Embed Size (px)
Citation preview

1
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
TEMA 13. HIPERSENSIBILIDAD
There are four types of hypersensitivity reaction. Type I mast cells bind IgE via their Fc receptors. On encountering allergen the IgE becomes cross-linked, in ducing degranulation and release ofmediators that produce allergic reactions. Type II anti body is directed against antigen on anindividual's own cells (target cell) or foreign antigen, such as transfused red blood cells. This may lead to cytotoxic action by K cells, or complement-media ted lysis. Type III immune complexes are deposited in the tissue. Complement is activated and poly morphs are attracted to the site ofdeposition, causing local tissue damage and inflammatio n. Type IV antigen-sensitized T cellsrelease lymphokines following a secondary contact with th e same antigen. Cytokines induce inflammatory reactions and activate and attract macrophag es, which release inflammatorymediators.
When a patient becomes 'allergic' to one of the well-recog nized sources of allergens, theyhave actually produced an IgE antibody response to one or mo re of the proteins that are produced by mites, trees, grass, cats or fungi. The pro teins are predominantly water soluble with a molecular weight (MW) ranging from 10 000 to 40 0 00 kDa. In many cases the functionof the proteins is known, but it is not clear whether functio n such as enzymic activity altersthe ability of these proteins to induce an allergic respons e. The properties of the particlescarrying these allergens are very important because they i nfluence both how much becomesairborne, and also where the allergen is deposited in the r espiratory tract. The dimensions ofthe particles airborne vary from ≤2 µm for Aspergillus or Penicillium spores to ≥20 µm formite faecal pellets and some pollen grains (sizes are given as diameter in micrometres).
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

