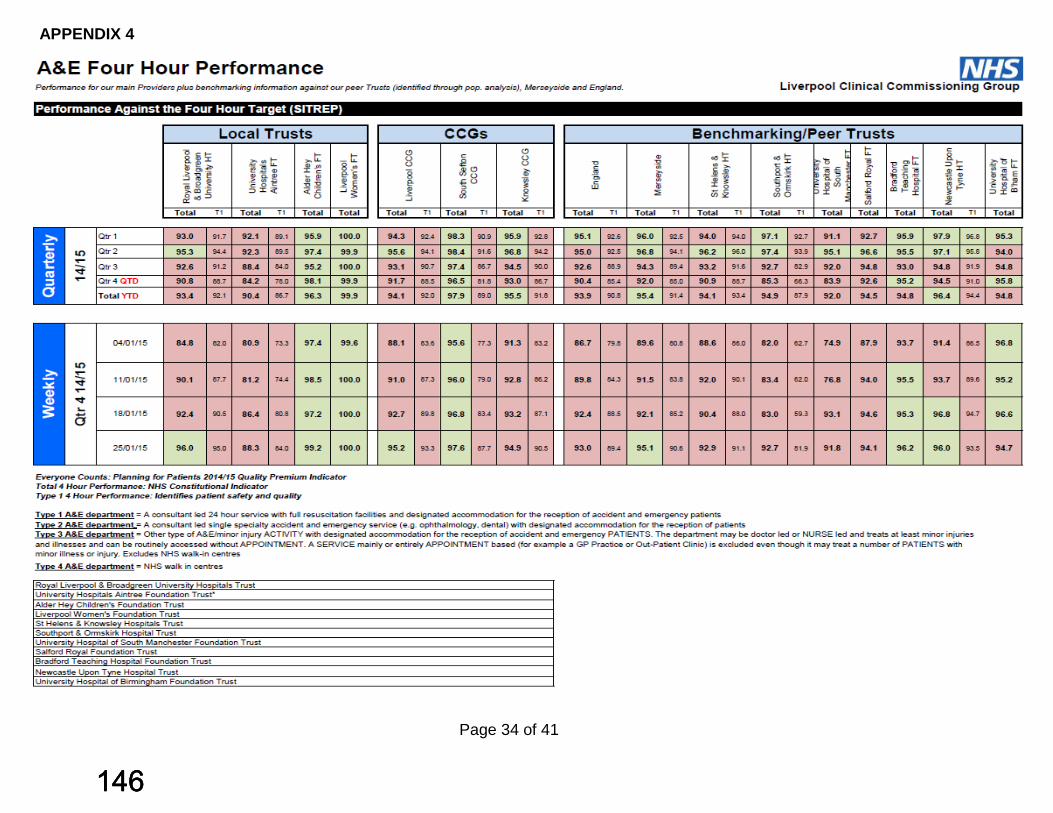
APPENDIX 4
Page 34 of 41
146146146

Page 35 of 41
147147147
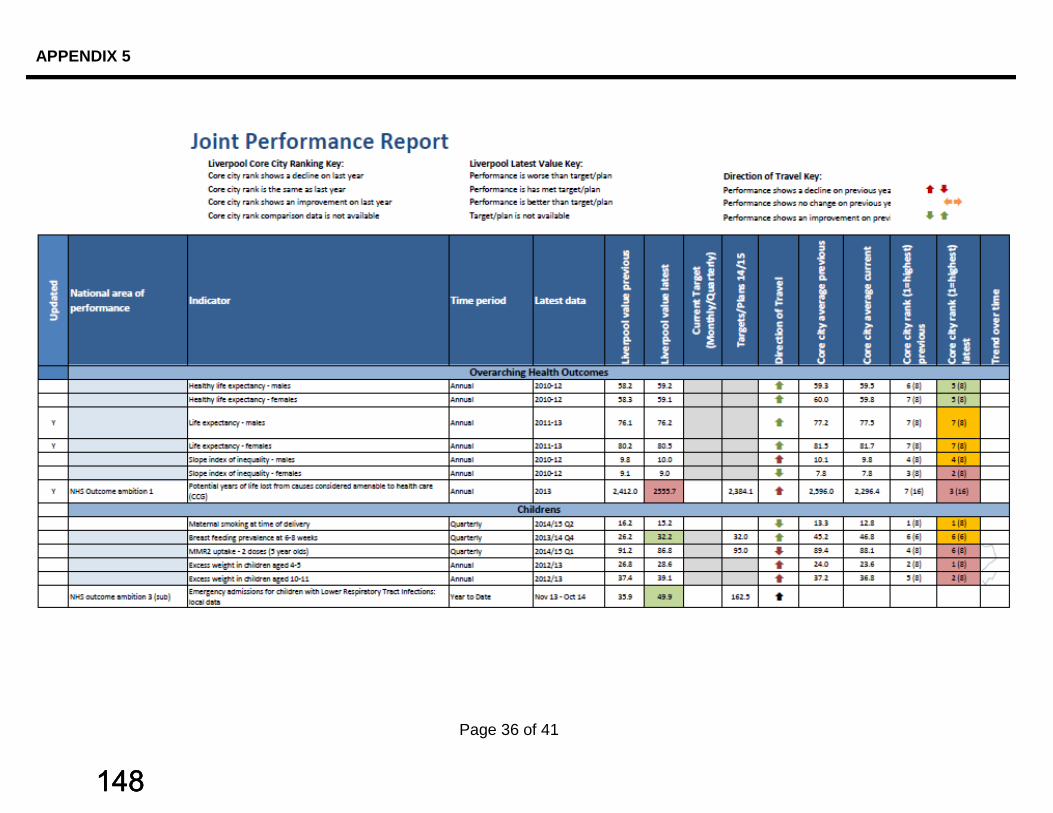
APPENDIX 5
Page 36 of 41
148148148
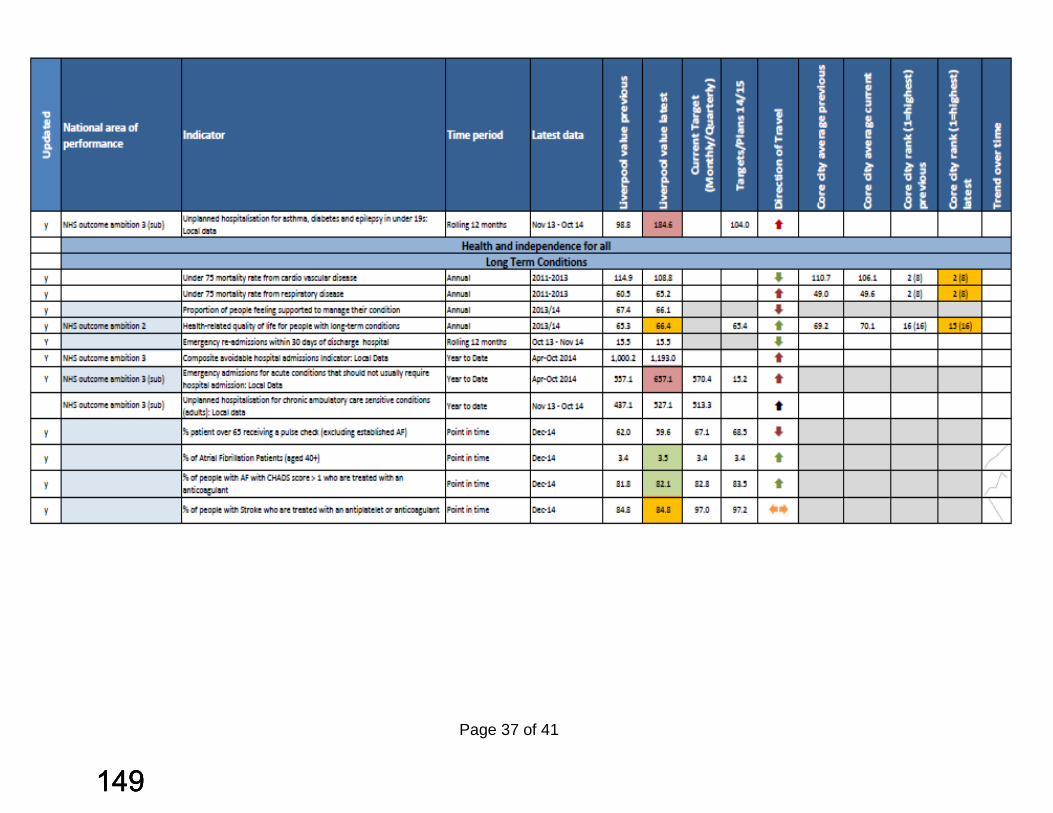
Page 37 of 41
149149149

Page 38 of 41
150150150

Page 39 of 41
151151151
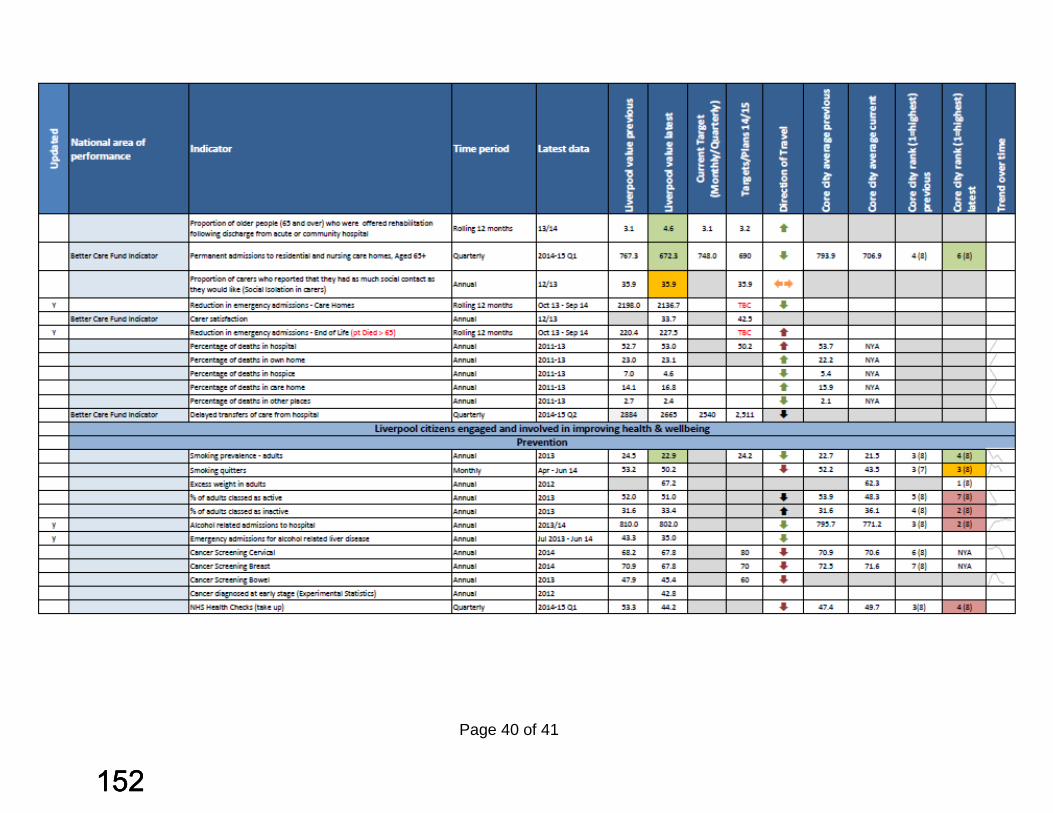
Page 40 of 41
152152152
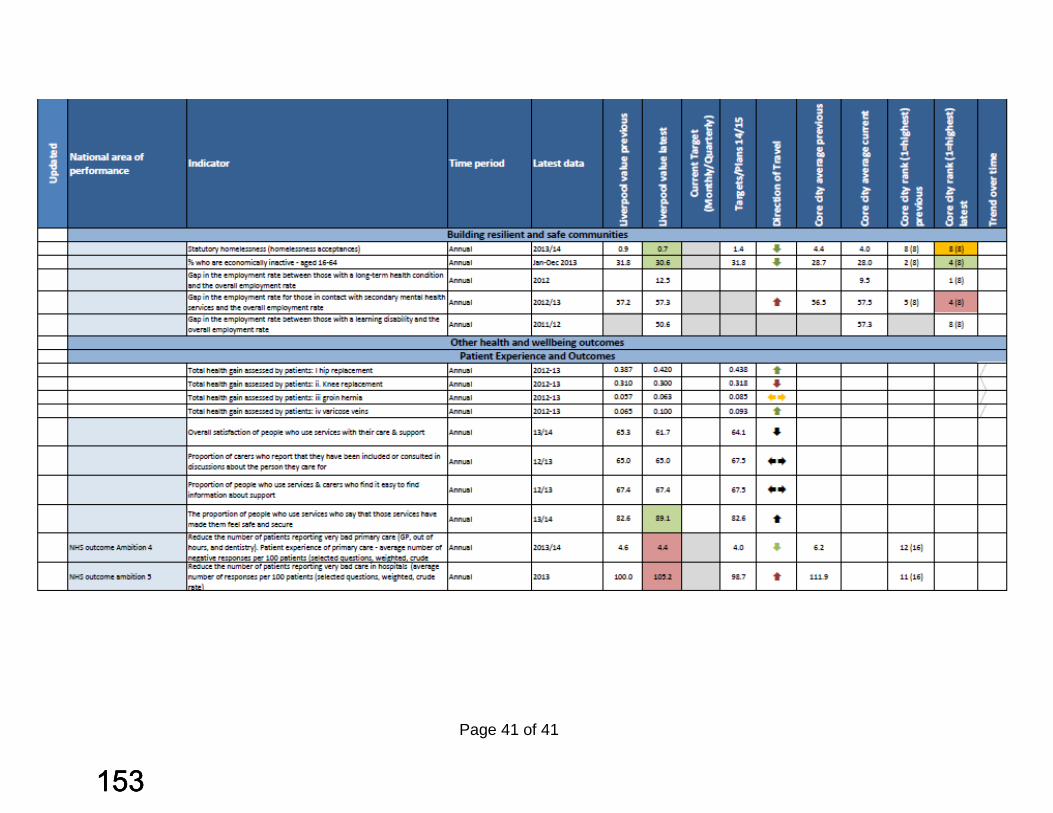
Page 41 of 41
153153153

154154154
HEALTHY LIVERPOOL PROGRAMME
HOSPITAL BASED SERVICES
COMMITTEE(S) IN COMMON
KNOWSLEY, LIVERPOOL AND SOUTH SEFTON CCGS AND NHSE
WEDNESDAY 5TH NOVEMBER 2014
MINUTES
PRESENT:
Katherine Sheerin Chief Officer NHS Liverpool CCG
Tom Jackson Chief Finance Officer Dr Donal O’Donoghue Secondary Care Doctor Ian Davies Fiona Clarke Chief Officer NHS Sefton CCG
NHS Southport and Formby CCG
Graham Morris Dr Rob Caldwell Dr Andy Pryce Chair NHS Knowsley Paul Brickwood Chief Finance Officer Knowsley, St Helens and
Halton CCG
APOLOGIES
Dr Nadim Fazlani Chair NHS Liverpool CCG Dianne Johnson Chief Officer NHS Knowsley CCG Martin McDowell Dr Fiona Lemmens GP/Governing Body Member NHS Liverpool CCG
155155155

1. Introductions
KS welcomed everyone to the meeting and introductions were made.
2. Background and purpose of the meeting
KS explained the background to the Healthy Liverpool Programme, how changes are described across three settings of care –
Living Well Transformed Community Services The best hospital care
Underpinned by six priority clinical areas –
Children’s Services Healthy Ageing Long Term Conditions Mental Healthy Learning Disabilities Cancer
Work has been progressing well, with clear plans emerging. However there is now a requirement for decisions regarding hospital services to be aligned across commissioners, and as such, the Committee in Common has been established as the vehicle to enable this to happen.
