Embed Size (px)
Citation preview

THE OFFICIAL CME PUBLICATION OF THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Volume 30 Number 3 March 2016
Lumbar puncture (LP) is used in the diagnostic evaluation of central nervous system (CNS) processes, most commonly in cases of suspected infection and subarachnoid hemorrhage. Less commonly, the procedure is used for therapeutic purposes (eg, in cases of idiopathic intracranial hypertension).
Primetime ViewingAll resuscitative efforts ultimately will fail if the patient cannot be adequately oxygenated and ventilated. There is a rapidly growing body of evidence to support the use of video laryngoscopy for the management of both routine and difficult airways. Emergency physicians, in particular, must understand the design and clinical applications of this burgeoning technology.
Tectonic PlateletsThrombocytopenia can be a benign incidental finding, or an ominous sign of a more serious disease process. Emergency physicians must be able to discern dangerous from innocuous clinical conditions caused by low platelet counts, and understand how the etiology of each case can help guide diagnostic testing and the initiation of lifesaving treatments.

Contributor Disclosures. In accordance with the ACCME Standards for Commercial Support and policy of the American College of Emergency Physicians, all individuals with control over CME content (including but not limited to staff, planners, reviewers, and authors) must disclose whether or not they have any relevant financial relationship(s) to learners prior to the start of the activity. These individuals have indicated that they have a relationship which, in the context of their involvement in the CME activity, could be perceived by some as a real or apparent conflict of interest (eg, ownership of stock, grants, honoraria, or consulting fees), but these individuals do not consider that it will influence the CME activity. Sharon E. Mace, MD, FACEP; Baxter Healthcare, consulting fees, fees for non-CME services, and contracted research; Gebauer Company, contracted research; Halozyme, consulting fees. Joshua S. Broder, MD, FACEP; GlaxoSmithKline; his wife is employed by GlaxoSmithKline as a research organic chemist. All remaining individuals with control over CME content have no significant financial interests or relationships to disclose.
Method of Participation. This educational activity consists of two lessons, a post-test, and evaluation questions; as designed, the activity it should take approximately 5 hours to complete. The participant should, in order, review the learning objectives, read the lessons as published in the print or online version, and complete the online post-test (a minimum score of 75% is required) and evaluation questions. Release date April 1, 2016. Expiration date March 31, 2019.
Accreditation Statement. The American College of Emergency Physicians is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
The American College of Emergency Physicians designates this enduring material for a maximum of 5 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Each issue of Critical Decisions in Emergency Medicine is approved by ACEP for 5 ACEP Category I credits. Approved by the AOA for 5 Category 2-B credits.
Commercial Support. There was no commercial support for this CME activity.Target Audience. This educational activity has been developed for emergency physicians.
Critical Decisions in Emergency Medicine is a trademark owned and published monthly by the American College of Emergency Physicians, PO Box 619911, Dallas, TX 75261-9911. Send address changes and comments to Critical Decisions in Emergency Medicine, PO Box 619911, Dallas, TX 75261-9911, or to [email protected]; call toll-free 800-798-1822, or 972-550-0911.
Copyright 2016 © by the American College of Emergency Physicians. All rights reserved. No part of this publication may be reproduced, stored, or transmitted in any form or by any means, electronic or mechanical, including storage and retrieval systems, without permission in writing from the Publisher. Printed in the USA.
The American College of Emergency Physicians (ACEP) makes every effort to ensure that contributors to its publications are knowledgeable subject matter experts. Readers are nevertheless advised that the statements and opinions expressed in this publication are provided as the contributors’ recommendations at the time of publication and should not be construed as official College policy. ACEP recognizes the complexity of emergency medicine and makes no representation that this publication serves as an authoritative resource for the prevention, diagnosis, treatment, or intervention for any medical condition, nor should it be the basis for the definition of, or standard of care that should be practiced by all health care providers at any particular time or place. Drugs are generally referred to by generic names. In some instances, brand names are added for easier recognition. Device manufacturer information is provided according to style conventions of the American Medical Association. ACEP received no commercial support for this publication.
To the fullest extent permitted by law, and without limitation, ACEP expressly disclaims all liability for errors or omissions contained within this publication, and for damages of any kind or nature, arising out of use, reference to, reliance on, or performance of such information.
Lesson 5 n Thrombocytopenia . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
LLSA Literature Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Critical Procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Critical ECG . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Lesson 6 n Video Laryngoscopy . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Critical Image . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
CME Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
Drug Box/Tox Box . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24
Critical Decisions in Emergency Medicine is the official CME publication of the American College of Emergency Physicians. Additional volumes are available to keep emergency medicine professionals up to date on relevant clinical issues.
EDITOR-IN-CHIEFLouis G. Graff, IV, MD, FACEP
University of Connecticut, Farmington, CT [email protected]
EDITOR-ELECTMichael S. Beeson, MD, MBA, FACEP
Northeastern Ohio Universities, Rootstown, OH
SECTION EDITORSJ. Stephen Bohan, MD, MS, FACEP
Brigham & Women’s Hospital/Harvard Medical School, Boston, MA
Joshua S. Broder, MD, FACEP Duke University, Durham, NC
Amal Mattu, MD, FACEP University of Maryland, Baltimore, MD
Lynn P. Roppolo, MD, FACEP University of Texas Southwestern Medical Center,
Dallas, TX
Christian A. Tomaszewski, MD, MS, MBA, FACEP University of California Health Sciences, San Diego, CA
Steven J. Warrington, MD Kaweah Delta Medical Center, Visalia, CA
ASSOCIATE EDITORSWalter L. Green, MD, FACEP
University of Texas Southwestern Medical Center, Dallas, TX
John C. Greenwood, MD University of Pennsylvania, Philadelphia, PA
Daniel A. Handel, MD, MPH, FACEP Medical University of South Carolina, Charleston, SC
Frank LoVecchio, DO, MPH, FACEP Maricopa Medical Center/Banner Phoenix Poison
and Drug Information Center, Phoenix, AZ
Sharon E. Mace, MD, FACEP Cleveland Clinic Lerner College of Medicine/Case
Western Reserve University, Cleveland, OH
Jennifer L. Martindale, MD SUNY Downstate Medical Center/
Kings County Hospital Center, Brooklyn, NY
Robert A. Rosen, MD, FACEP University of Virginia, Charlottesville, VA
George Sternbach, MD, FACEP Stanford University Medical Center, Stanford, CA
Kathleen Wittels, MD Brigham & Women’s Hospital/
Harvard Medical School, Boston, MA
RESIDENT EDITORNathaniel Mann, MD
University of Cincinnati Medical Center, Cincinnati, OH
EDITORIAL STAFFRachel Donihoo, Managing Editor
[email protected] Hamilton, Educational Products Assistant
Lexi Schwartz, Subscriptions CoordinatorMarta Foster, Director, Educational Products
ISSN2325-0186(Print) ISSN2325-8365(Online)
n Nerve Blocks
n Concussion
I N T H I S I S S U E
N E X T M O N T H

March 2016 n Volume 30 Number 3 3
FROM THE EM MODEL8.0 Hematologic Disorders
8.2.3 Platelet Disorders
8.2.3.1 Thrombocytopenia
LESSON 5
By Rebecca A. Merrill, MD, and Tyler Gillen, MDDr. Merrill is the associate emergency medicine program director, and Dr. Gillen is an emergency medicine resident at Akron General Medical Center in Akron, Ohio.
Reviewed by Michael S. Beeson, MD, MBA, FACEP
n How can the etiology of a patient’s disorder help guide the treatment of thrombocytopenia?
n What physical and laboratory examination findings should raise concern for thrombocytopenia?
n What treatments should be initiated in the emergency department for patients with thrombocytopenia?
n Can asymptomatic patients be safely discharged for outpatient follow up?
n When should platelets be administered?
CRITICAL DECISIONSOBJECTIVESOn completion of this lesson, you should be able to:
1. Identify the various mechanisms of acquired thrombocytopenia.
2. Detail appropriate laboratory tests that should be initiated in the emergency department.
3. Explain the treatment options for the most common mechanisms of thrombocytopenia.
4. Identify which patients can be safely discharged for outpatient management.
5. Identify which patients require platelet transfusions.
Thrombocytopenia
Thrombocytopenia commonly is discovered in the emergency department in one of two ways. It may be an incidental finding on a workup for unrelated pathology or the primary culprit behind a patient’s symptomatic presentation. The emergency physician must be able to discern between dangerous and innocuous clinical conditions caused by the disorder, and immediately begin the appropriate diagnostic and treatment process.
Techtonic Platelets

Critical Decisions in Emergency Medicine4
CASE PRESENTATIONS■ CASE ONE
A 44-year-old woman presents with weakness, nausea, and vomiting that has persisted for 2 days. She visited the emergency department yesterday, and was discharged with a diagnosis of gastroenteritis; however, she now has returned with worsening symptoms.
The patient’s husband states she has been “out of it.” She normally is a healthy individual and takes no medications. On physical examination, the patient is ill appearing. Vital signs are blood pressure 115/75, heart rate 105, respiratory rate 18, temperature 38.3°C (100.9°F), and oxygen saturation 96% on room air. A HEENT examination is normal. The heart and lungs are unremarkable. A petechial rash is found on her back and lower extremities with no edema present.
■ CASE TWOA 34-year-old woman with
no medical history presents with gums that have been bleeding for the last 2 days. She has been taking trimethoprim/sulfmethoxazole for 10 days to treat a urinary tract infection, but states that she otherwise feels fine. She denies a fever, nausea/vomiting, and diarrhea.
Vital signs are blood pressure 135/79, pulse rate 83, respiration rate 14, temperature 37.4°C (99.3°F), and oxygen saturation 98% on room air. On physical examination, active gingival bleeding is noted; and an inspection of the patient’s legs reveals petechiae.
Thrombocytopenia, which is defined by a platelet count below 100,000 to 150,000 per microliter, can be an isolated condition due to a single mechanism, or the result of a syndrome caused by multiple factors. The risk of spontaneous bleeding usually does not become problematic until platelet counts drop below 20,000.
Acquired thrombocytopenia can be sorted into four categories: decreased platelet production, increased platelet destruction, platelet loss, and splenic sequestration. Examples of decreased production include marrow infiltration, viral infection, drugs, radiation, and vitamin B12/folate deficiencies. Increased platelet destruction may be the result of immune thrombocytopenic purpura, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, or disseminated intravascular coagulation.
Bleeding patterns frequently associated with platelet pathology include petechiae and mucosal bleeding. Emergency physicians must be able to recognize various presentations of thrombocytopenia and be capable of stabilizing and starting the diagnostic process in these patients.
CRITICAL DECISIONHow can the etiology of a patient’s disorder help guide the treatment of thrombocytopenia?
The presentation of thrombo-cytopenia differs depending on its various etiologies and the patient populations in which it occurs (Figure 1). In children, for example, immune thrombocytopenia (ITP) usually results in an acute process that occurs a few days or weeks after a viral illness. In adult patients, however, ITP often is a chronic condition without preceding illness. ITP is a diagnosis of exclusion; patients should demonstrate normal values in the other cell lines.
Thrombotic thrombocytopenic purpura (TTP) and hemolytic uremic syndrome (HUS) share some similarities, including fever and renal failure; however, there are distinct differences between the two conditions. HUS, which is more common in the pediatric population, often is preceded by bloody diarrhea and is associated with infection by Escherichia coli O157:H7, which produces the Shiga toxin.1 Its diagnostic characteristics
include autoimmune hemolysis, renal failure, and thrombocytopenia. In contrast, TTP tends to occur in adults and has a broader symptomatology. The disease is defined by hemolytic anemia, renal failure, and thrombocytopenia, as well as fever and neurologic abnormalities. The five symptoms do not always occur together, and not all are required for diagnosis.
Because TTP poses a significant risk of morbidity and mortality if left untreated, it is important to maintain a low threshold for suspicion. One predisposing factor is decreased ADAMTS13 activity, which can be acquired or caused by a mutation of the gene that codes for the enzyme (Upshaw Schulman syndrome).
The gene cleaves ultra-large von Willbrand (vWF) factor multimers into smaller, less adhesive proteins.2 These large multimers cause platelet aggregation, which diminishes the available platelets. In one large report, only 7% of patients with severe ADAMTS13 deficiency demonstrated all five symptoms within the 2-week window of initial presentation.3 Patients with this condition may develop TTP when stressed or exposed to infection.
■ CASE THREEA 5-year-old boy is brought in by
his concerned mother at the urging of the patient’s pediatrician, after the results of a routine CBC revealed a platelet count of 30,000/mm3. The boy was diagnosed with influenza 2 weeks earlier, but today he is afebrile and does not show any other symptoms. He is active and playful in the examination room.
Vital signs are blood pressure 100/65, heart rate 105, respiratory rate 24, and oxygen saturation 98% on room air. The heart, lung, and HEENT examinations are unremarkable, and the child’s abdomen is soft and nontender. His skin is dry, warm, and without a rash or lesions.

