Embed Size (px)
Citation preview

Techniques in Gastrointestinal Endoscopy 18 (2016) 22–28
Contents lists available at ScienceDirect
Techniques in Gastrointestinal Endoscopy
http://d0049-01
B.D.Chas receand anfrom PA
n CorrE-m1 G2 Co
feedbacmanusc
journal homepage: www.techgiendoscopy.com/locate/tgie
New horizons for sedation: The ultrashort acting benzodiazepineremimazolam
Daniel J. Pambiancoa,1,2,n, Brooks D. Cashb,2
a Charlottesville Medical Research, 325 Winding River Lane, Suite 102, Charlottesville, Virginia 22911b Digestive Health Center, University of South Alabama, Mobile, Alabama
a r t i c l e i n f o
Article history:Received 17 November 2015Accepted 11 February 2016
Keywords:RemimazolamBenzodiazepineProcedural sedationPharmacokineticsClinical trialsGastrointestinal endoscopy
x.doi.org/10.1016/j.tgie.2016.02.00472/& 2016 Elsevier Inc. All rights reserved.
. has served as a consultant and an advisory bived research funding from PAION. D.J.P. has sadvisory board member for PAION, and haION.esponding author.ail address: [email protected] (D.J. Puarantor of article.ntributed equally to the concept for the reviewk on previous drafts and approved the finript.
a b s t r a c t
Procedural sedation is used in 98% of endoscopies performed in the United States. The predominant agentsused are benzodiazepines, opioids, and propofol. The optimal sedation depends on the procedure beingperformed and its duration. An ideal sedative would allow for flexible, rapid onset and offset of sedationwith predictable short duration of action with minimal cardiopulmonary risk factors. Remimazolam is anovel “soft drug” with the characteristics of a benzodiazepine and organ-independent metabolism.Remimazolam binds selectively and with high affinity to the gamma-aminobutyric acid receptor, withno off-target activities. In animal studies, remimazolam has a short, initial phase half-life and high volumeof distribution, indicating extensive tissue distribution, minimal tissue accumulation, and rapid elimina-tion. Remimazolam is hydroxylated to an inactive metabolite, and its effects can be reversed withflumazenil. In clinical studies for procedural sedation, remimazolam was well tolerated with no seriousadverse events. Times to onset or offset of sedation were shorter with remimazolam versus active control.All remimazolam-related adverse reactions are well known to clinicians and can be managed by trainedstaff. This article summarizes the preclinical and clinical data on the efficacy and safety or remimazolam forendoscopic sedation. Remimazolam is in clinical development for procedural sedation, general anesthesia,and sedation in the intensive care unit. Remimazolam is a promising new sedative or anesthetic agent withscientific support for continued clinical development. Phase III studies with remimazolam for proceduralsedation are underway.
& 2016 Elsevier Inc. All rights reserved.
1. Introduction
Since the advent of fiberoptic endoscopy, in the mid 1950s, thediagnosis and treatment of gastrointestinal (GI) disorders has beentransmogrified by the use of this modality to become the primarytool used in colon cancer screening and prevention, as well as theinvestigation of abdominal pain, anemia, altered bowel habits, GIblood loss, and abnormal imaging [1]. Currently our armamen-tarium includes the use of not only routine diagnostic andtherapeutic esophagogastroduodenoscopy and colonoscopy but
oard member for PAION anderved as a speaker, consultants received research funding
ambianco).
article, provided substantialal, submitted version of the
also advanced endoscopic procedures such as endoscopic ultra-sound, double balloon enteroscopy, and endoscopic retrogradecholangiopancreatography. Simultaneously, there has been a log-arithmic growth in the use of and need for sedation, allowing forgreater patient comfort and safety in the evolution of theseerstwhile nonsurgical procedures. As the number and complexityof endoscopic procedures increase, the role of sedation has beenintegral in patient and physician satisfaction. Presently, 98% ofendoscopic procedures in the United States are performed withsedation administered by gastroenterologist or anesthesia profes-sionals [2]. However, unlike surgery that requires general anes-thesia, optimal sedation requirements for endoscopy need to bematched to patient comfort, comorbidity risks, the anticipatedprocedural discomfort, and the length of the procedure in order tominimize the unnecessary risk of deeper sedation or generalanesthesia [3]. Most of the patients require moderate sedationfor relatively short procedures for which the ideal agent or admin-istration model is still being sought.
