Embed Size (px)
Citation preview

Chapter FourteePz
Anewvsmal S;tzbarachnoid
Harold l? Adams, JK and Patricia H. Davis
Subarachnoid hemorrhage (SAH) accounts for 5% to 10% of all strokes and, unlike most other types of stroke, has not declined in incidence during the last 30 years. The leading cause of SAH, accounting for approximately 80% of cases, is rupture of an intracranial saccular aneurysm. This dlstinction is important, because patients with bleed- ing secondary to ruptured saccular aneurysms have a poorer prognosis and present more complicated manage- ment problems than patients with SAH of other causes.
Outcomes among patients who do not have aneurysms are also better. Such patients, including those with a peri- mesencephalic pattern of bleeding found on computed tomography (CT), often are not seriously ill and unconi- monly ex erience either rebleedmg or delayed cerebral ischemia. ' As a result, the treatment of patients with non- aneurysmal SAH differs from that of patients with aneurysmal SAH. We restrict discussion in this chapter to management of patients with aneurysmal SAH and emphasize medical measures to treat these seriously affected patients.
Despite early diagnosis and better medical and surgical treatment that probably are reducing the mortality, SAH remains a common cause of death and disability. The 30- day mortality rate of SAH approaches 50%. Most deaths occur within 1 week of the ictus; 10% of patients die before reachin medical attention, and 25% dle within 24 hours.%' Causes of sudden death include a large intra- parenchymal hematoma, destruction of brain tissue, acute hydrocephalus, increased intracranial pressure, myocardial ischemia, cardiac arrhythmias, pulmonary edema, and res- piratory failure. These critically ill patients, who are mori- bund, often have ataxic or periodic respirations, suggesting brainstem failure. In these cases, CT usually shows massive intracerebral, intraventricular, or subarachnoid hemor- rhage. Survival in these instances is unlikely even with prompt and aggressive medical care.
Even if terminally ill patients are excluded from consid- eration, the natural history of SAH is grim. The 3-month mortality rate among patients who reach a major medical center is approximately 25%.fi The leading causes of death are sequelae of the initial hemorrhage, recurrent aneurys- mal rupture, and vasospasm leading to ischemic stroke. In addition, severe medical complications may add
K
significantly to mortality rates after SAH.' Another 20% to 40% of hospitalized patients have major neurologic impair- ments."" Because SAH affects a relatively young group of otherwise healthy patients, the economic and social effects of the disease are great." The chief reasons for neurologic residual effects are the consequences of the initial rupture, vasospasm and ischemia, recurrent hemorrhage, hydro- cephalus, complications of surgery, and complications of medical inanagement.I2 Sequelae include cranial nerve palsies, paralysis, aphasia, cognitive impairments, behav- ioral disorders, and psychiatric disturbances that could hamper return to gainful employment or independence. Nevertheless, improvements in care are leadin to reduc- tions in mortality and disability after SAH.11.13,1K
The two most important factors that influence progno- sis after SAH are the interval from the ictus and the person's level of consciousness.1" Most deaths and compli- cations occur within 2 weeks of SAH; patients surviving this period without major complications generally have a favorable prognosis. When examining the possible useful- ness of any intervention, one should consider the interval from the onset of SAH to initiation of treatment. The key test of any medlcal or surgical therapy is whether it improves outcome among acutely ill patients treated within the first few days after SAH. The admitting level of consciousness is the most predictive clinical factor (Table 14.1). In one study, the 6-month mortality rate among comatose patients was 71%, whereas only 11% of initially alert patients died during the same period.lS
The size of the aneurysm was a major determinant of prognosis in one study,lfi but not in another study.' Although data conflict, aneurysms located on the basilar artery or its branches appear to be associated with a poorer prognosis."," Patients older than 65 years have a poorer prognosis than younger patient^.'".'^ Favorable outcomes are less common among women than among men.g.'* Fever, presumably of central origin, occurs commonly with SAH, and patients with fever often have poor outcomes.'Y Preexisting medical conditions, such as hypertension and diabetes mellitus, do not have major effects on prognosis. In one study, smoking had a protective effect on mor- tality"; the reason for this effect is not clear, and the
% b n
377

378 Stroke: Patbopbysiology, Diagnosis, and Management
Table 14.1 after Subarachnoid Hemorrhage
Pactors Predicting Less Favorable Outcome Table 14.2 Complications of Aneurysmal Subarachnoid Hemorrhage