March 2016 n Volume 30 Number 3 5
Drug-induced thrombocytopenia (DIT) occurs in a minimum of 10 patients per million per year.4 Many of these cases are caused by increased platelet destruction, often via an immune-mediated mechanism.5 The disorder usually occurs 1 to 2 weeks after the start of a new drug or immediately after restarting a drug the patient previously has taken.
Common medications associated with thrombocytopenia include penicillin, β-lactams, sulfonamides, fluoroquinolones, quinine, ganciclovir, linezolid, and rifampin (Table 1). The symptoms should begin to resolve a few days after the medication is ceased. Chronic alcohol abuse also can cause thrombocytopenia, and usually resolves after the patient stops using the substance.
Heparin-induced thrombocytopenia can occur following the administration of heparin (less commonly, low-molecular-weight heparin). The mechanism is different than other drug-induced thrombocytopenia in that antibodies form against complexes of platelet factor 4 (PF4) and heparin, inducing platelet activation and aggregation.
Disseminated intravascular
coagulopathy (DIC) is an acquired syndrome prompted by the inappropriate activation of the coagulation system, which results in the formation of intravascular fibrin. The fibrinolytic system simultaneously is in full swing, breaking down fibrin clots and consuming the coagulation factors. Situations in which DIC can occur include sepsis, trauma, and cancer. Patient presentations may include ecchymoses, petechiae, hematuria, bleeding from surgical or venipuncture sites, multiple organ failure, gangrene, and purpura.6
CRITICAL DECISIONWhat physical and laboratory examination findings should raise concern for thrombocytopenia?
Patients with thrombocytopenia may present with symptoms such as bruising, petechiae, and epistaxis; or more serious symptoms, including purpura and bleeding from the gums or nose, gastrointestinal or urinary tract bleeding, or pulmonary hemorrhage.5 The initial clinical evaluation should entail a thorough history, including details on drug use, new medications, travel, and family history.
Initial laboratory evaluations should involve a complete blood count (CBC), basic metabolic panel (BMP), peripheral blood smear, and coagulation studies (Table 2). The CBC will reveal whether thrombocytopenia is an isolated finding, or if other cell lines are affected. A peripheral blood smear will indicate if a low platelet count is due to clumping — a finding that can lead to a falsely low reading.
The smear also will allow for a morphology evaluation of the cell lines, including platelets and red and white blood cells. Schistocytes, which may be seen in cases of DIC and TTP, are created when red blood cells are sheared as they pass between fibrin strands attached to a thrombus. A BMP may reveal an increased blood urea nitrogen or creatinine.
Indirect bilirubin will be elevated if hemolysis is present. If anemia is identified, a reticulocyte count should be ordered to assess whether the patient’s body is attempting to compensate for the deficiency of red blood cells. If the thrombocytopenia is the only pathology present, coagulation studies should be normal. In HUS and TTP, LDH and haptoglobin tests also should be administered.
FIGURE 1. Common Causes of Thrombocytopenia
Courtesy of Viral Thakerar, MD
Decreased Production
1. Bone marrow dysfunction
2. Inadequate hematinics
Increased Destruction
1. Immune thrombocytopenia (primary or secondary)
2. Hypersplenism3. MAHA* (eg, TTP, HUS)
Increased Consumption
1. Disseminated intravascular coagulation (DIC)
2. Bleeding
Mixed Etiology
1. Infections2. Drugs — esp. alcohol and heparin
3. Pregnancy (gestational thrombocytopenia, HELLP)
THROMBOCYTOPENIA(platelet count <50 x 10^9/L)
*Microangiopathic hemolytic anemia
Critical Decisions in Emergency Medicine6
CRITICAL DECISION What treatments should be initiated in the emergency department for patients with thrombocytopenia?
Urgent treatment is not necessary for most patients with ITP, unless there is serious hemorrhage or a need for surgery. The emergency department management of ITP should include methylprednisolone (30 mg/kg/day over 20 to 30 minutes) with a maximum dose of 1 g/day, and IV immunoglobulin (1 g/kg/day for 2 to 3 days).9 Oral prednisone (1 to 1.5 mg/kg) can be used in place of methylprednisolone.
Platelet transfusions should be avoided except in cases of serious bleeding. In such patients, the required platelet dose should be 2 to 3 times greater than the usual amount needed.9 Anti-D immune globulin is a good alternative to prednisone in Rh-positive patients; however, it is more expensive.10 Splenectomy may be required if treatment with steroids and immunoglobulin cannot maintain platelet counts in the acceptable range.
Heparin or low-molecular-weight heparin should be stopped immediately in cases of HIT. These patients are at an increased risk for significant thrombosis and should be treated with a nonheparin anticoagulant such as a direct thrombin inhibitor (eg, bivalirudin or argatroban)8. Platelet transfusions should be avoided because HIT antibodies can activate the
administered platelets and provoke thrombosis.11
The treatments for HUS and TTP are different, despite their similar presentations. For children with HUS, the treatment is mainly supportive, with possible dialysis in cases of severe or persistent renal failure. TTP, on the other hand, requires active management. Current guidelines state that a microangiopathic hemolytic anemia with thrombocytopenia and without an alternative explanation is sufficient to diagnose and treat TTP.12
Plasma exchange, which is the treatment of choice in TTP, should be initiated without delay. It should include a 17-gauge needle for withdrawal and a 18-gauge intravenous catheter for return of plasma.12 A central venous catheter also should be placed due to the likely need for multiple procedures.13 Cryosupernate is preferred as an
exchange fluid over fresh frozen plasma.14 High-dose corticosteroids such as methylprednisolone should accompany daily plasma exchanges.12 Aspirin is required when platelet counts rise above 50 x 109/L.12
Another treatment option is rituximab, which may lead to system improvement within weeks of the first dose in patients with autoimmune-mediated TTP who have frequent relapses or failed plasma exchange therapy.15
The treatment for HUS includes hydration, accompanied by electrolyte replacement when needed. Patients with severe renal disease may require dialysis.16 Antibiotic therapy rarely is required in the treatment of diarrhea-associated HUS; however, antibiotics may be needed in cases that are associated with streptococcal infection.17 Hematology should be consulted with HUS, particularly when TTP is suspected.
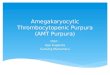
TABLE 1. Drugs Commonly Implicated as Triggers of Drug-Induced Thrombocytopenia24
n A patient with thrombocytopenia and neurological symptoms has TTP until proven otherwise.
n Patients with TTP rarely present with the symptomatic pentad of fever, thrombocytopenic purpura, renal disease, anemia, and neurologic symptoms.
n A hematology consultation is warranted in cases of suspected HUS or TTP.
n Children with isolated thrombocytopenia may be discharged and monitored, as long as their platelet counts are >30,000mm3.
Drug Category Drugs Implicated in Five or More Reports
Heparins Unfractionated heparin, low-molecular-weight heparin
Cinchona alkaloids Quinine, quninidine
Platelet inhibitors Abciximab, eptifibatide, tirofiban
Antirheumatic agents Gold salts D-penicillamine
Antimicrobial agents Ganciclovir, linezolid, rifampin, sulfonamides, vancomycin
Sedatives and anticonvulsant agents Carbamazepine, phenytoin, valproic acid Diazepam
Histamine-receptor antagonists Cimetidine Ranitidine
Analgesic agents Acetaminophen, diclofenac, naproxen Ibuprofen
Diuretic agents Chlorothiazide Hydrochlorothiazide
Chemotherapeutic and immune-suppressant agents Fludarabine, oxaliplatin Cyclosporine, rituximab
March 2016 n Volume 30 Number 3 7
The main treatment for DIT is discontinuation of the inciting drug. Evidence to support other treatments is lacking. One study on vancomycin-induced thrombocytopenia found that treatment with platelet transfusions, corticosteroids, intravenous immune globulin, plasma exchange, and anti-Rh immune globulin did not increase in platelet counts until the vancomycin was removed.18
CRITICAL DECISION Can asymptomatic patients be safely discharged for outpatient follow-up?
Treatment generally is required if signs of bleeding are present with a platelet count <50,000 mm3, or if platelets are <20,000 to <30,000 mm3.7 ITP and drug-induced thrombocytopenia are the two most common etiologies of isolated cases. The symptoms of ITP tend to be less severe in children than in adults; 70% of pediatric cases resolve within 6 months, regardless of treatment.19
Adult patients, on the other hand, are more likely to be admitted for further workup. Platelet counts greater than 30,000 mm3 without serious symptoms generally can be managed with observation.19 If thrombocytopenia is an isolated incidental finding in the emergency department and the patient’s platelet count is >50,000 mm3 with no signs of bleeding, the patient can be safely discharged home.7 Those with thrombocytopenia not related to ITP or drug-induced thrombocytopenia should be admitted for further workup and treatment.
According to American Society of Hematology guidelines,20 pediatric
patients generally do not require hospitalization if their platelet counts are greater than 30,000 mm3. Children should receive IV immunoglobulin or corticosteroids if their platelet counts are less than 20,000 mm3 with significant bleeding, or less than 10,000 mm3 with no or minimal bleeding.20
CRITICAL DECISIONWhen should platelets be administered?
Platelet transfusion should be avoided unless there is serious bleeding or the need for a surgical procedure. Although a 1981 study linked the death of a patient to a platelet transfusion given for TTP,
more recent research asserts that the procedure provides neither benefit nor harm.21,22
It is appropriate, however, to administer platelets for patients with severe thrombocytopenia and overt bleeding, and in the setting of a major invasive procedure.17 These patients
should receive platelets at a rate that is 2 to 3 times higher than the usual dose.
The 2010 international consensus report on ITP, which recommends further investigation in patients older than 60 years, warns that isolated thrombocytopenia may be the initial abnormality of a myelodysplastic syndrome.23
SUMMARYThrombocytopenia can be a benign
incidental finding, or an ominous sign of a more serious disease process. Clinicians must be prepared to initiate a diagnostic investigation and treatment in the emergency department. Platelet administration should be held except in cases of life-threatening bleeding or the need for a lifesaving surgical procedure.
The first-line treatment for ITP in adults is steroids; in children, the disease process usually can be managed with observation alone. In cases of drug-in-duced thrombocytopenia, removal of the
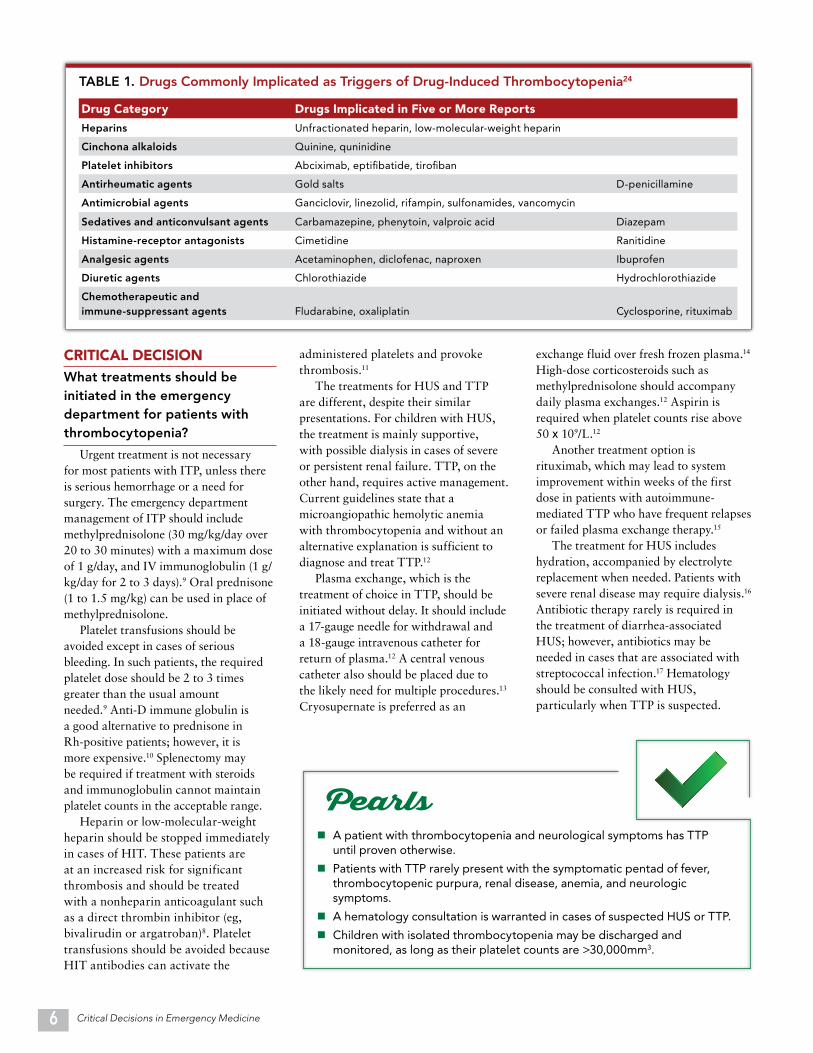
TABLE 2. Laboratory Values Indicative of Thrombocytopenia
n Administering platelets for the routine management of thrombocytopenia. This treatment is only warranted in cases of life-threatening bleeding or the need for surgery.
n Failing to remove the offending agent in cases of drug-induced thrombocytopenia.
n Dismissing the risks of low-molecular-weight heparin, which can lead to heparin-induced thrombocytopenia (although it is less likely to do so than heparin).
n Treating diarrhea-associated HUS with antibiotics. (Antibiotics are only warranted in cases of streptococcal-associated HUS.)