This article focuses on the unmet needs of our current sedationpractices and the evolution and potential of the novel compound,remimazolam, an ultrashort acting benzodiazepine.

Minimal seda�on“anxiolysis”
Moderate seda�on/analgesia
“conscious seda�on” Deep seda�on/analgesia General Anesthesia
ResponsivenessNormal response
to verbal communica�on
Purposeful response to verbal or tac�le
s�mula�on
Purposeful response following repeated or
painful s�mula�on
Unarousable even with painful s�mulus
Airway Unaffected No interven�on required Interven�on may be required
Interven�on o�en required
Spontaneous Ven�la�on Unaffected Adequate May be inadequate Frequently inadequate
Cardiovascular func�on Unaffected Usually maintained Usually maintained May be impaired
Midazolam
Colonoscopy
Minor procedures
Biopsies
Major surgeryBronchoscopy
ICU seda�on
Remimazolam
MRI/Scanning procedures
Trauma (limb rese�ng, wound dressing)
Upper GI endoscopy
Propofol
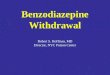
Fig. 1. Continuum of sedation: definition of general anesthesia and levels of sedation/analgesia (ASA, 1999—modified) [19] and intended use of remimazolam. (Color versionof figure is available online.)
D.J. Pambianco, B.D. Cash / Techniques in Gastrointestinal Endoscopy 18 (2016) 22–28 23
2. Sedation background
The goals of sedation are to balance patient comfort andtolerability with the risks of drug-related side effects andover sedation. It is intended to reduce patient anxiety anddiscomfort for procedures that may need to be repetitive whileallowing the endoscopist patient stability to perform a thoroughexamination [4].
Sedation has been defined as a drug-induced suppression ofconsciousness that is a continuum from anxiolysis (minimal) toconscious sedation (moderate) to unconsciousness (general anes-thesia). The American Society of Anesthesiologists (ASA) hasdeveloped and defined the continuum of sedation for medicalprocedures of varying invasiveness (Figure 1). The ability toachieve and maintain the balance of appropriate necessary depthof individualized sedation with minimal adversity is a combinationof expertise and pharmacology.
Currently, midazolam and propofol are the most commonly usedintravenous (IV) sedatives used for procedural sedation often inconjunctionwith IV opioids [5], however each agent has disadvantages.
Propofol, an anesthetic alkylphenol, is an IV sedative orhypnotic that is used for sedation and general anesthesia in higherdoses. Among its major advantages for brief procedural sedationsuch as endoscopy are its exceptional sedative properties with fastinduction and extremely short half-life, allowing for rapid recoveryfrom sedation and rapid discharge from the endoscopy suite.However, there are some safety and tolerability concerns, includ-ing injection site pain, susceptibility to bacterial contamination,and cardiovascular and respiratory depression. The induction ormaintenance dosing to effect-site concentration is not linear owingto tissue compartment variability, and repeated or prolongedadministration can lead to unpredictable clinical consequences,predominantly apnea, and hypotension. As a result of this potentialnarrow therapeutic window, rapid progression to respiratorydepression and hypoxia can cause the potential need for respira-tory rescue with endotracheal intubation. Consequently, thepresence of an anesthesia professional is required to monitor the
patient and manage the level of sedation for the endoscopicprocedure [6,7].
Benzodiazepines were discovered in the 1950s with the van-guard of chlordiazepoxide and later diazepam, the latter of whichwas widely used for endoscopic sedation until the advent ofmidazolam in the 1980s. Owing to midazolam's water solubility,which eliminated pain on injection and its shorter half-life, itusurped the use of diazepam [8].
