Embed Size (px)
Citation preview

VYVANSE- lisdexamfetamine dimesylate capsule VYVANSE- lisdexamfetamine dimesylate tablet, chewable Takeda Pharmaceuticals America, Inc.----------
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use VYVANSE safely andeffectively. See full prescribing information for VYVANSE.
VYVANSE (lisdexamfetamine dimesylate) capsules, for oral use, CIIVYVANSE (lisdexamfetamine dimesylate) chewable tablets, for oral use, CIIInitial U.S. Approval: 2007
WARNING: ABUSE AND DEPENDENCESee full prescribing information for complete boxed warning.
CNS stimulants, including VYVANSE, other amphetamine-containing products, andmethylphenidate have a high potential for abuse and dependence (5.1, 9.3)Assess the risk of abuse prior to prescribing and monitor for signs of abuse anddependence while on therapy (5.1, 9.2)
RECENT MAJOR CHANGES
Indications and Usage (1) 7/2021Warnings and Precautions (5.5) 7/2021
INDICATIONS AND USAGEVYVANSE is a central nervous system (CNS) stimulant indicated for the treatment of (1):
Attention Deficit Hyperactivity Disorder (ADHD) in adults and pediatric patients 6 years and olderModerate to severe binge eating disorder (BED) in adults
Limitations of Use:Pediatric patients with ADHD younger than 6 years of age experienced more long-term weight loss thanpatients 6 years and older (8.4)VYVANSE is not indicated for weight loss. Use of other sympathomimetic drugs for weight loss has beenassociated with serious cardiovascular adverse events. The safety and effectiveness of VYVANSE forthe treatment of obesity have not been established (5.2)
DOSAGE AND ADMINISTRATION
IndicatedPopulation Initial Dose Titration
Schedule Recommended Dose Maximum DoseADHD (Adults andpediatric patients 6years and older) (2.2)
30 mg everymorning
10 mg or 20 mgweekly 30 mg to 70 mg per day 70 mg per day
BED (Adults) (2.3) 30 mg everymorning 20 mg weekly 50 mg to 70 mg per day 70 mg per day
Prior to treatment, assess for presence of cardiac disease (2.4)Severe renal impairment: Maximum dose is 50 mg/day (2.5)End stage renal disease (ESRD): Maximum dose is 30 mg/day (2.5)
DOSAGE FORMS AND STRENGTHSCapsules: 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg, 70 mg (3)Chewable tablets: 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg (3)
CONTRAINDICATIONS
®®

CONTRAINDICATIONSKnown hypersensitivity to amphetamine products or other ingredients in VYVANSE (4)Use with monoamine oxidase (MAO) inhibitor, or within 14 days of the last MAO inhibitor dose (4, 7.2)
WARNINGS AND PRECAUTIONSSerious Cardiovascular Reactions: Sudden death has been reported in association with CNS stimulanttreatment at recommended doses in pediatric patients with structural cardiac abnormalities or otherserious heart problems. In adults, sudden death, stroke, and myocardial infarction have been reported.Avoid use in patients with known structural cardiac abnormalities, cardiomyopathy, serious heartarrhythmia, or coronary artery disease (5.2)Blood Pressure and Heart Rate Increases: Monitor blood pressure and pulse. Consider benefits andrisks before use in patients for whom blood pressure increases may be problematic (5.3)Psychiatric Adverse Reactions: May cause psychotic or manic symptoms in patients with no priorhistory, or exacerbation of symptoms in patients with pre-existing psychosis. Evaluate for bipolardisorder prior to stimulant use (5.4)Suppression of Growth: Monitor height and weight in pediatric patients during treatment (5.5)Peripheral Vasculopathy, including Raynaud's phenomenon: Stimulants are associated with peripheralvasculopathy, including Raynaud's phenomenon. Careful observation for digital changes is necessaryduring treatment with stimulants (5.6)Serotonin Syndrome: Increased risk when co-administered with serotonergic agents (e.g., SSRIs, SNRIs,triptans), but also during overdosage situations. If it occurs, discontinue VYVANSE and initiatesupportive treatment (4, 5.7, 10)
ADVERSE REACTIONSMost common adverse reactions (incidence ≥5% and at a rate at least twice placebo) in pediatric patientsages 6 to 17 years, and/or adults with ADHD were anorexia, anxiety, decreased appetite, decreasedweight, diarrhea, dizziness, dry mouth, irritability, insomnia, nausea, upper abdominal pain, and vomiting(6.1)Most common adverse reactions (incidence ≥ 5% and at a rate at least twice placebo) in adults with BEDwere dry mouth, insomnia, decreased appetite, increased heart rate, constipation, feeling jittery, andanxiety (6.1)
To report SUSPECTED ADVERSE REACTIONS, contact Takeda Pharmaceuticals at 1-800-828-2088 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONSAcidifying and Alkalinizing Agents: Agents that alter urinary pH can alter blood levels of amphetamine.Acidifying agents decrease amphetamine blood levels, while alkalinizing agents increase amphetamineblood levels. Adjust VYVANSE dosage accordingly (2.6, 7.1)
USE IN SPECIFIC POPULATIONSPregnancy: May cause fetal harm (8.1)Lactation: Breastfeeding not recommended (8.2)
See 17 for PATIENT COUNSELING INFORMATION and Medication Guide.Revised: 7/2021
FULL PRESCRIBING INFORMATION: CONTENTS*WARNING: ABUSE AND DEPENDENCE1 INDICATIONS AND USAGE2 DOSAGE AND ADMINISTRATION
2.1 Pre-treatment Screening2.2 General Instructions for Use2.3 Dosage for Treatment of ADHD2.4 Dosage for Treatment of Moderate to Severe BED in Adults2.5 Dosage in Patients with Renal Impairment2.6 Dosage Modifications due to Drug Interactions

3 DOSAGE FORMS AND STRENGTHS4 CONTRAINDICATIONS5 WARNINGS AND PRECAUTIONS
5.1 Potential for Abuse and Dependence5.2 Serious Cardiovascular Reactions5.3 Blood Pressure and Heart Rate Increases5.4 Psychiatric Adverse Reactions5.5 Suppression of Growth5.6 Peripheral Vasculopathy, including Raynaud's Phenomenon5.7 Serotonin Syndrome
6 ADVERSE REACTIONS6.1 Clinical Trials Experience6.2 Postmarketing Experience
7 DRUG INTERACTIONS7.1 Drugs Having Clinically Important Interactions with Amphetamines7.2 Drugs Having No Clinically Important Interactions with VYVANSE
8 USE IN SPECIFIC POPULATIONS8.1 Pregnancy8.2 Lactation8.4 Pediatric Use8.5 Geriatric Use8.6 Renal Impairment
9 DRUG ABUSE AND DEPENDENCE9.1 Controlled Substance9.2 Abuse9.3 Dependence
10 OVERDOSAGE11 DESCRIPTION12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action12.2 Pharmacodynamics12.3 Pharmacokinetics
13 NONCLINICAL TOXICOLOGY13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility13.2 Animal Toxicology and/or Pharmacology
14 CLINICAL STUDIES14.1 Attention Deficit Hyperactivity Disorder (ADHD)14.2 Binge Eating Disorder (BED)
16 HOW SUPPLIED/STORAGE AND HANDLING16.1 How Supplied16.2 Storage and Handling
17 PATIENT COUNSELING INFORMATION*
FULL PRESCRIBING INFORMATION
Sections or subsections omitted from the full prescribing information are not listed.

WARNING: ABUSE AND DEPENDENCECNS stimulants, including VYVANSE, other amphetamine-containingproducts, and methylphenidate, have a high potential for abuse anddependence. Assess the risk of abuse prior to prescribing and monitorfor signs of abuse and dependence while on therapy [see Warnings andPrecautions (5.1), and Drug Abuse and Dependence (9.2, 9.3)].
1 INDICATIONS AND USAGEVYVANSE is indicated for the treatment of:
Attention Deficit Hyperactivity Disorder (ADHD) in adults and pediatric patients 6years and older [see Clinical Studies (14.1)]Moderate to severe binge eating disorder (BED) in adults [see Clinical Studies (14.2)].
Limitations of Use:Pediatric patients with ADHD younger than 6 years of age experienced more long-term weight loss than patients 6 years and older [see Use in Specific Populations(8.4)].VYVANSE is not indicated or recommended for weight loss. Use of othersympathomimetic drugs for weight loss has been associated with seriouscardiovascular adverse events. The safety and effectiveness of VYVANSE for thetreatment of obesity have not been established [see Warnings and Precautions (5.2)].
2 DOSAGE AND ADMINISTRATION
2.1 Pre-treatment ScreeningPrior to treating patients with CNS stimulants, including VYVANSE, assess for thepresence of cardiac disease (e.g., a careful history, family history of sudden death orventricular arrhythmia, and physical exam) [see Warnings and Precautions (5.2)].To reduce the abuse of CNS stimulants including VYVANSE, assess the risk of abuse,prior to prescribing. After prescribing, keep careful prescription records, educatepatients about abuse, monitor for signs of abuse and overdose, and re-evaluate theneed for VYVANSE use [see Warnings and Precautions (5.1), Drug Abuse andDependence (9)].
2.2 General Instructions for UseTake VYVANSE by mouth in the morning with or without food; avoid afternoon dosesbecause of the potential for insomnia. VYVANSE may be administered in one of thefollowing ways:Information for VYVANSE capsules:
Swallow VYVANSE capsules whole, orOpen capsules, empty and mix the entire contents with yogurt, water, or orangejuice. If the contents of the capsule include any compacted powder, a spoon may beused to break apart the powder. The contents should be mixed until completelydispersed. Consume the entire mixture immediately. It should not be stored. The
®

dispersed. Consume the entire mixture immediately. It should not be stored. Theactive ingredient dissolves completely once dispersed; however, a film containing theinactive ingredients may remain in the glass or container once the mixture isconsumed.
Information for VYVANSE chewable tablets:VYVANSE chewable tablets must be chewed thoroughly before swallowing.
VYVANSE capsules can be substituted with VYVANSE chewable tablets on a unit perunit/mg per mg basis (for example, 30 mg capsules for 30 mg chewable tablet) [seeClinical Pharmacology (12.3)].Do not take anything less than one capsule or chewable tablet per day. A single doseshould not be divided.
2.3 Dosage for Treatment of ADHDThe recommended starting dosage in adults and pediatric patients 6 years and older is30 mg once daily in the morning. Dosage may be adjusted in increments of 10 mg or 20mg at approximately weekly intervals up to maximum recommended dosage of 70 mgonce daily [see Clinical Studies (14.1)].
2.4 Dosage for Treatment of Moderate to Severe BED in AdultsThe recommended starting dosage in adults is 30 mg once daily to be titrated inincrements of 20 mg at approximately weekly intervals to achieve the recommendedtarget dose of 50 mg to 70 mg once daily. The maximum recommended dosage is 70mg once daily [see Clinical Studies (14.2)]. Discontinue VYVANSE if binge eating does notimprove.
2.5 Dosage in Patients with Renal ImpairmentIn patients with severe renal impairment (GFR 15 to < 30 mL/min/1.73 m ), themaximum dosage should not exceed 50 mg once daily. In patients with end stage renaldisease (ESRD, GFR < 15 mL/min/1.73 m ), the maximum recommended dosage is 30mg once daily [see Use in Specific Populations (8.6)].
2.6 Dosage Modifications due to Drug InteractionsAgents that alter urinary pH can impact urinary excretion and alter blood levels ofamphetamine. Acidifying agents (e.g., ascorbic acid) decrease blood levels, whilealkalinizing agents (e.g., sodium bicarbonate) increase blood levels. Adjust VYVANSEdosage accordingly [see Drug Interactions (7.1)].
3 DOSAGE FORMS AND STRENGTHSVYVANSE (lisdexamfetamine dimesylate) capsules:
Capsules 10 mg: pink body/pink cap (imprinted with S489 and 10 mg)Capsules 20 mg: ivory body/ivory cap (imprinted with S489 and 20 mg)Capsules 30 mg: white body/orange cap (imprinted with S489 and 30 mg)Capsules 40 mg: white body/blue green cap (imprinted with S489 and 40 mg)Capsules 50 mg: white body/blue cap (imprinted with S489 and 50 mg)Capsules 60 mg: aqua blue body/aqua blue cap (imprinted with S489 and 60 mg)
2
2

Capsules 70 mg: blue body/orange cap (imprinted with S489 and 70 mg)
VYVANSE (lisdexamfetamine dimesylate) chewable tablets:Chewable tablets 10 mg: White to off-white round shaped tablet debossed with '10'on one side and 'S489' on the otherChewable tablets 20 mg: White to off-white hexagonal shaped tablet debossed with'20' on one side and 'S489' on the otherChewable tablets 30 mg: White to off-white arc triangular shaped tablet debossedwith '30' on one side and 'S489' on the otherChewable tablets 40 mg: White to off-white capsule shaped tablet debossed with '40'on one side and 'S489' on the otherChewable tablets 50 mg: White to off-white arc square shaped tablet debossed with'50' on one side and 'S489' on the otherChewable tablets 60 mg: White to off-white arc diamond shaped tablet debossed with'60' on one side and 'S489' on the other
4 CONTRAINDICATIONSVYVANSE is contraindicated in patients with:
Known hypersensitivity to amphetamine products or other ingredients of VYVANSE.Anaphylactic reactions, Stevens-Johnson Syndrome, angioedema, and urticaria havebeen observed in postmarketing reports [see Adverse Reactions (6.2)].Patients taking monoamine oxidase inhibitors (MAOIs), or within 14 days of stoppingMAOIs (including MAOIs such as linezolid or intravenous methylene blue), because ofan increased risk of hypertensive crisis [see Warnings and Precautions (5.7) andDrug Interactions (7.1)].
5 WARNINGS AND PRECAUTIONS
5.1 Potential for Abuse and DependenceCNS stimulants, including VYVANSE, other amphetamine-containing products, andmethylphenidate, have a high potential for abuse and dependence. Assess the risk ofabuse prior to prescribing, and monitor for signs of abuse and dependence while ontherapy [see Drug Abuse and Dependence (9.2, 9.3)].
5.2 Serious Cardiovascular ReactionsSudden death, stroke, and myocardial infarction have been reported in adults with CNSstimulant treatment at recommended doses. Sudden death has been reported inpediatric patients with structural cardiac abnormalities and other serious heart problemstaking CNS stimulants at recommended doses for ADHD. Avoid use in patients withknown structural cardiac abnormalities, cardiomyopathy, serious heart arrhythmia,coronary artery disease, and other serious heart problems. Further evaluate patientswho develop exertional chest pain, unexplained syncope, or arrhythmias duringVYVANSE treatment.
5.3 Blood Pressure and Heart Rate IncreasesCNS stimulants cause an increase in blood pressure (mean increase about 2 to 4 mm