Etiology PT, aPTT Platelets Fibrinogen D-Dimer Other FeaturesITP Normal Decreased Normal Normal Normal RBC
TTP-HUS Normal Decreased Normal Normal Schistocytes
DIC Prolonged Decreased Decreased Elevated Schistocytes
Liver disease ProlongedNormal to decreased
Normal to decreased
Normal to mild elevation
Stigmata of liver disease
Massive transfusion/trauma
Prolonged Decreased Decreased Normal Hypothermia, acidosis
PT = prothrombin time; aPTT = activated partial thromboplastin time.

Critical Decisions in Emergency Medicine8
CASE RESOLUTIONS■ CASE ONE
The febrile, confused woman’s new symptoms were concerning upon her return visit to the emergency department.
A chest radiograph was unremark-able and revealed no source for the fever. The patient’s laboratory work revealed a platelet level of 28,000 mm3 and a hemoglobin of 8.8 g/dL. The only abnormalities discovered on the BMP were a potassium level of 5.1 mEq/L, creatinine 1.45, and BUN 30 mg/dL. The UA was normal.
The astute physician ordered a blood smear, lactate dehydrogenase, direct Coombs test, coagulation profile, and haptoglobin and liver function tests. The blood smear was remarkable for schistocytes; lactate dehydrogenase was elevated at 400 IU/L; bilirubin was slightly elevated at 2.5 mg/dL; and haptoglobin was below the normal reference range.
Given the laboratory values, which indicated hemolytic anemia with a thrombocytopenia, the clinician suspected TTP and arranged for a
offending agent is the only true treatment option.
The primary treatment for TTP is plasmapheresis. HUS usually can be managed with supportive care, which may include hemodialysis if renal failure is present. A hematology consultation should be initiated early to avoid serious complications.
REFERENCES 1. Nangaku M, Nishi H, Fujita T. Pathogenesis and
prognosis of thrombotic microangiopathy. Clin Exp Nephrol. 2007;11(2):107-114.
2. Tsai HM. Mechanisms of microvascular thrombosis in thrombosis in thrombotic thrombocytopenic purpura. Kidney Int Suppl. 2009;(112):S11-S14.
3. George JN, Chen Q, Deford CC, Al-Nouri Z. Ten patient stories illustration the extraordinarily diverse clinical features of patients with thrombotic thrombocytopenic purpura and severe ADAMTS13 deficiency. J Clin Apher. 2012;27(6):302-311.
4. van den Bemt PM, Meyboom RH, Egberts AC. Drug-induced immune thrombocytopenia. Drug Saf. 2004;27(15):1243-1252.
5. Aster RH, Bougie DW. Drug-induced immune thromb-ocytopenia. N Engl J Med. 2007;357(6):580-587.
6. Blaisdell FW. Causes, prevention, and treatment of intravascular coagulation and disseminated
intravascular coagulation. J Trauma Acute Care Surg. 2012;72(6):1719-1722.
7. Santen SA, Hemphill RR. Chapter 228. Acquired Bleeding Disorders. In: Tintinalli J, Kelen GD, Stapczynski JS, eds. Tintinalli’s Emergency Medicine. 7th ed. New York, NY: McGraw-Hill; 2011:1464-1470.
8. Hurwitz A, Massone R, Lopez BL. Acquired bleeding disorders. Emerg Med Clin North Am. 2014;32(3):691-713.
9. Cines DB, Blanchette VS. Immune thrombocytopenic purpura. N Engl J Med. 2002;346(13):995-1008.
10. Newman GC, Novoa MV, Fodero EM, et al. A dose of 75 g/kg/d of i.v. anti-D increases the platelet count more rapidly and for a longer period of time than 50g /kg/d in adults with immune thrombocytopenia purpura. Br J Haematol. 2001;112(4);1076-1078.
11. Warkentin TE. Heparin-induced thrombocytopenia. Hematol Oncol Clin North Am. 2007;21(4):589-607.
12. Kessler CS, Khan BA, Lai-Miller K. Thrombotic thrombocytopenic purpura: a hematological emergency. J Emerg Med. 2012;43(3):538-544.
13. Binder WD, Traum AZ, Makar RS, Colvin RB. Case records of the Massachusetts General Hospital. Case 37-2010. A 16-year-old girl with confusion, anemia, and thromcocytopenia. N Engl J Med. 2010;363(24):2352-2361.
14. Allford SL, Hunt BJ, Rose P, et al. Guidelines on the diagnosis and management of the thrombotic microangiopathic haemolytic anaemias. Br J Haematol. 2003;120(4):556-573.
15. Elliott MA, Heit JA, Pruthi RK, et al. Rituximab for refractory and or relapsing thrombotic thrombocytopenic purpura related to immune-mediated severe ADAMTS13-deficiency: a report of
plasma exchange. Two large-bore
IVs and a central line were placed,
high-dose methylprednisolone was
administered, and hematology was
consulted regarding admission and
further treatment.
■ CASE TWOThe previously healthy woman with
bleeding gums and a petechial rash on
her lower extremities was evaluated
with a workup that included CBC and
BMP tests, coagulation studies, and a
hepatic panel. The CBC results were
within normal limits, except for a
platelet count of 16,000 mm3. The BMP
and coagulation studies were within
normal limits.
An isolated drug-induced
thrombocytopenia was diagnosed, and
the patient was admitted for observation.
Her symptoms were believed to have
been triggered by the TMP/sulfa
antibiotic she was taking for a urinary
tract infection. No further treatment
was required. (Removal of the offending
agent is sufficient therapy for DIT.)
■ CASE THREEThe 5-year-old boy posed a difficult
diagnostic challenge for the emergency physician. The patient appeared well and did not show any signs of disease; however, HUS was a concern.
Laboratory studies revealed a platelet count of 33,000 mm3 and a hemoglobin of 12.4 g/dL; bilirubin was within the normal reference range; and kidney function and lactate dehydrogenase were both within normal limits.
The child was diagnosed with ITP, likely secondary to the viral illness he had 2 weeks earlier. Since his platelet count was above the 30,000 mm3 threshold, he could be discharged safely.
The patient’s mother was told to follow up with the pediatrician in a few days for a repeat CBC, and was instructed to return to the emergency department if her son experienced bleeding from any site that would not stop. Although medications were not immediately indicated, the mother was advised that hospitalization and treatment with IV immunoglobulin or corticosteroids might be required if the boy’s platelet count dropped below 20,000 mm3.
four cases and systematic review of the literature. Eur J Haematol. 2009;83(4):365-372.
16. Salvadori M, Bertoni E. Update on hemolytic uremic syndrome: diagnostic and therapeutic recommendations. World J Nephrol. 2013;2(3):56-76.
17. George JN, Al-Nouri ZL. Diagnostic and therapeutic challenges in the thrombotic thrombocytopenic purpura and hemolytic uremic syndromes. Hematology Am Soc Hematol Educ Program. 2012;2012:604-609.
18. Von Drygalski A, Curtis BR, Bougie DW, et al. Vancomycin-induced immune thrombocytopenia. N Engl J Med. 2007;356(9):904-910.
19. Cines DB, Blanchette VS. Immune thrombocytopenic purpura. N Engl J Med. 2002;346(13):995-1008.
20. Tarantino MD, Bolton-Maggs PH. Update on the management of immune thrombocytopenic purpura in children. Curr Opin Hematol. 2007;14(5):526-534.
21. Harkness DR, Byrnes JJ, Lian EC, et al. Hazard of platelet transfusion in thrombotic thrombocytopenic purpura. JAMA. 1981;246(17):1931-1933.
22. Swisher KK, Terrell DR, Vesely SK, et al. Clinical outcomes after platelet transfusions in patients with thrombotic thrombocytopenic purpura. Transfusion. 2009;49(5):873-887.
23. Provan D, Stasi R, Newland AC, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115(2):168-186.
24. Aster RH, Curtis BR, McFarland JG, et al. Drug-induced immune thrombocytopenia: pathogenesis, diagnosis, and management. J Thromb Haemost. 2009;7(6):911-918.
March 2016 n Volume 30 Number 3 9
Small bowel obstruction (SBO) is a common clinical diagnosis in the emergency department. Two percent of patients who present with abdominal pain will have an SBO, as will 15% of those admitted to a surgical unit.
The diagnosis most frequently is secondary to adhesions from prior abdominal surgery. Other causes include neoplasms, hernias, and Crohn’s disease. The risk of serious complications such as strangulation and bowel necrosis is high; it is essential to diagnose SBO early.
Although abdominal pain is present in most cases of SBO, no other components of a patient’s history can reliably and accurately predict the diagnosis. However, some studies indicate that a history of prior SBO coupled with abdominal pain might serve as a reliable predictor for a subsequent obstruction. Abnormal bowel sounds and abdominal pain with constipation also may indicate SBO. Abdominal distension is the most reliable physical examination finding for predicting the disorder.
Diagnostic modalities that can be used to evaluate for SBO include radiography, computerized tomography (CT),
Adult Small Bowel ObstructionTaylor M, Lalani, N. Acad Emerg Med. 2013;20(6):528-544
The LLSA Literature Review
Critical Decisions in Emergency Medicine’s series of LLSA reviews features articles articles from ABEM’s 2016 Lifelong Learning and Self-Assessment Reading List. Available online at acep.org/llsa and on the ABEM website.
Reviewed by J. Stephen Bohan, MS, MD, FACEP
n Causes of small bowel obstruction include adhesions, neoplasms, hernias, and Crohn’s disease; adhesions are the most common.
n Abdominal pain plus constipation or a history of prior SBO increases the likelihood of obstruction.
n Physical examination findings suggestive of SBO include abdominal distension and decreased bowel sounds.
n CT scan is the most sensitive and specific diagnostic modality for making this diagnosis. With appropriate training, however, an emergency medicine practitioner can accurately diagnose an SBO using ultrasound.
KEY POINTS
magnetic resonance imaging (MRI), and ultrasound (US). Plain radiography is the least reliable modality; an SBO on x-ray is characterized by dilated loops of bowel and air fluid levels.
CT has high sensitivity and specificity for small bowel obstruction, particularly when using 64-slice cuts. An SBO on CT is characterized by dilated loops of bowel proximal to decompressed loops (also known as a transition point).
The diagnostic findings on US are similar to those found on CT; however,
absent or decreased peristalsis also needs to be present to confirm SBO on ultrasound. Although ultrasonography provides diagnostic accuracy, its effectiveness relies, in part, on the training and skill level of the operator. Of note, US is unable to pinpoint the transition point or etiology of an SBO.
MRI offers diagnostic accuracy, but is less optimal than other imaging modalities given its limited availability and the increased time required to perform the test. The diagnostic criteria of MRI are similar to those of CT.
By Erika Phindile Chowa, MD, and Kathleen Wittels, MD Harvard Affiliated Emergency Medicine Residency, Brigham and Women’s Hospital/Massachusetts General Hospital, Boston, MA
ILLU
ST
RA
TIO
N C
OU
RT
ESY
OF
CLE
AR
PA
SSA
GE
Critical Decisions in Emergency Medicine10
The emergency practitioner generally
can remove a corneal foreign body
with a simple procedure as long as
the patient is cooperative and the
irritant is uncomplicated (ie, not deeply
embedded and without signs of globe
perforation).
CORNEAL FOREIGN BODY REMOVAL
By Steven J. Warrington, MDDr. Warrington is a core faculty member of the general surgery and emergency medicine residency programs, and the associate medical director for emergency department outreach and education at Kaweah Delta Medical Center in Visalia, California.