Midazolam is considered a safe and effective sedation agent.The mean elimination half-life of midazolam is about 3 hours(range: 1.8-6.4 hour), and it is metabolized by cytochrome P450-3A4. It is well established that individual variability in P450activity and interactions with drugs that inhibit or activate the3A4 system can contribute to the unpredictability in onset orduration of midazolam's sedative effects. As such and similar topropofol, plasma effect-site concentration after an IV dose and itsrelationship to pharmacodynamic measures (ie, reaction time, eyemovement, sedation depth) have shown extensive intersubjectvariability [9].
Moreover, midazolam is hydroxylated into active and inactivemetabolites, which can increase the risk of excessive sedation bydrug interactions. About 60%-70% of the biotransformation prod-uct is 1-hydroxy-midazolam (alpha-hydroxy-midazolam), whichis at least as potent as the parent compound and may contributeto the net pharmacologic activity of midazolam [9]. Midazolamaccumulates with renal impairment, prolonged infusion, and afterrepeated single dose infusions—a common dosing schedule dur-ing short, conscious sedation administration. Owing to thesevariable pharmacokinetic and pharmacodynamic effects, midazo-lam can be difficult to titrate and may produce prolongedsedation, thus delaying recovery. These characteristics makemidazolam a suboptimal candidate as a sedative or anestheticagent.
The development of new sedative and anesthetic drugs overthe last decade has been driven by the changing demands ofclinical practice, where procedures once performed in the hospitalare now performed in ambulatory settings, on an increasingly

N
N
NN
BrO
O
CH3
Remimazolam
Diazepam(1960s)
Midazolam(1980s)
Lorazepam(1970s)
Benzodiazepine Safety
• Aqueous solubility• Availability of antagonist• No injection pain• Respiratory depression• Risk for CV effects• Anxiolysis• Amnesia
Fentanyl(1960s)
Remifentanil(1990s)
Ester Technology
• Short duration of action• Predictable response• Inactive metabolite
Rapid Onset/Offset
Dexmedetomidine(1990s)
Ketamine(1960s)
• Rapid onset• Rapid offset• Predictable response
Propofol(1980s)
Etomidate(1960s)
GABAA Mechanism
• No psychomimetic effects• Control of major inhibitory NT
Fig. 2. Pharmacological milestones leading to the development of remimazolam.
D.J. Pambianco, B.D. Cash / Techniques in Gastrointestinal Endoscopy 18 (2016) 22–2824
elderly population with multiple comorbidities [5]. As per theAmerican Gastroenterological Association—
The ideal agent for endoscopic sedation should possess seda-tive, analgesic, and amnestic properties and a pharmacokineticprofile compatible with rapid onset (1-2 min), brief duration(5-10 min), and fast recovery (15-20 min). It also should pro-vide a predictable pharmacodynamic response within the rangeof moderate sedation, exert minimal depressant effects on thecardiopulmonary system, and possess a pharmacologic antag-onist. Finally, its use by an endoscopist and/or nurse shouldcomply with state and federal regulations, and it should be costeffective compared with current methods of sedation [10].
These demands and recent advances in clinical pharmacologyhave led to the concept of “soft” drugs, which are designed to be
Fig. 3. Pharmacokinetics of remimazolam and its inactive m
safer with an increased therapeutic index and a rapid predictablemetabolism to inactive metabolites [11].
3. Remimazolam
3.1. Historical overview
Midazolam is the parent compound of remimazolam; therefore,remimazolam has the characteristic safety profile of a benzodia-zepine and a gamma-aminobutyric acid (GABAA) neurotransmitterreceptor mechanism of action. Remimazolamwas created as a newcandidate compound after a confluence of historical milestones inpharmacology [12] (Figure 2). The critical step in the creation ofremimazolam was the addition of a carboxylic ester linkage to themolecule, as was also done with an analgesic compound inwidespread use, remifentanil. This technology creates a “soft drug”
etabolite. (Color version of figure is available online.)

Remimazolam(CNS 7056)
CNS 7054(inac�ve metabolite)
NO
OMe
N
NN
Br NO
OH
N
NN
Br
Carboxylesterases
Fig. 4. Metabolism of remimazolam.