Alison Tonge commented that it is really important that the CIC is established now in order to bring together commissioners to facilitate joint decision making.
3. Draft Terms of Reference
The draft TOR were discussed. Minor amendments were agreed. It was highlighted that it would be useful to understand the scrutiny arrangements for each Local Authority, in order that we can timetable key meetings.
ACTIONS – KS to circulate revised TOR
FC / DJ / KS to pull together scrutiny process / timetable
156156156
4. Update on Hospital Based Services Work Stream
ID/DO’D explained that the work is structured around 5 key areas –
Urgent Care Cancer Women’s Services (including Neonatology) Stroke Cardiac Care
For each area, clinical workshops are held, with standards for delivery agreed. Work had progressed furthest in Urgent Care, with standards nearly agreed. It was planned that standards will be clear by Christmas.
5. Update from Specialist Commissioning (NHSE)
AT outlined the changes to NHSE structure currently being worked through, and the impact of this on decision making regarding commissioning. There is much to be learned from the Healthier Together Programme, and it is key that the governance arrangements are clearly described from the outset.
AT explained that NHSE is keen that providers develop network based solutions for delivery of services which meet national service specifications, with full scale procurements avoided where possible.
In terms of co-commissioning, AT explained that 4 services are likely to be delegated to CCGs from April 2015, with all ‘tier 2’ services delegated or commissioned jointly from April 2016. We need to prepare carefully for this.
