Embed Size (px)
Citation preview

Central Annals of Public Health and Research
Cite this article: Vizcarra CB, Safaei J (2016) Stunting in Peruvian Children: an Empirical Analysis. Ann Public Health Res 3(4): 1047.
*Corresponding authorJalil Safaei, Department of Economics, University of Northern British Columbia, Prince George, BC, V2N 4Z9, Canada, Tel: 12509606698; Fax: 12509605545; Email:
Submitted: 16 July 2016
Accepted: 06 September 2016
Published: 08 September 2016
Copyright© 2016 Safaei et al.
OPEN ACCESS
Keywords•Stunting•Under-nutrition•Peruvian children•Logistic regression
Research Article
Stunting in Peruvian Children: an Empirical AnalysisClaudia Benavides Vizcarra1 and Jalil Safaei2*1Ministry of Social Development, Peru2Department of Economics, University of Northern British Columbia, Canada
Abstract
Objective: To analyze the various factors underlying stunting status in Peruvian children aged between two and five years.
Design: Using pooled cross-sectional data for children aged 24 - 59 months from the Peruvian Demographic and Health Survey for the period 2009-2012, a multivariate logistic regression model is used to estimate the effect of individual, household and community factors on stunting status for children in this age group.
Findings: The results indicate considerable effects at each of the individual, household and community levels. Significant determinants at the individual level are gender and low birth weight. At the household level, wealth and mother’s education are significantly associated with child stunting. Access to delivery services and living in mountains (the Andes area) are significant factors at the community or environmental level.
Conclusion: The findings of this study are consistent with those in the literature, and provide support for the multifaceted approach to reducing stunting. Policies to provide more equitable maternal care and nutrition, educating mothers and improving the economic wellbeing of the poor and less wealthy families can reduce stunting in Peruvian children. Also, the Articulated Nutrition Program implemented by the Peruvian government since 2008 appears to have had favorable impact on younger children who have had the opportunity to potentially benefit from it.
ABBREVIATIONSANP: Articulated Nutrition Program; DHS: Demographic
and Health Survey; LAC: Latin America and Caribbean; MDG: Millennium Development Goals
INTRODUCTIONChronic Under-nutrition is a major problem of public health
whose effects are manifested throughout the human life cycle. These effects include a greater likelihood of illness or premature death in children less than five years of age, a greater likelihood of later entry to school, poor cognitive development, poor school performance, reduced productivity and low work capacity leading to increased costs and economic losses to the family and society [1-3].
In a study of 3 000 children born between the years 1994-1995 and 2000-2001in four countries (Ethiopia, India, Peru and Vietnam), Save the Children [4] estimated the global economic impact of child under-nutrition at 125 billion dollars a year by the time today’s children reach working age in 2030. The study finds that chronically under-nourished children are significantly less able to read, write a simple sentence, or perform basic arithmetic,
and their average adult earnings will be 20% less than healthy children.
Therefore, child under-nutrition is a global problem that has been recognized by many developing countries as well as aid organizations. It has been an explicit part of the first Millennium Development Goals (MDG), namely eradicating poverty, hunger and under-nutrition, which is critically related to other goals such as reducing child mortality and improving maternal health [5].The global agenda still considers child under-nutrition as a priority even after 2015. At the 65th World Health Assembly in May 2012, WHO Member States endorsed a Comprehensive Implementation Plan on Maternal, Infant and Child Nutrition that included a 40% reduction in the number of stunted children by 2025 against the 2010 baseline as a part of six global targets to be achieved [6].
Under-nutrition is defined as the outcome of insufficient food intake and repeated infectious diseases [7]. However, its manifestations on children health status will vary depending on severity, duration and age of the children [8]. As such, under-nutrition has been divided in two categories of acute and chronic, most often demonstrated by wasting and stunting, respectively [9], or by underweight if it is a combination of both categories

Central
Safaei et al. (2016)Email:
Ann Public Health Res 3(4): 1047 (2016) 2/7
[10]. Acute under-nutrition is considered to be the effect of an immediate problem such as sudden catastrophes, seasonal depressions/shortages, highly infection-disease environments. Whereas, chronic under-nutrition is more closely associated with latent poverty, chronic food insecurity, poor feeding practices, and prolonged health problem [11,9]. Stunting is a problem of chronic under-nutrition. It is more specifically defined as “the inability to attain potential height for a particular age” [9], and is measured by the percentage of children aged 0 to 59 months whose height for age is below minus two standard deviations moderate stunting and minus three standard deviations (severe stunting) from the median of WHO child growth standards [10].