Hg) and heart rate (mean increase about 3 to 6 bpm). Monitor all patients for potentialtachycardia and hypertension.
5.4 Psychiatric Adverse ReactionsExacerbation of Pre-existing PsychosisCNS stimulants may exacerbate symptoms of behavior disturbance and thoughtdisorder in patients with a pre-existing psychotic disorder.Induction of a Manic Episode in Patients with Bipolar DisorderCNS stimulants may induce a mixed/manic episode in patients with bipolar disorder. Priorto initiating treatment, screen patients for risk factors for developing a manic episode(e.g., comorbid or history of depressive symptoms or a family history of suicide, bipolardisorder, and depression).New Psychotic or Manic SymptomsCNS stimulants, at recommended doses, may cause psychotic or manic symptoms(e.g., hallucinations, delusional thinking, or mania) in patients without a prior history ofpsychotic illness or mania. If such symptoms occur, consider discontinuing VYVANSE. Ina pooled analysis of multiple short-term, placebo-controlled studies of CNS stimulants,psychotic or manic symptoms occurred in 0.1% of CNS stimulant-treated patientscompared to 0% in placebo-treated patients.
5.5 Suppression of GrowthCNS stimulants have been associated with weight loss and slowing of growth rate inpediatric patients. Closely monitor growth (weight and height) in pediatric patientstreated with CNS stimulants, including VYVANSE. In a 4-week, placebo-controlled trial ofVYVANSE in pediatric patients ages 6 to 12 years old with ADHD, there was a dose-related decrease in weight in the VYVANSE groups compared to weight gain in theplacebo group. Additionally, in studies of another stimulant, there was slowing of theincrease in height [see Adverse Reactions (6.1)].Patients who are not growing or gaining height or weight as expected may need to havetheir treatment interrupted. VYVANSE is not approved for use in pediatric patients below6 years of age [see Use in Specific Populations (8.4)].
5.6 Peripheral Vasculopathy, including Raynaud's PhenomenonStimulants, including VYVANSE, are associated with peripheral vasculopathy, includingRaynaud's phenomenon. Signs and symptoms are usually intermittent and mild;however, very rare sequelae include digital ulceration and/or soft tissue breakdown.Effects of peripheral vasculopathy, including Raynaud's phenomenon, were observed inpost-marketing reports at different times and at therapeutic doses in all age groupsthroughout the course of treatment. Signs and symptoms generally improve afterreduction in dose or discontinuation of drug. Careful observation for digital changes isnecessary during treatment with stimulants. Further clinical evaluation (e.g.,rheumatology referral) may be appropriate for certain patients.
5.7 Serotonin SyndromeSerotonin syndrome, a potentially life-threatening reaction, may occur when

amphetamines are used in combination with other drugs that affect the serotonergicneurotransmitter systems such as monoamine oxidase inhibitors (MAOIs), selectiveserotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors(SNRIs), triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan,buspirone, and St. John's Wort [see Drug Interactions (7.1)]. The co-administration withcytochrome P450 2D6 (CYP2D6) inhibitors may also increase the risk with increasedexposure to the active metabolite of VYVANSE (dextroamphetamine). In thesesituations, consider an alternative non-serotonergic drug or an alternative drug thatdoes not inhibit CYP2D6 [see Drug Interactions (7.1)].Serotonin syndrome symptoms may include mental status changes (e.g., agitation,hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile bloodpressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms(e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/orgastrointestinal symptoms (e.g., nausea, vomiting, diarrhea).Concomitant use of VYVANSE with MAOI drugs is contraindicated [see Contraindications(4)].Discontinue treatment with VYVANSE and any concomitant serotonergic agentsimmediately if symptoms of serotonin syndrome occur, and initiate supportivesymptomatic treatment. If concomitant use of VYVANSE with other serotonergic drugsor CYP2D6 inhibitors is clinically warranted, initiate VYVANSE with lower doses, monitorpatients for the emergence of serotonin syndrome during drug initiation or titration, andinform patients of the increased risk for serotonin syndrome.
6 ADVERSE REACTIONSThe following adverse reactions are discussed in greater detail in other sections of thelabeling:
Known hypersensitivity to amphetamine products or other ingredients of VYVANSE[see Contraindications (4)]Hypertensive Crisis When Used Concomitantly with Monoamine Oxidase Inhibitors[see Contraindications (4) and Drug Interactions (7.1)]Drug Dependence [see Boxed Warning, Warnings and Precautions (5.1), and DrugAbuse and Dependence (9.2, 9.3)]Serious Cardiovascular Reactions [see Warnings and Precautions (5.2)]Blood Pressure and Heart Rate Increases [see Warnings and Precautions (5.3)]Psychiatric Adverse Reactions [see Warnings and Precautions (5.4)]Suppression of Growth [see Warnings and Precautions (5.5)]Peripheral Vasculopathy, including Raynaud's phenomenon [see Warnings andPrecautions (5.6)]Serotonin Syndrome [see Warnings and Precautions (5.7)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reactionrates observed in the clinical trials of a drug cannot be directly compared to rates in theclinical trials of another drug and may not reflect the rates observed in practice.Attention Deficit Hyperactivity Disorder

The safety data in this section is based on data from the 4-week controlled parallel-group clinical studies of VYVANSE in pediatric and adult patients with ADHD [see ClinicalStudies (14.1)].Adverse Reactions Associated with Discontinuation of Treatment in ADHD Clinical Trials
In the controlled trial in pediatric patients ages 6 to 12 years (Study 1), 8% (18/218) ofVYVANSE-treated patients discontinued due to adverse reactions compared to 0%(0/72) of placebo-treated patients. The most frequently reported adverse reactions (1%or more and twice rate of placebo) were ECG voltage criteria for ventricularhypertrophy, tic, vomiting, psychomotor hyperactivity, insomnia, decreased appetite andrash [2 instances for each adverse reaction, i.e., 2/218 (1%)]. Less frequently reportedadverse reactions (less than 1% or less than twice rate of placebo) included abdominalpain upper, dry mouth, weight decreased, dizziness, somnolence, logorrhea, chest pain,anger and hypertension.In the controlled trial in pediatric patients ages 13 to 17 years (Study 4), 3% (7/233) ofVYVANSE-treated patients discontinued due to adverse reactions compared to 1%(1/77) of placebo-treated patients. The most frequently reported adverse reactions (1%or more and twice rate of placebo) were decreased appetite (2/233; 1%) and insomnia(2/233; 1%). Less frequently reported adverse reactions (less than 1% or less thantwice rate of placebo) included irritability, dermatillomania, mood swings, and dyspnea.In the controlled adult trial (Study 7), 6% (21/358) of VYVANSE-treated patientsdiscontinued due to adverse reactions compared to 2% (1/62) of placebo-treatedpatients. The most frequently reported adverse reactions (1% or more and twice rate ofplacebo) were insomnia (8/358; 2%), tachycardia (3/358; 1%), irritability (2/358; 1%),hypertension (4/358; 1%), headache (2/358; 1%), anxiety (2/358; 1%), and dyspnea(3/358; 1%). Less frequently reported adverse reactions (less than 1% or less thantwice rate of placebo) included palpitations, diarrhea, nausea, decreased appetite,dizziness, agitation, depression, paranoia and restlessness.Adverse Reactions Occurring at an Incidence of ≥5% or More Among VYVANSE TreatedPatients with ADHD in Clinical Trials
The most common adverse reactions (incidence ≥5% and at a rate at least twiceplacebo) reported in pediatric patients ages 6 to 17 years, and/or adults were anorexia,anxiety, decreased appetite, decreased weight, diarrhea, dizziness, dry mouth,irritability, insomnia, nausea, upper abdominal pain, and vomiting.Adverse Reactions Occurring at an Incidence of 2% or More Among VYVANSE TreatedPatients with ADHD in Clinical Trials
Adverse reactions reported in the controlled trials in pediatric patients ages, 6 to 12years (Study 1), pediatric patients ages 13 to 17 years (Study 4), and adult patients(Study 7) treated with VYVANSE or placebo are presented in Tables 1, 2 and 3 below.
Table 1 Adverse Reactions Reportedby 2% or More of Pediatric Patients
Ages 6 to 12 Years with ADHD TakingVYVANSE and Greater than or Equal toTwice the Incidence in Patients Taking
Placebo in a 4-Week Clinical Trial
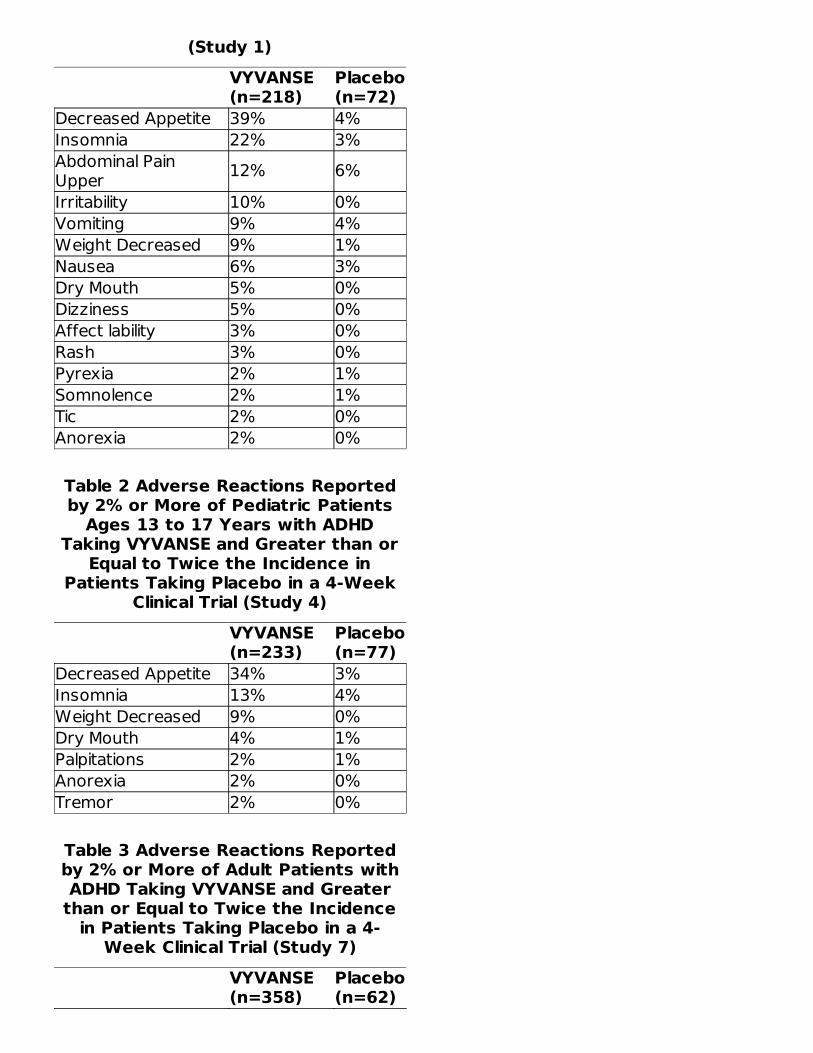
(Study 1)VYVANSE(n=218)
Placebo(n=72)
Decreased Appetite 39% 4%Insomnia 22% 3%Abdominal PainUpper 12% 6%Irritability 10% 0%Vomiting 9% 4%Weight Decreased 9% 1%Nausea 6% 3%Dry Mouth 5% 0%Dizziness 5% 0%Affect lability 3% 0%Rash 3% 0%Pyrexia 2% 1%Somnolence 2% 1%Tic 2% 0%Anorexia 2% 0%
Table 2 Adverse Reactions Reportedby 2% or More of Pediatric Patients
Ages 13 to 17 Years with ADHDTaking VYVANSE and Greater than or
Equal to Twice the Incidence inPatients Taking Placebo in a 4-Week
Clinical Trial (Study 4)VYVANSE(n=233)
Placebo(n=77)
Decreased Appetite 34% 3%Insomnia 13% 4%Weight Decreased 9% 0%Dry Mouth 4% 1%Palpitations 2% 1%Anorexia 2% 0%Tremor 2% 0%
Table 3 Adverse Reactions Reportedby 2% or More of Adult Patients withADHD Taking VYVANSE and Greater
than or Equal to Twice the Incidencein Patients Taking Placebo in a 4-
Week Clinical Trial (Study 7)VYVANSE(n=358)
Placebo(n=62)

Decreased Appetite 27% 2%Insomnia 27% 8%Dry Mouth 26% 3%Diarrhea 7% 0%Nausea 7% 0%Anxiety 6% 0%Anorexia 5% 0%Feeling Jittery 4% 0%Agitation 3% 0%Increased BloodPressure 3% 0%Hyperhidrosis 3% 0%Restlessness 3% 0%Decreased Weight 3% 0%Dyspnea 2% 0%Increased Heart Rate 2% 0%Tremor 2% 0%Palpitations 2% 0%
In addition, in the adult population erectile dysfunction was observed in 2.6% of maleson VYVANSE and 0% on placebo; decreased libido was observed in 1.4% of subjects onVYVANSE and 0% on placebo.Weight Loss and Slowing Growth Rate in Pediatric Patients with ADHD
In a controlled trial of VYVANSE in pediatric patients ages 6 to 12 years (Study 1), meanweight loss from baseline after 4 weeks of therapy was -0.9, -1.9, and -2.5 pounds,respectively, for patients receiving 30 mg, 50 mg, and 70 mg of VYVANSE, compared toa 1 pound weight gain for patients receiving placebo. Higher doses were associated withgreater weight loss with 4 weeks of treatment. Careful follow-up for weight in pediatricpatients ages 6 to 12 years who received VYVANSE over 12 months suggests thatconsistently medicated pediatric patients (i.e., treatment for 7 days per week throughoutthe year) have a slowing in growth rate, measured by body weight as demonstrated byan age- and sex-normalized mean change from baseline in percentile, of -13.4 over 1year (average percentiles at baseline and 12 months were 60.9 and 47.2, respectively).In a 4-week controlled trial of VYVANSE in pediatric patients ages 13 to 17 years, meanweight loss from baseline to endpoint was -2.7, -4.3, and -4.8 lbs., respectively, forpatients receiving 30 mg, 50 mg, and 70 mg of VYVANSE, compared to a 2.0 poundweight gain for patients receiving placebo.Careful follow-up of weight and height in pediatric patients ages 7 to 10 years who wererandomized to either methylphenidate or non-medication treatment groups over 14months, as well as in naturalistic subgroups of newly methylphenidate-treated and non-medication treated pediatric patients over 36 months (to the ages of 10 to 13 years),suggests that consistently medicated pediatric patients ages 7 to 13 years (i.e.,treatment for 7 days per week throughout the year) have a temporary slowing ingrowth rate (on average, a total of about 2 cm less growth in height and 2.7 kg lessgrowth in weight over 3 years), without evidence of growth rebound during this periodof development. In a controlled trial of amphetamine (d- to l-enantiomer ratio of 3:1) in