With regard to Major Trauma services, much work has been done on this. It was agreed that a clear decision making path is needed.
ACTION- ID to develop decision making path for discussion at next CIC (working with Louise Sinnott for Major Trauma)
6. Development of options
The process was discussed. It was explained that following the work by the clinicians on developing standards, this is then reviewed by the Chief Executive’s Group, who’s role is to reach alignment regarding the optimum service delivery model by site. It is planned that alignment should be reached by Christmas.
157157157
It would then be for the CIC to determine which option(s) go forward for consultation, with the backing of each statutory body.
TJ outlined the economic modelling work which has been commissioned from FTI to support this. This will confirm future needs, and model the sustainability of different options.
7. NHSE Assurance Process
Healthy Liverpool is now on the ‘tracker’ and part of the NHSE assurance process. The first assurance meeting was held at the beginning of October, with positive informal feedback. An update will be provided at the next meeting.
8. Key Milestones for the Healthy Liverpool Programme
Key milestones were shared and discussed. It was explained that a period of intensive community engagement will commence in the new year, in order to explain the need for change to local people, based on the Prospectus for Change document.
The programme plan is being updated and will be shared.
9. Meetings schedule for CIC
1st Wednesday of the month, approx 4pm (to follow the CCG Network meeting).
Venue – as per CCG network meeting
10. Date and time of next meeting
4pm, Wednesday 7th January 2015, Merton House, Bootle.