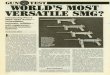
Stunting rates vary significantly across the regions of the globe. However, there have been substantial reductions in the rates from 1990 to 2014 (except for Oceania). Eastern Asia, Southern Asia (SA) and South-Eastern Asia (SEA) have achieved remarkable reductions in the prevalence of stunting between 1990 and 2014. The reduction in Sub-Saharan Africa (SSA), a region with very high prevalence of stunting, has not been as remarkable, however (See Figure 1 below).
Figure (1) implies that stunting rates are related to the level of economic development and income in different regions. In fact, stunting rates have been calculated for different groups of countries categorized as Low Income, Lower Middle Income, Upper Middle Income and Higher Income groups. There is a clear income gradient of stunting prevalence among the countries. As shown in Figure (2), the lower the income, the higher the prevalence of stunting.
The stunting rate in the Americas region has been below the global average See Figure (2). However, the rates are varied in this region as well. The variations cannot be explained by income group alone. As Figure (3) shows, significant variation in the stunting rates is observed for the Upper Middle Income countries of Latin America and Caribbean (LAC), which includes Peru.
Among the upper middle income countries of LAC, Peru had
29
49
23
36
60
47
30
37 37
18
36
117
36
27
17
39
15
0
10
20
30
40
50
60
NA SSA LAC EA SA SEA WA OCEN CCA
1990
2014
Figure 1 Estimated prevalence (%) of stunting (moderate or severe) for children under-five years of age by region: 1990 and 2014Note: This figure is constructed with information from the joint data of UNICEF, WHO and World Bank [12]. The abbreviations are: NA (Northern Africa); SSA (Sub-Saharan Africa); LAC (Latin America and Caribbean); EA (Eastern Asia); SA (Southern Asia); SEA (South-Eastern Asia); WA (Western Asia); OCEN (Oceania); CCA (Caucasus and Central Asia).
37.633.5
7.53.3
0
5
10
15
20
25
30
35
40
Low IncomeGroup
Lower middleincome Group
Upper middleincome Group
High IncomeGroup
Figure 2 Prevalence (%) of stunting (moderate or severe) in children less than five years old by Income Groups in 2014Note: This figure is constructed with information from the joint data of UNICEF, WHO and World Bank [12]. The Income Groups are the categorizations by the MDG.
7
13
67
1214
1918
0
5
10
15
20
25
BR CO CR DR LAC MEX PAN PER
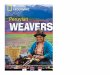
Figure 3 Prevalence (%) of stunting (moderate or severe) in children under-five years of age in Upper Middle Income countries of Latin American and Caribbean over the period 2006-2013.Note: This figure is constructed with information from the joint data of UNICEF, WHO and World Bank [12]. The data are from surveys in different years covering the period 2006-2013. The countries are labeled as: BR (Brazil); CO (Colombia); CR (Costa Rica); DR (Dominican Republic); LAC (Latin America and Caribbean); MEX (Mexico); PAN (Panama) and PER (Peru).
the highest rate of stunting after Panama (It should be noted that the rate for Panama is for 2008, whereas the rate for Peru is for 2013). Yet, this rate is about half the rate prevailing in 1990 See Figure (4). According to the Demographic and Family Health Survey (DFHS) for the years 2000-2012, stunting in Peruvian children less than five years old stood at 38% in 1990. A decade later the rate dropped to 30%, which remained more or less unchanged during the following decade till 2008.There has been a marked decline in the rate over the 2009-2012 period, bringing the rate down to 18.1. Figure 4 shows the stunting trend in Peru since 1990. It shows a wide difference in stunting rates between the rural and urban areas since 2007 when separate data became available. Despite these improvements, the rates of stunting still remain high in the rural areas and in some geographic regions of Peru such as Huancavelica, Cajamarca and Loreto where the stunting prevalence is as high as 50, 35 and 30%, respectively [13,14].

Central
Safaei et al. (2016)Email:
Ann Public Health Res 3(4): 1047 (2016) 3/7
Understandably, chronic under-nutrition and stunting has been a priority for the Peruvian Government. It was one of the main indicators of the National Plan to Take Action for the Infancy and Adolescence for the year 2021 [16]. It was also one of the main outcomes of the Budget for Results policy, which was implemented since 2007 [17].