2
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
The IgE molecule has four heavy chain constant regions. Th ebinding sites for the high-affinity IgE receptor Fc εRI, and forthe low-affinity receptor Fc εRII, or CD-23 are shown. Monoclonal antibodies to the binding site for Fc εRI also blockFcεRII.
The serum concentration of IgE(which is around 100thinsp;IU/ml) is only ∼∼∼∼0.001% that of IgG(around 10thinsp;mg/ml) andcomprises less than 0.001% ofthe total immunoglobulin. Levelsin atopic patients tend to be raised, and this is especially so in atopic eczema (1thinsp;IU = 2.4thinsp;ng). (2) The higher thelevel of IgE the smaller thepercentage of the populationaffected, but the greater thelikelihood of atopy. Where thelevel is greater than450thinsp;IU/ml the majority ofsubjects are atopic.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
3
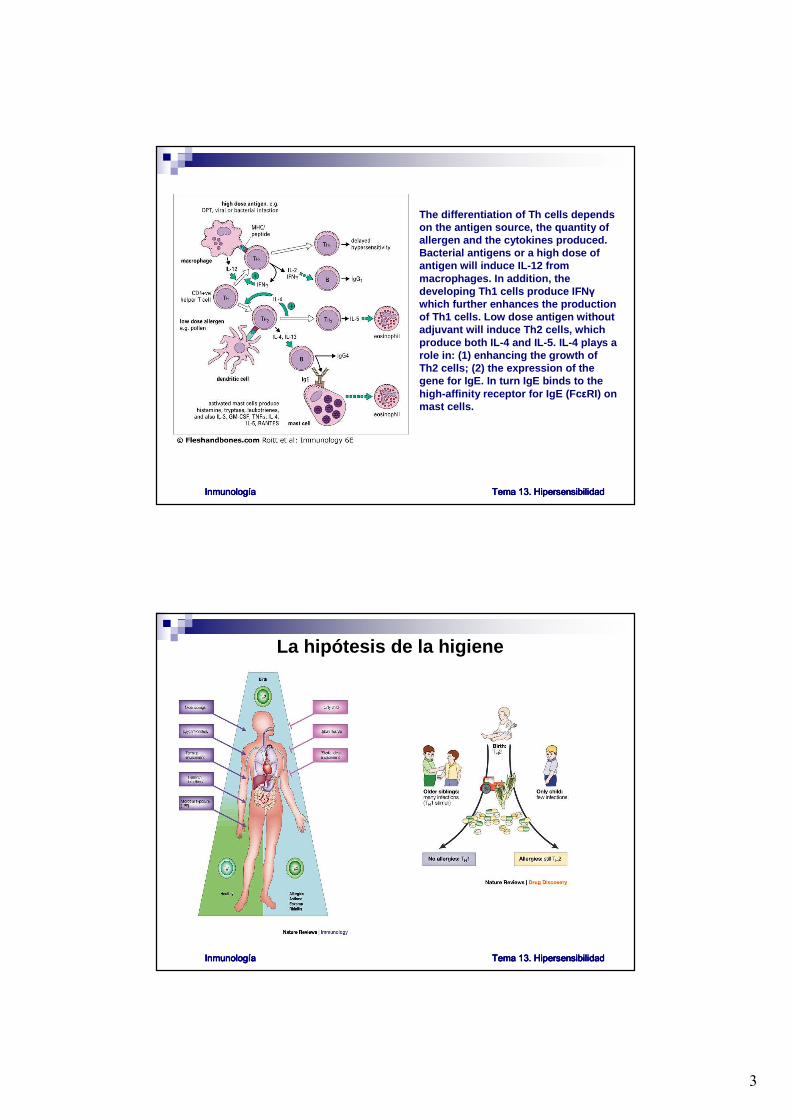
The differentiation of Th cells dependson the antigen source, the quantity ofallergen and the cytokines produced. Bacterial antigens or a high dose ofantigen will induce IL-12 frommacrophages. In addition, thedeveloping Th1 cells produce IFN γ
which further enhances the productionof Th1 cells. Low dose antigen withoutadjuvant will induce Th2 cells, whichproduce both IL-4 and IL-5. IL-4 plays a role in: (1) enhancing the growth ofTh2 cells; (2) the expression of thegene for IgE. In turn IgE binds to thehigh-affinity receptor for IgE (Fc εRI) onmast cells.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
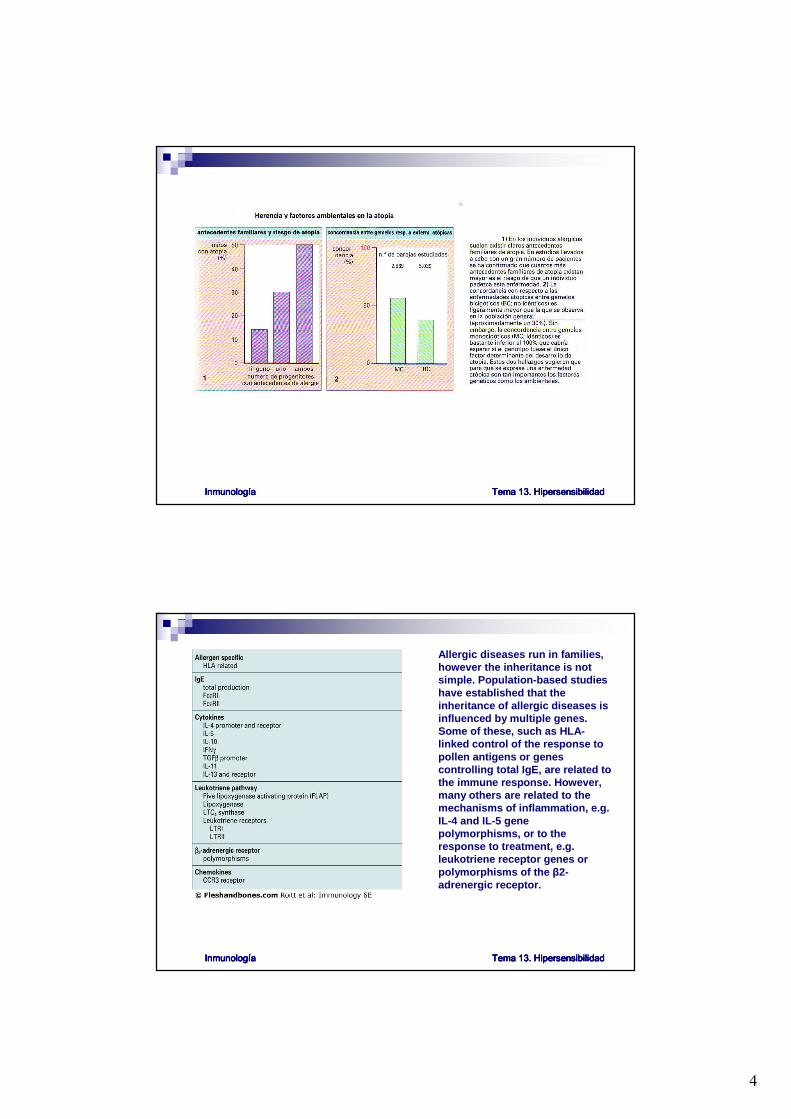
La hipótesis de la higiene
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
4
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Allergic diseases run in families, however the inheritance is notsimple. Population-based studieshave established that theinheritance of allergic diseases isinfluenced by multiple genes. Some of these, such as HLA-linked control of the response topollen antigens or genes controlling total IgE, are related tothe immune response. However, many others are related to themechanisms of inflammation, e.g. IL-4 and IL-5 gene polymorphisms, or to theresponse to treatment, e.g. leukotriene receptor genes orpolymorphisms of the β2-adrenergic receptor.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