D.J. Pambianco, B.D. Cash / Techniques in Gastrointestinal Endoscopy 18 (2016) 22–28 25
that allows for organ-independent metabolism of remimazolam bynonspecific and widespread tissue esterases, for which there areno known deficiency conditions. Importantly, it allows for rapidonset of sedation and a rapid offset with a predictable shortduration of action and a favorable cardiostability profile [11]. Withthe unique characteristics of a benzodiazepine, remimazolam haspotential for 3 main indications: procedural sedation, generalanesthesia, and sedation in the intensive care unit.
3.2. Preclinical trials
Remimazolam binds selectively and with high affinity to brainbenzodiazepine sites (GABAA receptor), with no evidence of off-target activities. The same properties were demonstrated for itsprincipal metabolite, CNS7054, which displayed a 417-fold loweraffinity than its parent compound in homogenates of human braintissue [13].
In all animal species studied, remimazolam showed sedativeactivity with a rapid onset, short duration, and reversal withflumazenil. Remimazolam showed inhibition of human ether-a-go-go-related gene (hERG) tail currents at concentrations wellabove those required to activate GABAA receptors in vitro, andconsiderably higher than free plasma levels reached in anytoxicology or human study. Deep sedation was observed withoutexcessive respiratory or cardiovascular depression in pigs, sheep,and monkeys [14].
In various animal species, a very short initial phase half-lifeand high volume of distribution were observed, indicatingrapid elimination after extensive tissue distribution (Figure 3).
Fig. 5. Therapeutic window in animals and human
Distribution studies showed minimal accumulation in any tissue.The main route of metabolism of remimazolam is via the inactivemetabolite CNS7054, which is subject to hydroxylation andglucuronidation (Figure 4). The hydrolyzation of CNS7056 toCNS7054 is catalyzed by tissue carboxylesterases, without invol-vement of cytochrome P450 isoenzymes [14]. Moreover, remi-mazolam causes no relevant inhibition of the studied cytochromeP450 isoenzymes, nor are there inducing effects on CYP iso-enzymes when studied in vitro [14].
Results from preclinical studies showed remimazolam to havepredictable PD and PK profiles, with rapid onset and offset ofaction [14]. Remimazolam-induced sedation can be effectivelyreversed with flumazenil, and hypotension is not observed withphysiologically relevant doses of remimazolam. Importantly, thereis a wide therapeutic window between therapeutic doses and toxicdoses (Figure 5).
3.3. Clinical trials
3.3.1. Phase I: First-in-man studyThe first-in-man trial of remimazolam (CNS7056-001) was a
double-blind, single dose, phase I trial enrolling healthy volunteersin the United States (N ¼ 81) [15]. Subjects were randomized toreceive remimazolam, placebo, or midazolam (6:1:3); 9 cohorts ofsubjects received escalating doses of remimazolam (0.01-0.30 mg/kg)via IV infusion for 1 minute. The stopping rule was loss of conscious-ness (LoC); Modified Observer's Assessment of Alertness/SedationScale (MOAA/S) o2 for Z5 minutes in 450% of subjects in anysingle dose cohort [15] (Table 1).
Remimazolam was well tolerated at all doses administered andno SAEs (serious adverse events) were reported. Airway patencyand spontaneous respiration were maintained throughout the trialwith no requirement for mechanical ventilation in any patient.Remimazolam safely and rapidly induced sedation at dosesZ0.05 mg/kg. The depth and duration of sedation appeared tobe sufficient to allow a short procedure requiring proceduralsedation at doses of Z0.075 mg/kg. Offset of sedation was rapid(�10 minutes at doses of 0.075-0.20 mg/kg) compared withmidazolam (�40 minutes at 0.075 mg/kg). Other results aresummarized in Table 2.
s. (Color version of figure is available online.)

Table
1Description
ofco
mpletedan
dplanned
clinical
trials
ofremim
azolam
forprocedu
ralsedation.