pediatric patients ages 13 to 17 years, mean weight change from baseline within theinitial 4 weeks of therapy was -1.1 pounds and -2.8 pounds, respectively, for patientsreceiving 10 mg and 20 mg of amphetamine. Higher doses were associated with greaterweight loss within the initial 4 weeks of treatment [see Warnings and Precautions (5.5)].Weight Loss in Adults with ADHD
In the controlled adult trial (Study 7), mean weight loss after 4 weeks of therapy was 2.8pounds, 3.1 pounds, and 4.3 pounds, for patients receiving final doses of 30 mg, 50mg, and 70 mg of VYVANSE, respectively, compared to a mean weight gain of 0.5pounds for patients receiving placebo.Binge Eating DisorderThe safety data in this section is based on data from two 12-week parallel group,flexible-dose, placebo-controlled studies in adults with BED [see Clinical Studies 14.2].Patients with cardiovascular risk factors other than obesity and smoking were excluded.Adverse Reactions Associated with Discontinuation of Treatment in BED Clinical Trials
In controlled trials of patients ages 18 to 55 years, 5.1% (19/373) of VYVANSE-treatedpatients discontinued due to adverse reactions compared to 2.4% (9/372) of placebo-treated patients. No single adverse reaction led to discontinuation in 1% or more ofVYVANSE-treated patients. Less commonly reported adverse reactions (less than 1% orless than twice rate of placebo) included increased heart rate, headache, abdominal painupper, dyspnea, rash, insomnia, irritability, feeling jittery and anxiety.Adverse Reactions Occurring at an Incidence of 5% or More and At Least Twice PlaceboAmong VYVANSE Treated Patients with BED in Clinical Trials
The most common adverse reactions (incidence ≥5% and at a rate at least twiceplacebo) reported in adults were dry mouth, insomnia, decreased appetite, increasedheart rate, constipation, feeling jittery, and anxiety.Adverse Reactions Occurring at an Incidence of 2% or More and At Least Twice PlaceboAmong VYVANSE Treated Patients with BED in Clinical Trials
Adverse reactions reported in the pooled controlled trials in adult patients (Study 11 and12) treated with VYVANSE or placebo are presented in Table 4 below.
Table 4 Adverse Reactions Reported by2% or More of Adult Patients with BEDTaking VYVANSE and Greater than or
Equal to Twice the Incidence in PatientsTaking Placebo in 12-Week Clinical Trials
(Study 11 and 12)VYVANSE(N=373)
Placebo(N=372)
Dry Mouth 36% 7%Insomnia 20% 8%Decreased Appetite 8% 2%Increased Heart Rate 7% 1%Feeling Jittery 6% 1%
*
†

*
†
Constipation 6% 1%Anxiety 5% 1%Diarrhea 4% 2%Decreased Weight 4% 0%Hyperhidrosis 4% 0%Vomiting 2% 1%Gastroenteritis 2% 1%Paresthesia 2% 1%Pruritus 2% 1%Upper Abdominal Pain 2% 0%Energy Increased 2% 0%Urinary Tract Infection 2% 0%Nightmare 2% 0%Restlessness 2% 0%Oropharyngeal Pain 2% 0%
6.2 Postmarketing ExperienceThe following adverse reactions have been identified during postapproval use ofVYVANSE. Because these reactions are reported voluntarily from a population ofuncertain size, it is not always possible to reliably estimate their frequency or establish acausal relationship to drug exposure. These events are as follows: cardiomyopathy,mydriasis, diplopia, difficulties with visual accommodation, blurred vision, eosinophilichepatitis, anaphylactic reaction, hypersensitivity, dyskinesia, dysgeusia, tics, bruxism,depression, dermatillomania, alopecia, aggression, Stevens-Johnson Syndrome, chestpain, angioedema, urticaria, seizures, libido changes, frequent or prolonged erections,constipation, and rhabdomyolysis.
7 DRUG INTERACTIONS
7.1 Drugs Having Clinically Important Interactions with Amphetamines
Table 5 Drugs having clinically important interactions with amphetamines.MAO Inhibitors (MAOI)
Clinical Impact
MAOI antidepressants slow amphetamine metabolism,increasing amphetamines effect on the release ofnorepinephrine and other monoamines from adrenergicnerve endings causing headaches and other signs ofhypertensive crisis. Toxic neurological effects and malignanthyperpyrexia can occur, sometimes with fatal results.
InterventionDo not administer VYVANSE during or within 14 daysfollowing the administration of MAOI [see Contraindications(4)].
Includes all preferred terms containing the word"insomnia."Includes the preferred terms "heart rate increased"and "tachycardia."
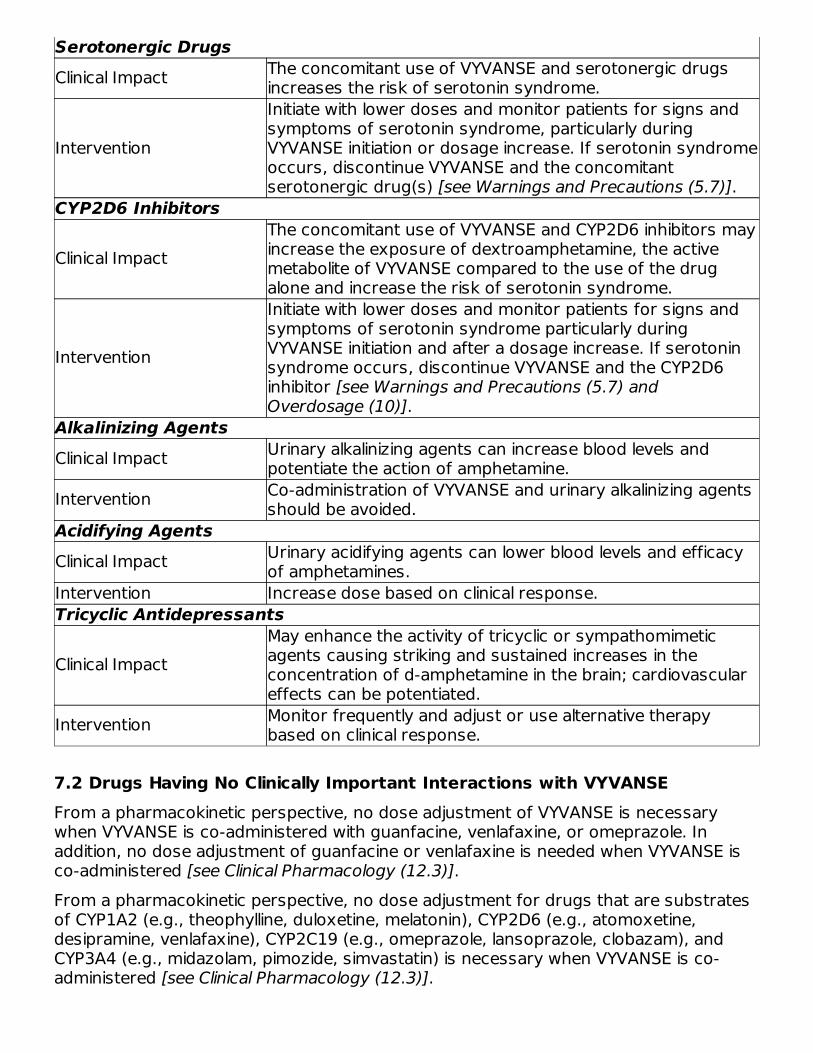
Serotonergic DrugsClinical Impact The concomitant use of VYVANSE and serotonergic drugs
increases the risk of serotonin syndrome.
Intervention
Initiate with lower doses and monitor patients for signs andsymptoms of serotonin syndrome, particularly duringVYVANSE initiation or dosage increase. If serotonin syndromeoccurs, discontinue VYVANSE and the concomitantserotonergic drug(s) [see Warnings and Precautions (5.7)].
CYP2D6 Inhibitors
Clinical ImpactThe concomitant use of VYVANSE and CYP2D6 inhibitors mayincrease the exposure of dextroamphetamine, the activemetabolite of VYVANSE compared to the use of the drugalone and increase the risk of serotonin syndrome.
Intervention
Initiate with lower doses and monitor patients for signs andsymptoms of serotonin syndrome particularly duringVYVANSE initiation and after a dosage increase. If serotoninsyndrome occurs, discontinue VYVANSE and the CYP2D6inhibitor [see Warnings and Precautions (5.7) andOverdosage (10)].
Alkalinizing AgentsClinical Impact Urinary alkalinizing agents can increase blood levels and
potentiate the action of amphetamine.Intervention Co-administration of VYVANSE and urinary alkalinizing agents
should be avoided.Acidifying AgentsClinical Impact Urinary acidifying agents can lower blood levels and efficacy
of amphetamines.Intervention Increase dose based on clinical response.Tricyclic Antidepressants
Clinical ImpactMay enhance the activity of tricyclic or sympathomimeticagents causing striking and sustained increases in theconcentration of d-amphetamine in the brain; cardiovasculareffects can be potentiated.
Intervention Monitor frequently and adjust or use alternative therapybased on clinical response.
7.2 Drugs Having No Clinically Important Interactions with VYVANSEFrom a pharmacokinetic perspective, no dose adjustment of VYVANSE is necessarywhen VYVANSE is co-administered with guanfacine, venlafaxine, or omeprazole. Inaddition, no dose adjustment of guanfacine or venlafaxine is needed when VYVANSE isco-administered [see Clinical Pharmacology (12.3)].From a pharmacokinetic perspective, no dose adjustment for drugs that are substratesof CYP1A2 (e.g., theophylline, duloxetine, melatonin), CYP2D6 (e.g., atomoxetine,desipramine, venlafaxine), CYP2C19 (e.g., omeprazole, lansoprazole, clobazam), andCYP3A4 (e.g., midazolam, pimozide, simvastatin) is necessary when VYVANSE is co-administered [see Clinical Pharmacology (12.3)].

8 USE IN SPECIFIC POPULATIONS
8.1 PregnancyPregnancy Exposure RegistryThere is a pregnancy exposure registry that monitors pregnancy outcomes in womenexposed to ADHD medications during pregnancy. Healthcare providers are encouragedto register patients by calling the National Pregnancy Registry for Psychostimulants at 1-866-961-2388 or visiting online at https://womensmentalhealth.org/clinical-andresearchprograms/pregnancyregistry/adhd-medications/.Risk SummaryThe limited available data from published literature and postmarketing reports on use ofVYVANSE in pregnant women are not sufficient to inform a drug-associated risk formajor birth defects and miscarriage. Adverse pregnancy outcomes, including prematuredelivery and low birth weight, have been seen in infants born to mothers dependent onamphetamines [see Clinical Considerations]. In animal reproduction studies,lisdexamfetamine dimesylate (a prodrug of d-amphetamine) had no effects on embryo-fetal morphological development or survival when administered orally to pregnant ratsand rabbits throughout the period of organogenesis. Pre- and postnatal studies werenot conducted with lisdexamfetamine dimesylate. However, amphetamine (d- to l- ratioof 3:1) administration to pregnant rats during gestation and lactation caused a decreasein pup survival and a decrease in pup body weight that correlated with a delay indevelopmental landmarks at clinically relevant doses of amphetamine. In addition,adverse effects on reproductive performance were observed in pups whose motherswere treated with amphetamine. Long-term neurochemical and behavioral effects havealso been reported in animal developmental studies using clinically relevant doses ofamphetamine [see Data].The estimated background risk of major birth defects and miscarriage for the indicatedpopulation is unknown. All pregnancies have a background risk of birth defect, loss orother adverse outcomes. In the U.S. general population, the estimated background riskof major birth defects and miscarriage in clinically recognized pregnancies is 2-4% and15-20%, respectively.Clinical ConsiderationsFetal/Neonatal Adverse Reactions
Amphetamines, such as VYVANSE, cause vasoconstriction and thereby may decreaseplacental perfusion. In addition, amphetamines can stimulate uterine contractionsincreasing the risk of premature delivery. Infants born to amphetamine-dependentmothers have an increased risk of premature delivery and low birth weight.Monitor infants born to mothers taking amphetamines for symptoms of withdrawal suchas feeding difficulties, irritability, agitation, and excessive drowsiness.DataAnimal Data
Lisdexamfetamine dimesylate had no apparent effects on embryo-fetal morphologicaldevelopment or survival when administered orally to pregnant rats and rabbits

throughout the period of organogenesis at doses of up to 40 and 120 mg/kg/day,respectively. These doses are approximately 5.5 and 33 times, respectively, themaximum recommended human dose (MRHD) of 70 mg/day given to adults, on amg/m body surface area basis.A study was conducted with amphetamine (d- to l- enantiomer ratio of 3:1) in whichpregnant rats received daily oral doses of 2, 6, and 10 mg/kg from gestation day 6 tolactation day 20. All doses caused hyperactivity and decreased weight gain in the dams.A decrease in pup survival was seen at all doses. A decrease in pup body weight wasseen at 6 and 10 mg/kg which correlated with delays in developmental landmarks, suchas preputial separation and vaginal opening. Increased pup locomotor activity was seenat 10 mg/kg on day 22 postpartum but not at 5 weeks postweaning. When pups weretested for reproductive performance at maturation, gestational weight gain, number ofimplantations, and number of delivered pups were decreased in the group whosemothers had been given 10 mg/kg.A number of studies from the literature in rodents indicate that prenatal or earlypostnatal exposure to amphetamine (d- or d, l-) at doses similar to those used clinicallycan result in long-term neurochemical and behavioral alterations. Reported behavioraleffects include learning and memory deficits, altered locomotor activity, and changes insexual function.
8.2 LactationRisk SummaryLisdexamfetamine is a pro-drug of dextroamphetamine. Based on limited case reports inpublished literature, amphetamine (d-or d, l-) is present in human milk, at relative infantdoses of 2% to 13.8% of the maternal weight-adjusted dosage and a milk/plasma ratioranging between 1.9 and 7.5. There are no reports of adverse effects on the breastfedinfant. Long-term neurodevelopmental effects on infants from amphetamine exposureare unknown. It is possible that large dosages of dextroamphetamine might interferewith milk production, especially in women whose lactation is not well established.Because of the potential for serious adverse reactions in nursing infants, includingserious cardiovascular reactions, blood pressure and heart rate increase, suppressionof growth, and peripheral vasculopathy, advise patients that breastfeeding is notrecommended during treatment with VYVANSE.
8.4 Pediatric UseADHDSafety and effectiveness of VYVANSE have been established in pediatric patients withADHD ages 6 to 17 years [see Dosage and Administration (2.3), Adverse Reactions (6.1),Clinical Pharmacology (12.3), and Clinical Studies (14.1)].Safety and effectiveness of VYVANSE have not been established in pediatric patientsbelow the age of 6 years.Safety and efficacy of VYVANSE were evaluated in a double-blind, randomized, parallel-group, placebo-controlled, fixed-dose study in pediatric patients ages 4 to 5 years withADHD, followed by a 1-year open-label extension study. In these studies, patientsexperienced elevated rates of adverse reactions, including weight loss, decreased BMI,decreased appetite, insomnia, infections (upper respiratory and nasopharyngitis),
2