The Critical Procedure
CONTRAINDICATIONSn Intraocular foreign body
n Concern for globe penetration/perforation
n Multiple foreign bodies (relative, as this can result in scarring if a large portion of the corneal epithelium is removed)
n Deeply embedded foreign body (relative, as removal poses a risk of globe injury/penetration)
Risks and BenefitsIn experienced hands, corneal foreign body removal poses little risk when performed on a cooperative patient in a controlled environment. The most significant danger is iatrogenic globe perforation/penetration, which can occur when attempting to remove a deeply embedded object. There is a potential for scarring when a large area of corneal
March 2016 n Volume 30 Number 3 11
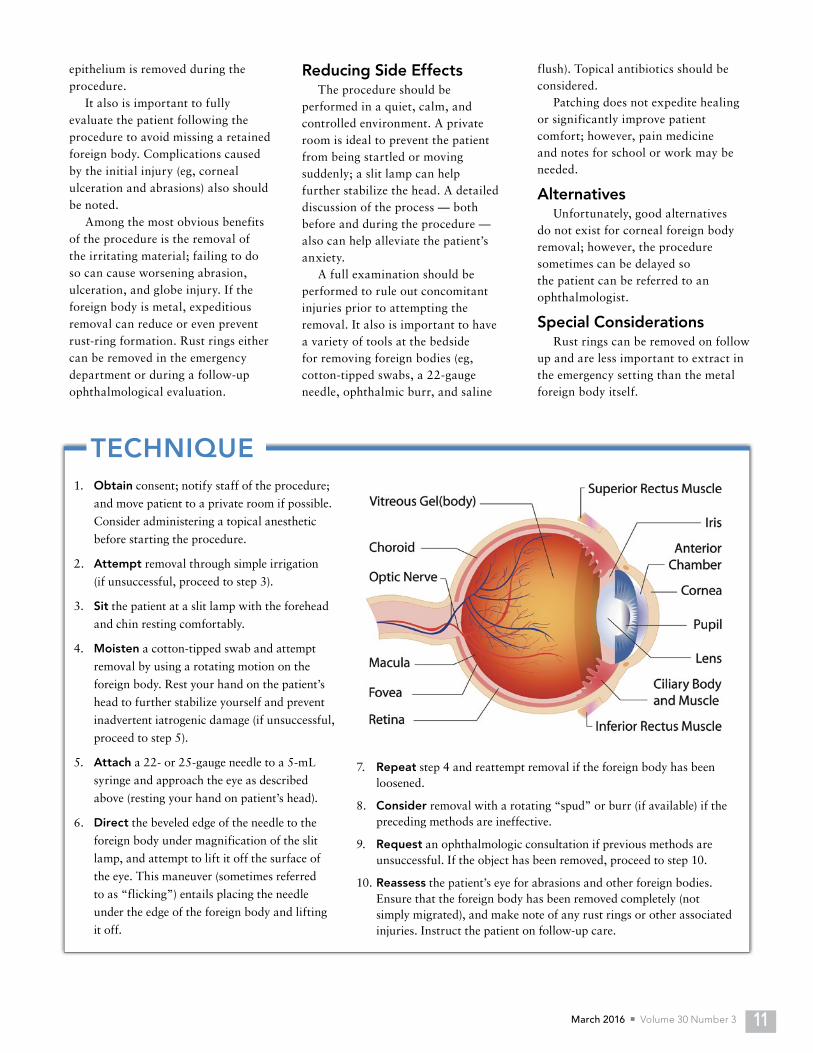
1. Obtain consent; notify staff of the procedure;
and move patient to a private room if possible.
Consider administering a topical anesthetic
before starting the procedure.
2. Attempt removal through simple irrigation
(if unsuccessful, proceed to step 3).
3. Sit the patient at a slit lamp with the forehead
and chin resting comfortably.
4. Moisten a cotton-tipped swab and attempt
removal by using a rotating motion on the
foreign body. Rest your hand on the patient’s
head to further stabilize yourself and prevent
inadvertent iatrogenic damage (if unsuccessful,
proceed to step 5).
5. Attach a 22- or 25-gauge needle to a 5-mL
syringe and approach the eye as described
above (resting your hand on patient’s head).
6. Direct the beveled edge of the needle to the
foreign body under magnification of the slit
lamp, and attempt to lift it off the surface of
the eye. This maneuver (sometimes referred
to as “flicking”) entails placing the needle
under the edge of the foreign body and lifting
it off.
TECHNIQUE
7. Repeat step 4 and reattempt removal if the foreign body has been loosened.
8. Consider removal with a rotating “spud” or burr (if available) if the preceding methods are ineffective.
9. Request an ophthalmologic consultation if previous methods are unsuccessful. If the object has been removed, proceed to step 10.
10. Reassess the patient’s eye for abrasions and other foreign bodies. Ensure that the foreign body has been removed completely (not simply migrated), and make note of any rust rings or other associated injuries. Instruct the patient on follow-up care.
epithelium is removed during the procedure.
It also is important to fully evaluate the patient following the procedure to avoid missing a retained foreign body. Complications caused by the initial injury (eg, corneal ulceration and abrasions) also should be noted.
Among the most obvious benefits of the procedure is the removal of the irritating material; failing to do so can cause worsening abrasion, ulceration, and globe injury. If the foreign body is metal, expeditious removal can reduce or even prevent rust-ring formation. Rust rings either can be removed in the emergency department or during a follow-up ophthalmological evaluation.
Reducing Side EffectsThe procedure should be
performed in a quiet, calm, and controlled environment. A private room is ideal to prevent the patient from being startled or moving suddenly; a slit lamp can help further stabilize the head. A detailed discussion of the process — both before and during the procedure — also can help alleviate the patient’s anxiety.
A full examination should be performed to rule out concomitant injuries prior to attempting the removal. It also is important to have a variety of tools at the bedside for removing foreign bodies (eg, cotton-tipped swabs, a 22-gauge needle, ophthalmic burr, and saline
flush). Topical antibiotics should be considered.
Patching does not expedite healing or significantly improve patient comfort; however, pain medicine and notes for school or work may be needed.
AlternativesUnfortunately, good alternatives
do not exist for corneal foreign body removal; however, the procedure sometimes can be delayed so the patient can be referred to an ophthalmologist.
Special ConsiderationsRust rings can be removed on follow
up and are less important to extract in the emergency setting than the metal foreign body itself.
Critical Decisions in Emergency Medicine12
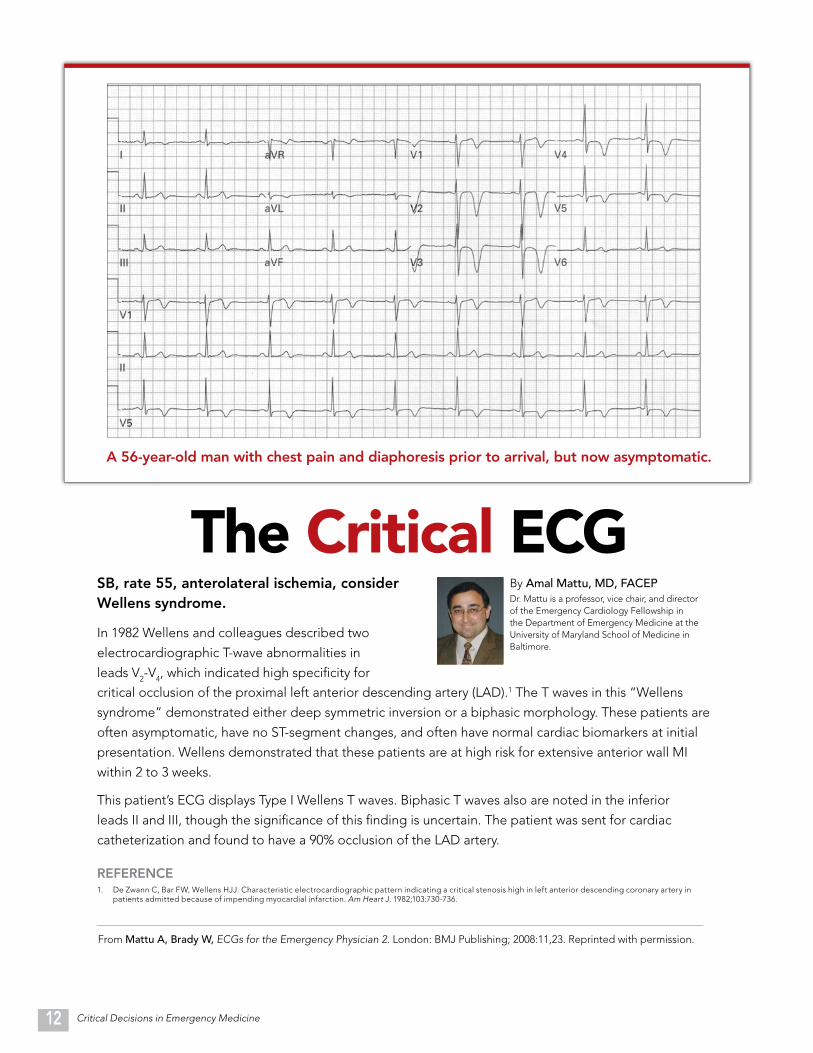
A 56-year-old man with chest pain and diaphoresis prior to arrival, but now asymptomatic.
The Critical ECGSB, rate 55, anterolateral ischemia, consider Wellens syndrome.
In 1982 Wellens and colleagues described two
electrocardiographic T-wave abnormalities in
leads V2-V4, which indicated high specificity for
From Mattu A, Brady W, ECGs for the Emergency Physician 2. London: BMJ Publishing; 2008:11,23. Reprinted with permission.
By Amal Mattu, MD, FACEPDr. Mattu is a professor, vice chair, and director of the Emergency Cardiology Fellowship in the Department of Emergency Medicine at the University of Maryland School of Medicine in Baltimore.
critical occlusion of the proximal left anterior descending artery (LAD).1 The T waves in this “Wellens
syndrome” demonstrated either deep symmetric inversion or a biphasic morphology. These patients are
often asymptomatic, have no ST-segment changes, and often have normal cardiac biomarkers at initial
presentation. Wellens demonstrated that these patients are at high risk for extensive anterior wall MI
within 2 to 3 weeks.
This patient’s ECG displays Type I Wellens T waves. Biphasic T waves also are noted in the inferior
leads II and III, though the significance of this finding is uncertain. The patient was sent for cardiac
catheterization and found to have a 90% occlusion of the LAD artery.
REFERENCE1. De Zwann C, Bar FW, Wellens HJJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in
patients admitted because of impending myocardial infarction. Am Heart J. 1982;103:730-736.
March 2016 n Volume 30 Number 3 13
FROM THE EM MODEL19.0 Procedures and Skills Integral to the Practice of Emergency Medicine
19.4 Diagnostic and Therapeutic Procedures
19.4.4 Head, Ear, Eye, Nose, and Throat
LESSON 6
By Samuel Kim, MD, Calvin A. Brown III, MD and Alexander Y. Sheng, MDDr. Kim is an emergency medicine resident at Boston University Medical Center in Boston, Massachusetts. Dr. Brown is assistant professor of emergency medicine at Harvard Medical School, director of faculty affairs at Brigham and Women’s Hospital Urgent Care, and an attending physician in the Department of Emergency Medicine at Brigham and Women’s Hospital in Boston, Massachusetts. Dr. Sheng is the assistant residency program director and an assistant professor in the Depart-ment of Emergency Medicine, also at Boston University Medical Center.
Reviewed by Frank LoVecchio, DO, MPH, FACEP
n What clinical presentations warrant the use of video laryngoscopy over direct laryngoscopy?
n When and how should video laryngoscopy be used as a first-line instrument for airway management?
n What technical challenges are of greatest concern when using video laryngoscopy?
n Do all VL models have emergency department applications, and what are the benefits and limitations of each?
CRITICAL DECISIONS
OBJECTIVESOn completion of this lesson, you should be able to:
1. Describe the major limitations of conventional direct laryngoscopy.
2. List the advantages of video laryngoscopy for difficult intubations.
3. Describe the major video laryngoscopes available and the design differences between each device.
4. Explain the strengths and weakness of each of the major video laryngoscopes.
5. Apply video laryngoscopy in a variety of difficult airway scenarios.
Video Laryngoscopy
Primetime Viewing

Critical Decisions in Emergency Medicine14
CASE PRESENTATIONS■ CASE ONE
An 84-year-old woman with severe shortness of breath arrives via ambulance. She reports sudden-onset chest pain at rest with progressive dyspnea. Vital signs are blood pressure 122/56, a heart rate 99, and oxygen saturation 93% on non-rebreather facemask. The patient is tachypneic and in respiratory distress, using accessory muscles to breathe. Her jugular vein pulsations are elevated, and diffuse crackles and a 2/6 systolic murmur are noted at the apex radiating to the axilla.
The patient has 1+ bilateral lower-extremity edema. An ECG shows lateral-wall STEMI, and a portable chest radiograph shows diffuse pulmonary edema. Furosemide and nitroglycerin are administered, and she is placed on bilevel positive airway pressure (BI-PAP); however, she continues to struggle.
The emergency physician suspects ischemic mitral regurgitation from papillary muscle rupture. Cardiology at the bedside recommends immedi-ately catheterization. Preparations are made to secure the airway for impending respiratory failure prior to percutaneous coronary intervention.
■ CASE TWOEMS arrives with a 91-year-
old man who has been transferred from an outside hospital. He was a restrained passenger in a motor vehicle that rear-ended a bus at a high rate of speed. EMS reports that he had to be extricated and appears to have an unstable C2 fracture and weakness in both of his arms.