Article
orNCT/(study#)
Studydesign
Population
N(total)
N(REM
)REM
doses
Endpoints
Studydates
Antonik
etal
[15]
PI,R
,DB,P
C,A
C(m
idazolam
),SA
DUSvo
lunteers(18-55
y)81
540.01
-0.30mg/kg
Safety
andPK
;bloo
d,v
itals,
ECG,B
IS,M
OAA/S
July-N
ovem
ber,20
08
Worthington
etal
[16]
PIb,
2parts:DB,P
C(flumazen
ilreve
rsal);
OL(doseescalation
)USvo
lunteers(18-75
y)51
51Pt
A:0.25
mg/kg
PtB:
0.04
-0.10mg/kg
Safety,P
K,a
ndPD
colonosco
pyApril-Se
ptem
ber,20
09
Borke
ttet
al[17]
PIIa,R
,DB,A
C(m
idazolam
),dosefinding
USpatients
(18-65
y)undergo
ingEG
D10
075
0.10
-0.20mg/kg
Safety,e
fficacy,M
OAA/S
April-Se
ptem
ber,20
09
Pambian
coet
al[18]
PIIb,R
,DB,A
C(m
idazolam
),doseresp
onse
USPa
tien
ts(18-70
y)undergo
ing
colonosco
py16
012
05.0or
8.0mg(3.0
mgtop-ups),
7.0mg(2.0
mgtop-ups)
Safety,e
fficacy,M
OAA/S,
Aldrete
score
May
-Sep
tembe
r,20
10
NCT
0229
0873
(CNS70
56-0
06)
PIII,R
,DB,P
C,A
C(m
idazolam
)Pa
tien
ts(Z
18y)
undergo
ing
colonosco
py46
030
0Induction:5mgmaintenan
ce:
2.5mg
Proc
edure
success,
times
tostart/pea
ksedation
Plan
ned
for20
14/201
5
NCT
0229
6892
(CNS70
56-0
08)
PIII,R
,DB,P
C,A
C(m
idazolam
)Pa
tien
ts(Z
18y)
undergo
ing
bron
chosco
py46
030
0Induction:5mgmaintenan
ce:
2.5mg
Proc
edure
success,
times
tostart/pea
ksedation
Plan
ned
for20
14/201
5
(CNS70
56-0
05)
PI,R
,DB,S
D,þC(m
oxiflox
acin),
AC(m
idazolam
),CO
Thorou
ghQT
5454
10or
20mg
QTc
intervals,
ECG
param
eters,
PK20
15
(CNS70
56-012
)PI,O
L,SD
Ren
alinsu
fficien
cy16
161.5mg
PK,s
afety
2015
(CNS70
56-014
)PI,R
,DB,S
D,A
C(m
idazolam
),CO
Abu
selia
bility
4040
5or
10mg
Abu
sepoten
tial,P
D/PK
2015
(CNS70
56-015
)PIII,R
,DB,P
C,A
C(m
idazolam
)Pa
tien
ts(Z
18y)
withASA
III/IV
undergo
ingco
lonosco
py75
30Induction:5mgmaintenan
ce:
2.5mg
Safety,p
rocedure
success
Plan
ned
for20
15
Abb
reviations:
AC,active
controlled;BIS,bisp
ectral
index
;þC,positiveco
ntrolled;CO,crossove
r;DB,dou
bleblind;EC
G,electroc
ardiog
ram;Lo
C,loss
ofco
nsciousn
ess;
OL,
open
labe
l;P,
phase;
PC,placebo
controlled;PD
,pharmacod
ynam
ics;
PK,p
harmacok
inetics;
R,ran
domized
;REM
,rem
imazolam
;SA
D,single,
ascendingdose;
SD,s
ingledose;
US,
United
States.