5
There are at least two subpopulations of mast cells, themucosal mast cells (MMCs) and the connective tissuemast cells (CTMCs). The differences in their morphologyand pharmacology suggest different functional roles in vivo. MMCs are associated with parasitic worminfections and, possibly, allergic reactions. In cont rast tothe CTMC, the MMC is smaller, shorter lived, T-celldependent, has more Fc ε receptors and containsintracytoplasmic IgE. Both cells contain histamine andserotonin in their granules; the higher histamine conten tof the CTMC may be accounted for by the greaternumber of granules. Major arachidonic acid (AA) metabolites (prostaglandins and leukotrienes) are produced by both mast-cell types, but in differentamounts. For example, the ratios of production of theleukotriene LTC4 to the prostaglandin PGD2 are 25 1 in the MMC and 1 40 in the CTMC. The effect of drugs ondegranulation is different between the two cell types. Sodium cromoglycate (DSCG) and theophylline bothinhibit histamine release from the CTMC but not from theMMC. (This may have important implications in thetreatment of asthma.) Note that many of these data come from rodent studies and may not apply to humans. Tryptase is a tetramer of 134thinsp;kDa which may comprise as much as 25% of the mast-cell protein. Chymase is a monomer of 30thinsp;kDa. The relativeproportions of these proteases in mast cells define MCtand MCtc populations, which have different distributionsin human tissues. Basophils have very low amounts ofboth proteases. (The suffixes t and tc represent tryptaseand chymase present in the respective cells.)
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

6
Mast cells release mediators aftercross-linking of the IgE receptorson their surface. Preformedmediators are released rapidly whilearachidonic acid metabolites suchas leukotriene D4 and prostaglandinD2 are released more slowly. Mastcells can also be triggered by opiates, contrast media, vancomycin and the complementcomponents C3a and C5a. Themediators which are also releasedby basophils include histamine, TNFα and IL-4. Histamine releasedby mast cells can be measured in serum following anaphylaxis orextensive urticaria, but it has a half-life in minutes. By contrast, tryptase can be measured in serumfor many hours after ananaphylactic reaction.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

7
Skin tests are carried out by introducing 0.02thinsp;ml of extract intradermally. With allergens such as pollen, cat or dust mite, the positive reaction is an imme diate (i.e. within 20 min) wheal, which in somecases is followed by an indurated response occurring lat e (i.e. at 4-12 hours). Non-allergic individualsmake no discernable reaction to testing with these allerge ns. A delayed skin response is thecommonest form of positive response to tuberculin, teta nus and mumps, or to fungi such as Trichophyton and Candida. The skin typically shows no reaction up to 12 hours and t hen graduallydevelops an erythematous indurated, delayed hypersensit ivity response, which is maximum at 24-48 hours. Patch tests are performed by applying a gauze pad with allergen to a patch of skin which has been mildly abraided. This procedure may give an immediat e wheal response, but this is followed at 24-48 hours by an indurated, erythematous response, which has many of the features of eczema. The patchtest is not a diagnostic test but has provided extensive in formation about the role of allergens in atopicdermatitis.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Mast cells release factors that can induce immediate bron chospasm, e.g. histamine and LTD4, but alsorelease chemotactic factors such as LTB4, IL-5 and TNF α. The spasmogens can induce oedema, increased mucus and smooth muscle constriction resulting in immediate decrease in airwayconductance and a fall in the forced expiratory volume at 1 second (FEV1). By contrast, chemotacticfactors recruit cells out of the circulation including eos inophils, neutrophils, lymphocytes andmacrophages. These cells can chronically modify the lung with goblet cell hyperplasia, collagendeposition below the basement membrane and possibly smooth muscle hyperplasia. In addition, thesecells and their products produce non-specific bronchial h yper-reactivity (BHR). Thus, chronicbronchospasm includes elements of hypersecretion, infla mmatory infiltrate thickening the walls of thesmall bronchi and bronchial smooth muscle spasm. Evidence for this inflammatory response can be obtained from increased exhaled nitric oxide (eNO); incr eased eosinophils or ECP in induced sputum; and experimentally from biopsies of the lung. neutrophils = 1; basophils = 2; eosinophils = 3; monocytes = 4.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