irritability, and affect lability.With the same VYVANSE dose, mean steady state exposure of dextroamphetamine wasapproximately 44% higher in pediatric patients ages 4 to 5 years compared to thepediatric patients ages 6 to 11 years.BEDSafety and effectiveness of VYVANSE have not been established in patients less than 18years of age.Growth SuppressionGrowth should be monitored during treatment with stimulants, including VYVANSE, andpediatric patients who are not growing or gaining weight as expected may need to havetheir treatment interrupted [see Warnings and Precautions (5.5) and Adverse Reactions(6.1)].Juvenile Animal DataStudies conducted in juvenile rats and dogs at clinically relevant doses showed growthsuppression that partially or fully reversed in dogs and female rats but not in male ratsafter a four-week drug-free recovery period.A study was conducted in which juvenile rats received oral doses of 4, 10, or 40mg/kg/day of lisdexamfetamine dimesylate from day 7 to day 63 of age. These dosesare approximately 0.3, 0.7, and 3 times the maximum recommended human daily doseof 70 mg on a mg/m basis for a child. Dose-related decreases in food consumption,bodyweight gain, and crown-rump length were seen; after a four-week drug-freerecovery period, bodyweights and crown-rump lengths had significantly recovered infemales but were still substantially reduced in males. Time to vaginal opening wasdelayed in females at the highest dose, but there were no drug effects on fertility whenthe animals were mated beginning on day 85 of age.In a study in which juvenile dogs received lisdexamfetamine dimesylate for 6 monthsbeginning at 10 weeks of age, decreased bodyweight gain was seen at all doses tested(2, 5, and 12 mg/kg/day, which are approximately 0.5, 1, and 3 times the maximumrecommended human daily dose on a mg/m basis for a child). This effect partially orfully reversed during a four-week drug-free recovery period.
8.5 Geriatric UseClinical studies of VYVANSE did not include sufficient numbers of subjects aged 65 andover to determine whether they respond differently from younger subjects. Otherreported clinical experience and pharmacokinetic data [see Clinical Pharmacology (12.3)]have not identified differences in responses between the elderly and younger patients. Ingeneral, dose selection for an elderly patient should start at the low end of the dosingrange, reflecting the greater frequency of decreased hepatic, renal, or cardiac function,and of concomitant disease or other drug therapy.
8.6 Renal ImpairmentDue to reduced clearance in patients with severe renal impairment (GFR 15 to < 30mL/min/1.73 m ), the maximum dose should not exceed 50 mg/day. The maximumrecommended dose in ESRD (GFR < 15 mL/min/1.73 m ) patients is 30 mg/day [see
2
2
22

Clinical Pharmacology (12.3)].Lisdexamfetamine and d-amphetamine are not dialyzable.
9 DRUG ABUSE AND DEPENDENCE
9.1 Controlled SubstanceVYVANSE contains lisdexamfetamine, a prodrug of amphetamine, a Schedule IIcontrolled substance.
9.2 AbuseCNS stimulants, including VYVANSE, other amphetamine-containing products, andmethylphenidate have a high potential for abuse. Abuse is the intentional non-therapeutic use of a drug, even once, to achieve a desired psychological or physiologicaleffect. Abuse is characterized by impaired control over drug use, compulsive use,continued use despite harm, and craving. Drug addiction is a cluster of behavioral,cognitive, and physiological phenomena that may include a strong desire to take thedrug, difficulties in controlling drug use (e.g., continuing drug use despite harmfulconsequences, giving higher priority to drug use than other activities and obligations),and possible tolerance or physical dependence. Both abuse and misuse may lead toaddiction, and some individuals may develop addiction even when taking VYVANSE asprescribed.Signs and symptoms of amphetamine abuse may include increased heart rate,respiratory rate, blood pressure, and/or sweating, dilated pupils, hyperactivity,restlessness, insomnia, decreased appetite, loss of coordination, tremors, flushed skin,vomiting, and/or abdominal pain. Anxiety, psychosis, hostility, aggression, suicidal orhomicidal ideation have also been seen. Abusers of CNS stimulants may chew, snort,inject, or use other unapproved routes of administration which can result in overdoseand death [see Overdosage (10)].To reduce the abuse of CNS stimulants, including VYVANSE, assess the risk of abuseprior to prescribing. After prescribing, keep careful prescription records, educatepatients and their families about abuse and on proper storage and disposal of CNSstimulants. Monitor for signs of abuse while on therapy, and re-evaluate the need forVYVANSE use.Studies of VYVANSE in Drug AbusersA randomized, double-blind, placebo-control, cross-over, abuse liability study in 38patients with a history of drug abuse was conducted with single-doses of 50, 100, or150 mg of VYVANSE, 40 mg of immediate-release d-amphetamine sulphate (a controlledII substance), and 200 mg of diethylpropion hydrochloride (a controlled IV substance).VYVANSE 100 mg produced significantly less "Drug Liking Effects" as measured by theDrug Rating Questionnaire-Subject score, compared to d-amphetamine 40 mg; and 150mg of VYVANSE demonstrated similar "Drug-Liking Effects" compared to 40 mg of d-amphetamine and 200 mg of diethylpropion.Intravenous administration of 50 mg lisdexamfetamine dimesylate to individuals with ahistory of drug abuse produced positive subjective responses on scales measuring"Drug Liking", "Euphoria", "Amphetamine Effects", and "Benzedrine Effects" that were

greater than placebo but less than those produced by an equivalent dose (20 mg) ofintravenous d-amphetamine.
9.3 DependencePhysical DependenceVYVANSE may produce physical dependence from continued therapy. Physicaldependence is a state of adaptation manifested by a withdrawal syndrome produced byabrupt cessation, rapid dose reduction, or administration of an antagonist. Withdrawalsymptoms after abrupt cessation following prolonged high-dosage administration ofCNS stimulants include extreme fatigue and depression.ToleranceVYVANSE may produce tolerance from continued therapy. Tolerance is a state ofadaptation in which exposure to a specific dose of a drug results in a reduction of thedrug's desired and/or undesired effects over time.
10 OVERDOSAGEConsult with a Certified Poison Control Center (1-800-222-1222) for up-to-date guidanceand advice for treatment of overdosage. Individual patient response to amphetaminesvaries widely. Toxic symptoms may occur idiosyncratically at low doses.Manifestations of amphetamine overdose include restlessness, tremor, hyperreflexia,rapid respiration, confusion, assaultiveness, hallucinations, panic states, hyperpyrexiaand rhabdomyolysis. Fatigue and depression usually follow the central nervous systemstimulation. Serotonin syndrome has been reported with amphetamine use, includingVYVANSE. Cardiovascular effects include arrhythmias, hypertension or hypotension andcirculatory collapse. Gastrointestinal symptoms include nausea, vomiting, diarrhea andabdominal cramps. Fatal poisoning is usually preceded by convulsions and coma.Lisdexamfetamine and d-amphetamine are not dialyzable.
11 DESCRIPTIONVYVANSE (lisdexamfetamine dimesylate), a CNS stimulant, is for once-a-day oraladministration. The chemical designation for lisdexamfetamine dimesylate is (2S)-2,6-diamino-N-[(1S)-1-methyl-2-phenylethyl] hexanamide dimethanesulfonate. The molecularformula is C H N O∙(CH O S) , which corresponds to a molecular weight of 455.60.The chemical structure is:
Lisdexamfetamine dimesylate is a white to off-white powder that is soluble in water (792mg/mL).
15 25 3 4 3 2

Information for VYVANSE capsules:
VYVANSE capsules contain 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg, and 70 mg oflisdexamfetamine dimesylate (equivalent to 5.8 mg, 11.6 mg, 17.3 mg, 23.1 mg, 28.9mg, 34.7 mg, and 40.5 mg of lisdexamfetamine).Inactive ingredients: microcrystalline cellulose, croscarmellose sodium, and magnesiumstearate. The capsule shells contain gelatin, titanium dioxide, and one or more of thefollowing: FD&C Red #3, FD&C Yellow #6, FD&C Blue #1, Black Iron Oxide, and YellowIron Oxide.Information for VYVANSE chewable tablets:
VYVANSE chewable tablets contain 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, and 60 mg oflisdexamfetamine dimesylate (equivalent to 5.8 mg, 11.6 mg, 17.3 mg, 23.1 mg, 28.9mg, and 34.7 mg of lisdexamfetamine).Inactive ingredients: colloidal silicon dioxide, croscarmellose sodium, guar gum,magnesium stearate, mannitol, microcrystalline cellulose, sucralose, artificial strawberryflavor.
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of ActionLisdexamfetamine is a prodrug of dextroamphetamine. Amphetamines are non-catecholamine sympathomimetic amines with CNS stimulant activity. The exact mode oftherapeutic action in ADHD and BED is not known.
12.2 PharmacodynamicsAmphetamines block the reuptake of norepinephrine and dopamine into the presynapticneuron and increase the release of these monoamines into the extraneuronal space. Theparent drug, lisdexamfetamine, does not bind to the sites responsible for the reuptakeof norepinephrine and dopamine in vitro.
12.3 PharmacokineticsPharmacokinetic studies after oral administration of lisdexamfetamine dimesylate havebeen conducted in healthy adult (capsule and chewable tablet formulations) and pediatric(6 to 12 years) patients with ADHD (capsule formulation). After single doseadministration of lisdexamfetamine dimesylate, pharmacokinetics of dextroamphetaminewas found to be linear between 30 mg and 70 mg in a pediatric study (6 to 12 years),and between 50 mg and 250 mg in an adult study. Dextroamphetamine pharmacokineticparameters following administration of lisdexamfetamine dimesylate in adults exhibitedlow inter-subject (<25%) and intra-subject (<8%) variability. There is no accumulation oflisdexamfetamine and dextroamphetamine at steady state in healthy adults.AbsorptionCapsule formulation
Following single-dose oral administration of VYVANSE capsule (30 mg, 50 mg, or 70 mg)in patients ages 6 to 12 years with ADHD under fasted conditions, T ofmax

lisdexamfetamine and dextroamphetamine was reached at approximately 1 hour and 3.5hours post dose, respectively. Weight/Dose normalized AUC and C values were thesame in pediatric patients ages 6 to 12 years as the adults following single doses of 30mg to 70 mg VYVANSE capsule.Effect of food on capsule formulation
Neither food (a high fat meal or yogurt) nor orange juice affects the observed AUC andC of dextroamphetamine in healthy adults after single-dose oral administration of 70mg of VYVANSE capsules. Food prolongs T by approximately 1 hour (from 3.8 hoursat fasted state to 4.7 hours after a high fat meal or to 4.2 hours with yogurt). After an8-hour fast, the AUC for dextroamphetamine following oral administration oflisdexamfetamine dimesylate in solution and as intact capsules were equivalent.Chewable Tablet formulation
After a single dose administration of 60 mg VYVANSE chewable tablet in healthy subjectsunder fasted conditions, T of lisdexamfetamine and dextroamphetamine wasreached at approximately 1 hour and 4.4 hours post dose, respectively. Compared to60 mg VYVANSE capsule, exposure (C and AUC) to lisdexamfetamine was about15% lower. The exposure (C and AUC ) of dextroamphetamine is similar betweenVYVANSE chewable tablet and VYVANSE capsule.Effect of food on tablet formulation
Administration of 60 mg VYVANSE chewable tablet with food (a high-fat meal) decreasesthe exposure (C and AUC ) of dextroamphetamine by about 5% to 7%, andprolongs mean T by approximately 1 hour (from 3.9 hours at fasted state to 4.9hours).EliminationPlasma concentrations of unconverted lisdexamfetamine are low and transient, generallybecoming non-quantifiable by 8 hours after administration. The plasma elimination half-life of lisdexamfetamine typically averaged less than one hour in volunteers ages 6 yearsand older The plasma elimination half-life of dextroamphetamine was approximately 8.6to 9.5 hours in pediatric patients 6 to 12 years and 10 to 11.3 hours in healthy adults.Metabolism
Lisdexamfetamine is converted to dextroamphetamine and l-lysine primarily in blood dueto the hydrolytic activity of red blood cells after oral administration of lisdexamfetaminedimesylate. In vitro data demonstrated that red blood cells have a high capacity formetabolism of lisdexamfetamine; substantial hydrolysis occurred even at low hematocritlevels (33% of normal). Lisdexamfetamine is not metabolized by cytochrome P450enzymes.Excretion
Following oral administration of a 70 mg dose of radiolabeled lisdexamfetaminedimesylate to 6 healthy subjects, approximately 96% of the oral dose radioactivity wasrecovered in the urine and only 0.3% recovered in the feces over a period of 120 hours.Of the radioactivity recovered in the urine, 42% of the dose was related toamphetamine, 25% to hippuric acid, and 2% to intact lisdexamfetamine.Specific Populations
max
max
maxmax
max
maxmax inf
max infmax
.