158158158
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP
PRIMARY CARE COMMITTEE Minutes of meeting held on Tuesday 25th November 2014 at 1pm
Boardroom Arthouse Square Present: Nadim Fazlani (NF) Chair Dr Rosie Kaur (RK) GP Governing Body Member/Vice Chair Moira Cain (MC) Practice Nurse Governing Body Member Shamim Rose (SR) GP/Governing Body Prescribing Lead Dave Antrobus (DA) Governing Body Lay Member – Patient
Engagement Paula Finnerty (PF) GP – North Locality Chair Ray Guy (RG) Governing Body Practice Manager co-opted
member In attendance: Rob Barnett (RB) LMC Secretary Simon Bowers (SB) GP Governing Body Member Jenny Levy (JL) Neighbourhood Transformational Manager –
North Colette Morris (CMo) Locality Development Manager – Liverpool
Central Jacqui Waterhouse (JW) Locality Development Manager – Matchworks Peter Johnstone (PJ) Transformation Change Manager –
Prescribing Rose Gorman (RGo) Contract Manager, Commissioning
Directorate - NHS England Laura Buckels (LB) Senior Intelligence Analyst Scott Aldridge (SA) Neighbourhood Manager - North
Locality/Local Quality Improvement Schemes and Veteran Health Lead
Paula Jones (PJ) PA/Note Taker Apologies: Jude Mahadanaarachchi GP Governing Body member /Liverpool (JM) Central Locality Chair Paula Parvulescu (PP) Consultant in Public Health Medicine,
Liverpool City Council
Page 1 of 12
159159159

James Cuthbert (JC) GP Governing Body Member/Matchworks Locality Chair
Steve Appleton (SAp) Head of Clinical Informatics, Informatics Merseyside
Cheryl Mould (CM) Head of Primary Care Quality and Improvement
PART 1: INTRODUCTIONS & APOLOGIES
1.1 DECLARATIONS OF INTEREST
There were no declarations of interest made specific to the Agenda
1.2 MINUTES OF PREVIOUS MEETING, ACTIONS AND MATTERS
ARISING NOT ALREADY ON THE AGENDA
The minutes of the previous meeting held on 28th October 2014 were accepted as an accurate record of the discussions which had taken place. 1.2.1 Action Point One – PJ updated the Primary Care
Committee that the commercial Sponsorship Policy had been sent to the Lay Member for Governance/Deputy Chair of the Liverpool CCG Governing Body for review.
1.2.2 Action Point Two – DA noted that new guidelines for
Equality Delivery had been received from NHS England and a paper was being prepared by the Head of Contracts & Procurement which would supersede the paper brought to the Primary Care Committee in March 2014. This would hopefully be brought back to the Primary Care Committee in December 2014 but given the other priorities of the Head of Contracts & Procurement before Christmas 2014 this was a tight deadline.
1.2.3 Action Point Three – it was noted that the Primary Care
Quality Framework was to be brought to the Primary Care Committee on a six monthly basis and would next come to back to the Primary Care Committee in January 2015.
1.2.4 Action point Five – Community Pain Service, it was noted
that this was ongoing.
Page 2 of 12
160160160
1.2.5 Action Point Six it was noted that the Organisational Development update was coming back to the January 2015 meeting.
1.2.6 Action Point Seven – CMo noted that the issue of Gold
Standard IM&T was in progress and iMerseyside were working on the project and more information would be available at the end of the week.
The Primary Care Committee:
Noted the points made under matter arising.
PART 2: UPDATES
2.1 WORKSTREAMs UPDATE – REPORT NO: PCC 42-14
a) Localities – Report No PCC 42a-14
North – PF
• Update given on achievements in North Locality, the Leadership Team were pleased with the progress made on reducing outpatient referrals, ACS admissions and improving the control of cholesterol and hypertension. It was felt that a summary of achievements should be put together for sharing with all providers, for all Localities not just North. RG advocated sharing with the Health & Wellbeing Board. LB noted that the Chief Officer already had something prepared for the Kings Fund which could be used. However RB advocated caution over what information was shared as General Practice was already under significant pressures and the result of promoting successful performance in reducing activity in Secondary Care might result increased pressures on an already stretched resource. NF agreed that the process needed to be managed with different nuances for different audiences but it would be could to celebrate the achievements of Primary Care. It was confirmed in response to a query from MC that she could share this information with Practice Nurses and Practice Managers. SB noted that the achievements of Primary Care supported the application for co-commissioning as evidence of the CCG’s commissioning
Page 3 of 12
161161161

intentions i.e. increased investment resulted in improved output.
• GP Specification Validation Report – an audit of clinical
input was needed and some practices might require assistance. JW noted that a pack was being put together to help practices prepare for audit and this would be sent to the Validation Panel for approval before being sent out to practices.
• Congress meeting – Walton Neighbourhood had now
identified a clinical lead and the Croxteth Neighbourhood had two potential candidates.
• Data had been submitted to the national diabetes audit.
Central – CMo
• MCAS Pilot evaluation was presented and the recommendations agreed.
• Pain Management Service would be discussed again at the
next meeting.
• Mental Health Team provided an update regarding the Primary Care Mental Health Strategy.
• Strategy meeting held 6th November 2014 – discussed the
Healthy Liverpool Programme Prospectus for Change.
• Sharon Poll had presented the Organisational Development Strategy which had been well received, looked at the Locality priorities and how mutual support could be given.
• Transforming Neighbourhoods – Neighbourhood updates
given and concerns raised around the pace of change particularly around step down care/rehabilitation therefore Michelle Urwin was to be invited to the next meeting to give an overview.
Matchworks – JW
• Transforming Neighbourhoods – Gateacre/Woolton were struggling to identify a lead to replace Dr David Webster.
Page 4 of 12
162162162

• Mental Health Team feedback – waiting times for IML had
reduced, link between mental health and physical activity had been highlighted.
• Coding was required for electronic cigarettes and Claire
Gornall was ensuring that this was set up again.
• The Group looking at variations in the use of the template had been re-instated. It was noted that information from Walk In Centres was not being fed back to General Practice as patients were being asked whether or not they wanted their GP to be informed of their attendance or not which needed to be looked into. SR noted that particularly regarding the Children’s Walk In Centre this had safeguarding implications. RB noted that this was however the correct procedure of GUM clinics.
.
b) Medicines Management Sub Committee Report: PCC 42b-14 SR updated: • Medicines Management were attempting to analyse trends
in prescribing cost growth. Further analysis did not always substantiate the explanations given. The risk to the CCG was that by the next validation round over 50% of practices would fail the Key Performance Indicator set which would then discredit the indicator itself as not achievable. PJ added that the issue was increase in cost and growth in prescribing. The CCG had limited influence over SSP practices and RGo agreed to speak to Alan Cummings at NHS England who could raise this at contract meetings.