Clinical Admitting level of consciousness (coma) factors Interval from subarachnoid hemorrhage
(<3 days) Age (>65 years) Prior unrecognized hemorrhage or warning leak Presence of focal neurologic signs on admission Presence of severe comorbid disease or
extraneural organ involvement Diagnostic Hyponatremia or hypovolemia
test results Abnormal CT scan Local, thick, or diffuse collection of
Intracerebral or intraventricular blood subarachnoid blood
Mass effect Hydrocephalus Evidence of rebleeding detected by sequential
CT scans Vasospasm detected by arteriography or by
transcranial Doppler ultrasonography Aneurysm located on anterior cerebral or
vertebrobasilar arteries Size of aneurysm (2lOmm)
Neurologic (intraparenchymal hematoma) Intraventricular hemorrhage Brain edema Hydrocephalus (acute, subacute, chronic) Recurrent hemorrhage Vasospasm-induced ischemic stroke Seizures Systemic
Arterial hypotension or hypertension Electrolyte disturbances (hyponatremia, hypernatremia,
Cardiac (myocardial infarction, arrhythmia, congestive heart hypokalemia)
failure)
distress syndrome, atelectasis, pneumonia) Pulmonary (neurogenic pulmonary edema, adult respiratory
Gastrointestinal bleeding Sepsis Renal or hepatic dysfunction Venous thromboembolisin Bleeding disorders, including throinbocytopenia
observation needs further study. Patients who do not reach medical attention until after a second rupture of the aneurysm have a worse prognosis than patients who have a single hemorrhage.6 Evidence of extracerebral organ dysfunction and acute systemic inflammatory response syndrome also predict higher mortality and morbidity in patients with SAH.20,21
The results of the initial CT examination also provide prognostic clues (see Table 14.1).10,15 In general, CT and clinical findings are parallel and correlate with the time lag from SAH.lS Patients with CT evidence of hydrocephalus, mass effect, intracerebral hematoma, intraventricular evidence, or diffuse subarachnoid blood have a poorer prognosis than those with normal CT findings or a minimal amount of subarachnoid blood. Early elevations in thrombin-antithrombin 111 complex, plasmin ct-plasmin inhibitor complex, and D dimer are more common amon
Mack and colleagues23 noted that elevations of serum intercellular adhesion molecule-1 (ICAM-1) levels were associated with poorer outcomes after SAH.
The complications of SAH that can lead to death or dis- ability are summarized in Table 14.2. Neurologic injuries secondary to a number of complications lead to greater morbidity or mortality from SAH, especially among the most seriously ill patients.24 Because rebleeding and ischemic complications from cerebral vasospasm account for approximately 60% of unfavorable outcomes, consid- erable attention is directed toward their prevention or treatment. Still, approximately one third of patients who die or are disabled from SAH are injured rimarily by the consequences of the initial hem0rrhage.R' The goals of medical management are (1) to stabilize an acutely ill patient and to prevent early complications, (2) to forestall recurrent hemorrhage, and (3) to avoid the ischemic com- plications of vasospasm. Treatment is multifactorial and
patients with severe hemorrhages and poor outcomes. f2
complex; therapies aimed at prevention of one complica- tion might interfere with management of another com- plication. In addition, successful treatment of one complication can leave the patient at risk for another. For example, prevention of early rebleeding means that cere- bral ischemia from vasospasm might develop. Consider- able research has focused on individual components of management. Still, much of the treatment of SAH is empirical or is based on anecdotal evidence; several com- ponents of care have not been tested in clinical trials. Thus, some recommendations for management are based on weak or conflicting scientific evidence. In the future, con- siderable research will focus on refining the utility of several elements of acute management after SAH.
DIAGNOSIS The key to successful management of SAH is early treat- ment, which, in turn, is based on prompt recognition and accurate diagnosk6 The drive to popularize the concept of stroke as a "brain attack is stimulated, in part, by the successful early treatment of patients with ruptured aneurysms.25 Therapies of proven utility are available, and the goal is to offer these interventions to patients with SAH, who are acutely ill. Approximately 10% of patients or their families do not recognize the serious nature of the symptoms and do not seek medical attention quickly. More disconcerting is that physicians initially dia nose disorders other than SAH in 25% to 50% of cases?"' Such misdi- agnoses can delay treatment for day^.^'-^' Even more both- ersome is that the chance of misdiagnosis is greatest among the least seriously ill patients-who are most likely to be helped by early medical or surgical interventions.