D.J. Pambianco, B.D. Cash / Techniques in Gastrointestinal Endoscopy 18 (2016) 22–2826
3.3.2. Phase Ib: Multiple dose colonoscopy studyThe phase Ib study (CNS7056-002) was comprised of 2 parts
part A was a double-blind, placebo-controlled, crossover trialevaluating the efficacy of flumazenil as a reversal agent forremimazolam in healthy volunteers (N ¼ 6). Subjects received a1-minute IV infusion of 0.25 mg/kg remimazolam and 3 minutesafter successful sedation (MOAA/S score r3) subjects received0.5 mg flumazenil or placebo. Alternate treatment was adminis-tered on the following day. In the flumazenil and placebo groups,the median times to fully alert (first of 3 consecutive MOAA/Sscores ¼ 5) were 1.0 and 10.5 minutes, respectively [16].
Part B was an open-label, dose-escalation study investigatingthe efficacy of remimazolam in combination with fentanyl insubjects undergoing colonoscopy (N ¼ 45). The initial dose ofremimazolam was 0.04-0.10 mg/kg, followed by up to 6 top-updoses of 0.04 mg/kg as necessary to induce and maintain sedationduring the procedure. Remimazolam was well tolerated at alldoses administered and no SAEs were reported. Remimazolamhad a rapid time to onset of sedation (0.18-0.40 minute) and timeto recovery, with the mean time to becoming fully alert rangingfrom 6.9-9.8 minutes. Overall, the depth and duration of sedationwas sufficient to achieve successful procedures for 64%-100% ofsubjects in each dose cohort [16].
3.3.3. Phase IIa: Single dose endoscopy studyA randomized, double-blind, dose finding, phase IIa trial
(CNS7056-003) evaluated the safety and efficacy of 3, single doses(ie, no top-ups) of remimazolam (0.10, 0.15, or 0.20 mg/kg) vs asingle dose of midazolam (0.075 mg/kg) in patients undergoing adiagnostic upper GI endoscopy (N ¼ 100) [17]. All 3 doses ofremimazolam were well tolerated and no SAEs were reported.Remimazolam had a rapid onset and offset of sedation and thedepth and duration of sedation were sufficient to achieve success-ful procedures for 32%-64% of patients who received remimazolamin the lowest and highest dose groups, respectively. The successrate was 44% with midazolam [17].
3.3.4. Phase IIb: Multiple dose colonoscopy studyThe safety and efficacy of multiple doses of remimazolam
were evaluated in a phase IIb study versus midazolam in patientsundergoing colonoscopy (CNS7056-004) [18]. This is the firststudy to use fixed doses of remimazolam and patients wererandomized to the following 3 loading/top-up combinations:8.0 mg/3.0 mg, 7.0 mg/2.0 mg, and 5.0 mg/3.0 mg. Patientsrandomized to midazolam received 2.5 mg/1.0 mg. A total of160 patients entered the study. All doses of remimazolam werewell tolerated and no SAEs were reported. In the remimazolamgroups, mean times to peak sedation ranged from 2.7-4.4minutes; the mean time in the midazolam group was 6.4 minutes.Mean times to fully alert ranged from 11.3-13.6 minutes in theremimazolam groups and 15.2 minutes in the midazolam group.The depth and duration of sedation were sufficient to achievesuccessful procedures in Z92% of all patients who receivedremimazolam and in 75% of patients who received midazolam(P r 0.007) [18].
3.4. Safety profile of remimazolam
For the procedural sedation, remimazolam has shown a safetyprofile similar to that of midazolam. In studies for this indication,240 patients received remimazolam (0.1, 0.15, and 0.2 mg/kg;5 mg/3 mg, 7 mg/2 mg, and 8 mg/3 mg), and 66 patients receivedmidazolam (0.075 mg/kg and 2.5 mg/1 mg). There were no appa-rent differences in oxygen saturation between remimazolam andmidazolam groups, and the number of respiratory events and

Table 2Summary of results from completed clinical trials of remimazolam for procedural sedation.