Upon arrival, the patient is supine on a stretcher and is wearing a cervical collar. Vital signs are stable and he is conversant, in no obvious distress, and complaining of neck pain. A secondary survey reveals tenderness to palpation on the posterior midline of the man’s neck. An outside cervical spine CT shows a displaced pedicle fracture of C2, and significant soft-tissue swelling from C2 down to C5.
Shortly thereafter, the patient suddenly begins having difficulty speaking and breathing, and complains of feeling “strangled.” Within minutes, he appears to be in respiratory distress. Suspecting a retropharyngeal hematoma, the clinician decides to intubate emergently to secure airway protection.
■ CASE THREEA 42-year-old woman with facial
swelling and a history of hereditary angioedema is brought to the emergency department of a small community hospital by EMS. Thirty minutes before her symptoms began, she ate an omelet seasoned with a “new” type of pepper. She immediately experienced a tingling sensation in her face, which has progressed to worsening facial, periorbital, and lingual edema within the last hour.
On arrival, she is afebrile. Vital signs are blood pressure 115/74; heart rate 89; and oxygen saturation 94% on room air, which improved to 97% with an oxygen facemask (reservoir at 15 L/min flow). Edema is apparent in her face, lips, and the area around her eyes. The patient’s tongue is swollen, filling the majority of her oral cavity, and her voice is hoarse; expiratory wheezing and stridor are noted.
While awaiting fresh frozen plasma from the blood bank, antihistamines, steroids, and epinephrine are administered without effect. C1 esterase-inhibitor concentrates are not readily available in this emergency department. Meanwhile, the patient develops worsening stridor, voice changes, and decreasing oxygen saturation on a non-rebreather mask. The decision is made to intubate.
There is a rapidly growing body of evidence to support the use of video laryngoscopy for the management of both routine and difficult airways. Emergency physicians, in particular, must understand the design and clinical applications of these devices to achieve improved first-pass success.
All resuscitative efforts ultimately will fail if the patient cannot be adequately oxygenated and ventilated. For the majority of those who are critically ill or injured, this requires the successful placement of an endotracheal tube (ETT). Since it first was introduced in the early 1940s, direct laryngoscopy (DL) has been a reliable and successful method for obtaining glottic visualization and tracheal intubation. While nearly every other aspect of medicine has undergone dramatic advances in recent decades,
however, DL largely has remained unchanged.
Direct visualization, which requires a straight line of sight from the operator’s eye to the glottic inlet, can be difficult or even impossible to acquire in many emergency department patients. Cervical spine precautions, reduced mouth openings, small mandibles, airway obstruction, blood, vomit, secretions, and large tongues all contribute to poor direct visualization.
Some of these challenges can be over-come with optimal patient positioning, meticulous DL technique, and external laryngeal manipulation. However, even in the hands of a skilled operator, many patients remain difficult — or even impossible — to intubate under direct vision. Many of these patients will require multiple attempts and prolonged
intubation times, which can put them at risk for dire traumatic and hypoxic consequences.
Through improved glottic visual-ization and user-friendly designs, video laryngoscopy (VL) has transformed our current understanding of what constitutes a difficult-to-manage airway, and has provided a new process for overcoming these clinical challenges. Over the past decade, advances in video-enhanced devices have launched an “airway management revolution.”
Fundamentally, all video laryngoscopes possess the same critical design elements that improve glottic visualization. Each device features a curved blade structure with a narrow profile that can curl around the tongue to mirror an oral airway. Embedded along the curve of the blade are a microcamera and light
March 2016 n Volume 30 Number 3 15
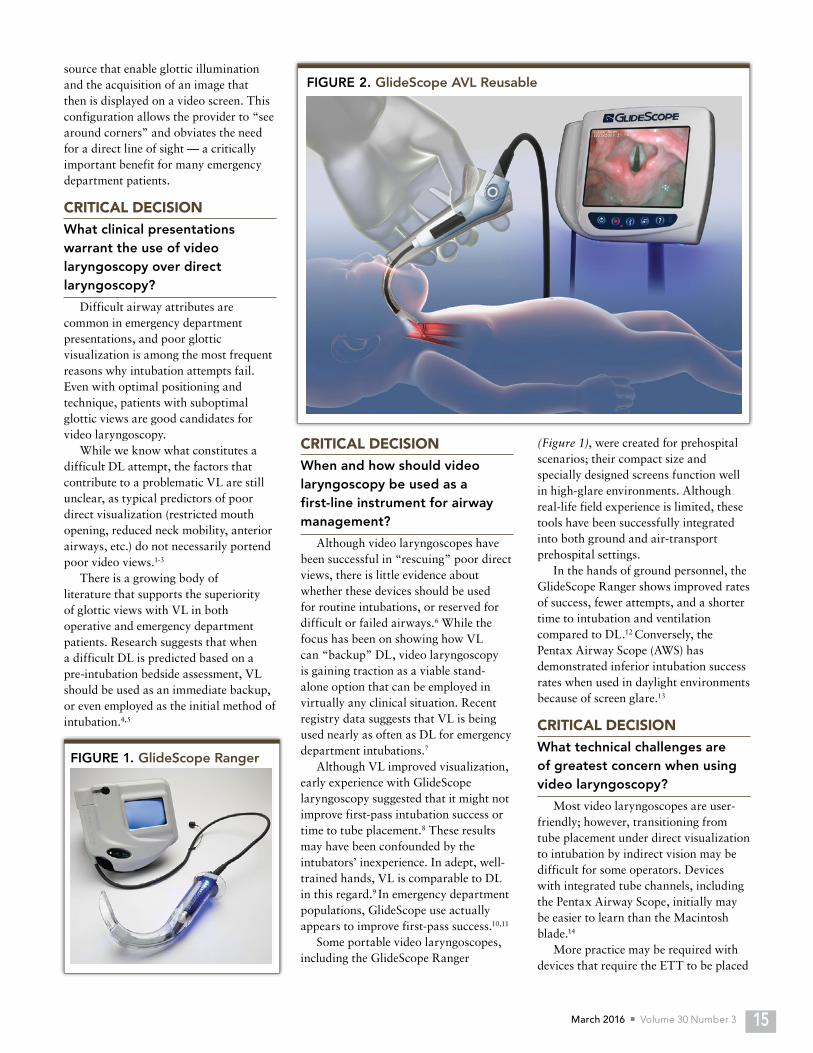
FIGURE 2. GlideScope AVL Reusablesource that enable glottic illumination and the acquisition of an image that then is displayed on a video screen. This configuration allows the provider to “see around corners” and obviates the need for a direct line of sight — a critically important benefit for many emergency department patients.
CRITICAL DECISIONWhat clinical presentations warrant the use of video laryngoscopy over direct laryngoscopy?
Difficult airway attributes are common in emergency department presentations, and poor glottic visualization is among the most frequent reasons why intubation attempts fail. Even with optimal positioning and technique, patients with suboptimal glottic views are good candidates for video laryngoscopy.
While we know what constitutes a difficult DL attempt, the factors that contribute to a problematic VL are still unclear, as typical predictors of poor direct visualization (restricted mouth opening, reduced neck mobility, anterior airways, etc.) do not necessarily portend poor video views.1-3
There is a growing body of literature that supports the superiority of glottic views with VL in both operative and emergency department patients. Research suggests that when a difficult DL is predicted based on a pre-intubation bedside assessment, VL should be used as an immediate backup, or even employed as the initial method of intubation.4,5
CRITICAL DECISIONWhen and how should video laryngoscopy be used as a first-line instrument for airway management?
Although video laryngoscopes have been successful in “rescuing” poor direct views, there is little evidence about whether these devices should be used for routine intubations, or reserved for difficult or failed airways.6 While the focus has been on showing how VL can “backup” DL, video laryngoscopy is gaining traction as a viable stand-alone option that can be employed in virtually any clinical situation. Recent registry data suggests that VL is being used nearly as often as DL for emergency department intubations.7
Although VL improved visualization, early experience with GlideScope laryngoscopy suggested that it might not improve first-pass intubation success or time to tube placement.8 These results may have been confounded by the intubators’ inexperience. In adept, well-trained hands, VL is comparable to DL in this regard.9 In emergency department populations, GlideScope use actually appears to improve first-pass success.10,11
Some portable video laryngoscopes, including the GlideScope Ranger
(Figure 1), were created for prehospital scenarios; their compact size and specially designed screens function well in high-glare environments. Although real-life field experience is limited, these tools have been successfully integrated into both ground and air-transport prehospital settings.
In the hands of ground personnel, the GlideScope Ranger shows improved rates of success, fewer attempts, and a shorter time to intubation and ventilation compared to DL.12 Conversely, the Pentax Airway Scope (AWS) has demonstrated inferior intubation success rates when used in daylight environments because of screen glare.13
CRITICAL DECISIONWhat technical challenges are of greatest concern when using video laryngoscopy?
Most video laryngoscopes are user-friendly; however, transitioning from tube placement under direct visualization to intubation by indirect vision may be difficult for some operators. Devices with integrated tube channels, including the Pentax Airway Scope, initially may be easier to learn than the Macintosh blade.14
More practice may be required with devices that require the ETT to be placed
FIGURE 1. GlideScope Ranger

Critical Decisions in Emergency Medicine16
independently by hand (eg, GlideScope or McGrath). The curved trajectory of the ETT as it approaches the laryngeal inlet can make navigation of the cords challenging.15
VL offers superior glottic exposure over DL in nearly every scenario. However, devices with distal image acquisition are susceptible to soiling by airway bleeding and secretions, which can make it difficult to maintain adequate visualization. To achieve indirect visualization of the laryngeal inlet and vocal cords, the ETT must follow the same trajectory of the blade as it approaches the airway.
Since this path follows a steep arc and not a straight line, it can be difficult to navigate the vocal cords with the tube tip; the stylet often must be retracted to complete the intubation. This unique extra step can result in a slightly pro-longed time to tracheal tube placement, although it does not affect intubation success.13 According to a recent study, predictors of difficult VL include pa-tients with poor upper lip bite tests (Ta-ble 1), although the study only included subjects with grade I or II Cormack and Lehane (C-L) glottic views.16
CRITICAL DECISION Do all VL models have emergency department applications, and what are the benefits and limitations of each?
GlideScope Video LaryngoscopeAnatomy
The GlideScope Video Laryngoscope (GVL), which has been on the market for more than a decade, is the prototypical VL model. The standard GVL system consists of a curved Macintosh-like blade; its 80-degree hyperacute anterior angulation curves around the tongue.
LED lights are positioned along the underbelly of the blade with a video camera that utilizes complementary metal-oxide semiconductor (CMOS) technology. A light source is placed in close proximity to a rectangular glass window, enabling the LEDs to warm the lens to prevent misting and fogging (a common problem with such devices).
A single video cable transmits processed images to a 7-inch LCD display, which can be placed on a flat surface or mounted to a mobile stand and brought to the bedside. The original GVL blade comes in a variety of shapes and sizes (GVL-2 through GVL-5) suitable for virtually any patient population — from small children to adults with physical limitations such as morbid obesity.
Most average-sized adults can be intubated with a size 3 or 4 blade. Standard GVL blades are reusable; after each intubation, they must undergo cleaning to remove gross debris, as well as high-level disinfection. The handle, made of high-grade medical plastic, is submersible.
Every GlideScope system includes a rigid stylet, which should be used to maintain ETT shape during intubation by allowing the tube to follow the curved trajectory of the blade without becoming deformed.
The GlideScope Cobalt AVL (Figure 2) is a disposable, single-use system that circumvents the cost and downtime associated with the maintenance and disinfection of the original model. Both
pediatric and standard-sized wands are available.
The GlideScope Ranger is a lightweight, portable version originally designed for field use. The handle, cable, and display are built into one self-contained unit, and its 3.5-inch LCD screen remains visible despite sun glare.
Devices in the GlideScope family also include a steel video blade with geometry similar to that of direct laryngoscopes. This “direct intubation trainer” is designed to allow the operator to maintain skill with conventional DL mechanics, while benefitting from video enhancements that facilitate real-time instructor feedback. The most recent GlideScope iteration features a thin titanium profile and disposable high-grade plastic blades.
TechniqueLimited by its shape and design, the
GlideScope does not function and should not be used as a direct laryngoscope. Like all such devices, the GlideScope is a left-handed instrument. After opening the patient’s mouth, the blade should be inserted directly in the midline with the top surface of the blade touching, but not manipulating, the tongue. While the patient can be placed in the “sniffing position,” this is not required.
With an eye on the screen, the intubator should guide the distal tip of the blade around the tongue while watching for key midline structures, including the uvula and the tip of the epiglottis. The blade tip should be maneuvered into the vallecula and then a gentle backward lift should be used to expose the laryngeal inlet.
A common mistake is to advance the blade too far into the hypopharynx, which results in an “up-close” image of the vocal cords that appears highly optimized; in reality, however, the blade may be too close and incorrectly positioned in the laryngeal inlet.