To help finding the appropriate policy responses to stunting, especially in the rural areas, we need to better understand the underlying causes and covariates of stunting.
There are numerous studies on child under-nutrition or stunting. Some studies examine the relationship between under-nutrition and child health condition (e.g. diarrhea, respiratory infection, and low weight at birth. Others have focused on availability of child and maternal care - notably breastfeeding and nutritional intake – and access to health care as determinants of under-nutrition. Yet other studies investigate the impact of the country’s economic standing as whole, or the socioeconomic status of households (notably mother’s education) on under-nutrition.
Following the introduction of the conceptual framework by UNICEF [18], and recognition that the causes of chronic under-nutrition are numerous ranging from immediate to underlying to basic causes, a number of empirical studies use multilevel models to study child under-nutrition throughout the developing world. They include studies in Africa [19-22], India [23], Latin America [24-26], and Peru [27-30], among others.
Of the studies on Peru, Lescano [27] uses the 1996 DHS data to predict the prevalence of stunting in children between the ages of two and four years for separate regions of Peru. The study considers access to quality diet, water and sanitation, access to health services, mother’s education and practice of hygiene as predictors. It finds access to sanitation and mother’s education as significant predictors of stunting in most regions. Marini and Gragnolaty [28] use the 2000 DHS data to study
the nonlinear effect of altitude on child growth (measured by height-for-age z-score) among the children under five years. The study finds a negative relationship between child growth and altitude upto 3500 meters, above which the relationship turns positive. The study controls for age subgroups, mother’s height and education and a host of demographic covariates along with access to sanitation and other services. Among the covariates, age subgroup, mother’s height and education as well as access to sanitation are found to be statistically significant. Similarly, Ravina and Chavez [29], uses the four cycles of DHS data from 1992, 1996, 2000 and 2004 to estimate child growth (z-score) with a series of linear models. In addition to the typical variables considered in previous studies, it considers breastfeeding and fixed assets of households. The study finds age, breastfeeding, episodes of diarrhea and access to sanitation as statistically significant contributors to child growth. Arocena [30] uses the 2008 DHS data to estimate a series of logistic regression for the prevalence of stunting in children less than five years. Duration of breastfeeding, child’s birth weight and the type of housing floor are extra variables that are considered along with the typical socio-demographic variables. This study also finds mother’s height and education as well as the type of floor and economic status of the household as statistically significant predictors of stunting. Finally, Gutierrez [31] uses the 2011 DHS data to estimate the prevalence of stunting for children less than five years using almost all the variables used in previous studies along with the presence of at least two children in the household and the order of child birth. This study also finds altitude (above 2500 meters), and mother’s education statistically significant, along with the order of birth (being the third child or a successive child increases the risk of stunting).
The above studies have either used the DHS data for a single year or used the data during a period in which the stunting rates have been fairly stable in Peru. As mentioned earlier, stunting rates in Peru started to decline in 2009 (See Figure 4). An important empirical question is whether such decline could be b attributed to the implementation of the Articulated Nutrition Program (ANP) program in 2008. To answer this question, our study uses the most current data based on the updated WHO child growth curves. Unlike the previous studies, we focus on the children between two and five years for whom the stunted designation is more reliable and may be irreversible. Doing so also avoids the problem of nonlinearity between age and growth outcomes.
DATA AND METHODOLOGYA particular adaptation of the UNICEF conceptual framework
to the Peruvian context is the Tuft University framework [32], which is focused on stunting and specifies the immediate, underlying and basic causes as individual, household and community causes, respectively. This framework was the foundation for the ANP, part of the Budget for Results policy that has been implemented in Peru since 2007 to reduce the prevalence of stunting in children in Peru [13,17,33]. We use variables from this framework to estimate the effects of individual, household and community factors on the probability of being stunted for the
38
30 29 29 2824 23
20 19
16 14 1410 11
46
40 39 3732
0
10
20
30
40
50
60
1990 2000 2005 2007 2008 2009 2010 2011 2012
National Urban Rural
Figure 4 Estimated Prevalence (%) of children under-five years of age affected by stunting (moderate or severe) in Peru for the period 1990-2012.Note: The information is only available at national level for the whole period 1990-2012, but for urban and rural areas only since the year of 2007 when the sample of Demographic Health Survey in Peru was expanded in order to obtain significant estimations for urban and rural areas [15].