ACUTE MANAGEMENT The patient with recent SAH is critically ill and should be evaluated and treated ~ rgen t ly .~ ' .~~ He or she should be

Chapter 14: Aneurysmal Subarachnoid HemorrhaBe 379
transported rapidly to a medical center that has the expert- ise to treat a patient with a ruptured aneurysm. Acute, potentially life-threatening complications should be anticipated (see Table 14.2). Personnel should assess the patient quickly and should measure vital signs and assess neurologic status frequently. The heart rate and rhythm should be monitored. The airway, breathing, and circula- tion should be supported, and if necessary, supplemental oxygen, endotracheal intubation, or ventilatory assistance should be given.31 Intravenous access is established to expedte emergency administration of medications. Normal saline can be given at a slow rate to maintain patency of the intravenous line. Unfortunately, the urgent approach to acute management of SAH is often suboptimal in emer- gency departments.32 Each institution should develop a protocol for the management of SAH in the emergency department, includmg plans for both acute treatment and urgent evaluation.
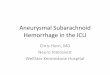
The initial evaluation should include CT scan, chest radiograph, electrocardiogram, and blood studies (Table 14.3). CT can demonstrate subarachnoid blood and a number of other acute intracranial complications (Table 14.4 and Fig. 14-1). When CT shows intracranial bleed- ing, a lumbar puncture can be avoided. The findings of CT that is performed within 24 hours after onset of symptoms with the use of third-generation scanners are normal in approximately 2% to 7% of cases." If the CT findings are normal, a cerebrospinal fluid (CSF) specimen should be obtained.
Magnetic resonance imaging (MRI) may not be as sen- sitive as CT in detecting subarachnoid blood in the acute setting but may be more sensitive than CT in patients pre- senting in the subacute phase. The most sensitive MRI sequences for detecting SAH are gradient-echo T2 images
Table 14.3 Initial Diagnostic Evaluation of a Patient with a Suspected Subarachnoid Hemorrhage
Laboratory tests Complete blood count and platelet count International Normalized Ratio, activated partial
Serum electrolytes, glucose, calcium Blood urea nitrogen and serum creatinine Urinalysis Electrocardiogram
Imaging studies Non-contrast-enhanced cranial CT Chest radiograph Cerebral angiogram (4-vessel)
thromboplastin time
Cerebrospinal fluid exam (if CT results are negative) Optional tests
CT angiography Cervical spine radiography (if patient is comatose with a
MRI of brain or cervical spine (if angiogram results are
Arterial blood gas measurements Liver function tests Electroencephalogram Cerebral blood flow study Transcranial Doppler ultrasonography
possible spine injury)
negative)
Table 14.4 Abnormalities Found by Unenhanced Cranial CT in Patients with Recent Subarachnoid Hemorrhage
Abnormality YO
Subarachnoid blood 93-98 (<24 hours) Focal, thin collection Focal, thick collection Diffuse, thin collection Diffuse, thick collection
Intraventricular blood 15-20 Intraparenchymal blood 15-20 Subdural blood 1-2 Hydrocephalus
Ischemic lesion 1-2 Aneurysm 5
k 10-20 3 0
Mass effect 5-8 q 2 3 ;. 3. k 2
w 0
followed by fluid attenuation inversion recovery (FLAIR) images (Fig. 14-2).33 Once the diagnosis of SAH is confirmed, arteriography is needed to demonstrate the presence and location of the aneurysm (Fig. lM)." Both carotid circulations and the entire vertebrobasilar system should be examined, although the sequence of the arterial studies is influenced by the findmgs on CT.
Magnetic resonance angiography can be used to screen for larger aneurysms, but it is probably not as effective as arteriography in the evaluation of patients with SAH. CT angiography is becoming a useful alternative to conven- tional arteriography to detect aneurysms%.% and in some cases may detect aneurysms missed by angiography.3fi A potential advantage of CT angiography is its ability to demonstrate the topographic anatomy of the cerebral aneurysms and surrounding structure^.^' If results of the first arteriographic study are normal, a second study is usually performed approximately 10 to 14 days after SAH among patients whose bleeding is not in a perimesen- cephalic pattern. The second arteriogram obtained 1 week later can detect an aneurysm in an additional 1% to 2% of patients.