8
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Effector cells - K cells, platelets, neutrophils, eosinophils, and cells of themononuclear phagocyte series - all have receptors for Fc, which they use to engageantibody bound to targettissues. Activation ofcomplement C3 can generatecomplement-mediated lyticdamage to target cells directly, and also allows phagocyticcells to bind to their targetsvia C3b, C3bi or C3d, whichalso activate the cells.
HIPERSENSIBILIDAD TIPO II
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

9
Neutrophil-mediated damage is a reflection of normal antibacterialaction. (1) Neutrophils engagemicrobes with their Fc and C3 receptors. (2) The microbe is thenphagocytosed and destroyed as lysosomes fuse to form thephagolysosome (3). In Type II hypersensitivity reactions, individual host cells coated with antibody may be similarly phagocytosed, but wherethe target is large, for example a basement membrane (I), theneutrophils are frustrated in theirattempt at phagocytosis (II). Theyexocytose their lysosomal contents, causing damage to cells in thevicinity (III).
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Not all blood groups are equallyantigenic in transfusion reactions: thus, RhD evokes a stronger reactionin an incompatible recipient than theother Rhesus antigens; and Fya isstronger than Fyb. Frequenciesstated are for Caucasian populations- other races have different gene frequencies.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

10
The diagram shows how the ABO blood groups are constructed. Theenzyme produced by the H gene attaches a fucose residue (Fuc) to theterminal galactose (Gal) of theprecursor oligosaccharide. Individualspossessing the A gene now attach N-acetylgalactosamine (NAGA) to thisgalactose residue, while those with theB gene attach another galactose, producing A and B antigens, respectively. People with both genes make some of each. The tableindicates the genotypes and antigensof the ABO system. Most peoplenaturally make antibodies to theantigens they lack. NAG = N-acetylglucosamine.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Note that blood group epitopesbased on carbohydrate moieties, such as ABO and Ii (expressed onthe precursor of the ABO polysaccharide), can appear onmany different proteins, includingRh antigens. Antigens such as Rhesus and Duffy are proteins, so the epitope only appears on onetype of molecule. In general, themost important blood groupantigens are present at high levelson the erythrocytes, thus providingplenty of targets for complement-mediated lysis or Fc receptor-mediated clearance.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