There were unavoidable costs such as increase in Category M pricing and also the pressure on Primary Care prescribing from use of NOACs by Secondary Care now that NICE Guidance had changed. RB who was a member of the Medicines Management Sub-Committee noted that practices were moving from average spend to cost therefore the comparison between years was not appropriate. However PJ maintained that cost issues could be explained/evidence at validation, the issue of concern was unexplained growth. The Validation process was time consuming but a very robust and powerful tool.
Page 5 of 12
163163163
SR noted that she had met with the Prescribing Leads for SSP and had shared how to implement savings which they had taken on board. RB advised caution where practices had invested GP Specification money in extra staff and failed to produce change/saving and that they should be able to keep the resource. Again it was noted that this was part of the validation process. On the subject of NOAC prescribing from Secondary Care the difficulty was highlighted of how GPs could or could not overturn prescribing decisions in Secondary Care.
• Prescribing for Primary Prevention in Coronary Heart
Disease – the new NICE guidance on statins prescribing could possibly have a significant on prescribing levels It was agreed that it was up to the patient and the GP to decide between them on what was most appropriate rather than a blanket interpretation of the guidance.
c) Community Settings of Care (HLP) - Report PCC 42c-14
PF updated: • First meeting under the new group name had taken place
on 6th November 2014.
• Core Community Services Offer – the offer was to be shared prior to the next meeting.
• Communication – there was to be a clear message from
the external steering group.
• Governance – providers were to report back on how information was fed into the group.
• The meeting had gone very well but there had been no
representation from Mersey Care and hopefully this would not be the case at the next meeting.
• Second meeting of Clinical and Non Clinical leads had
been held and had been well attended. The output was being shared with the Neighbourhoods and would be discussed again at the December meeting.
Page 6 of 12
164164164
d) Patient Engagement & Experience Sub-Committee - Report
PCC 42d-14 DA updated: • VCSE engagement delivery plan was discussed and there
was a further meeting to take place the following week.
• Healthy Liverpool Programme – capacity to look at all engagement templates before they go out.
• Patient Experience – report to go to Senior Management
Team and Finance Procurement & Contracting Committee.
• Patient opinion – 90% of the comments for the Royal Liverpool Hospital were positive.
The Primary Care Committee:
Noted the reporting templates.
2.2 UPDATE FROM NHS ENGLAND – VERBAL
RGo updated the Governing Body on recent activity in NHS England Merseyside Area Team:
• Offer to all practices across Merseyside re the Direct Enhanced
Service • Care Quality Commissioning information had been sent out the
previous week.
• Re guidance for the Care Quality Commission visits there was a meeting the following day with the Care Quality Commission/CCGs/Trusts.
• Friends & Family Test information event to be held at Everton
FC.
• New guidance on co-commissioning had come out the previous week and a local contract manager allocated to each CCG.
• Dementia identification scheme commenced.
• Area Team interviews for positions had commenced.
Page 7 of 12
165165165

PART 3: SERVICE DEVELOPMENT/IMPLEMENTATION
3.1 FEEDBACK FROM GROUP SET UP TO LOOK AT DEMANDS ON PRIMARY CARE FROM SECONDARY CARE VERBAL
An initial meeting of this group had taken place at RB’s practice. JW had been asked to get more information from constituent practices and the recommendation had been to complete the analysis in a sensible and constructive way. JW confirmed that she had asked practices to send examples of inappropriate request ready for the next meeting in January 2014. These would be used for the basis of clinician to clinician conversations with trusts. The Primary Care Committee:
Noted the verbal update.
3.2 GUIDANCE ON THE NEW OUT OF AREA PATIENT REGISTRATION ARRANGEMENTS REPORT NO: PCC 43-14
PJ introduced the paper to the Primary Care Committee on change to the GP contract allowing the registration of patients who lived outside current practice boundaries and the ensuing problems over out of hours and community services. SA noted that this would be discussed at the Liverpool CCG Senior Management Team meeting on 1st December led by the Head of Operations & Corporate Performance. Suggestions were that each Neighbourhood could have at least one provider as it was not sure that UC24 could pick this up. There were contract implications for UC24 and Liverpool Community Health on their interaction with patients registered with Liverpool GPs and over the sharing of patient information between the health professionals providing primary care services for patients out of hours and in the community as well as at GP surgery. RG noted that if no practices took up the Direct Enhanced Service NHS England would need to source something themselves. DA noted that there were implications for the Better Care Fund and the Local Authority dealing with patients from outside the Merseyside area.
Page 8 of 12
166166166
RB noted the need for caution with patients with complex needs and that more thought was required around this area. SB added the clinical risk for elderly patients moving to live close to or with adult children and the challenges they represented. RB felt that in some cases it would not be clinically appropriate for the patient and that it should be up to the patient and the GP to decide which was supported by the guidance. He requested that the detail should be worked up and put in the public domain as soon as possible. It was agreed that RB, SA, PJ and NF would draft a letter to be sent out to all GPs in NF’s name. RGo agreed to keep the Primary Care Team (CMo) updated. RB queries if NHS England would accept sign up to the Direct Enhanced Service from practices with whom they were not satisfied with around performance.
The Primary Care Committee:
Noted the content of the guidance. Considered actions to communicate to general practices Considered CCG responsibilities and the arrangements
required to co-commission service. Agreed for a letter to be drafted to go out in NF’s name to
all practices.
PART 4: QUALITY & PERFORMANCE
4.1 LOCAL IMPROVEMENT SCHEMES 2015-16 REPORT NO: PCC 44-14
RK introduced a paper to the Primary Care Committee on the reviews of the current Local Enhanced Services and copies of the specifications had been provided. Only minor changes had been made to the specifications which for H Pylori, Near Patient Testing, Travellers, Asylum Seekers and Impaired Glucose Regulation were unchanged, minor changes had been made to ABPI and minor surgery. Re Homeless the Clinical Lead Dr Debbie Faint was looking at this and recommended the inclusion of provision for ‘flu’ and TB screening which had not been done yet and would be included next year. The Specifications would then
Page 9 of 12
167167167

go to the Local Medical Committee and then the CCG contracting process for practices to then sign up. A discussion took place about minor surgery and providers demonstrating competency every three years as 43 out of the 80 practices offering this service had not responded with evidence of competency. This was not restricted to certificates or training but being able to demonstrate experience and good outcomes/lack of ensuing complications. Provided practices could evidence this this would be considered satisfactory but failure to respond at all should result in the contract being terminated.
The Primary Care Committee:
Approved the specifications to allow progression of
engagement with the LMC and NHS England before progressing to issuing NHS Standard Contracts.