Patients should be admitted to a unit that has monitor- ing equipment and is staffed by neurologically trained nurses. Acute care can be divided into general supportive efforts and therapies aimed at preventing or controlling specific complications (Table 14.5).30,31 For the first 24 hours, blood pressure, vital signs, and neurologic status should be assessed hourly. Thereafter, examinations can be spaced further apart in stable patients. Cardiac monitoring and, if necessary, continuous intra-arterial or noninvasive blood pressure monitoring are extended for at least 24 to 48 hours after admission.
Forced bed rest is a traditional part of management. Visitors and external stimuli are restricted. Passive range- of-motion exercises and frequent turning are performed. A water mattress or an alternating-pressure pneumatic bed can reduce the risk of pressure sores and atelectasis. Patients are assisted with self-care activities, such as bathing and eating. Black and associates3' showed that external pneumatic calf compression stockings and devices reduce the incidence of deep vein thrombosis. The use of heparin as a prophylaxis against deep venous thrombosis is generally avoided until the ruptured aneurysm is treated.

A 6
FIGURE 14-1 Two CT scans obtaiiterl ripproxiitmtely 4 hours upurt in a patient icho hud ri recurrent heinorrhnge A, Stibarachiroitl blood can be seen in inter~ieinisphericfissure and basal cisterns. The patient’s condition suddenly deteriorated. B, The second sttidy shows additional subarachnoid blood and intraoentriculrir heinorrhage. Hydrocephalus (enlargement of the teniporal horns) is cilso present.
FIGURE 14-2 T1-weighted MRI scan deinonstrates a large aneurysm (arrow) arising from the right internal carotid artery
FIGURE 14-3 Left lateral carotid arteriogrclni obtained with the use of subtraction technique s h o ~ s an rinewtystn of the inter- nal carotid artery (arrow) in the region of the carotid siphit.

Chapter 14: Aneurysmal Subarachnoid HemorrhaBe 38 1
Table 14.5 Medical Management of Persons with Aneurysmal Subarachnoid Hemorrhage
Emergency treatment Support airway Supplemental oxygen Ventilatory assistance Intravenous access-normal saline
Close observation Other immediate treatment
Cardiac monitoring Arterial pressure monitoring
Passive/active range of movement Watedalternating-pressure mattress Assistance with self-care Gentle pulmonary toilet Avoidance of indwelling bladder catheter, if possible Pneumatic compression stockings
Bed rest
Intravenous saline with multiple vitamins-2.5-3.5 L per day Stool softeners Stress ulcer prophylaxis Diet-soft, high-fiber if patient is alert; nasogastric feeding if
patient is obtunded Symptomatic treatment
acetaminophen
promethazine, trimethobenzamide, ondansetron
Pain or discomfort-odeine, meperidine, morphine,
Nausea and vomiting-prochlorperazine,
Seizures-anticonvulsants Cardiac arrhythmias-correct electrolytes, P-blocker, calcium
channel blocker Arterial hypertension
Moderate-labetalol, enalaprilat, hydralazine Severe-nicardipine, esmolol, nitropmsside, fenoldopam
Hyponatremia-isotonic or hypertonic fluids, fludrocortisone, no diuretics, fluid restriction only if patient is euvolemic or hypervolemic
Elevate head of bed Intracranial pressure monitoring Correct metabolic disturbances Hyperventilation Mannitol, furosemide, hypertonic saline Cerebrospinal fluid drainage-multiple lumbar punctures
or intraventricular catheter placement Surgical decompression
Aminocaproic acidhanexamic acid Secure aneurysm-surgical clipping or endovascular
Increased intracranial pressure
Rebleeding
obliteration Neurogenic pulmonary edema
Dobutamine Positive end-expiratory pressure, gentle diuresis
Gentle pulmonary suctioning and nursing care are impor- tant for avoiding pneumonia. The value of absolute bed rest in preventing rebleeding was tested by the Coopera- tive Study of Intracranial Aneurysms and Subarachnoid Hemorrhage; the cumulative rate of rebleeding was 25% during the first 14 days after SAHS3’ In general, the prog- nosis of patients treated only with absolute bed rest now represents the natural history of SAH.