11
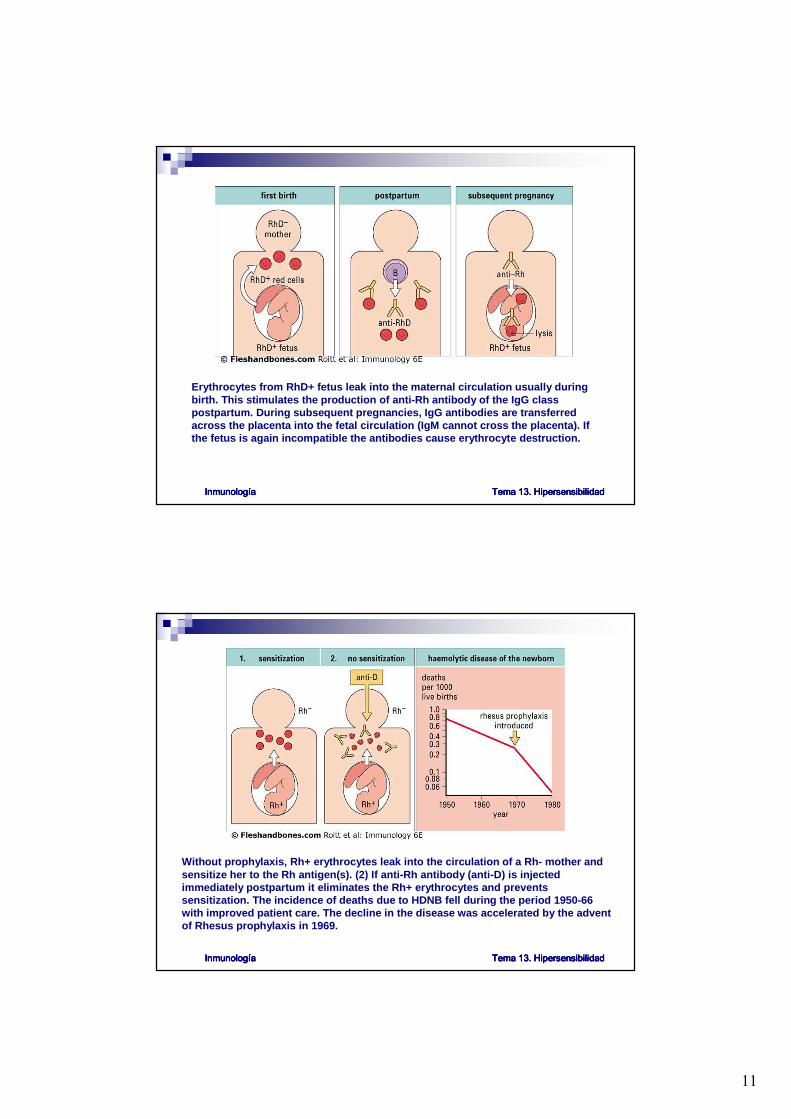
Erythrocytes from RhD+ fetus leak into the maternal circu lation usually duringbirth. This stimulates the production of anti-Rh antibody of the IgG classpostpartum. During subsequent pregnancies, IgG antibod ies are transferredacross the placenta into the fetal circulation (IgM canno t cross the placenta). Ifthe fetus is again incompatible the antibodies cause eryt hrocyte destruction.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Without prophylaxis, Rh+ erythrocytes leak into the circ ulation of a Rh- mother andsensitize her to the Rh antigen(s). (2) If anti-Rh antibod y (anti-D) is injectedimmediately postpartum it eliminates the Rh+ erythrocyte s and preventssensitization. The incidence of deaths due to HDNB fell du ring the period 1950-66 with improved patient care. The decline in the disease wa s accelerated by the adventof Rhesus prophylaxis in 1969.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
12
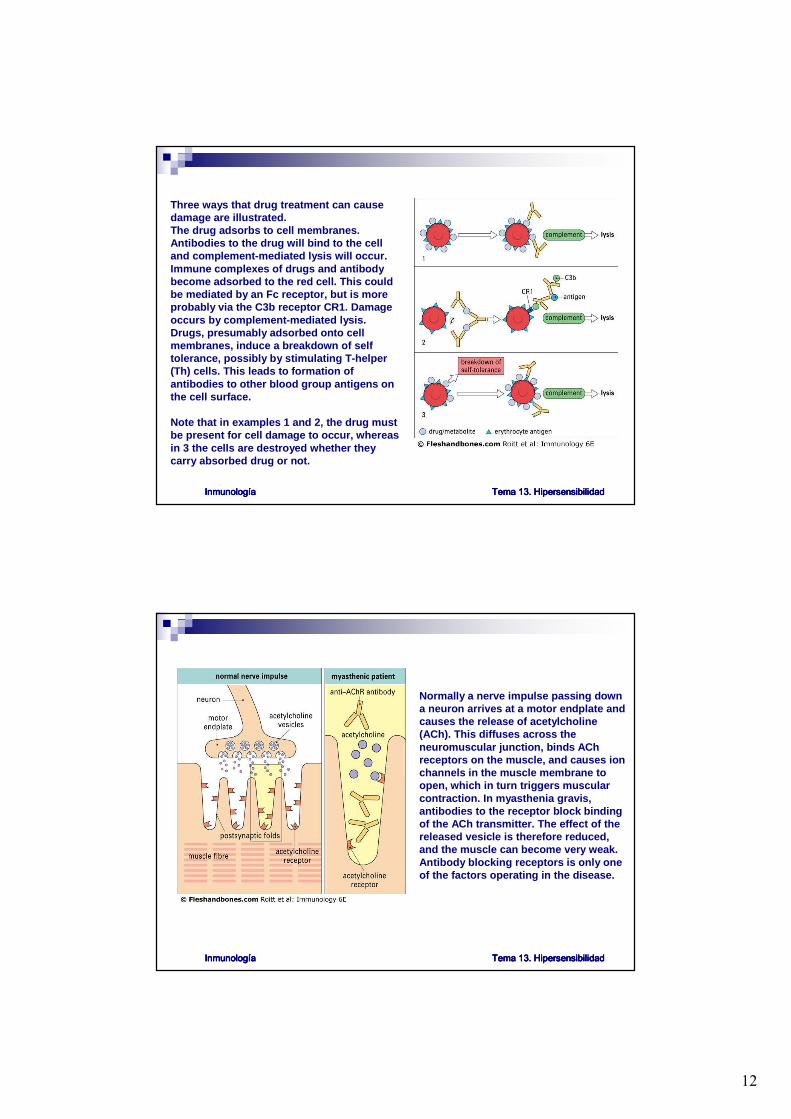
Three ways that drug treatment can cause damage are illustrated. The drug adsorbs to cell membranes. Antibodies to the drug will bind to the celland complement-mediated lysis will occur. Immune complexes of drugs and antibodybecome adsorbed to the red cell. This couldbe mediated by an Fc receptor, but is more probably via the C3b receptor CR1. Damageoccurs by complement-mediated lysis. Drugs, presumably adsorbed onto cellmembranes, induce a breakdown of selftolerance, possibly by stimulating T-helper(Th) cells. This leads to formation ofantibodies to other blood group antigens onthe cell surface.
Note that in examples 1 and 2, the drug mustbe present for cell damage to occur, whereasin 3 the cells are destroyed whether theycarry absorbed drug or not.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Normally a nerve impulse passing downa neuron arrives at a motor endplate andcauses the release of acetylcholine(ACh). This diffuses across theneuromuscular junction, binds AChreceptors on the muscle, and causes ionchannels in the muscle membrane toopen, which in turn triggers muscular contraction. In myasthenia gravis, antibodies to the receptor block bindingof the ACh transmitter. The effect of thereleased vesicle is therefore reduced, and the muscle can become very weak. Antibody blocking receptors is only oneof the factors operating in the disease.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