Central
Safaei et al. (2016)Email:
Ann Public Health Res 3(4): 1047 (2016) 4/7
children aged 24 – 59 months using a logistic multiple regression model.
Data
The data used for the analysis in this study is taken from the Peruvian Demographic and Health Survey (DHS). The data has been pooled from the consecutive years 2009, 2010, 2011 and 2012. The DHS data includes information on community and household characteristics as well as on nutrition and health of women aged 15-49 and their children under five years old at the time of the survey. The DHS samples cover all Peruvian regions, and include both urban and rural areas. All women registered as living in the households have been interviewed.
The complete DHS database contains basic information for 38, 766 Peruvian children under five years old (from 0 to 59 months), in 30, 446 households and in 2, 259 clusters or Primary Sampling Units. The information is about children (provided by the mothers), their household and their area of residence. In this study, we use only the data for children aged 25 – 59 month old for the reason stated above. The number of children aged 25 to 59 months is 23, 277 in 20, 860 households and 2, 245 clusters. However, there is a high proportion (about 75%) of missing data for certain variables (e.g. vaccination), reducing the number of observations used for estimation to 5,154.
A summary of sample data and variables used in our analysis is given in Tables (1) and (2). Table (1) includes the data for variables related to the individuals and households. The data and variables reported in Table 2 are for the community.
A child is considered stunted if her/his weigh-for-age z-score is less than -2. The presence or absence of a disease is for the last two weeks before the interview. The wealth index or quintile is calculated by the DHS Program based on a composite measure of a household’s ownership of selected assets such as television and bicycles, materials used for housing construction and types of water access and sanitation facilities [34].
Modeling Approach
We consider a multivariate binary logistic regression in which individual, households and community effects are explicitly modeled.
The Dependent Variable: The dependent variable, stunting status, is a binary variable taking the value of 1 (If the child is stunted) and 0 (If the child is not stunted). Stunting status is determined with respect to the updated International Growth Reference Curves [35].
The Independent variables: The selection of the independent variables or covariates is guided by the conceptual framework regarding the determinants at individual, household and community levels. Unfortunately, not all of the determinants are available in the survey, especially those at the community level as related to vaccination. The variables included at the individual level are age (in months), gender, birth cohort, weight at birth (if below 2.5 kg), and (poor) health status as indicated by the presence of acute respiratory infection and acute diarrheal disease. The birth cohort is used to capture the potential effect on stunting of the ANP program implemented in 2008, if any.
Table 1:.Summary of Sample Data – Individual and Household Variables.
Variables
Stunting Status Stunted Not Stunted Total
5,722 17,043 22, 765
Gender Male Female
11,743 11,534 23,277
Birth Weight Low (< 2.5 kg) Normal
1478 17,491 18,969
Diarrhial Disease Infected Not Infected
1643 12,077 13,720Acute Respiratory
Disease Infected Not Infected
1643 12,077 13,720
Mother’s Education Secondary or Higher Otherwise
12,923 9,126 22,049
Age Cohorts 2006 2007 2008 2009 2010
4,748 5,324 5,153 3,056 1,045 18,529Wealth Quintile
Poor-est Poor Middle Richer Richest
7,408 6,158 4,810 3,147 1,754 23,277Note: The total numbers are different for various categories due to missing data.
Table 2: Summary of Sample Data – Community Variables.
Variables
Health Services No Access With Access Total
Delivery Services 3,592 13,528 17,120
Antenatal Care 2,764 12,850 15,614
Growth Contol 16,410 4,742 21,152
Vaccination 4,407 2,276 6,683Water and Sanitation
Services No Access With Access
Piped Water 7,461 15,186 22,647
Improved Sanitation 13,457 9,820 23,277
Treated Water 6,353 16,924 23,277Geographical
VariablesArea of Residence Rural Urban
10,670 12,607 23,277
Place of Residece Metropoli-tan Lima
Rest of Coast
Andes Area
Jungle Area
1,544 5,509 9,677 6,547 23,277Note: The total numbers are different for various categories due to missing data.
At the household level, the independent variables included are wealth index (indicated by wealth quintile with the poorest quintile considered as reference) and the mother’s education (with no education or primary education considered as reference).