Approved the requirement that all Minor Surgery provider have to provide evidence every three years of their competencies to provide the service.
4.2 REVIEW OF LOCAL AND NATIONAL INITIATIVES IN PRIMARY CARE 2014/15 – A FRAMEWORK FOR EVALUATION REPORT NO: PCC 45-14
CMo presented a paper to the Primary Care Committee to present the proposed framework for evaluation of the national and local initiatives in primary care for the winter period 2014/15. There were two elements to the evaluation, qualitative and quantitative. Monitoring would be carried out monthly or quarterly as set out in the paper with all practices having to provide information via completion of a template. A full report would be sent to the Primary Care Committee in July 2015. Regular updates would be brought to the Primary Care Committee in the interim as and when required.
The Primary Care Committee:
Noted the content of the framework for evaluation
Page 10 of 12
168168168
Agreed process and timescales for reporting of full evaluation to July 2015 Primary Care Committee
4.3 CARE QUALITY COMMISSION INTELLIGENT MONITORING VERBAL JW tabled a document on the Care Quality Commission’s intelligent monitoring to prioritise general practice visits. It was noted the there was no particular sense to the format used as some very good practices were showing as needing a priority visit. However it was also noted that the criteria used were part of the Primary Care Quality Framework. The top three areas of risk were:
• Percentage of cephalosporins & Quinolones as a proportion of antibiotics prescribed
• Hypnotics • Cervical Cytology.
The practices and scores were named on the Care Quality Commission website. Four practices were in Band One (Princes Park, Dharmana, Syed & Priory Medical Centre) and Four in Band Two (Choudhary – Speke, Benim, Abercrombie and Brookes – Garston). It was stressed that the scorings were to determine visit priorities. The Primary Care Committee:
Noted the verbal update.
5. ANY OTHER BUSINESS
5.1 Neighbourhood Development Fund – it was noted that the interim version had been approved by the Finance Procurement & Contracting Committee that morning. The longer term proposal would be available in April 2015.
5.2 It was noted that an Informatics Merseyside paper was
being submitted to the Local Medical Committee on full access for District Nurses to GP records and had been well received so far.
6. DATE AND TIME OF NEXT MEETING
Page 11 of 12
169169169

Tuesday 30th December 2014 – 1pm to 3pm.
Page 12 of 12
170170170

Minutes of the Healthy Liverpool Programme – Leads Board Boardroom, Arthouse Square
Tuesday 9th December 2014 – 4pm
Present: Members Dr Nadim Fazlani Kathrine Sheerin Tom Jackson Prof Maureen Williams Dr Simon Bowers Dr Janet Bliss Dr Fiona Lemmens Dr Shamin Rose DrJim Cuthbert Dr Jude Mahadanaarachchi Dave Antrobus Dr Donal O’Donoghue Moira Cain Jane Lunt In Attendance: Dr Paula Finnety Ian Davies Derek Rothwell Tony Woods Kim McNaught Carole Hill Sue Lavell Jenny Levy Mark Horncastle Andrea Astbury Michelle Urwin Julie Byrne Apologies: Cheryl Mould Dr Maurice Smith Dr Roise Kaur Councillor Roz Gladden Kathy Hull
Chair / GP Chief Officer Chief Finance Officer Deputy Chair / Lay Member GP / Clinical Vice Chair GP GP GP GP / Matchworks Locality Chair GP / Liverpool Central Locality Chair Lay Member / Patient Engagement Secondary Care Doctor Practice Nurse Chief Nurse / Head of Quality GP / North Locality Chair Head of Operations and Corporate Performance Head of Contracts and Procurement Head of Strategy and Outcomes Deputy Chief Finance Officer Head of Communications Programme Office Manager Locality Development Manager PA Consulting (Agenda Item 3) Transformation Change Manager (Agenda Item 7) Transformation Change Manager (Agenda Item 4) PA / Minutes Head of Primary Care Quality & Improvement GP Governing Body Member GP Governing Body Member Liverpool City Council Executive Officer / Health Watch Liverpool Scrutiny
1
171171171
1.0
1.1
Welcome, Introductions and apologies Chair welcomed all and noted apologies as above. Introductions were made.
2.0
2.1
2.2
Minutes & Actions of the Meeting held on the 11 November 2014 There was one amendment from the minutes of the 11th November 2014 “Dave Antrobus was present”. The rest of the minutes were agreed as an accurate record of the meeting. The Board agreed all actions from the 11th November 2014 meeting had been met.
3.0
3.1
3.2
3.3
3.4
3.5
Programme Diagnostic Initial Feedback M Horncastle presented the initial diagnostic feedback to Board. A written report will be produced at the end of this week. Interviews with key internal senior management, key external stakeholders and partners had taken place and questionnaires have been completed. Recommendations were made in the following areas:
• Scope • Timeline • Stakeholders • Governance • Delivery • Assurance • Capacity and Capability
M Horncastle reviewed the conclusions and highlighted the next steps. A report will be finalised and shared with the senior management team to develop a high level mobilisation plan and diagnostic feedback. Chair said this would be discussed at the Governing Body session scheduled this Friday. D O’Donogue said that there was a need to expand the clinical forum and that a broad range of clinical input was required, who are the clinical leaders and do they get together to make the decision regarding conflicting clinical decisions. What is the best way to deliver the best clinical model, need to bring in the clinical groups with a whole system together.
2
172172172
4.0
4.1
4.2
4.3
Dementia Update M Urwin presented a paper on the re-design of dementia care in Liverpool. The purpose of the paper was to provide an overview of the plans to transform dementia services over the next 5 years and also to seek approval for the establishment of a Clinical Network for dementia and the development of new working practices. The Network is due to commence in January 2015. M Urwin reviewed the 7 areas that have been prioritised for action over the next 5 years. The Board approved the setup of the new Dementia Clinical Network. M Urwin stated that as plans advance business case will be developed and presented at a future Programme Leads meetings.
5.0
5.1
Priority List agreed at Governing Body Development Session Due to time constraint’s Board agreed to discuss this item at the Governing Body session scheduled this Friday.
6.0
6.1
Engagement Update
Again due to time constraints this agenda item was deferred to the January 2015 Board.