13
HIPERSENSIBILIDAD TIPO III
This table indicates the source of the antigen and the organs most frequently affected.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
When fungal antigen is inhaled into the lung of a sensitized individual, immunecomplexes are formed in the alveoli (2). Complement fixa tion leads to cell accumulation, inflammation and fibrosis. The histological appearance o f the lung in extrinsic allergicalveolitis (1) shows consolidated areas due to cell accumu lation. Precipitin antibodypresent in the serum of a patient with pigeon fancier's lun g: P (3) is directed against thefungal antigen Micro-polyspora faeni. Anormal serum (N) lacks antibodies to this fungus.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

14
Immune complexes normally bindcomplement and are removed to theliver and spleen after binding to CR1 on RBC. In inflammation, immunecomplexes act on basophils andplatelets (in humans) to produce vasoactive amine release. Theamines released (e.g. histamine, 5-hydroxytryptamine) cause endothelial cell retraction and thusincrease vascular permeability.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
In primates, complexes solubilized by complement are bound by CR1 on erythrocytes and transported tothe liver where they are removed by hepatic macrophages. Complexesreleased from erythrocytes by Factor I are taken up by cells(including macrophages) bearingreceptors for Fc and complement.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

15
Increased vascular permeability allows immunecomplexes to be deposited in the blood vessel wall. This induces platelet aggregation and complementactivation. The aggregated platelets formmicrothrombi on the exposed collagen of thebasement membrane of the endothelium. Neutrophils are attracted to the site by complementproducts, but cannot ingest the complexes. Theytherefore exocytose their lysosomal enzymes, causing further damage to the vessel wall.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
A bolus of immune complexeswas infused into the circulationof a primate. In animals with a normal complement system thecomplexes were bound quicklyby the CR1 on erythrocytes. In animals whose complement hadbeen depleted by treatment withcobra venom factor, theerythrocytes hardly boundimmune complexes at all. Paradoxically, this results in slightly faster removal ofcomplexes in the depletedanimals, with the complexesbeing deposited in the tissuesrather than being removed by the spleen.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