Lastly, the independent variables at the community level

Central
Safaei et al. (2016)Email:
Ann Public Health Res 3(4): 1047 (2016) 5/7
include availability of water and sanitary services (as indicated by access to piped water inside, access to improved sanitation, and access to treated water), availability of health services (as indicated by access to delivery, growth control, vaccination, and antenatal services), place of residence (with urban as reference), and geographical region (categorized as Rest of the Coast, Mountain Range, Jungle, and Metropolitan Lima which is used as the reference).
RESULTSUsing the statistical software STATA 12, we estimated a
logistic model for the stunting status of the Peruvian children that belonged to the age group 25 – 59 months. The estimation results are provided in Table (3). The table shows the estimated Odds Ratios along with their 95% confidence intervals for each of the three groups of variables. The estimated coefficients that are statistically significant at 5% are flagged by “**” symbol.
DISCUSSION Among the individual variables, being female and
underweight are statistically significant. As per standard analysis, Odds Ratio less than one indicate lower chances, and those more than one indicate higher chances of being stunted compared to the reference (base) categories. We find that female children are less likely to be stunted compared to males. This finding is consistent with the results of a previous work in Peru [29]. As well, we find that children with low birth weight (less than 2.5 kg) are more than twice as likely to be stunted compared to those with normal weights. Such finding reinforces those obtained by other researchers [18,19,21]. Also, the two dummy variables capturing the cohort effects of 2006 and 2007 are statistically significant. The cohort variables were included to capture the effects of the APN program on children growth implemented in 2008. Our interpretation is that APN appears to have favored the younger cohorts (2009 and 2010) since the older cohorts (2006 and 2007) are found to have higher likelihood of being stunted compared to the reference cohort of 2008. One could argue that the children born before 2008 have not had the chance to benefit from the ANP program during the critical first two years of their lives.
The household variables of wealth index and mother’s education are all statistically significant. The Odds Ratios for the wealth indices are all less than one, indicating that households with higher wealth are less likely to have stunted children compared to the poor households. What is most noticeable here is the “wealth gradient” for the odds of being stunted. As the wealth index (quintile) goes up, the odds of being stunted diminishes consistently. So much so that the odds of being stunted for a child who belongs to the richest family is only one tenth of that for a child in a poor family. Such result is comparable to findings in Bangladesh [36] and Cambodia [37], for example. The other important variable at this level is the mother’s education. As Table shows, children whose mothers are more educated are almost 50% less likely to be stunted compared to those whose mothers have no education or only primary education. Again, this finding is consistent with the results from a previous study in Peru [28] and another study on a large group of countries [38].
Table 3: Estimated Odds Ratios of Being Stunted for Children 25 – 59 Months.
Odds Ratios 95% Confidence Interval
Individual Variables:
Age (in months) 0.9887 [0.9642, 1.0139]
Gender (Female) 0.7309** [0.6278, 0.8509]
Birth Cohort (base: 2008)
Cohort 2006 1.3525** [1.0446, 1.7509]
Cohort 2007 1.2656** [1.0439, 1.5345]
Cohort 2009 0.7584 [0.7246, 1.2083]
Cohort 2010 0.9390 [0.7459, 1.1821]
Weight at birth (Underweight) 2.2230** [1.7421, 2.8366]
Health Status
Acute Respiratory Infection 1.0153 [0.8298, 1.2423]
Acute Diarrheal Disease 1.2403 [1.0125, 1.5194]
Household Variables:
Wealth Index (base: poorest quintile)
Second Quintile 0.7482** [0.6089, 0.9194]
Middle Quintile 0.3858** [0.2885, 0.5159]
Fourth Quintile 0.2249** [0.1499, 0.3374]
Richest Quintile 0.1069** [0.0552, 0.2068]
Mother’s Education (base: no or primary education) 0.4960** [0.4177, 0.5890]
Community Variables:
Water and sanitation Services
No access to piped water inside 1.1673 [0.9785, 1.3925]
No access to improved sanitation 0.9692 [0.8052, 1.1666]
No access to treated water 0.9913 [0.8254, 1.1905]
Health Services
No access to delivery services 1.7050** [1.3982, 2.0790]
No access to growth control 0.9820 [0.7606, 1.2678]
No access to vaccination 0.8592 [0.7267, 1.0158]
No access to antenatal care 0.8677 [0.7144, 1.0540]
Place of Residence (rural) 0.8922 [0.7252, 1.0978]
Geographical Region (base: Metro Lima)
Rest of the Coast 0.9044 [0.5667, 1.4433]
Mountain range (Andes) 2.2692** [1.4362, 3.5853]
Jungle 1.3946 [0.8750, 2.2228]
Constant 0.6412 [0.0122, 1.2701]
Number of Observations:
Children 5,154
Households 5,104
Communities (Clusters) 1899

Central
Safaei et al. (2016)Email:
Ann Public Health Res 3(4): 1047 (2016) 6/7
Only two of the community variables are statistically significant: access to delivery services (among the sanitation and health services variables), and living in the mountains or the Andes areas (among the geographical variables). The lack of access to delivery services increases the chances of children being stunted by 70%. Children living in mountainous areas of Peru are more than double as likely to be stunted compared to those living in metropolitan Lima, the capital. Other studies have found similar results for Peru [28, 30].