Exposures of dextroamphetamine in specific populations are summarized in Figure 1.
*
Figure 1: Specific Populations :
Drug Interaction Studies
Effects of other drugs on the exposures of dextroamphetamine are summarized inFigure 2.
Figure 2: Effect of Other Drugs on VYVANSE:
Figure 1 shows the geometric mean ratios and the 90% confidence limits for C and AUC of d-amphetamine. Comparison for gender uses males as the reference. Comparison for age uses 55-64 years as the reference.
max
*

The effects of VYVANSE on the exposures of other drugs are summarized in Figure 3.
Figure 3: Effect of VYVANSE on Other Drugs:
13 NONCLINICAL TOXICOLOGY
13.1 Carcinogenesis, Mutagenesis, and Impairment of Fertility

CarcinogenesisCarcinogenicity studies of lisdexamfetamine dimesylate have not been performed. Noevidence of carcinogenicity was found in studies in which d-, l-amphetamine (enantiomerratio of 1:1) was administered to mice and rats in the diet for 2 years at doses of up to30 mg/kg/day in male mice, 19 mg/kg/day in female mice, and 5 mg/kg/day in male andfemale rats.MutagenesisLisdexamfetamine dimesylate was not clastogenic in the mouse bone marrowmicronucleus test in vivo and was negative when tested in the E. coli and S. typhimuriumcomponents of the Ames test and in the L5178Y/TK mouse lymphoma assay in vitro.Impairment of FertilityAmphetamine (d- to l-enantiomer ratio of 3:1) did not adversely affect fertility or earlyembryonic development in the rat at doses of up to 20 mg/kg/day.
13.2 Animal Toxicology and/or PharmacologyAcute administration of high doses of amphetamine (d- or d, l-) has been shown toproduce long-lasting neurotoxic effects, including irreversible nerve fiber damage, inrodents. The significance of these findings to humans is unknown.
14 CLINICAL STUDIES
14.1 Attention Deficit Hyperactivity Disorder (ADHD)Pediatric Patients Ages 6 to 12 Years with ADHDA double-blind, randomized, placebo-controlled, parallel-group study (Study 1) wasconducted in pediatric patients ages 6 to 12 years (N=290) who met DSM-IV criteria forADHD (either the combined type or the hyperactive-impulsive type). Patients wererandomized to receive final doses of 30 mg, 50 mg, or 70 mg of VYVANSE or placeboonce daily in the morning for a total of four weeks of treatment. All patients receivingVYVANSE were initiated on 30 mg for the first week of treatment. Patients assigned tothe 50 mg and 70 mg dose groups were titrated by 20 mg per week until they achievedtheir assigned dose. The primary efficacy outcome was change in Total Score frombaseline to endpoint in investigator ratings on the ADHD Rating Scale (ADHD-RS), an 18-item questionnaire with a score range of 0-54 points that measures the core symptomsof ADHD which includes both hyperactive/impulsive and inattentive subscales. Endpointwas defined as the last post-randomization treatment week (i.e., Weeks 1 through 4) forwhich a valid score was obtained. All VYVANSE dose groups were superior to placebo inthe primary efficacy outcome. Mean effects at all doses were similar; however, thehighest dose (70 mg/day) was numerically superior to both lower doses (Study 1 inTable 6). The effects were maintained throughout the day based on parent ratings(Conners' Parent Rating Scale) in the morning (approximately 10 am), afternoon(approximately 2 pm), and early evening (approximately 6 pm).A double-blind, placebo-controlled, randomized, crossover design, analog classroomstudy (Study 2) was conducted in pediatric patients ages 6 to 12 years (N=52) who metDSM-IV criteria for ADHD (either the combined type or the hyperactive-impulsive type).
+/-
®

Following a 3-week open-label dose optimization with Adderall XR , patients wererandomly assigned to continue their optimized dose of Adderall XR (10 mg, 20 mg, or 30mg), VYVANSE (30 mg, 50 mg, or 70 mg), or placebo once daily in the morning for 1week each treatment. Efficacy assessments were conducted at 1, 2, 3, 4.5, 6, 8, 10,and 12 hours post-dose using the Swanson, Kotkin, Agler, M.Flynn, and PelhamDeportment scores (SKAMP-DS), a 4-item subscale of the SKAMP with scores rangingfrom 0 to 24 points that measures deportment problems leading to classroomdisruptions. A significant difference in patient behavior, based upon the average ofinvestigator ratings on the SKAMP-DS across the 8 assessments were observedbetween patients when they received VYVANSE compared to patients when theyreceived placebo (Study 2 in Table 6). The drug effect reached statistical significancefrom hours 2 to 12 post-dose, but was not significant at 1 hour.A second double-blind, placebo-controlled, randomized, crossover design, analogclassroom study (Study 3) was conducted in pediatric patients ages 6 to 12 years(N=129) who met DSM-IV criteria for ADHD (either the combined type or thehyperactive-impulsive type). Following a 4-week open-label dose optimization withVYVANSE (30 mg, 50 mg, 70 mg), patients were randomly assigned to continue theiroptimized dose of VYVANSE or placebo once daily in the morning for 1 week eachtreatment. A significant difference in patient behavior, based upon the average ofinvestigator ratings on the SKAMP-Deportment scores across all 7 assessmentsconducted at 1.5, 2.5, 5.0, 7.5, 10.0, 12.0, and 13.0 hours post-dose, were observedbetween patients when they received VYVANSE compared to patients when theyreceived placebo (Study 3 in Table 6, Figure 4).Pediatric Patients Ages 13 to 17 Years with ADHDA double-blind, randomized, placebo-controlled, parallel-group study (Study 4) wasconducted in pediatric patients ages 13 to 17 years (N=314) who met DSM-IV criteriafor ADHD. In this study, patients were randomized in a 1:1:1:1 ratio to a daily morningdose of VYVANSE (30 mg/day, 50 mg/day or 70 mg/day) or placebo for a total of fourweeks of treatment. All patients receiving VYVANSE were initiated on 30 mg for the firstweek of treatment. Patients assigned to the 50 mg and 70 mg dose groups weretitrated by 20 mg per week until they achieved their assigned dose. The primary efficacyoutcome was change in Total Score from baseline to endpoint in investigator ratings onthe ADHD Rating Scale (ADHD-RS). Endpoint was defined as the last post-randomizationtreatment week (i.e., Weeks 1 through 4) for which a valid score was obtained. AllVYVANSE dose groups were superior to placebo in the primary efficacy outcome (Study4 in Table 6).Pediatric Patients Ages 6 to 17 Years: Short-Term Treatment in ADHDA double-blind, randomized, placebo- and active-controlled parallel-group, dose-optimization study (Study 5) was conducted in pediatric patients ages 6 to 17 years(n=336) who met DSM-IV criteria for ADHD. In this eight-week study, patients wererandomized to a daily morning dose of VYVANSE (30, 50 or 70 mg/day), an activecontrol, or placebo (1:1:1). The study consisted of a Screening and Washout Period (upto 42 days), a 7-week Double-blind Evaluation Period (consisting of a 4-week Dose-Optimization Period followed by a 3-week Dose-Maintenance Period), and a 1-weekWashout and Follow-up Period. During the Dose Optimization Period, subjects weretitrated until an optimal dose, based on tolerability and investigator's judgment, wasreached. VYVANSE showed significantly greater efficacy than placebo. The placebo-
®
adjusted mean reduction from baseline in the ADHD-RS-IV total score was 18.6.Subjects on VYVANSE also showed greater improvement on the Clinical GlobalImpression-Improvement (CGI-I) rating scale compared to subjects on placebo (Study 5in Table 6).Pediatric Patients Ages 6 to 17 Years: Maintenance Treatment in ADHDMaintenance of Efficacy Study (Study 6) - A double-blind, placebo-controlled,randomized withdrawal study was conducted in pediatric patients ages 6 to 17 years(N=276) who met the diagnosis of ADHD (DSM-IV criteria). A total of 276 patients wereenrolled into the study, 236 patients participated in Study 5 and 40 subjects directlyenrolled. Subjects were treated with open-label VYVANSE for at least 26 weeks prior tobeing assessed for entry into the randomized withdrawal period. Eligible patients had todemonstrate treatment response as defined by CGI-S <3 and Total Score on the ADHD-RS ≤22. Patients that maintained treatment response for 2 weeks at the end of theopen label treatment period were eligible to be randomized to ongoing treatment withthe same dose of VYVANSE (N=78) or switched to placebo (N=79) during the double-blind phase. Patients were observed for relapse (treatment failure) during the 6 weekdouble blind phase. A significantly lower proportion of treatment failures occurredamong VYVANSE subjects (15.8%) compared to placebo (67.5%) at endpoint of therandomized withdrawal period. The endpoint measurement was defined as the last post-randomization treatment week at which a valid ADHD-RS Total Score and CGI-S wereobserved. Treatment failure was defined as a ≥50% increase (worsening) in the ADHD-RS Total Score and a ≥2-point increase in the CGI-S score compared to scores at entryinto the double-blind randomized withdrawal phase. Subjects who withdrew from therandomized withdrawal period and who did not provide efficacy data at their last on-treatment visit were classified as treatment failures (Study 6, Figure 5).Adults: Short-Term Treatment in ADHDA double-blind, randomized, placebo-controlled, parallel-group study (Study 7) wasconducted in adults ages 18 to 55 (N=420) who met DSM-IV criteria for ADHD. In thisstudy, patients were randomized to receive final doses of 30 mg, 50 mg, or 70 mg ofVYVANSE or placebo for a total of four weeks of treatment. All patients receivingVYVANSE were initiated on 30 mg for the first week of treatment. Patients assigned tothe 50 mg and 70 mg dose groups were titrated by 20 mg per week until they achievedtheir assigned dose. The primary efficacy outcome was change in Total Score frombaseline to endpoint in investigator ratings on the ADHD Rating Scale (ADHD-RS).Endpoint was defined as the last post-randomization treatment week (i.e., Weeks 1through 4) for which a valid score was obtained. All VYVANSE dose groups weresuperior to placebo in the primary efficacy outcome (Study 7 in Table 6).The second study was a multi-center, randomized, double-blind, placebo-controlled,cross-over, modified analog classroom study (Study 8) of VYVANSE to simulate aworkplace environment in 142 adults ages 18 to 55 who met DSM-IV-TR criteria forADHD. There was a 4-week open-label, dose optimization phase with VYVANSE (30mg/day, 50 mg/day, or 70 mg/day in the morning). Patients were then randomized toone of two treatment sequences: 1) VYVANSE (optimized dose) followed by placebo,each for one week, or 2) placebo followed by VYVANSE, each for one week. Efficacyassessments occurred at the end of each week, using the Permanent Product Measureof Performance (PERMP), a skill-adjusted math test that measures attention in ADHD.PERMP total score results from the sum of the number of math problems attempted

plus the number of math problems answered correctly. VYVANSE treatment, comparedto placebo, resulted in a statistically significant improvement in attention across all post-dose time points, as measured by average PERMP total scores over the course of oneassessment day, as well as at each time point measured. The PERMP assessments wereadministered at pre-dose (-0.5 hours) and at 2, 4, 8, 10, 12, and 14 hours post-dose(Study 8 in Table 6, Figure 6).Adults: Maintenance Treatment in ADHDA double-blind, placebo-controlled, randomized withdrawal design study (Study 9) wasconducted in adults ages 18 to 55 (N=123) who had a documented diagnosis of ADHDor met DSM-IV criteria for ADHD. At study entry, patients must have had documentationof treatment with VYVANSE for a minimum of 6 months and had to demonstratetreatment response as defined by Clinical Global Impression Severity (CGI-S) ≤3 andTotal Score on the ADHD-RS <22. ADHD-RS Total Score is a measure of core symptomsof ADHD. The CGI-S score assesses the clinician's impression of the patient's currentillness state and ranges from 1 (not at all ill) to 7 (extremely ill). Patients that maintainedtreatment response at Week 3 of the open label treatment phase (N=116) were eligibleto be randomized to ongoing treatment with the same dose of VYVANSE (N=56) orswitched to placebo (N=60) during the double-blind phase. Patients were observed forrelapse (treatment failure) during the 6-week double-blind phase. The efficacy endpointwas the proportion of patients with treatment failure during the double-blind phase.Treatment failure was defined as a ≥50% increase (worsening) in the ADHD-RS TotalScore and ≥2-point increase in the CGI-S score compared to scores at entry into thedouble-blind phase. Maintenance of efficacy for patients treated with VYVANSE wasdemonstrated by the significantly lower proportion of patients with treatment failure(9%) compared to patients receiving placebo (75%) at endpoint during the double-blindphase (Study 9, Figure 7).
Table 6: Summary of Primary Efficacy Results from Short-term Studies ofVYVANSE in Pediatric Patients (Ages 6 to 17) and Adults with ADHD
StudyNumber(Agerange)
PrimaryEndpoint
Treatment Group MeanBaseline
Score (SD)
LS MeanChange
fromBaseline
(SE)
Placebo-subtracted
Difference (95%CI)
Study 1(6 - 12years)
ADHD-RS-IV
VYVANSE (30mg/day) 43.2 (6.7) -21.8 (1.6) -15.6 (-19.9, -11.2)VYVANSE (50mg/day) 43.3 (6.7) -23.4 (1.6) -17.2 (-21.5, -12.9)VYVANSE (70mg/day) 45.1(6.8) -26.7 (1.5) -20.5 (-24.8, -16.2)Placebo 42.4 (7.1) -6.2 (1.6) --
Study 2(6 - 12years)
AverageSKAMP-DS
VYVANSE (30, 50 or70 mg/day) -- 0.8 (0.1) -0.9 (-1.1, -0.7)Placebo -- 1.7 (0.1) --
Study 3(6 - 12years)
AverageSKAMP-DS
VYVANSE (30, 50 or70 mg/day) 0.9 (1.0) 0.7 (0.1) -0.7 (-0.9, -0.6)Placebo 0.7 (0.9) 1.4 (0.1) --
*
†
†
†
† ‡ §
‡ §
† ¶ §
¶ §

SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI:confidence interval.*†‡§
¶
Study 4(13 - 17years)
ADHD-RS-IV
VYVANSE (30mg/day) 38.3 (6.7) -18.3 (1.2) -5.5 (-9.0, -2.0)VYVANSE (50mg/day) 37.3 (6.3) -21.1 (1.3) -8.3 (-11.8, -4.8)VYVANSE (70mg/day) 37.0 (7.3) -20.7 (1.3) -7.9 (-11.4, -4.5)Placebo 38.5 (7.1) -12.8 (1.2) --
Study 5(6 - 17years)
ADHD-RS-IV
VYVANSE (30, 50 or70 mg/day) 40.7 (7.3) -24.3 (1.2) -18.6 (-21.5, -15.7)Placebo 41.0 (7.1) -5.7 (1.1) --
Study 7(18 - 55years)
ADHD-RS-IV
VYVANSE (30mg/day) 40.5 (6.2) -16.2 (1.1) -8.0 (-11.5, -4.6)VYVANSE (50mg/day) 40.8 (7.3) -17.4 (1.0) -9.2 (-12.6, -5.7)VYVANSE (70mg/day) 41.0 (6.0) -18.6 (1.0) -10.4 (-13.9, -6.9)Placebo 39.4 (6.4) -8.2 (1.4) --
Study 8(18 - 55years)
AveragePERMP
VYVANSE (30, 50 or70 mg/day)
260.1(86.2) 312.9 (8.6) 23.4 (15.6, 31.2)
Placebo 261.4(75.0) 289.5 (8.6) --
Figure 4 LS Mean SKAMP Deportment Subscale Score by Treatment andTime-point for Pediatric Patients Ages 6 to 12 with ADHD after 1 Week ofDouble Blind Treatment (Study 3)
Difference (drug minus placebo) in least-squares mean change from baseline.Doses statistically significantly superior to placebo.Pre-dose SKAMP-DS was not collected.LS Mean for SKAMP-DS (Study 2 and 3) or PERMP (Study 8) is post-dose average score over allsessions of the treatment day, rather than change from baseline.Pre-dose SKAMP-DS (Study 3) or PERMP (Study 8) total score, averaged over both periods.
†
†
†
†
†
†
†
† ¶ §
¶ §
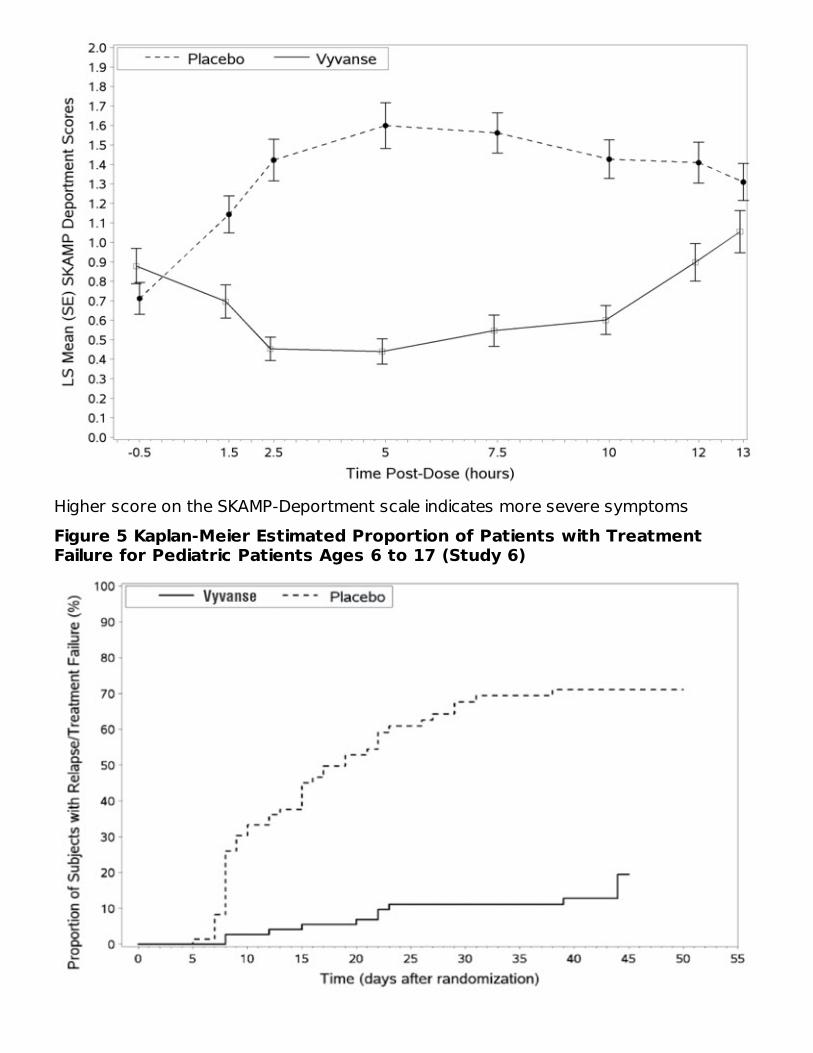
Higher score on the SKAMP-Deportment scale indicates more severe symptomsFigure 5 Kaplan-Meier Estimated Proportion of Patients with TreatmentFailure for Pediatric Patients Ages 6 to 17 (Study 6)

Figure 6 LS Mean (SE) PERMP Total Score by Treatment and Time-point forAdults Ages 18 to 55 with ADHD after 1 Week of Double Blind Treatment(Study 8)
Higher score on the PERMP scale indicates less severe symptoms.Figure 7 Kaplan-Meier Estimated Proportion of Subjects with Relapse inAdults with ADHD (Study 9)
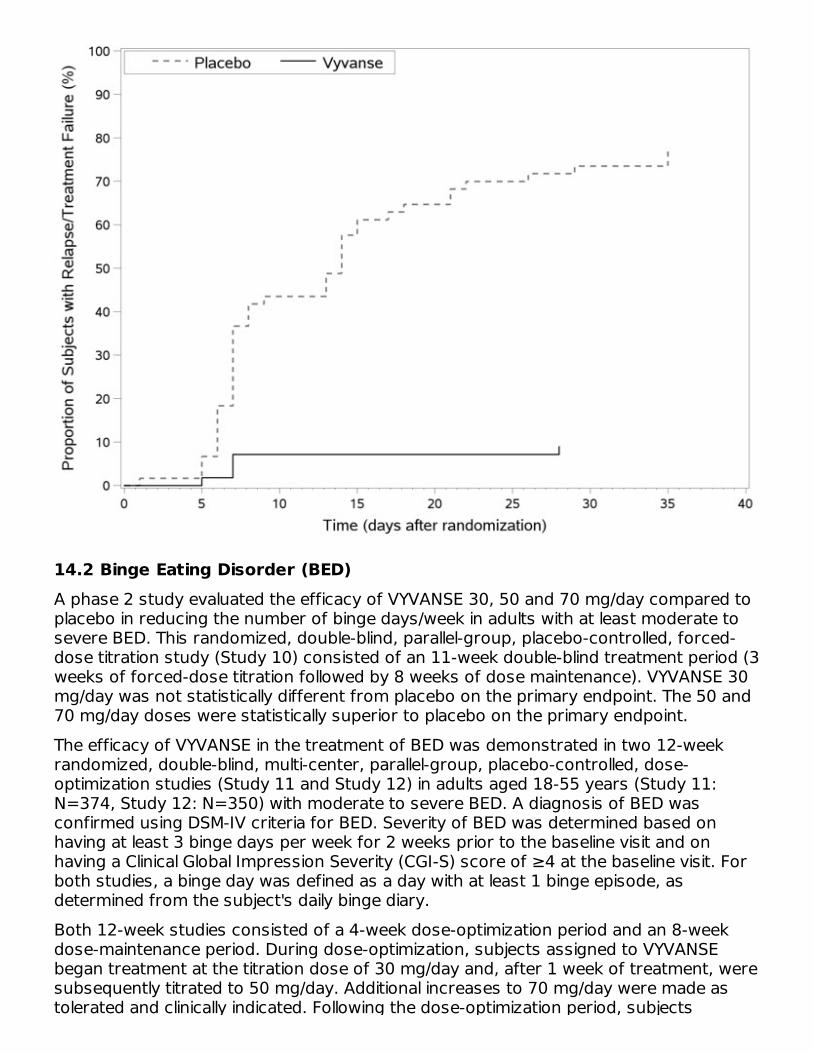
14.2 Binge Eating Disorder (BED)A phase 2 study evaluated the efficacy of VYVANSE 30, 50 and 70 mg/day compared toplacebo in reducing the number of binge days/week in adults with at least moderate tosevere BED. This randomized, double-blind, parallel-group, placebo-controlled, forced-dose titration study (Study 10) consisted of an 11-week double-blind treatment period (3weeks of forced-dose titration followed by 8 weeks of dose maintenance). VYVANSE 30mg/day was not statistically different from placebo on the primary endpoint. The 50 and70 mg/day doses were statistically superior to placebo on the primary endpoint.The efficacy of VYVANSE in the treatment of BED was demonstrated in two 12-weekrandomized, double-blind, multi-center, parallel-group, placebo-controlled, dose-optimization studies (Study 11 and Study 12) in adults aged 18-55 years (Study 11:N=374, Study 12: N=350) with moderate to severe BED. A diagnosis of BED wasconfirmed using DSM-IV criteria for BED. Severity of BED was determined based onhaving at least 3 binge days per week for 2 weeks prior to the baseline visit and onhaving a Clinical Global Impression Severity (CGI-S) score of ≥4 at the baseline visit. Forboth studies, a binge day was defined as a day with at least 1 binge episode, asdetermined from the subject's daily binge diary.Both 12-week studies consisted of a 4-week dose-optimization period and an 8-weekdose-maintenance period. During dose-optimization, subjects assigned to VYVANSEbegan treatment at the titration dose of 30 mg/day and, after 1 week of treatment, weresubsequently titrated to 50 mg/day. Additional increases to 70 mg/day were made astolerated and clinically indicated. Following the dose-optimization period, subjects

tolerated and clinically indicated. Following the dose-optimization period, subjectscontinued on their optimized dose for the duration of the dose-maintenance period.The primary efficacy outcome for the two studies was defined as the change frombaseline at Week 12 in the number of binge days per week. Baseline is defined as theweekly average of the number of binge days per week for the 14 days prior to thebaseline visit. Subjects from both studies on VYVANSE had a statistically significantlygreater reduction from baseline in mean number of binge days per week at Week 12. Inaddition, subjects on VYVANSE showed greater improvement as compared to placeboacross key secondary outcomes with higher proportion of subjects rated improved onthe CGI-I rating scale, higher proportion of subjects with 4-week binge cessation, andgreater reduction in the Yale-Brown Obsessive Compulsive Scale Modified for BingeEating (Y-BOCS-BE) total score.
Table 7: Summary of Primary Efficacy Results in BEDStudyNumber
TreatmentGroup
Primary Efficacy Measure: Binge Days perWeek at Week 12
Mean BaselineScore (SD)
LS MeanChange fromBaseline (SE)
Placebo-subtractedDifference
(95% CI)
SD: standard deviation; SE: standard error; LS Mean: least-squares mean; CI:confidence interval.*†
Study 11VYVANSE (50 or70 mg/day) 4.79 (1.27) -3.87 (0.12) -1.35 (-1.70, -
1.01)Placebo 4.60 (1.21) -2.51 (0.13) --
Study 12VYVANSE (50 or70 mg/day) 4.66 (1.27) -3.92 (0.14) -1.66 (-2.04, -
1.28)Placebo 4.82 (1.42) -2.26 (0.14) --
A double-blind, placebo controlled, randomized withdrawal design study (Study 13) wasconducted to evaluate maintenance of efficacy based on time to relapse betweenVYVANSE and placebo in adults aged 18 to 55 (N=267) with moderate to severe BED. Inthis longer-term study patients who had responded to VYVANSE in the preceding 12-week open-label treatment phase were randomized to continuation of VYVANSE orplacebo for up to 26 weeks of observation for relapse. Response in the open-label phasewas defined as 1 or fewer binge days each week for four consecutive weeks prior to thelast visit at the end of the 12-week open-label phase and a CGI-S score of 2 or less atthe same visit. Relapse during the double-blind phase was defined as having 2 or morebinge days each week for two consecutive weeks (14 days) prior to any visit and havingan increase in CGI-S score of 2 or more points compared to the randomized-withdrawalbaseline. Maintenance of efficacy for patients who had an initial response during theopen-label period and then continued on VYVANSE during the 26-week double-blindrandomized-withdrawal phase was demonstrated with VYVANSE being superior overplacebo as measured by time to relapse.Figure 8 Kaplan-Meier Estimated Proportions of Subjects with Relapse inAdults with BED (Study 13)
*
Difference (drug minus placebo) in least-squares mean change from baseline.Doses statistically significantly superior to placebo.
†
†

Examination of population subgroups based on age (there were no patients over 65),gender, and race did not reveal any clear evidence of differential responsiveness in thetreatment of BED.
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How SuppliedVYVANSE (lisdexamfetamine dimesylate) capsules:
VYVANSE capsules 10 mg: pink body/pink cap (imprinted with S489 and 10 mg),bottles of 100, NDC 59417-101-10VYVANSE capsules 20 mg: ivory body/ivory cap (imprinted with S489 and 20 mg),bottles of 100, NDC 59417-102-10VYVANSE capsules 30 mg: white body/orange cap (imprinted with S489 and 30 mg),bottles of 100, NDC 59417-103-10VYVANSE capsules 40 mg: white body/blue green cap (imprinted with S489 and 40mg), bottles of 100, NDC 59417-104-10VYVANSE capsules 50 mg: white body/blue cap (imprinted with S489 and 50 mg),bottles of 100, NDC 59417-105-10VYVANSE capsules 60 mg: aqua blue body/aqua blue cap (imprinted with S489 and60 mg), bottles of 100, NDC 59417-106-10VYVANSE capsules 70 mg: blue body/orange cap (imprinted with S489 and 70 mg),bottles of 100, NDC 59417-107-10
VYVANSE (lisdexamfetamine dimesylate) chewable tablets:VYVANSE chewable tablets 10 mg: White to off-white round shaped tablet debossedwith '10' on one side and 'S489' on the other, bottles of 100, NDC 59417-115-01VYVANSE chewable tablets 20 mg: White to off-white hexagonal shaped tabletdebossed with '20' on one side and 'S489' on the other, bottles of 100, NDC 59417-116-01VYVANSE chewable tablets 30 mg: White to off-white arc triangular shaped tablet

debossed with '30' on one side and 'S489' on the other, bottles of 100, NDC 59417-117-01VYVANSE chewable tablets 40 mg: White to off-white capsule shaped tabletdebossed with '40' on one side and 'S489' on the other, bottles of 100, NDC 59417-118-01VYVANSE chewable tablets 50 mg: White to off-white arc square shaped tabletdebossed with '50' on one side and 'S489' on the other, bottles of 100, NDC 59417-119-01VYVANSE chewable tablets 60 mg: White to off-white arc diamond shaped tabletdebossed with '60' on one side and 'S489' on the other, bottles of 100, NDC 59417-120-01
16.2 Storage and HandlingDispense in a tight, light-resistant container as defined in the USP.Store at room temperature, 20ºC to 25ºC (68ºF to 77ºF). Excursions permitted between15ºC and 30ºC (59 to 86ºF) [see USP Controlled Room Temperature].DisposalComply with local laws and regulations on drug disposal of CNS stimulants. Dispose ofremaining, unused, or expired VYVANSE by a medicine take-back program.
17 PATIENT COUNSELING INFORMATIONAdvise the patient to read the FDA-approved patient labeling (Medication Guide).Controlled Substance Status/High Potential for Abuse and DependenceAdvise patients that VYVANSE is a controlled substance and it can be abused and lead todependence and not to give VYVANSE to anyone else [see Drug Abuse and Dependence(9.1, 9.2, and 9.3)]. Advise patients to store VYVANSE in a safe place, preferably locked,to prevent abuse. Advise patients to dispose of remaining, unused, or expired VYVANSEby a medicine take-back program.Serious Cardiovascular RisksAdvise patients that there is a potential serious cardiovascular risk including suddendeath, myocardial infarction, stroke, and hypertension with VYVANSE use. Instructpatients to contact a healthcare provider immediately if they develop symptoms such asexertional chest pain, unexplained syncope, or other symptoms suggestive of cardiacdisease [see Warnings and Precautions (5.2)].Hypertension and TachycardiaInstruct patients that VYVANSE can cause elevations of their blood pressure and pulserate and they should be monitored for such effects.Psychiatric RisksAdvise patients that VYVANSE at recommended doses may cause psychotic or manicsymptoms even in patients without prior history of psychotic symptoms or mania [seeWarnings and Precautions (5.4)].Suppression of Growth

Advise patients that VYVANSE may cause slowing of growth including weight loss [seeWarnings and Precautions (5.5)].Impairment in Ability to Operate Machinery or VehiclesAdvise patients that VYVANSE may impair their ability to engage in potentially dangerousactivities such as operating machinery or vehicles. Instruct patients to find out howVYVANSE will affect them before engaging in potentially dangerous activities [seeAdverse Reactions (6.1, 6.2)].Circulation problems in fingers and toes [Peripheral vasculopathy, including Raynaud'sphenomenon]Instruct patients beginning treatment with VYVANSE about the risk of peripheralvasculopathy, including Raynaud's phenomenon, and associated signs and symptoms:fingers or toes may feel numb, cool, painful, and/or may change from pale, to blue, tored. Instruct patients to report to their physician any new numbness, pain, skin colorchange, or sensitivity to temperature in fingers or toes. Instruct patients to call theirphysician immediately with any signs of unexplained wounds appearing on fingers ortoes while taking VYVANSE. Further clinical evaluation (e.g., rheumatology referral) maybe appropriate for certain patients [see Warnings and Precautions (5.6)].Serotonin SyndromeCaution patients about the risk of serotonin syndrome with concomitant use ofVYVANSE and other serotonergic drugs including SSRIs, SNRIs, triptans, tricyclicantidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, St. John's Wort, andwith drugs that impair metabolism of serotonin (in particular MAOIs, both those intendedto treat psychiatric disorders and also others such as linezolid [see Contraindications (4),Warnings and Precautions (5.7) and Drug Interactions (7.1)]. Advise patients to contacttheir healthcare provider or report to the emergency room if they experience signs orsymptoms of serotonin syndrome.Concomitant MedicationsAdvise patients to notify their physicians if they are taking, or plan to take, anyprescription or over-the-counter drugs because there is a potential for interactions [seeDrug Interactions (7.1)].PregnancyAdvise patients of the potential fetal effects from the use of VYVANSE during pregnancy.Advise patients to notify their healthcare provider if they become pregnant or intend tobecome pregnant during treatment with VYVANSE [see Use in Specific Populations (8.1)].LactationAdvise women not to breastfeed if they are taking VYVANSE [see Use in SpecificPopulations (8.2)].Administration Instructions
Capsules: Advise patients to take the capsules whole or empty and mix the entirecontents with yogurt, water, or orange juice. Advise patients to consume the mixtureimmediately and not to store for future use [see Dosage and Administration (2.2)].Chewable tablets: Advise patients that chewable tablets must be chewed thoroughlybefore swallowing [see Dosage and Administration (2.2)].