16
Complement can solubilize precipitable complexes in vitro. Addition of fresh serum containingactive complement to insoluble complexes induces solub ilization over about 15 minutes at 37°C. Some of the complexes resist resolubilization. Heated ser um (56°C for 30 minutes) lacks active complement and cannot resolubilize the complexes. Interc alation of complement componentsC3b and C3d into the complex causes their solubilization by disrupting antigen-antibody bonds. Complexes that have been artificially connected by covale nt bonds cannot be solubilized by complement.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Large immune complexes are cleared most quickly because th ey present an IgG-Fc lattice tomononuclear phagocytes cells with Fc receptors, permitti ng higher avidity binding to these cells. They also fix complement better than small complexes.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

17
Factors that affect complex deposition include filtration and high blood pressure, both of whichoccur in the formation of ultrafiltrate in the renal glom erulus (1). Turbulence at curves orbifurcations of arteries (2) also favours deposition of im mune complexes.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Contact and tuberculin-type hypersensitivity have a simi lar time course andare maximal at 48-72 hours. In certain circumstances (e .g. with insoluble antigen) granulomatous reactions also develop at 21-28 d ays (e.g. skintesting in leprosy).
HIPERSENSIBILIDAD TIPO IV
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

18
The hapten forms a hapten-carriercomplex in the epidermis. Langerhans' cells internalize theantigen, undergo maturation, andmigrate via afferent lymphatics tothe paracortical area of theregional lymph node wherepeptide/MHC complexes on thesurface of the Langerhans' cell can also be directly haptenated. As interdigitating cells, they presentantigen to CD4+ T cells.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
Langerhans' cells carrying the hapten-carriercomplex (1) move from the epidermis to thedermis, where they present the hapten-carriercomplex to memory CD4+ T cells (2). ActivatedCD4+ T cells release IFN γ, which induces expression of ICAM-1 (3) and, later, MHC class II molecules (4) on the surface of keratinocytes andon endothelial cells of dermal capillaries andactivates keratinocytes which releaseproinflammatory cytokines such as IL-1, IL-6 andGM-CSF (5). Non-antigen-specific CD4+ T cells are attracted to the site by cytokines (6) and may bindto keratinocytes via ICAM-1 and class II molecules. Activated macrophages are also attracted to theskin, but this occurs later. Thereafter the reactionstarts to downregulate. This downregulation may be influenced by eicosanoids such as PGE, produced by activated keratinocytes andmacrophages (7).
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

19
Cytokines and prostaglandins are central to thecomplex interactions between Langerhans' cells, CD4+ T cells, keratinocytes, macrophages andendothelial cells in contact hypersensitivity. Theact of antigen presentation (1) causes the releaseof a cascade of cytokines (2). This cascade initiallyresults in the activation and proliferation of CD4+ T cells (3), the induction of expression of ICAM-1 andMHC class II molecules on keratinocytes andendothelial cells (4), and the attraction of further T cells and macrophages to the skin (3, 5). Subsequent PGE production by keratinocytes andmacro-phages may have an inhibitory effect on IL-1 and IL-2 production. Production of PGE, binding ofactivated T cells to keratinocytes and enzymaticand cellular degradation of the hapten- carriercomplex all contribute to the downregulation of thereaction.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
This diagram illustrates cellularmovements following intradermalinjection of tuberculin. Within 1-2 hours there is expression of E-selectinon capillary endothelium leading to a brief influx of neutrophil leucocytes. By 12 hours ICAM-1 and VCAM-1 onendothelium bind the integrins LFA-1 and VLA-4 on monocytes andlymphocytes, leading to accumulationof both cell types in the dermis. Thispeaks at 48 hours and is followed by expression of the HLA class II molecules on keratinocytes. There isno oedema of the epidermis.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad

20
Bacterial products stimulatemacrophages to secrete IL-12. Activation of T cells in the presenceof IL-12 leads to the release of IFN γ
and other cytokines, lymphotoxin(LT), IL-3, and GM-CSF. Thesecytokines activate macrophages tokill intracellular parasites. Failure toeradicate the antigenic stimuluscauses persistent cytokine releaseand promotes differentiation ofmacrophages into epithelioid cellswhich secrete large amounts of TNF α. Some fuse to form multinucleategiant cells.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad
The characteristics of Type IV reactions comparing contac t, tuberculin andgranulomatous reactions.
InmunologInmunologInmunologInmunologíííía a a a Tema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. HipersensibilidadTema 13. Hipersensibilidad





