Article Dose groups End points
Antonik et al [15] Onset of sedation, m Offset of sedation, m Sedation level (MOAS/S)0.01-0.05 n/a n/a None—Limited (4-5)0.075-0.20 o1 710 710 m: medium (↓ to 1.5)0.25-0.30 o1 730 730 m: LoC (↓ to 0)
Worthington et al [16] Time to LoC, m Time to awake, m Success rate (%) Time to discharge, m0.04 0.33 9.8 66.7 23.80.075 0.40 9.6 100 24.10.10 0.18 6.9 64.3 19.3
Borkett et al [17] Time to LoC, m Time to awake, m Success rate (%) Time to discharge, m0.10 90 11.0 32 14.00.15 NR 13.4 56 12.80.20 150 12.1 64 11.8
Pambianco et al [18] Time to peak sedation, m Time to awake, m Success rate (%) Time to discharge, m5.0/3.0 4.4 13.3 97.5 11.37.0/2.0 4.0 11.3 95.0 12.48.0/3.0 2.7 13.6 92.5 14.6
Abbreviation: LoC, loss of consciousness.
D.J. Pambianco, B.D. Cash / Techniques in Gastrointestinal Endoscopy 18 (2016) 22–28 27
airway interventions (chin lifts and jaw thrusts) were low andsimilar among all groups. No ventilator support was necessary inany patient and there were no SAEs.
3.5. Discussion
As with other benzodiazepines, there is likely to be an increasedrisk of apnea, airway obstruction, desaturation, or hypoventilationin the presence of alcohol or other CNS depressants. Similarly, thereis the likelihood of an increase in any hypnotic effects of remima-zolam if opioids are used as concomitant medications. Theserisks are managed by omitting or reducing the doses of concom-itant narcotics for esophagogastroduodenoscopy and colonoscopy,respectively, similar to the risk mitigation strategies of otherbenzodiazepines. All of the above mentioned adverse reactionsare well known to clinicians and can be appropriately managedby adequately trained staff. Finally, as with all benzodiazepines, thereversal agent, flumazenil could be used as a rescue medicationfrom deeper than intended levels of sedation, in addition to otherroutine airway management practices [16].
4. Conclusions
Remimazolam, a new “soft drug” for sedation and anesthesia,has the characteristic safety profile of a benzodiazepine and aGABAA receptor mechanism of action, with a rapid onset, predict-able course, and rapid offset of action. For procedural sedation,results from 2 phase I studies suggest that remimazolam showslinear PK, was well tolerated at all doses tested, and fully reversiblewith flumazenil. In 2 phase II trials, remimazolam demonstratedefficacy during GI endoscopy and colonoscopy. Phase III studies areplanned or are underway to confirm the phase II findings forendoscopy/colonoscopy and to evaluate the efficacy of remimazo-lam in more seriously ill patients (ASA III/IV) undergoing colono-scopy. Additional phase III trials with remimazolam for theindications of sedation, general anesthesia and intensive care unitsedation are underway or planned.
The phase III program currently underway for the proceduralsedation indication consists of 2 confirmatory trials using 2procedure models: bronchoscopy and colonoscopy. Both trialswould be placebo and active controlled (ie, midazolam) to provideconfirmatory evidence of the safety and efficacy of remimazolamfor procedural sedation. In parallel to the 2 confirmatory trials, aseparate trial in ASA III/IV patients undergoing colonoscopy would
be conducted. These trials would be placebo and active controlled(ie, midazolam) focusing on the evaluation of the safety ofremimazolam in patients with poorer health status.
If these findings are confirmed in the phase III studies, it isexpected that remimazolam can be used like midazolam in thesetting of procedural sedation but with a faster and more predict-able clinical onset and offset. A sedation profile with a rapid reachof peak sedationwithin 1-2 minutes and rapid offset is comparableto propofol but with a broader therapeutic window, which maylead to more timely starts of procedures and should be expected tolead to increased patient satisfaction.
References
[1] Wilcox CM. Fifty years of gastroenterology at the University of Alabama atBirmingham: a festschrift for Dr. Basil I. Hirschowitz. Am J Med Sci 2009;338:84–8.
[2] Cohen LB, Wecsler JS, Gaetano JN, Benson AA, Miller KM, Durkalski V, et al.Endoscopic sedation in the United States: results from a nationwide survey.Am J Gastroenterol 2006;101:967–74.