We would like to point out some of the shortcomings of the present study and hint at possible remedies for future studies. A typical problem with cross-sectional studies such as ours is that it misses the dynamics of chronic under-nutrition or stunting for specific cohorts as they are not followed up in successive cycles of surveys. With the availability of longitudinal surveys this problem can be avoided. Also, there is a possibility of some overlap between the variables access to water and wealth index since the latter includes the former as a constituent part. Finally, re-estimating the model for the entire group of children under five would make the results of our study more comparable to others, although we wanted to make a distinction between stunting and being stunted.
CONCLUSIONStunting is still a global public health problem throughout
the developing world whose burden is inequitably borne by the poor and low income families. Our findings for Peru identify a number of factors at individual, household and community levels that have significant bearing on the chances of stunting among children aged 25 – 59 months. Of the variables that are responsive to policy, access to delivery care, antenatal care as related to low birth weight, mother’s education, the household economic wellbeing are key variables that governments and other organizations must target. The APN is a welcome policy initiative on the part of the Peruvian government, but its reach and effectiveness needs more evaluation.
ACKNOWLEDGEMENTSWe would like to thank two anonymous referees for their
valuable comments for improving the quality of this paper.
REFERENCES1. Black R, Allen L, Bhutta Z, Caulfield L, de Onis M, Ezzati M, et al.
Maternal and child undernutrition: global and regional exposures and health consequences. Lancet. 2008; 371: 243-260.
2. Bhutta ZA, Das J, Rizvi A, Gaffey M, Walker N, Horton S, et al. Evidence based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 2013; 382: 452-477.
3. Crookston B, Dearden K, Alder S, Porucznik C, Stanford J, Merrill R, et al. Impact of Early and Concurrent Stunting on Cognition. Matern Child Nutr. 2011; 7: 397-409.
4. Save the Children. Food for Thought: Tackling Child Malnutrition to Unlock Potential and Boost Prosperity. London: The Save the Children Fund. 2013.
5. United Nations. Millennium Project. 2002-2006.
6. WHO. Comprehensive implementation plan of maternal infant and young child nutrition. Sixty-fifth World Health Assembly, WHA
resolution 65.6 and Annex 2, Geneva. 2014.
7. UNICE. Strategy to reduce maternal and child undernutrition. Bangkok: UNICEF - East Asia and Pacific Regional Office. 2003.
8. Wright CM, Garcia AL. Child undernutrition in affluent societies: what are we talking about? Proc Nutr Soc. 2012; 71: 545-555.
9. Reinhardt K, Fanzo J. Addressing chronic malnutrition through multi-sectoral, sustainable approaches: a review of the causes and consequences. Front Nutr. 2014; 1: 1-11.
10. UNICEF. Improving child nutrition. The achievable imperative for global progress. New York: United Nations. 2013.
11. Bergeron G, Castleman T. Program Responses to Acute and Chronic Malnutrition: Divergences and Convergences. American Society for Nutrition. 2012; 34: 242-243.
12. Joint Child Malnutrition Estimates (UNICEF/WHO/World Bank)
13. MIDIS. Desnutrición Crónica Infantil: Metas al 2016.
14. INEI. InstitutoNacional de Estadística del Perú. 2014.
15. INEI. InstitutoNacional de Estadística del PerúPerú: EncuestaDe-mográfica y de Salud Familiar 2013. Lima: INEI, 2014.