7.0
7.1
7.2
7.3
HLP – Investment Approvals
• Diabetes Proposal J Bliss and A Astbury presented a paper regarding the proposed project of an integrated community diabetes service. Aintree University Hospital, Royal Liverpool and Broadgreen University hospital and Liverpool Community Health are the providers and have worked collaboratively to establish a service model for the provision of an integrated community diabetes service. Providers had raised a risk relating to recruitment to posts prior to the proposal being approved at Governing body and prior to a contract being issued. T Jackson explained that this was an outcomes based contract acknowledged the risk for the Providers to get this up and running. M Williams added that it was not unreasonable to approve phase 1 and review the costs in principle. A letter of assurance from this Board to the Providers will be issued. This will support the proposal and will give
3
173173173
assurance that up to £100k of mobilisation costs will be covered if the proposal is not approved. The recommendation from HLP leads to the Governing body is for approval. S Bowers added that there was no other CCG in the country that was undertaking an outcome based contract and that it was fundamental to the Healthy Liverpool Programme.
8.0
8.1
Any Other Business
There was no other business.
9.0
9.1
Date and Time of Next Meeting
Tuesday 13th January 2014 – (Approx. 4.30pm – 6.30pm immediately after the Governing Body) - 4th Floor Boardroom, Arthouse Square
4
174174174
NHS LIVERPOOL CLINICAL COMMISSIONING GROUP FINANCE, PROCUREMENT AND CONTRACTING COMMITTEE (FPCC)
TUESDAY 16 DECEMBER 2014 9:30AM – 12.00NOON MEETING ROOM 2 - ARTHOUSE SQUARE
MINUTES Members Nadim Fazlani (NF) Chair Maureen Williams (MW) Lay Member Dave Antrobus (DA) Lay Member Maurice Smith (MS) GP – Governing Body Member Katherine Sheerin (KS) Chief Officer Tom Jackson (TJ) Chief Finance Officer Ray Guy (RG) Practice Manager In Attendance Derek Rothwell (DR) Head of Contracts and Procurement Kim McNaught (KM) Deputy Chief Finance Officer Alison Ormrod (AO) Chief Accountant Phil Saha (PS) Head of Programme Finance Ian Davies (ID) Head of Operations and Corporate Performance Peter Johnstone (PJ) Transformational Change Manager (Prescribing) Terese Clarke(TCl) Contracts and Procurement Manager Jayne Dickson (JD) Finance Intern (observer) Lynne Hill (LH) PA/Minute Taker Apologies Cheryl Mould (CM) Head of Primary Care Quality & Improvement Jane Lunt (JL) Head of Quality/Chief Nurse Tony Woods (TW) Head of Strategy and Outcomes Michelle Urwin (MU) Transformational Change Manager - Dementia Alison Picton (AP) Senior Contracts Manager Tim Cain (TC) Principle Analyst 1. Welcome and Introductions The Chair welcomed everyone to the meeting and introductions were made. 2. Declarations of Interest No declarations were made. 3. Minutes of the meeting held on 25th November 2014 A number of changes were suggested to the minutes and then agreed as a correct record.
1
175175175
3a Actions from the meeting held on 25th November 2014 Commissioning of Widening Access Psychological Therapies (WAPT) FPCC53-14 DR confirmed that as part of the contract the requirement for the review and evaluation of the contract at specific points will be detailed. Mersey Extended Rehabilitation (MER) pathway for Acquired Brain Injury (FPCC54-14) DR agreed to follow up with Michelle Urwin on the Southport Element of the pathway. STARS Programme (FPCC55-14) MU to present the financial update on the STARS programme to the January 2015 Finance Procurement and Contracting Committee. GP Specification KS stated that modifications to the GP Specification are taking place and will need to be presented to the January or February 2015 Finance Procurement and Contracting Committee. 4. Point of Prescribing Procurement (FPCC63-14) Peter Johnstone (PJ) talked through the Point of Prescribing procurement paper and that the purpose of the paper is to present to the Finance, Procurement and Contracting Committee the recommendations of a Medicines Management Committee working group for a preferred provider of Point of Prescribing intervention software. PJ confirmed that the original PCTs across the Merseyside area agreed a specification for the GP Support systems. In April 2014 an LCCG procurement waiver was agreed in respect of an extension to the current provider (Scriptswitch) until the CCG could proceed through the procurement process for a provider. The procurement process has now been completed (via an existing procurement framework) and the committee are asked to approve the recommendation to award First Databank Europe Ltd (Optimise Rx) as the provider of the Point of Prescribing system for general practice for the next 2 years. The Committee raised the following queries: RG asked if this has this been trialled and tested in other organisations or practices. PJ confirmed that it has been tested in Norfork practices and in 5 (five) practices in Liverpool and worked well and PJ is confident that it works to the specification. MW queried how the tender process takes into account social value. DR stated that this is a piece of software and therefore social value would not generally form part of
2
176176176
the procurement process when using a framework for software. PJ stated that both organisations are UK based but owned by American companies. MW commented that this raises the fundamental question that if we have a procurement policy that includes Social Value, and this does not meet that policy then we need to consider this for the future procurement activities. If social value is not in the criteria then it needs to be considered for the future but acknowledged that (for some procurements) the social value determinants may be extremely difficult to incorporate KS queried the costing and if this needs to be presented to the Governing Body due to the pricing. KM stated that she believed that this was a procurement and not a new investment and that the recurrent budget was already available and therefore no additional funding was required and thus does not need to be authorised through the Investment Approval Process. ID asked if there is an implementation cost, i.e. training needs for the 94 practices. PJ confirmed that there are no additional implementation costs as it is an easy transfer of knowledge to understand the new data system and involved a software update to the PCs that could be done remotely. MS confirmed that his practice has been a pilot site and his team have used the database and it is easy to use and supported the view that there were no additional implementation costs. The Committee further discussed the procurement process and if there is a requirement for this to be presented to the Governing Body. It was agreed that the recurrent budget was agreed already and therefore not required to be presented to the Governing Body as this is not a new investment but a variation to (albeit new) contract. The procurement route and new supplier will be reported to the GB via the feedback template (as per normal FPCC process). Action: Confirmation of Social Value element within our procurement
approach will require review for future procurement activities (DR). Action: NF to feedback to the Governing Body via the feedback sheet
The Committee noted the procurement process and recommended the
approval of the award of a 2 year contract to First Databank Europe Ltd.
5. Re-Procurement of BME Community Mental Health Services (FPCC64-14) Teresa Clarke(TCl) talked through the paper and gave the background of BME Mental Health Services and requested approval for the re-procurement of the BME community services via the recommended procurement route and that the 3 services are joined together to provide one service.