Distributed by:Takeda Pharmaceuticals America, Inc.Lexington, MA 02421Made in USAFor more information call 1-800-828-2088VYVANSE and the VYVANSE Logo are registered trademarks of TakedaPharmaceuticals U.S.A., Inc.©2021 Takeda Pharmaceuticals U.S.A., Inc. All rights reserved.US Pat No. 7,105,486, 7,223,735, 7,655,630, 7,659,253, 7,659,254, 7,662,787,7,662,788, 7,671,030, 7,671,031, 7,674,774, 7,678,770, 7,678,771, 7,687,466,7,687,467, 7,713,936, 7,718,619, 7,723,305
MEDICATION GUIDEVYVANSE (Vi' – vans)
(lisdexamfetamine dimesylate)Capsules and Chewable Tablets, CII
What is the most important information I should know about VYVANSE?VYVANSE may cause serious side effects, including:
Abuse and dependence. VYVANSE, other amphetamine containing medicines, andmethylphenidate have a high chance for abuse and may cause physical andpsychological dependence. Your healthcare provider should check you or your childfor signs of abuse and dependence before and during treatment with VYVANSE.
Tell your healthcare provider if you or your child have ever abused or beendependent on alcohol, prescription medicines, or street drugs.Your healthcare provider can tell you more about the differences between physicaland psychological dependence and drug addiction.
Heart-related problems including:sudden death, stroke, and heart attack in adultssudden death in children who have heart problems or heart defectsincreased blood pressure and heart rate
Your healthcare provider should check you or your child carefully for heart problemsbefore starting treatment with VYVANSE. Tell your healthcare provider if you or yourchild have any heart problems, heart defects, high blood pressure, or a family historyof these problems.Your healthcare provider should check your or your child's blood pressure and heartrate regularly during treatment with VYVANSE.Call your healthcare provider or go to the nearest hospital emergencyroom right away if you or your child have any signs of heart problemssuch as chest pain, shortness of breath, or fainting during treatment withVYVANSE.Mental (psychiatric) problems, including:
new or worse behavior and thought problemsnew or worse bipolar illnessnew psychotic symptoms (such as hearing voices, or seeing or believing thingsthat are not real) or new manic symptoms
® ®
®

Tell your healthcare provider about any mental problems you or your child have orabout a family history of suicide, bipolar illness, or depression.Call your healthcare provider right away if you or your child have any newor worsening mental symptoms or problems during treatment withVYVANSE, especially hearing voices, seeing or believing things that arenot real, or new manic symptoms.
What is VYVANSE? VYVANSE is a central nervous system (CNS) stimulant prescription medicine used forthe treatment of:
Attention Deficit Hyperactivity Disorder (ADHD) in adults and children 6 years of ageand older. VYVANSE may help increase attention and decrease impulsiveness andhyperactivity in people with ADHD.Moderate to severe binge eating disorder (BED) in adults. VYVANSE may help reducethe number of binge eating days in people with BED.
VYVANSE is not for use in children under 6 years of age with ADHD.VYVANSE is not for weight loss. It is not known if VYVANSE is safe and effective for thetreatment of obesity.It is not known if VYVANSE is safe and effective for use in children with BED.VYVANSE is a federally controlled substance (CII) because it containslisdexamfetamine dimesylate that can be a target for people who abuseprescription medicines or street drugs. Keep VYVANSE in a safe place to protect itfrom theft. Never give your VYVANSE to anyone else because it may cause death orharm them. Selling or giving away VYVANSE may harm others and is against the law.Do not take VYVANSE if you or your child are:
allergic to amphetamine products or any of the ingredients in VYVANSE. See the endof this Medication Guide for a complete list of ingredients in VYVANSE.taking, or have stopped taking in the last 14 days, a medicine called a MonoamineOxidase Inhibitor (MAOI).being treated with the antibiotic linezolid or intravenous methylene blue.
Before taking VYVANSE, tell your healthcare provider about all medicalconditions, including if you or your child:
have heart problems, heart defects, or high blood pressurehave mental problems including psychosis, mania, bipolar illness, or depression orhave a family history of suicide, bipolar illness, or depressionhave circulation problems in fingers and toesare pregnant or plan to become pregnant. VYVANSE may harm the unborn baby.
There is a pregnancy registry for females who are exposed to VYVANSE duringpregnancy. The purpose of the registry is to collect information about the healthof females exposed to VYVANSE and their baby. If you or your child becomespregnant during treatment with VYVANSE, talk to your healthcare provider aboutregistering with the National Pregnancy Registry for Psychostimulants at 1-866-961-2388 or visit online at https://womensmentalhealth.org/clinical-and-research-programs/pregnancyregistry/adhd-medications/.
are breastfeeding or plan to breastfeed. VYVANSE passes into breast milk. Youshould not breastfeed during treatment with VYVANSE. Talk to your healthcareprovider about the best way to feed the baby during treatment with VYVANSE.

Tell your healthcare provider about all the medicines that you or your childtake, including prescription and over-the-counter medicines, vitamins, and herbalsupplements.VYVANSE can affect the way other medicines work and other medicines may affect howVYVANSE works. Taking VYVANSE with other medicines can cause serious side effects.Sometimes the doses of other medicines will need to be changed while taking VYVANSE.Especially tell your healthcare provider if you or your child take:
selective serotonin reuptake inhibitors(SSRIs)medicines used to treat migraineheadaches called triptanslithiumtramadolbuspirone
serotonin norepinephrine reuptakeinhibitors (SNRIs)tricyclic antidepressantsfentanyltryptophanSt. John's Wort
Keep a list of all medicines to show your healthcare provider and pharmacist when youget a new medicine. Your healthcare provider will decide if VYVANSE can be taken withother medicines.Do not start any new medicine during treatment with VYVANSE withouttalking to your healthcare provider first.How should VYVANSE be taken?
Take VYVANSE exactly as prescribed by your healthcare provider.Your healthcare provider may change the dose if needed.Take VYVANSE 1 time each day in the morning with or without food.Your healthcare provider may sometimes stop VYVANSE treatment for a while tocheck ADHD or BED symptoms.VYVANSE comes in capsules or chewable tablets.Taking VYVANSE Capsules:
VYVANSE capsules may be swallowed whole.If VYVANSE capsules cannot be swallowed whole, the capsule may be opened andthe entire contents sprinkled onto yogurt, or poured into water or orange juice.
Using a spoon, break apart any powder that is stuck together. Stir theVYVANSE powder and yogurt, water, or orange juice until they are completelymixed together.Swallow all the yogurt, water, or orange juice mixture right away. Do not storethe yogurt, water, or orange juice mixture.It is normal to see a filmy coating on the inside of your glass or container afteryou eat or drink all the VYVANSE mixture.
Taking VYVANSE Chewable Tablets:Chew VYVANSE tablets completely before swallowing.
If you or your child take too much VYVANSE, call your healthcare provider or poisoncontrol center at 1-800-222-1222 or go to the nearest hospital emergency room rightaway.What should I avoid while taking VYVANSE? Do not drive, operate machinery, or do other dangerous activities until you know howVYVANSE affects you.What are the possible side effects of VYVANSE?VYVANSE may cause serious side effects, including:
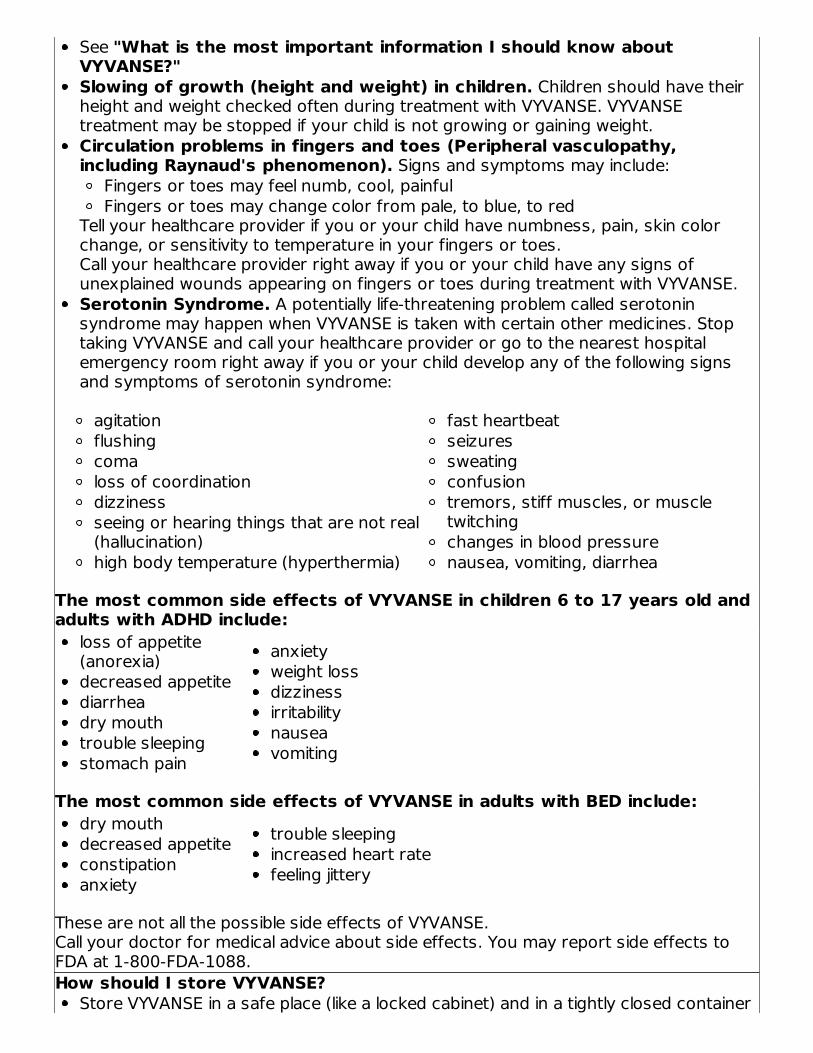
See "What is the most important information I should know aboutVYVANSE?"Slowing of growth (height and weight) in children. Children should have theirheight and weight checked often during treatment with VYVANSE. VYVANSEtreatment may be stopped if your child is not growing or gaining weight.Circulation problems in fingers and toes (Peripheral vasculopathy,including Raynaud's phenomenon). Signs and symptoms may include:
Fingers or toes may feel numb, cool, painfulFingers or toes may change color from pale, to blue, to red
Tell your healthcare provider if you or your child have numbness, pain, skin colorchange, or sensitivity to temperature in your fingers or toes.Call your healthcare provider right away if you or your child have any signs ofunexplained wounds appearing on fingers or toes during treatment with VYVANSE.Serotonin Syndrome. A potentially life-threatening problem called serotoninsyndrome may happen when VYVANSE is taken with certain other medicines. Stoptaking VYVANSE and call your healthcare provider or go to the nearest hospitalemergency room right away if you or your child develop any of the following signsand symptoms of serotonin syndrome:
agitationflushingcomaloss of coordinationdizzinessseeing or hearing things that are not real(hallucination)high body temperature (hyperthermia)
fast heartbeatseizuressweatingconfusiontremors, stiff muscles, or muscletwitchingchanges in blood pressurenausea, vomiting, diarrhea
The most common side effects of VYVANSE in children 6 to 17 years old andadults with ADHD include:
loss of appetite(anorexia)decreased appetitediarrheadry mouthtrouble sleepingstomach pain
anxietyweight lossdizzinessirritabilitynauseavomiting
The most common side effects of VYVANSE in adults with BED include:dry mouthdecreased appetiteconstipationanxiety
trouble sleepingincreased heart ratefeeling jittery
These are not all the possible side effects of VYVANSE.Call your doctor for medical advice about side effects. You may report side effects toFDA at 1-800-FDA-1088.How should I store VYVANSE?
Store VYVANSE in a safe place (like a locked cabinet) and in a tightly closed container