Ultimately, the blade competes for the same space as the approaching ETT, making tube delivery exceptionally difficult. The tip of the ETT should be inserted in the corner of the right side of the patient’s mouth, with the tube parallel to the ground. As the tube is advanced behind or adjacent to the
FIGURE 3. Storz C-MAC
TABLE 1. Upper Lip Bite Test
Class I: Lower incisors can bite the upper lip above the vermilion line.
Class II: Lower incisors can bite the upper lip below the vermilion line.
Class III: Lower incisors cannot bite the upper lip.

March 2016 n Volume 30 Number 3 17
blade and its distal tip guided toward the tip of the laryngoscope, the user should look at the screen while rotating the tube counterclockwise 90 degrees. (The tip of the ETT should be held at 12 o’clock, positioned in front of the laryngeal inlet curving into the trachea.)
Under real-time video supervision, the operator should advance the ETT through the vocal cords while simultaneously withdrawing the stylet by about 5 cm to complete the intubation. Withdrawal, which can be done by the operator’s thumb or by an assistant, should follow the arc of the instrument, eventually curving into the patient’s chest.
Obtaining an optimal view of the glottis with the GlideScope is rarely difficult. However, passage of the ETT through the glottis while observing the screen can be challenging for two reasons. First, some familiarity with the instrument is required. Second, due to the hyperangulation of the GlideScope blade, the tip of the ETT must follow the same path with an anterior trajectory that can impinge on the trachea at a sharp angle and fail to advance. Withdrawal of the stylet makes the end of the ETT flexible, enabling it to pass easily into the trachea.
The device is appropriate as a primary intubation tool, although it traditionally has been reserved for cases that are diffi-cult or impossible to complete under di-rect vision. The minimal force required to expose the glottis makes the GlideScope useful for patients in C-spine immobili-zation. Its sharp distal angulation allows better visualization of the anterior larynx.
Evidence Among inexperienced operators, the
device is able to provide a C-L grade I or II view in nearly every patient in which its used, with glottic visualization equal to or better than DL. Although rare, failures can occur due to the difficulty of passing the ETT, despite a sufficient glottic view.17
Success with this device is high (96% to 98%), even in patients who exhibit hallmarks of difficult laryngoscopy (eg, those with morbid obesity, cervical spine disease, or a cervical collar). The device performs equally well compared to flexible bronchoscopes in morbidly obese patients.29 The GlideScope also has shown promise as a rescue device, succeeding in 94% of intubations where DL failed. Evidence of altered upper-airway anatomy or head and neck surgery appear to be the only predictors of GlideScope difficulty.18 The device’s only limitation is that the patient’s mouth opening must be greater than 15 mm to accommodate the passage of the widest portion of the blade.
In a recent study aimed at identifying the clinical features associated with difficult GlideScope laryngoscopy, patients with high upper lip bite test scores and short sternothyroid distances required multiple attempts or lengthier intubation times. Despite these complications, a grade I or II view was obtained in every patient (all of whom were undergoing general anesthesia).16
In the hands of prehospital providers, the GlideScope also has been associated
with improved intubation success (97% compared to 95% with DL), fewer attempts (1.2 versus 2.3), less time without ventilation (37 seconds versus 55 seconds), and shorter time to intubation (21 versus 42 seconds).12
Storz C-MACAnatomy
The Storz C-MAC (Figure 3) is a reincarnation of the older video Macintosh laryn goscope (V-MAC). While the video Macintosh was a hybrid scope that combined both fiberoptic and video elements, the C-MAC utilizes a CMOS chip technology similar to that used in the GlideScope.
The device’s shape is that of a traditional direct Macintosh laryngoscope. A newer hyperangulated blade (called the “D-blade” or difficult blade) recently has been designed to help visualize a more anterior and superior larynx. A micro camera and light source are blended into the blade; and a video cartridge slips into the back of the handle, attached by a single cord to a high-resolution digital display that can sit on a flat surface or mount to a mobile pole.
The blades intrinsically possess anti-fog properties (the light source is contained in the blade itself, warming the lens), and the monitor system can record both still images and video clips.
TechniqueSince the standard C-MAC
blades feature Macintosh geometry, the mechanics of laryngoscopy are more akin to that of DL. Because of this, the trajectory to the airway is straighter, which can help facilitate the manipulation of the ETT tip to the laryngeal inlet. While it is possible to intubate without one, a malleable stylet should be used for the majority of emergency tracheal intubations; rigid stylets are unnecessary.19
When using the C-MAC, the operator can either insert the blade as if using a conventional direct laryngoscope, or place the blade in the midline and advance it using a GlideScope-like technique. With its anti-fog features, wider field of view, ease of use, and mobility, the C-MAC has become
FIGURE 4. McGrath Series 5

Critical Decisions in Emergency Medicine18
particularly popular in emergency department settings.
EvidenceBecause the C-MAC is a newer device,
it has yet to collect the robust body of evidence seen with the GlideScope; however, early studies are encouraging. In one dual-center study, V-MAC laryngoscopy succeeded in producing the best attainable direct and video view and a higher number of “good” glottic views (C-L grade I or II) compared to DL. Of the patients with an initial grade IV direct view, a grade I or II video view was obtained nearly 80% of the time. This data also supports the argument that early recourse to VL should be considered when glottic visualization is suboptimal.20
Video laryngoscopes also provide gentler intubation attempts since less effort is required to obtain an acceptable view. The force exerted on the maxillary incisors by the V-MAC is less than that associated with a standard Macintosh blade (2.1 N versus 15.3 N).21
As with the GlideScope, the V-MAC allows trainees to view the procedure on the screen in real time — a benefit that can improve the intubation process and reduce the learning curve.22 Preliminary experience with the C-MAC shows it performs on par with other video laryn-goscopes in its class. The device also may provide better first-pass success (93% ver-sus 84%) in predicted difficult airways.23
McGrath Series 5Anatomy
Compact and lightweight, the McGrath Series 5 video laryngoscope features a 1.7-inch integrated LCD screen mounted on the end of its handle (Figure 4). The monitor pivots and is adjustable to maintain optimal viewing during different phases of insertion. A curved video wand (called a “Camera Stick”) houses the light source with a single-use disposable hard plastic blade.
The McGrath’s main advantage is its portability; it weighs only 325 grams, and requires neither cables nor a separate display unit. However, the device’s small size can make it vulnerable to theft and damage during transport. The video wand and blade cover are fully adjustable to three different lengths.
The newest version of the device includes a slightly larger screen and an angled blade designed for both video and direct viewing. However, when used as a direct laryngoscope, the device may not provide adequate direct views of the glottic inlet.24
TechniqueMuch like the GlideScope, the
McGrath is designed to be inserted in the midline and “hugged” around the tongue, while being rotated backwards until the glottis can be visualized. The tip of the blade should be positioned in the vallecula. A slight upward lift may
n Use a rigid stylet when intubating with the GlideScope; this can help the ETT navigate the sharper anterior angulation of the blade to reach the laryngeal inlet.
n If maintaining DL skill is important in your practice, consider using a C-MAC blade, which maintains standard Macintosh geometry and can be used when DL mechanics are desired.
n Consider VL as the initial method for routine and difficult intubations, and be familiar with the specific devices available in your emergency department.
n Devices with plastic covers that go over or envelop the video and light elements (eg, C-MAC, GlideScope Cobalt, McGrath Series 5) are prone to fogging. Either warm the device or apply a commercial anti-fog solution prior to the intubation attempt.
be required to expose the glottis. A malleable stylet with a curve that follows the arc of the blade should be used within the tracheal tube to maintain its shape.
EvidenceAlthough not as extensively studied
as the GlideScope, the McGrath has performed well in operative reports, obtaining a C-L grade I or II view in 99% of subjects.25 The model also may be a particularly valuable rescue tool after DL has failed. In one operative study of patients undergoing general anesthesia with unsuccessful DL, the McGrath successfully intubated patients 95% of the time (58/61).9 As with other video laryngoscopes, novice clinicians may take longer to intubate when using the instrument than when using DL — a caveat that reflects the additional skill required to indirectly navigate the ETT through the vocal cords.26
The Pentax Airway Scope (AWS-100)Anatomy
The portable, self-contained Pentax Airway Scope includes a video camera, 2.4-inch LCD rectangular display, disposable blade, and tube holder (Figure 5). While the design is similar to that of other video laryngoscopes, several unique features are worth noting. Green “crosshairs” on the display allow the operator to properly position the device; when the ETT is advanced, it is more likely to traverse the laryngeal opening into the trachea.
The device’s handle is attached to a flexible video/light wand that fits inside a disposable plastic sheath and provides a 90-degree field of view. The blade, made from fog- and contamination-resistant Lexan plastic, incorporates a tracheal channel that holds the tube
FIGURE 5. Pentax Airway Scope
March 2016 n Volume 30 Number 3 19
CASE RESOLUTIONS■ CASE ONE
Airway equipment was prepared at the bedside to intubate the elderly woman with STEMI, including size-3 Macintosh and Miller blades, and a GlideScope video laryngoscope and bougie as backups. The patient was preoxygenated with BL-PAP with a starting oxygen saturation of 97%.
Etomidate (10 mg) and succinyl-choline (100 mg) were administered intravenously. Fasciculations appeared 30 seconds later with flaccid paralysis at 50 seconds. The emergency physi-cian’s first direct look with the Mac 3 provided a C-L grade III view; it be-came apparent that the patient suffered from advanced degenerative temporo-mandibular joint (TMJ), which limited the opening of her mouth. The view was not improved, even with use of the Miller blade and backwards, upwards, rightwards pressure.
The patient desaturated, but was successfully bagged and preoxygenated. A second attempt
during insertion and facilitates its passage during intubation. The channel can accommodate tubes with internal diameters from 6.0 to 8.5 mm.
Durable and highly water-resistant, the AWS-S100 model is particularly useful in outdoor prehospital environments. However, the lack of a robust anti-fog mechanism and
tendency for secretions and blood to contaminate the device’s optics can compromise visualization during intubation.
TechniqueMuch like other video laryngoscopes,
the AWS is advanced in the midline after the vocal cords have been positioned in the target site.
EvidenceIn 100 elective surgery patients,
the Pentax AWS obtained a grade I view in all cases, while the Mac blade achieved this only 65% of the time. The integrated channel, as opposed to freehanding, may result in faster times to intubation compared to the GlideScope in patents with normal airway anatomy.27
The Pentax also shows encouraging results in patients at risk for cervical spine injury.28 Even in the hands of novice operators, intubation with the Pentax may be faster and more successful than with DL.14 The screen,
which is difficult to view in bright light, can result in harder and longer intubation attempts in outdoor daylight settings.13
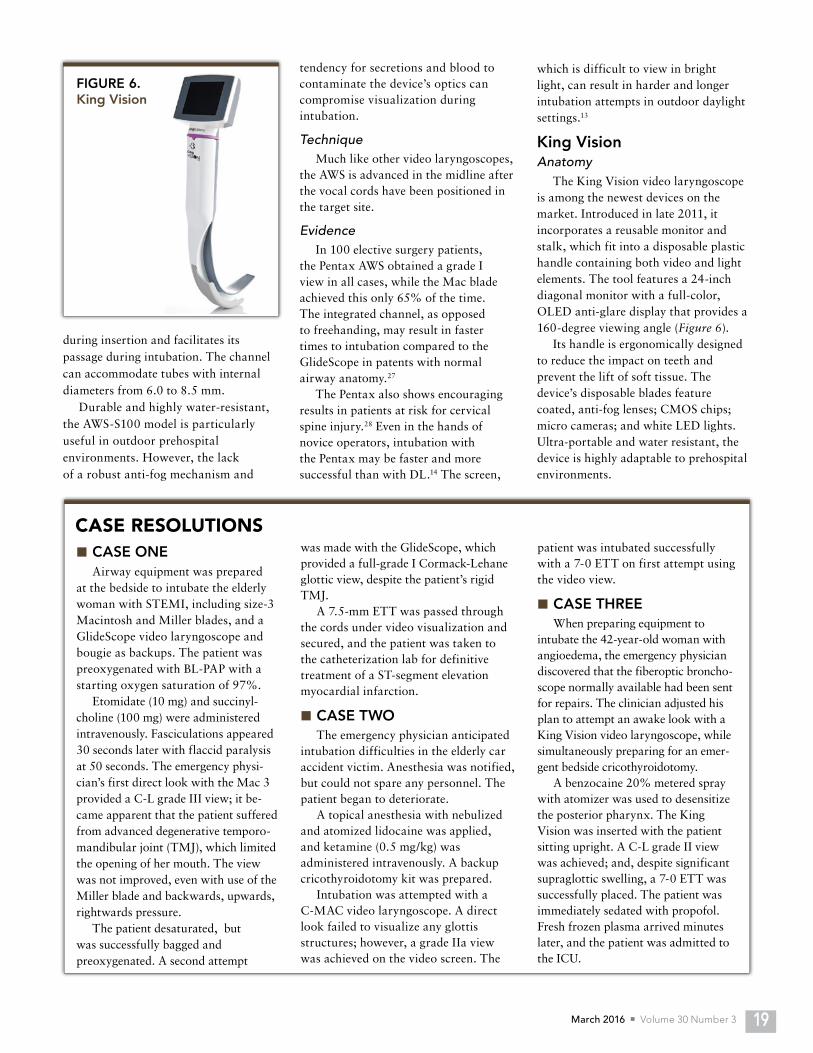
King VisionAnatomy
The King Vision video laryngoscope is among the newest devices on the market. Introduced in late 2011, it incorporates a reusable monitor and stalk, which fit into a disposable plastic handle containing both video and light elements. The tool features a 24-inch diagonal monitor with a full-color, OLED anti-glare display that provides a 160-degree viewing angle (Figure 6).