[3] Green SM. Research advances in procedural sedation and analgesia. AnnEmerg Med 2007;49:31–6.
[4] American Association for Study of Liver D, American College of G, AmericanGastroenterological Association I, American Society for Gastrointestinal E,Society for Gastroenterology N, Associates, et al. Multisociety sedationcurriculum for multisociety gastrointestinal endoscopy. Gastrointest Endosc2012, 76: e1–e25.
[5] Inadomi JM, Gunnarsson CL, Rizzo JA, Fang H. Projected increased growth rateof anesthesia professional-delivered sedation for colonoscopy and EGD in theUnited States: 2009 to 2015. Gastrointest Endosc 2010;72:580–6.
[6] Hemmings HJ. The pharmacology of intravenous anesthetic induction agents:a primer. Anesthesiology News. New York: McMahon Publishing; 2010, 9–16.
[7] Perouansky M, Hemmings HJ. Intravenous anesthetic agents. In: HemmingsHJ, Hopkins P, editors. Foundatons of Anesthsia: Basic Science and ClinicalPractice. 2nd ed. London: Mosby Elsevier; 2005. p. 295–310.
[8] Olkkola KT, Ahonen J. Midazolam and other benzodiazepines. Handbook ofExperimental Pharmacology 2008;182:335–60.
[9] Roche Pharmaceuticals. Versed (midazolam HCL injection): Full PrescribingInformation. Nutley, NJ; 1999.
[10] Cohen LB, Delegge MH, Aisenberg J, Brill JV, Inadomi JM, Kochman ML, et al.AGA institute review of endoscopic sedation. Gastroenterology 2007;133:675–701.
[11] Egan TD. Is anesthesiology going soft?: Trends in fragile pharmacology.Anesthesiology 2009;111:229–30.
[12] Feldman PL, James MK, Brackeen MF, Bilotta JM, Schuster SV, Lahey AP, et al.Design, synthesis, and pharmacological evaluation of ultrashort- to long-acting opioid analgetics. J Med Chem 1991;34:2202–8.
[13] Kilpatrick GJ, McIntyre MS, Cox RF, Stafford JA, Pacofsky GJ, Lovell GG, et al.CNS 7056: a novel ultra-short-acting benzodiazepine. Anesthesiology 2007;107:60–6.
[14] Ono Pharmaceutical Co. Ltd. Data on file. Osaka, Japan.[15] Antonik LJ, Goldwater DR, Kilpatrick GJ, Tilbrook GS, Borkett KM. A placebo-
and midazolam-controlled phase I single ascending-dose study evaluating the

D.J. Pambianco, B.D. Cash / Techniques in Gastrointestinal Endoscopy 18 (2016) 22–2828
safety, pharmacokinetics, and pharmacodynamics of remimazolam (CNS7056): part I. safety, efficacy, and basic pharmacokinetics. Anesth Analg 2012;115:274–83.
[16] Worthington MT, Antonik LJ, Goldwater DR, Lees JP, Wilhelm-Ogunbiyi K,Borkett KM, et al. A phase Ib, dose-finding study of multiple doses ofremimazolam (CNS 7056) in volunteers undergoing colonoscopy. AnesthAnalg 2013;117:1093–100.
[17] Borkett KM, Riff DS, Schwartz HI, Winkle PJ, Pambianco DJ, Lees JP, et al. APhase IIa, randomized, double-blind study of remimazolam (CNS 7056) versus
midazolam for sedation in upper gastrointestinal endoscopy. Anesth Analg2015;120:771–80.
[18] Pambianco DJ, Borkett KM, Riff DS, Winkle PJ, Schwartz HI, Melson TI, et al.A phase IIb study comparing the safety and efficacy of remimazolamand midazolam in patients undergoing colonoscopy. Gastrointest Endosc2015. http://dx.doi.org/10.1016/j.gie.2015.08.062 [Epub ahead of print].
[19] American Society of Anesthesiologists. Standard of Care Continuum ofDepth Sedation. Sample Policy and Procedure Statements. Schaumburg, IL:ASA; 1999.