3
177177177
DA queried the appointment of the community representative and how this person will be chosen. TCl stated that Andy Woods, Programme Delivery Manager (Mental Health, (NWCSU), has been consulted and requested to recruit the appropriate person to inform the panel. KS queried the single provider option and should this state “lead provider”. TCl highlighted the current provider will maintain the service for a short period of time. MS stated that Option B will need to be changed to multiple contracts and the wording needs to be changed accordingly to acknowledge that change. TCl stated that Irish communities are mentioned as an individual service at the moment. This will be incorporated into the one service within the new procurement process. TJ noted that the clinical model does not appear to be significant in the paper and this will need to be reviewed for others that are presented to future Finance Procurement and Contracting Committees, additionally TJ stated that there should be officers or clinicians that lead for each procurement attending this meeting MW stated that she was unhappy with the contract from the onset, however a number of issues have been addressed in the current paper and believes the paper is fit for purpose, however still does not feel that the single provider/contract is going to address the main issues. It is still unclear if it is a mental health project or a community project and would be reluctant to commission this as it stands in the future, this therefore needs to be reviewed for future, but satisfied to continue for this procurement. KS commented that as we are going for a lead provider, then they (lead provider) could decide to sub-contract some elements of the service. MS queried how the service has been specified as this needs to reflect the new neighbourhood re-design model and should state how the providers will communicate with others within the neighbourhood model. TJ stated that the specification needs to bring out the real requirements for the service that is to be provided. With regard to current status, DR stated that a Procurement Information Notice (PIN) had been issued and that 5 organisations have declared an interest. DR stated that this BME will come back to the committee on one further occasion (outcome of ITT / recommended bidder award) as part of the procurement process . The Committee agreed that this is not new investment and therefore does not need to be presented to the Governing Body.
4
178178178

The Committee discussed the clinical input requirement before it is put before the Governing Body. KS stated that it needs to be presented to the Mental Health committee / meeting although KS recognised that this meeting is not a formal approval process. NF stated that this paper is presented from a recurrent budget line and therefore the Committee are not approving a new investment and the Investment Prioritisation Process and the normal budget process are separate. MW stated that this is not her understanding and will need to consider this for future, however it also needs to be explicit in the contract and papers submitted to the Finance Procurement and Contracting Committee. KM confirmed that the Investment Prioritisation Process was not set up to review what we currently spend (i.e. recurrent budgets) however we still need to agree 2015/16 budget. TJ suggested providing a development session for the Committee in relation to the recurrent budgets, non-recurrent and contracts for 2015/ 2016 and this can be fed back to the Governing Body. Action: TJ/KM - Budget Development Session Jan/February 2015.
NF stated that the Finance Procurement and Contracting Committee approved the procurement route and it has agreed a single or lead provider route, however the additional comments should be taken on board and the paper to be recirculated via email to agree the correct wording. Action: TCl agreed to change the documentation to reflect the
comments. . Action: Amendments to be made and paper to be re-circulated to the
FPCC members (DR/TCl). The Committee agreed that the service provider should link with the
neighbourhoods as well as other organisations (i.e. Merseycare) and should be included in the specification.
The Committee agreed the procurement as a single or lead provider
route. 6. HLP Investment Proposals Integrated Community Diabetes Service DR talked through the requirement for the Integrated Community Diabetes procurement and recommended a single tender action be approved for Aintree University Hospital as lead provider for a 15 month programme to start immediately
5
179179179
and finish in March 16. The contract value is £205k for 2014/15 and £912,372 for 2015/16. TJ stated that Aintree University Hospital have approved this in their Board meeting, however the Royal Liverpool and Broadgreen University Hospital and Liverpool Community Health Boards have not yet approved this. DR stated that there is a tripartite agreement as a prerequisite of the contract and requires full approval from all 3 provider parties, this has not yet been agreed . ID commented that the contract provision is conditional on all 3 parties’ agreement, therefore if this does not happen then we will then need to look for a market solution. KS commented that she supports the approach and this enables Liverpool CCG to assess if the providers are happy to work together on a pilot basis. KS also stated that this investment proposal will need to be presented to the Governing Body for approval MW agreed on the approach, however the only issue would be the robust evaluation and requested that any learning is acted upon during the procurement / market management period and during the pilot phase of the service provision. MS stated that he would also be an agreement on the evaluation of the clinical provision. DR commented that during the phase 1 period, it would be necessary to clearly identify the reasons and rationale for going / not going to market for an integrated Diabetes Service procurement and that this would form part of the usual procurement process. Action: DR to compile the rationale for going / not going to market for a
procurement for the FPCC by Q3 of 2015. The Committee agreed the recommended procurement route of a Single
Tender to Aintree University Hospital for the Integrated Community Diabetes Service.
7 Any Other Business 7.1 Timetable of Contract Reviews DA referred to a timetable of reviews of contracts for the next 12 months. DR stated that all current Acute, Community and Mental Health NHS standard contracts / providers are reviewed as part of the annual renegotiation of contracts. DR stated that he would work with LCCG colleagues (during Q1) to ensure that reviews are undertaken Action: DR to submit a timetable to the January 2015 FPCC
6
180180180
7.2 WAPT DR reported that South Sefton CCG contract for WAPT was awarded to Cheshire and Wirral Partnership and a letter of concern from the current Provider has been received by South Sefton CCG with comments relating to the procurement process. DR has reviewed the letter and is of the view that the concerns may not be applicable to the LCCG procurement process. KS enquired what would be the impact if a query was raised regarding the LCCG procurement process. DR talked through the response timetable if a similar letter is received by Liverpool CCG . 7.3 Finance Staff Development Network TJ informed the Committee of the recognition of the development and training work within the Finance Department by the NHS North West Finance Skills Development (FSD) Team. FSD operate an accreditation process to acknowledge and formally recognise good practice in finance skills development. Towards Excellence Level 1 was awarded to the Liverpool CCG Finance Team in 2013 and the application for Level 2 accreditation was successful and awarded in December 2014. Liverpool CCG Finance Team has been encouraged to apply for Level 3 Accreditation as their systems and practice are acknowledged as evidence of good practice. Level 2 Accreditation is only awarded to those organisations who are considered to be exemplary in their approach to finance skills development and to date there are less than ten organisations who have been recognised at this level across the North West. The Committee gave thanks to Phil Saha, Kim McNaught, Alison Ormrod
and the Finance Team for the successful achievement of Level 2 Accreditation
Date of next meeting Tuesday 27th January 2015, 10am – 12:30pm, Room 2, Arthouse Square.
7
181181181





