This Medication Guide has been approved by the U.S. Food andDrug Administration. Revised: 10/2021
at room temperature between 68°F to 77°F (20°C to 25°C).Protect VYVANSE from light.Dispose of remaining, unused, or expired VYVANSE by a medicine take-backprogram at authorized collection sites such as retail pharmacies, hospital or clinicpharmacies, and law enforcement locations. If no take-back program or authorizedcollector is available, mix VYVANSE with an undesirable, nontoxic substance such asdirt, cat litter, or used coffee grounds to make it less appealing to children and pets.Place the mixture in a container such as a sealed plastic bag and throw away(discard) VYVANSE in the household trash.
Keep VYVANSE and all medicines out of the reach of children.General information about the safe and effective use of VYVANSE. Medicines are sometimes prescribed for purposes other than those listed in aMedication Guide. Do not use VYVANSE for a condition for which it was not prescribed.Do not give VYVANSE to other people, even if they have the same symptoms that youhave. It may harm them and it is against the law. You can ask your pharmacist orhealthcare provider for information about VYVANSE that is written for healthprofessionals.What are the ingredients in VYVANSE?Active ingredient: lisdexamfetamine dimesylateCapsule Inactive ingredients: microcrystalline cellulose, croscarmellose sodium, andmagnesium stearate. The capsule shells (imprinted with S489) contain gelatin, titaniumdioxide, and one or more of the following: FD&C Red #3, FD&C Yellow #6, FD&C Blue#1, Black Iron Oxide, and Yellow Iron Oxide.Chewable Tablet Inactive Ingredients: colloidal silicon dioxide, croscarmellosesodium, guar gum, magnesium stearate, mannitol, microcrystalline cellulose, sucralose,artificial strawberry flavor.Distributed by: Takeda Pharmaceuticals America, Inc., Lexington, MA 02421. VYVANSEand the VYVANSE Logo are registered trademarks of Takeda Pharmaceuticals U.S.A.,Inc. © 2021 Takeda Pharmaceuticals U.S.A., Inc. All rights reserved.For more information, go to www.vyvanse.com or call 1-800-828-2088.
PRINCIPAL DISPLAY PANEL - 10 mg Capsule Bottle LabelNDC 59417-101-10Vyvanse (lisdexamfetaminedimesylate) capsules10 mgCIIRx only100 CAPSULESTakeda
®®
®

PRINCIPAL DISPLAY PANEL - 20 mg Capsule Bottle LabelNDC 59417-102-10Vyvanse (lisdexamfetaminedimesylate) capsules20 mgCIIRx only100 CAPSULESTakeda
PRINCIPAL DISPLAY PANEL - 30 mg Capsule Bottle LabelNDC 59417-103-10Vyvanse (lisdexamfetaminedimesylate) capsules30 mgCIIRx only100 CAPSULESTakeda
®
®

PRINCIPAL DISPLAY PANEL - 40 mg Capsule Bottle LabelNDC 59417-104-10Vyvanse (lisdexamfetaminedimesylate) capsules40 mgCIIRx only100 CAPSULESTakeda
PRINCIPAL DISPLAY PANEL - 50 mg Capsule Bottle LabelNDC 59417-105-10Vyvanse (lisdexamfetaminedimesylate) capsules50 mgCIIRx only100 CAPSULESTakeda
®
®

PRINCIPAL DISPLAY PANEL - 60 mg Capsule Bottle LabelNDC 59417-106-10Vyvanse (lisdexamfetaminedimesylate) capsules60 mgCIIRx only100 CAPSULESTakeda
PRINCIPAL DISPLAY PANEL - 70 mg Capsule Bottle LabelNDC 59417-107-10Vyvanse (lisdexamfetaminedimesylate) capsules70 mgCIIRx only100 CAPSULESTakeda
®
®
PRINCIPAL DISPLAY PANEL - 10 mg Tablet Bottle LabelNDC 59417-115-01Vyvanse (lisdexamfetaminedimesylate) chewable tablets10 mg100 CHEWABLETABLETSChew tablets completelybefore swallowing. Donot swallow tablets whole.CIIRx onlyTakeda
PRINCIPAL DISPLAY PANEL - 20 mg Tablet Bottle LabelNDC 59417-116-01Vyvanse (lisdexamfetaminedimesylate) chewable tablets20 mg
®
®

100 CHEWABLETABLETSChew tablets completelybefore swallowing. Donot swallow tablets whole.CIIRx onlyTakeda
PRINCIPAL DISPLAY PANEL - 30 mg Tablet Bottle LabelNDC 59417-117-01Vyvanse (lisdexamfetaminedimesylate) chewable tablets30 mg100 CHEWABLETABLETSChew tablets completelybefore swallowing. Donot swallow tablets whole.CIIRx onlyTakeda
®

PRINCIPAL DISPLAY PANEL - 40 mg Tablet Bottle LabelNDC 59417-118-01Vyvanse (lisdexamfetaminedimesylate) chewable tablets40 mg100 CHEWABLETABLETSChew tablets completelybefore swallowing. Donot swallow tablets whole.CIIRx onlyTakeda
PRINCIPAL DISPLAY PANEL - 50 mg Tablet Bottle LabelNDC 59417-119-01
®
®

Vyvanse (lisdexamfetaminedimesylate) chewable tablets50 mg100 CHEWABLETABLETSChew tablets completelybefore swallowing. Donot swallow tablets whole.CIIRx onlyTakeda
PRINCIPAL DISPLAY PANEL - 60 mg Tablet Bottle LabelNDC 59417-120-01Vyvanse (lisdexamfetaminedimesylate) chewable tablets60 mg100 CHEWABLETABLETSChew tablets completelybefore swallowing. Donot swallow tablets whole.CIIRx onlyTakeda
®
®

VYVANSE lisdexamfetamine dimesylate capsule
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-101
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 10 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C RED NO. 3 (UNII: PN2ZH5LOQY)
Product CharacteristicsColor PINK Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;10mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date
1 NDC:59417-101-10
100 in 1 BOTTLE; Type 0: Not a CombinationProduct 08/30/2014
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA021977 08/30/2014
VYVANSE lisdexamfetamine dimesylate capsule
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-102
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 20 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FERRIC OXIDE YELLOW (UNII: EX438O2MRT)
Product CharacteristicsColor WHITE (ivory) Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;20mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-102-
10100 in 1 BOTTLE; Type 0: Not a CombinationProduct 12/10/2007

Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA021977 12/10/2007
VYVANSE lisdexamfetamine dimesylate capsule
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-103
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 30 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C RED NO. 3 (UNII: PN2ZH5LOQY) FD&C YELLOW NO. 6 (UNII: H77VEI93A8)
Product CharacteristicsColor WHITE (white) , ORANGE (orange) Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;30mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-103-
10100 in 1 BOTTLE; Type 0: Not a CombinationProduct 02/23/2007
Marketing InformationMarketing Application Number or Monograph Marketing Start Marketing End

Category Citation Date DateNDA NDA021977 02/23/2007
VYVANSE lisdexamfetamine dimesylate capsule
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-104
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 40 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FERROSOFERRIC OXIDE (UNII: XM0M87F357) FERRIC OXIDE YELLOW (UNII: EX438O2MRT)
Product CharacteristicsColor WHITE (white) , TURQUOISE (blue-green) Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;40mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-104-
10100 in 1 BOTTLE; Type 0: Not a CombinationProduct 12/10/2007
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA021977 12/10/2007

NDA NDA021977 12/10/2007
VYVANSE lisdexamfetamine dimesylate capsule
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-105
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 50 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C BLUE NO. 1 (UNII: H3R47K3TBD)
Product CharacteristicsColor WHITE (white) , BLUE (blue) Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;50mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-105-
10100 in 1 BOTTLE; Type 0: Not a CombinationProduct 02/23/2007
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA021977 02/23/2007
VYVANSE

lisdexamfetamine dimesylate capsule
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-106
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 60 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C BLUE NO. 1 (UNII: H3R47K3TBD)
Product CharacteristicsColor TURQUOISE (aqua) Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;60mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-106-
10100 in 1 BOTTLE; Type 0: Not a CombinationProduct 12/10/2007
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA021977 12/10/2007
VYVANSE lisdexamfetamine dimesylate capsule
Product Information

Product Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-107
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 70 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) GELATIN, UNSPECIFIED (UNII: 2G86QN327L) TITANIUM DIOXIDE (UNII: 15FIX9V2JP) FD&C BLUE NO. 1 (UNII: H3R47K3TBD) FD&C RED NO. 3 (UNII: PN2ZH5LOQY) FD&C YELLOW NO. 6 (UNII: H77VEI93A8)
Product CharacteristicsColor BLUE (blue) , ORANGE (orange) Score no scoreShape CAPSULE (CAPSULE) Size 16mmFlavor Imprint Code S489;70mgContains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-107-
10100 in 1 BOTTLE; Type 0: Not a CombinationProduct 02/23/2007
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA021977 02/23/2007
VYVANSE lisdexamfetamine dimesylate tablet, chewable
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-115
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 10 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) MANNITOL (UNII: 3OWL53L36A) SUCRALOSE (UNII: 96K6UQ3ZD4) GUAR GUM (UNII: E89I1637KE)
Product CharacteristicsColor WHITE (White to off-white) Score no scoreShape ROUND Size 7mmFlavor STRAWBERRY Imprint Code 10;S489Contains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-115-
01100 in 1 BOTTLE; Type 0: Not a CombinationProduct 01/28/2017
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA208510 01/28/2017
VYVANSE lisdexamfetamine dimesylate tablet, chewable
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-116
Route of Administration ORAL DEA Schedule CII

Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 20 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) MANNITOL (UNII: 3OWL53L36A) SUCRALOSE (UNII: 96K6UQ3ZD4) GUAR GUM (UNII: E89I1637KE)
Product CharacteristicsColor WHITE (White to off-white) Score no scoreShape HEXAGON (6 SIDED) Size 10mmFlavor STRAWBERRY Imprint Code 20;S489Contains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-116-
01100 in 1 BOTTLE; Type 0: Not a CombinationProduct 01/28/2017
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA208510 01/28/2017
VYVANSE lisdexamfetamine dimesylate tablet, chewable
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-117
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength

LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 30 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) MANNITOL (UNII: 3OWL53L36A) SUCRALOSE (UNII: 96K6UQ3ZD4) GUAR GUM (UNII: E89I1637KE)
Product CharacteristicsColor WHITE (White to off-white) Score no scoreShape TRIANGLE Size 11mmFlavor STRAWBERRY Imprint Code 30;S489Contains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-117-
01100 in 1 BOTTLE; Type 0: Not a CombinationProduct 01/28/2017
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA208510 01/28/2017
VYVANSE lisdexamfetamine dimesylate tablet, chewable
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-118
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 40 mg

Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) MANNITOL (UNII: 3OWL53L36A) SUCRALOSE (UNII: 96K6UQ3ZD4) GUAR GUM (UNII: E89I1637KE)
Product CharacteristicsColor WHITE (White to off-white) Score no scoreShape OVAL (CAPSULE) Size 14mmFlavor STRAWBERRY Imprint Code 40;S489Contains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-118-
01100 in 1 BOTTLE; Type 0: Not a CombinationProduct 01/28/2017
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA208510 01/28/2017
VYVANSE lisdexamfetamine dimesylate tablet, chewable
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-119
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 50 mg
Inactive Ingredients

Ingredient Name StrengthMICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U) SILICON DIOXIDE (UNII: ETJ7Z6XBU4) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) MANNITOL (UNII: 3OWL53L36A) SUCRALOSE (UNII: 96K6UQ3ZD4) GUAR GUM (UNII: E89I1637KE)
Product CharacteristicsColor WHITE (White to off-white) Score no scoreShape SQUARE Size 10mmFlavor STRAWBERRY Imprint Code 50;S489Contains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-119-
01100 in 1 BOTTLE; Type 0: Not a CombinationProduct 01/28/2017
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA208510 01/28/2017
VYVANSE lisdexamfetamine dimesylate tablet, chewable
Product InformationProduct Type HUMAN PRESCRIPTION DRUG Item Code (Source) NDC:59417-120
Route of Administration ORAL DEA Schedule CII
Active Ingredient/Active MoietyIngredient Name Basis of Strength Strength
LISDEXAMFETAMINE DIMESYLATE (UNII: SJT761GEGS) (LISDEXAMFETAMINE -UNII:H645GUL8KJ)
LISDEXAMFETAMINEDIMESYLATE 60 mg
Inactive IngredientsIngredient Name Strength
MICROCRYSTALLINE CELLULOSE (UNII: OP1R32D61U)

SILICON DIOXIDE (UNII: ETJ7Z6XBU4) CROSCARMELLOSE SODIUM (UNII: M28OL1HH48) MAGNESIUM STEARATE (UNII: 70097M6I30) MANNITOL (UNII: 3OWL53L36A) SUCRALOSE (UNII: 96K6UQ3ZD4) GUAR GUM (UNII: E89I1637KE)
Product CharacteristicsColor WHITE (White to off-white) Score no scoreShape DIAMOND Size 14mmFlavor STRAWBERRY Imprint Code 60;S489Contains
Packaging# Item Code Package Description Marketing Start
DateMarketing End
Date1 NDC:59417-120-
01100 in 1 BOTTLE; Type 0: Not a CombinationProduct 01/28/2017
Marketing InformationMarketingCategory
Application Number or MonographCitation
Marketing StartDate
Marketing EndDate
NDA NDA208510 01/28/2017
Labeler - Takeda Pharmaceuticals America, Inc. (830134016)
EstablishmentName Address ID/FEI Business Operations
AMRIRensselaer,Inc.
124193793
ANALYSIS(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106,59417-107, 59417-115, 59417-116, 59417-117, 59417-118, 59417-119, 59417-120), API MANUFACTURE(59417-101, 59417-102, 59417-103, 59417-104, 59417-105,59417-106, 59417-107, 59417-115, 59417-116, 59417-117, 59417-118, 59417-119,59417-120)
EstablishmentName Address ID/FEI Business Operations
CambrexCharlesCity, Inc
782974257
ANALYSIS(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106,59417-107, 59417-115, 59417-116, 59417-117, 59417-118, 59417-119, 59417-120) ,API MANUFACTURE(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106, 59417-107, 59417-115, 59417-116, 59417-117, 59417-118, 59417-119, 59417-120)
EstablishmentName Address ID/FEI Business Operations
PatheonManufacturingServices LLC
079415560ANALYSIS(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106,59417-107) , MANUFACTURE(59417-101, 59417-102, 59417-103, 59417-104,59417-105, 59417-106, 59417-107) , PACK(59417-101, 59417-102, 59417-103,

Takeda Pharmaceuticals America, Inc.
Services LLC 59417-104, 59417-105, 59417-106, 59417-107)
EstablishmentName Address ID/FEI Business Operations
Metrics,Inc. 867220261 ANALYSIS(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106,
59417-107)
EstablishmentName Address ID/FEI Business Operations
PatheonPharmaceuticalsInc.
005286822
ANALYSIS(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106, 59417-107, 59417-115, 59417-116, 59417-117, 59417-118, 59417-119,59417-120) , MANUFACTURE(59417-101, 59417-102, 59417-103, 59417-104,59417-105, 59417-106, 59417-107, 59417-115, 59417-116, 59417-117, 59417-118, 59417-119, 59417-120) , PACK(59417-101, 59417-102, 59417-103, 59417-104, 59417-105, 59417-106, 59417-107, 59417-115, 59417-116, 59417-117,59417-118, 59417-119, 59417-120)
EstablishmentName Address ID/FEI Business Operations
Sharp PackagingSystems, Inc. 143696495 PACK(59417-101, 59417-102, 59417-103, 59417-104, 59417-105,
59417-106, 59417-107)
Revised: 11/2021





