Its handle is ergonomically designed to reduce the impact on teeth and prevent the lift of soft tissue. The device’s disposable blades feature coated, anti-fog lenses; CMOS chips; micro cameras; and white LED lights. Ultra-portable and water resistant, the device is highly adaptable to prehospital environments.
was made with the GlideScope, which provided a full-grade I Cormack-Lehane glottic view, despite the patient’s rigid TMJ.
A 7.5-mm ETT was passed through the cords under video visualization and secured, and the patient was taken to the catheterization lab for definitive treatment of a ST-segment elevation myocardial infarction.
■ CASE TWOThe emergency physician anticipated
intubation difficulties in the elderly car accident victim. Anesthesia was notified, but could not spare any personnel. The patient began to deteriorate.
A topical anesthesia with nebulized and atomized lidocaine was applied, and ketamine (0.5 mg/kg) was administered intravenously. A backup cricothyroidotomy kit was prepared.
Intubation was attempted with a C-MAC video laryngoscope. A direct look failed to visualize any glottis structures; however, a grade IIa view was achieved on the video screen. The
patient was intubated successfully with a 7-0 ETT on first attempt using the video view.
■ CASE THREEWhen preparing equipment to
intubate the 42-year-old woman with angioedema, the emergency physician discovered that the fiberoptic broncho-scope normally available had been sent for repairs. The clinician adjusted his plan to attempt an awake look with a King Vision video laryngoscope, while simultaneously preparing for an emer-gent bedside cricothyroidotomy.
A benzocaine 20% metered spray with atomizer was used to desensitize the posterior pharynx. The King Vision was inserted with the patient sitting upright. A C-L grade II view was achieved; and, despite significant supraglottic swelling, a 7-0 ETT was successfully placed. The patient was immediately sedated with propofol. Fresh frozen plasma arrived minutes later, and the patient was admitted to the ICU.
FIGURE 6. King Vision

Critical Decisions in Emergency Medicine20
TechniqueThe King Vision should be introduced
into the patient’s mouth in much the same way it is with the GlideScope and Pentax AWS. Once fully inserted, slight upward force may be required to optimize the glottic view. If using a channeled blade, the tube simply can be pushed forward while the glottic opening is kept in the middle of the screen. Alternatively, a preformed stylet and ETT can be “freehanded” to complete the intubation.
Innovative, lightweight, compact, and affordable, the device includes the design elements that have proved successful in other VL models. Although formal studies are lacking, promising research is underway.
SummaryVL is changing the landscape of
emergency airway management. DL is a time-tested technique that relies on an outdated tool. Video laryngoscopes are highly successful, easy to use, and improve glottic visualization in almost every conceivable scenario. The combination of improved visualization, high first-pass success and gentler attempts undoubtedly will translate into a safer, more reliable intubation experience for the patient and provider.
In modern medicine, these devices help facilitate airway management education, quality assurance, and research through their ability to record still images and videos. While they traditionally have been thought of as “rescue” tools, there is no evidence that
we should relegate them to this role. Trauma, bleeding, and airway
swelling will occur with serial laryngoscopy attempts. Each device has its advantages and disadvantages, and the final choice will depend on practice setting, departmental budgets, provider preference, and the ability to reprocess reusable equipment. However, one thing is clear — when available, VL is quickly becoming standard care.
For the same reason we’ve moved away from ordering oral contrast dye studies to diagnose appendicitis or performing diagnostic peritoneal lavage for unstable trauma patients, we should begin to migrate away from DL. Although DL represents “the way we’ve always done it,” we must now perform intubation “the way it should be done.”
REFERENCES 1. Walls RM. Identification of the Difficult and
Failed Airway. In: Manual of Emergency Airway Management, 3rd Ed. LW&W; 2008:81-93.
2. Reed MJ, Dunn MJ, McKeown DW. Can an airway assessment score predict difficulty at intubation in the emergency department? Emerg Med J. 2005;22(2):99-102.
3. Hagiwara Y, Watase H, Okamoto H, et al. Prospective validation of the modified LEMON criteria to predict difficult intubation in the ED. Am J Emerg Med. 2015;33(10):1492-1496.
4. Kaplan MB, Hagberg CA, Ward DS, et al. Comparison of direct and video-assisted views of the larynx during routine intubation. J Clin Anesth. 2006;18(5):357-362.
5. Sakles JC, Mosier J, Chiu S, et al. A comparison of the C-MAC video laryngoscope to the Macintosh direct laryngoscope for intubation in the emergency department. Ann Emerg Med. 2012;60(6):739-748.
6. Piepho T, Fortmueller K, Heid FM, et al. Performance of the C-MAC video laryngoscope in patients after a limited glottic view using Macintosh laryngoscopy. Anaesthesia. 2011;66(12):1101-1105
7. Brown CA 3rd, Blair AE, Pallin DJ, et al. Techniques, success, and adverse events of emergency department adult intubations. Ann Emerg Med, 2015;65(4):363-370.e1.
8. Platts-Mills TF, Campagne D, Chinnock B, et al. A comparison of GlideScope video laryngoscopy
versus direct laryngoscopy intubation in the emergency department. Acad Emerg Med. 2009;16(9):866-871.
9. Noppens RR, Möbus S, Heid F, et al. Evaluation of the McGrath Series 5 videolaryngoscope after failed direct laryngoscopy. Anaesthesia. 2010;65(7):716-720
10. Sakles JC, Mosier JM, Chiu S, Keim SM. Tracheal intubation in the emergency department: a comparison of GlideScope® video laryngoscopy to direct laryngoscopy in 822 intubations. J Emerg Med. 2012;42(4):400-405.
11. Mosier JM, Stolz U, Chiu S, Sakles JC. Difficult airway management in the emergency department: GlideScope videolaryngoscopy compared to direct laryngoscopy. J Emerg Med. 2012;42(6):629-634.
12. Wayne MA, McDonnell M. Comparison of traditional versus video laryngoscopy in out-of-hospital tracheal intubation. Prehosp Emerg Care. 2010;14(2):278-282.
13. Ueshima H, Asai T. Tracheal intubation in daylight and in the dark: a randomised comparison of the Airway Scope, Airtraq, and Macintosh laryngoscope in a manikin. Anaesthesia. 2010;65(7):684-687.
14. Liu L, Tanigawa K, Kusunoki S, et al. Tracheal intubation of a difficult airway using Airway Scope, Airtraq, and Macintosh laryngoscope: a comparative manikin study of inexperienced personnel. Anesth Analg. 2010;110(4):1049-1055.
15. Walls RM, Samuels-Kalow M, Perkins A. A new maneuver for endotracheal tube insertion during difficult GlideScope intubation. J Emerg Med. 2010;39(1):86-88.
16. Tremblay MH, Williams S, Robitaille A, Drolet P. Poor visualization during direct laryngoscopy and high upper lip bite test score are predictors of difficult intubation with the Glidescope videolaryngoscope. Anesth Analg. 2005;106(5):1495-1500.
17. Cooper RM, Pacey JA, Bishop MJ, McCluskey SA. Early clinical experience with a new video laryngoscope (GlideScope) in 728 patients. Can J Anaesth. 2005;52(2):191-198.
18. Aziz MF, Healy D, Kheterpal S, et al. Routine clinical practice effectiveness of the Glidescope in difficult airway management: an analysis of 2,004 Glidescope intubations, complications, and failures from two institutions. Anesthesiology. 2011;114(1):34-41.
19. van Zundert A, Maassen R, Lee R, et al. A Macintosh laryngoscope blade for videolaryngoscopy reduces stylet use in patients with normal airways. Anesth Analg. 2009;109(3):825-831.
20. Brown CA 3rd, Bair AE, Pallin DJ, et al. Improved glottic exposure with the video Macintosh laryngoscope in adult emergency department tracheal intubations. Ann Emerg Med. 2010;56(2):83-88.
21. Lee RA, van Zundert AA, Maassen RL, et al. Forces applied to the maxillary incisors during video-assist-ed intubation. Anesth Analg. 2009;108(1):187-191.
22. Kaplan MB, Ward DS, Berci G. A new video laryngoscope—an aid to intubation and teaching. J Clin Anesth. 2002;14(8):620-626.
23. Aziz MF, Dillman D, Fu R, Brambrink AM. Comparative effectiveness of the C-MAC video laryngoscope versus direct laryngoscopy in the setting of the predicted difficult airway. Anesthesiology. 2012;116(3):629-636.
24. Wallace CD, Foulds LT, McLeod GA, et al. A comparison of the ease of tracheal intubation using a McGrath MAC® laryngoscope and a standard Macintosh laryngoscope. Anaesthesia. 2015;70(11):1281-1285.
25. Shippey B, Ray D, McKeown D. Case series: the McGrath videolaryngoscope—an initial clinical evaluation. Can J Anaesth. 2007;54(4):307-313.
26. Walker L, Brampton W, Halai M, et al. Randomized controlled trial of intubation with the McGrath Series 5 videolaryngoscope by inexperienced anaesthethists. Br J Anaesth. 2009;103(3):440-445.
27. Teoh WH, Shah MK, Sia AT. Randomised comparison of Pentax AirwayScope and Glidescope for tracheal intubation in patients with normal airway anatomy. Anaesthesia. 2009;64(10):1125-1129.
28. Liu EH, Goy RW, Tan BH, Asai T. Tracheal intubation with videolaryngoscopes in patients with cervical spine immobilization: a randomized trial of the Airway Scope and the GlideScope. Br J Anaesth. 2009; [e-pub ahead of print]. Available at: http://dx.doi.org/10.1093/bja/aep164.
29. Abdelmalak BB, Bernstein E, Egan C, et al. GlideScope® vs flexible fibreoptic scope for elective intubation in obese patients. Anaesthesia. 2011;66(7):550-555.
n Failing to practice the techniques for tube delivery with video laryngoscopy, which requires different hand-eye coordination, stereotactic skills, and experience than with DL.
n Advancing a video laryngoscope too deeply. This can result in a disorienting view of the esophageal opening, which is created when the camera is directed posterior to the laryngeal inlet.
n Intubating without a stylet or with the wrong stylet.
n Attempting to intubate without maintaining a curve on the tracheal tube; this mistake will make the procedure challenging or even impossible.
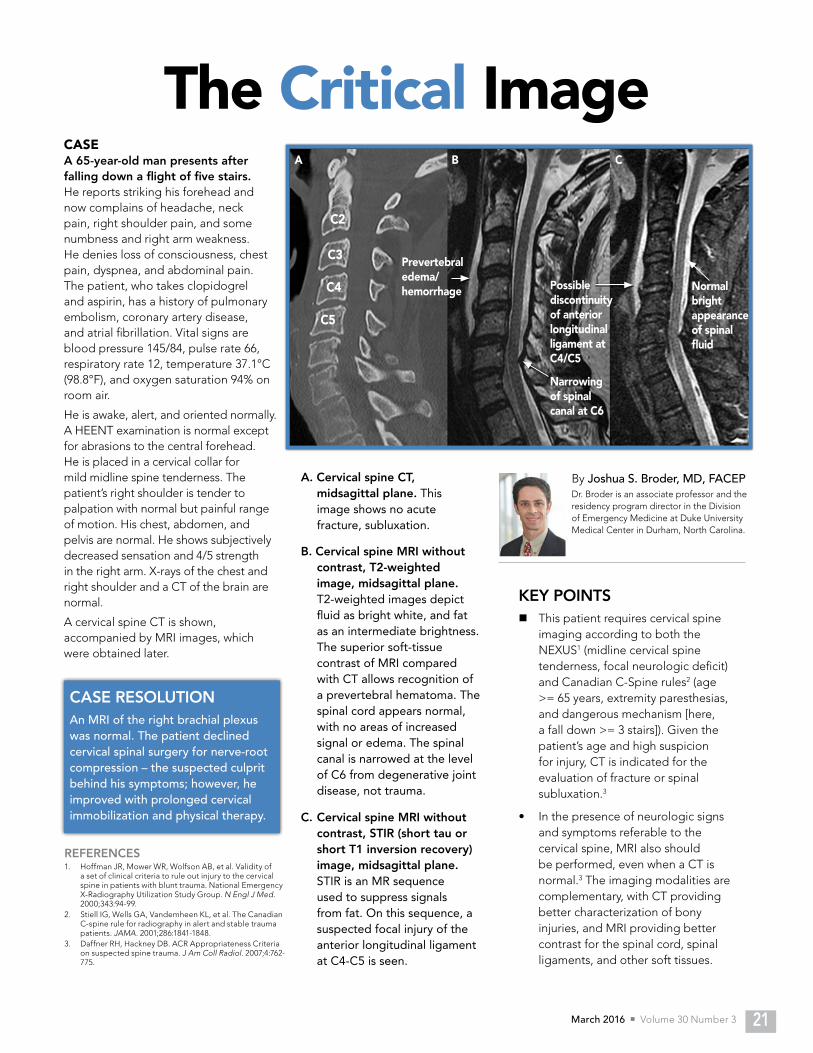
March 2016 n Volume 30 Number 3 21
The Critical ImageCASE A 65-year-old man presents after falling down a flight of five stairs. He reports striking his forehead and now complains of headache, neck pain, right shoulder pain, and some numbness and right arm weakness. He denies loss of consciousness, chest pain, dyspnea, and abdominal pain. The patient, who takes clopidogrel and aspirin, has a history of pulmonary embolism, coronary artery disease, and atrial fibrillation. Vital signs are blood pressure 145/84, pulse rate 66, respiratory rate 12, temperature 37.1°C (98.8°F), and oxygen saturation 94% on room air.