16. MMPV. Plan Nacional de Acciónpor la Infancia y la Adolescencia 2012-2021. Lima: MIMP. 2012.
17. MEF. ProgramaArticuladoNutricional. Lima: CooperaciónAlemana (GIZ). 2011.
18. UNICEF. Strategy for improved nutrition of children and women in developing countries. New York, N.Y., USA: UNICEF. 1990.
19. Chopra M. Risk factors for under nutrition of young children in a rural area of South Africa. Public Health Nutr. 2002; 6: 645-652.
20. Kabubo-Mariara J, Ndenge G, Mwabu D. Determinants of Children’s Nutritional Status in Kenya: Evidence from Demographic and Health Surveys. J Afr Econ. 2008; 18: 363-387.
21. Kandala N-B, Mandungu T, Emina JB, Nzita KP, Cappucio FP. Malnutrition among children under the age of five in the Democratic Republic of Congo (DRC): does geographic location matter? BMC Public Health. 2011; 11.
22. Mazumdar, S. Assessing Vulnerability to Chronic Undernutrition among Under-Five Children in Egypt: Contextual Determinants of and Individual Consequence. Int J Popul Res. 2012.
23. Fenske N, Burns J, Hothorn T, Rehfuess EA. Understanding Child Stunting in India: A Comprehensive Analysis of Socio-Economic, Nutritional and Environmental Determinants Using Additive Quintile Regression. PLoS ONE. 2013; 8: 78692.
24. Gragnolati, M. Children’s Growth and Poverty in Rural Guatemala. World Bank Policy Research Working Paper no 2193. September 1999.
25. World Bank. Nutritional Failure in Ecuador: Causes, Consequences and Solutions. Washington, DC: World Bank. 2007.
26. Monteiro C, D’Aquino M, Lisboa W, Konno S, Lovadino A, Barros A, et al. Narrowing Socioeconomic Inequality in Child Stunting: The Brazilian Experience, 1974-2007. Bulletin World Health Organization. 2010; 88: 305-311.
27. Lescano A. Modelopara el Análisis de Políticas de Intervención en Desnutrición. Lima: INEI. 2002.
28. Marini A, Gragnolati M. Nonlinear Effects of Altitude on Child Growth In Peru - A multilevel Analysis. World Bank Policy Research Working Paper 3823, January 2006.

Central
Safaei et al. (2016)Email:
Ann Public Health Res 3(4): 1047 (2016) 7/7
Vizcarra CB, Safaei J (2016) Stunting in Peruvian Children: an Empirical Analysis. Ann Public Health Res 3(4): 1047.
Cite this article
29. Ravina R, Chávez JC. Análisis de los factoresSubyacentesAsociados a la DesnutriciónCrónicaInfantil. Lima: InstitutoNacional de Estadística e Informática. 2007.
30. Arocena V. Factoresasociados a la desnutricióncrónicainfantil en Perú: unaaplicación de modelosmultinivel. RevistaLatinoamericana de Población. 2010; 3: 41-56.
31. Gutiérrez C, Cunha A, Dávila M, Alarcón J, Sobino, M. Desnutricióninfantil en menores de cincoaños en Perú: tendencias y factoresdeterminantes. Rev PanamSaludPublica. 2014; 35, 104-112.
32. Medford MA. Reducción de la DesnutriciónCrónica en el Perú: PropuestaparaunaEstrategia Nacional. Tufts University and United States Agency for International Development. 2001.
33. Cruzado V. Análisis del impacto del programapresupuestalArticulado Nutritional sobre la desnutricióncrónica en ninosmenores de 5 años. Lima: Ministerio de Economia y Finanzas. 2012.
34. DHS Program. Wealth Index. Retrieved from the Demographic and Health Surveys: (15 de 02 de 2015).
35. WHO Multicentre Group Reference Study. WHO Child Growth Standards based on length/height, weight and age. ActaPaedriatica. 2006; 450: 76-85.
36. Hong R, Banta JE, Betancourt JA. Relationship between household wealth inequality and chronic childhood under-nutrition in Bangladesh. Int J Equity Health. 2006; 5: 1-10.
37. Hong R, Mishra V. Effect of wealth inequality on chronic under-nutrition in Cambodian children. J Health PopulNutr. 2006; 24: 89-99.
38. Smith L, Haddad L. Reducing Child Undernutrition: Past Drivers and Priorities for the Post-MDG Era. Institute of Development Studies. 2014; 1-47.