He is awake, alert, and oriented normally. A HEENT examination is normal except for abrasions to the central forehead. He is placed in a cervical collar for mild midline spine tenderness. The patient’s right shoulder is tender to palpation with normal but painful range of motion. His chest, abdomen, and pelvis are normal. He shows subjectively decreased sensation and 4/5 strength in the right arm. X-rays of the chest and right shoulder and a CT of the brain are normal.
A cervical spine CT is shown, accompanied by MRI images, which were obtained later.
KEY POINTSn This patient requires cervical spine
imaging according to both the NEXUS1 (midline cervical spine tenderness, focal neurologic deficit) and Canadian C-Spine rules2 (age >= 65 years, extremity paresthesias, and dangerous mechanism [here, a fall down >= 3 stairs]). Given the patient’s age and high suspicion for injury, CT is indicated for the evaluation of fracture or spinal subluxation.3
• In the presence of neurologic signs and symptoms referable to the cervical spine, MRI also should be performed, even when a CT is normal.3 The imaging modalities are complementary, with CT providing better characterization of bony injuries, and MRI providing better contrast for the spinal cord, spinal ligaments, and other soft tissues.
By Joshua S. Broder, MD, FACEPDr. Broder is an associate professor and the residency program director in the Division of Emergency Medicine at Duke University Medical Center in Durham, North Carolina.
A. Cervical spine CT, midsagittal plane. This image shows no acute fracture, subluxation.
CASE RESOLUTIONAn MRI of the right brachial plexus was normal. The patient declined cervical spinal surgery for nerve-root compression – the suspected culprit behind his symptoms; however, he improved with prolonged cervical immobilization and physical therapy.
REFERENCES1. Hoffman JR, Mower WR, Wolfson AB, et al. Validity of
a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N Engl J Med. 2000;343:94-99.
2. Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001;286:1841-1848.
3. Daffner RH, Hackney DB. ACR Appropriateness Criteria on suspected spine trauma. J Am Coll Radiol. 2007;4:762-775.
B. Cervical spine MRI without contrast, T2-weighted image, midsagittal plane. T2-weighted images depict fluid as bright white, and fat as an intermediate brightness. The superior soft-tissue contrast of MRI compared with CT allows recognition of a prevertebral hematoma. The spinal cord appears normal, with no areas of increased signal or edema. The spinal canal is narrowed at the level of C6 from degenerative joint disease, not trauma.
C. Cervical spine MRI without contrast, STIR (short tau or short T1 inversion recovery) image, midsagittal plane. STIR is an MR sequence used to suppress signals from fat. On this sequence, a suspected focal injury of the anterior longitudinal ligament at C4-C5 is seen.
Normal bright appearance of spinal fluid
Possible discontinuity of anterior longitudinal ligament at C4/C5
Narrowing of spinal canal at C6
Prevertebral edema/hemorrhage
A B C
C5
C4
C3
C2
Critical Decisions in Emergency Medicine22
CME QUESTIONS
1 Which of the following characteristics is more likely to be associated with thrombotic thrombocytopenic purpura (TTP) than with hemolytic uremic syndrome (HUS)?A. Autoimmune hemolysisB. Changes in mental statusC. Renal failureD. Thrombocytopenia
2 How is the PT/PTT affected in cases of immune thrombocytopenia (ITP)?A. Both decreaseB. Both increaseC. Neither is affectedD. PT is increased and PTT is unchanged
3 Spontaneous bleeding becomes a concern when platelets fall below which of the following levels?A. 10,000 mm3
B. 20,000 mm3
C. 40,000 mm3
D. 50,000 mm3
4 Which of the following medications commonly is associated with drug-induced thrombocytopenia?A. AcetaminophenB. GanciclovirC. LoratidineD. Oxycodone
5 HUS most frequently is associated with which of the following bacteria?A. E. coliB. KlebsiellaC. StaphylococcusD. Streptococus
6 Which of the following is an example of increased platelet consumption?A. ITPB. RadiationC. TTPD. DIC
7 A 10-year-old boy is found to have ITP with no signs of serious bleeding; his platelet count is 15,000 mm3. What is the most appropriate initial treatment?A. Methylprednisolone and IVIGB. Monitor platelet countC. Platelet transfusionD. Splenectomy
8 After immediately stopping all unfractionated heparin products, which of the following medications is the most appropriate next step in the treatment of heparin-induced thrombocytopenia (HIT)?A. AspirinB. BivalirudinC. DiazepamD. Lovenox
9 A 21-year-old woman presents to the emergency department with a 2-day history of fever and palpable purpura. A CBC indicates anemia and thrombocytopenia, and a blood smear shows schistocytes. Which of the following management strategies is most appropriate?A. Admission with broad-spectrum antibioticsB. Plasma exchange and ICU admissionC. Plasma transfusion and steroids with admissionD. Surgical consultation for splenectomy
A 47-year-old woman is found on routine laboratory work to have thrombocytopenia with a platelet count of 40,000 mm3; other laboratory values are within normal limits. She recently began taking trimethoprim/sulfmethoxazole for a urinary tract infection. She does not show a mucosal bleed or rash. What is the most appropriate next step in the management of this patient? A. Plasma exchange B. Plasma transfusionC. Steroids for 5 daysD. Stop the antibiotic
Qualified, paid subscribers to Critical Decisions in Emergency Medicine may receive CME certificates for up to 5 ACEP Category I credits, 5 AMA PRA Category 1 Credits™, and 5 AOA Category 2-B credits for completing this activity in its entirety. Submit your answers online at acep.org/newcriticaldecisionstesting; a score of 75% or better is required. You may receive credit for completing the CME activity any time within three years of its publication date. Answers to this month’s questions will be published in next month’s issue.
10
Reviewed by Lynn Roppolo, MD, FACEP
March 2016 n Volume 30 Number 3 23
ANSWER KEY FOR FEBRUARY 2016, VOLUME 30, NUMBER 2
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20A C C A C A C A B C C A B C C B B A D A
Which of the following most accurately describes the advantages of video laryngoscopy compared to direct laryngoscopy?A. Most direct laryngoscopes have remained
unchanged for decades B. Video devices are cheaper and easier to maintain
than direct laryngoscopesC. Video laryngoscopy guarantees a good patient
outcome D. Video laryngoscopes provide improved glottic
visualization and a superior educational opportunity
Which of the follow devices comes with a preformed rigid stylet to assist with endotracheal tube placement?A. C-MAC B. GlideScopeC. King VisionD. McGrath
What is an absolute contraindication to the use of the GlideScope?A. Bedside airway evaluation concerning for anterior
laryngeal airwayB. Blood and secretions in the airway that obstruct
the glottic viewC. C-spine immobilizationD. Inability to open the mouth >15 mm
Which of the following devices may not perform as well in prehospital, sunlit conditions because of screen glare?A. C-MAC B. GlideScopeC. King VisionD. Pentax Airway Scope
Which of the following devices was the first to combine both direct and video techniques?A. C-MACB. GlideScopeC. King VisionD. McGrath
Which of the following devices features “crosshairs” as a targeting aid for intubation?A. C-MAC B. King VisionC. McGrathD. Pentax Airway Scope
Which of the following video laryngoscopes has demonstrated similar efficacy as a flexible bronchoscope in the intubation of obese patients?A. C-MAC B. GlideScopeC. King VisionE. Pentax Airway Scope
In which of the following devices would anti-fog solution be most helpful?A. C-MACB. GlideScopeC. King Vision D. Pentax Airway Scope
Which of the following video laryngoscopes contains a disposable blade, light source, and video camera?A. GlideScopeB. C-MAC C. King VisionD. Pentax Airway Scope
In which of the following situations is direct laryngoscopy a more appropriate choice than video laryngoscopy?A. In obese patientsB. In patients held in C-spine immobilization C. In patients with upper-airway obstruction (eg,
angioedema)D. When video laryngoscopes are unavailable
11
12
13
14
15
16
17
19
18
20
Drug Box Tox BoxCARBON MONOXIDEBy Daniel Lasoff, MD, University of California Health Sciences, San Diego, California
FOSFOMYCINBy Aimee Mishler, PharmD, BCPS, and Frank Lovecchio, DO, MPH, Maricopa and Banner University Medical Centers, Phoenix, Arizona
Fosfomycin is an oral broad-spectrum antibiotic with sensitivity to many gram-positive and -negative organisms, including E. coli, E. faecalis, Niesseria, Salmonella, and Proteus. However, B. fragilis and anerobic gram-negative cocci are resistant. Fosfomycin remains highly sensitive
to multidrug-resistant extended spectrum β-lactamases producing E. coli and K. pneumonia. The drug may be more appealing than other agents due to its ability to maintain adequate concentrations for up to 48 hours after a single dose.
Mechanism of Action
Bactericidal agent that inhibits bacterial-wall synthesis by inactivating pyruvyl transferase.
Indications Approved for uncomplicated urinary tract infections in females. Off-label uses include complicated urinary tract infections and prostatitis in males.
Dosing Uncomplicated urinary tract infection: 3 grams dissolved in 3-4 oz of cold water as a single doseNo dose adjustments for renal or hepatic impairment. Not approved for children.
Side Effects Most common: Diarrhea, nausea, and headache Less common: Dizziness, rash, abdominal pain, vaginitis, and rhinitis
Considerations Contraindications: Hypersensitivity Precautions: Prolonged use may increase the risk of a superinfection such as C. difficile diarrhea.Pregnancy and lactation: Pregnancy category B. Fosfomycin crosses the placenta, but has not been shown to cause adverse effects in animal reproductive studies. Avoid use when breastfeeding.
Carbon monoxide (CO) from incomplete combustion is one of the great imitators in medicine. Patients can present with a variety of nonspecific symptoms (eg, flu), so suspicion should be high, especially during colder months.PresentationCommon: Headache, dizziness, nausea, vomiting, ataxia, confusion, and/or fatigue Severe: Altered mental status, syncope, coma, convulsions, hypotension, dysrhythmias, cardiac ischemia, and metabolic acidosis ConsiderationsMultiple patients with similar symptoms should raise suspicion for CO. Most patients with CO exposure do well acutely if removed from source neurologically intact. However, a majority can develop neurologic sequelae ranging from subtle (eg, problems with memory, mood, or cognition) to severe (eg, Parkinsonism or a persistent vegetative state).Diagnostic EvaluationA noninvasive fingertip pulse CO-oximeter is available for rapid screening, but has poor accuracy. The diagnostic test of choice is a venous or arterial blood CO-oximeter that assesses carboxyhemoglobin (COHb) levels (<3% are normal; smokers can range 5-10%), but levels do not always correlate with symptoms or the potential for neurological sequelae. In addition, blood glucose levels should be checked if the patient is altered; female patients should receive pregnancy tests. ECG and troponin measurements may predict ongoing cardiac mortality risk in patients with cardiac ischemia. Seriously poisoned patients may have an impaired ejection fraction on echocardiography.AntidotePatients should be placed immediately on high-flow oxygen by non-rebreather. Oxygen decreases the half-life of circulating COHb from 4-5 hours to a mean of 85 min. Consider hyperbaric oxygen in patients with COHb levels >25%, syncope, abnormal neurologic exam (eg, ataxia), prolonged exposure (≥24 hours), pregnancy, or older age (>35 years).DispositionPatients can be discharged home once normal mental status and ambulation are normal. Those who remain altered or hypotensive may require admission. The initial site of CO exposure should be evaluated by fire or utility personnel to prevent further poisonings.
Reviewed by Christian Tomaszewski, MD, MS MBA, FACEP