Because intravenously administered medications are often needed, a slow infusion of saline is continued. Alert patients are usually given a soft, high-fiber diet
supplemented by stool s0ftene1-s.~~ Caffeinated beverages are avoided. Stuporous and comatose patients are not fed during the acute treatment period. If a seriously ill person is stable several days after SAH and the airway is secured, nasogastric feedings can be instituted.
SYMPTOMATIC TREATMENT Patients with SAH are often confused or agitated as a result of brain injury, hydrocephalus, or increased intracra- nial pressure. Pain or nausea can also lead to irritability. Agitation raises the risk of rebleeding and aggravates increased intracranial pressure. Control of pain or nausea can calm an upset patient. Regular administration of diazepam or phenobarbital may be useful in providing sedation for agitated patients.
The headache of SAH is intense, and patients should receive ample doses of analgesic^.^'^^^ Most alert patients require a medication such as codeine, meperidine, or morphine. The agent is usually administered parenterally. These medications can be combined with acetaminophen, hydroxyzine hydrochloride, or promethazine. Some patients have photophobia and phonophobia; a quiet, dark environment can help relieve some of these conditions, which otherwise might worsen the head pain. Sedation and sleep might also help control pain. Aspirin affects platelet aggregation and prolongs the bleeding time; there is concern that aspirin might potentiate rebleeding.
Severe nausea and vomiting are common and important complaints, particularly during the first 24 hours after SAH. Nauseated patients should receive an antiemetic, such as ondansetron, trimethobenzamide, or prochlorper- azine, to control these complaints.
ANTICONVULSANTS Approximately 25% of patients have seizures, most of which occur within the first 24 Rhoney and col- l e a g u e ~ ~ ~ reported that seizures were most common among patients with thick cisternal clots. Most seizures happen before the patient reaches the hospital.41 Hart and associ- a t e ~ ~ ’ noted that 63% of the seizures happened at the time of aneurysmal rupture. However, some of these “seizures” may not be truly epileptic phenomena but may represent transient decerebrate osturing secondary to increased intracranial pressure?’,’ There is no correlation between epileptic seizures at the time of aneurysmal rupture and the risk of rebleeding, early mortality, or major m~rbidi ty .~’ ,~~
Although seizures occurring after hospitalization are uncommon, they can be associated with recurrent hemor- rhage. Physicians prescribe anticonvulsants to patients who have experienced a seizure as part of SAH, but the pro- phylactic use of these agents in treatment of patients who have not had a seizure is controversial. The rationale for prophylactic administration of anticonvulsants is that a seizure is a dangerous event in a person with a recent SAH. Because of the low rate of seizures after admission, however, Hart and associates4’ and Sundaram and Chow4’ question the necessity for routine prescription of anticon- vulsants to patients with recent SAH. However, regular use

382 Stroke: Patbopbysiology, Diagnosis, and Management
of phenytoin or another parenterally administered anti- convulsant is recommended to reduce the likelihood of seizures. No trial has tested the value of anticonvulsants in management of patients with recent SAH. Pending such a trial, the decision to prescribe these medications is individualized. The benefit of prophylaxis against seizures must be weighed against potential adverse reactions, which occurred in 4.1% of patients in one series4’ If a patient has had or is having convulsions, intravenous doses of anti- convulsants are given.
TREATMENT OF MYOCARDIAL ISCHEMIA AND CARDIAC ARRHYTHMIAS Cardiac arrhythmias can be detected in almost all patients during the first few hours after SAH; in approximately 20% of cases, the arrhythmias can be severe or life-threatening (Table 14.6).-’ Ventricular arrhythmias are a potential cause of sudden death after SAH. Di Pasquale and cowork- e r ~ ~ ~ noted torsades de pointes in 3.8% of 132 patients with SAH who underwent Holter monitoring. Machado and colleagues49 correlated the development of torsades de pointes with hypokalemia rather than the direct effects of the SAH. Increased QT dispersion is a common electro- cardiographic finding after SAH.48
Changes resembling those seen in acute myocardial ischemia can be noted in 25% to 80% of patients.*,” In fact, many people with SAH have secondary myocardial ischemia and left ventricular An elevation of the cardiac isoenzyme creatine kinase can be detected. Subendocardial areas of focal ischemic necrosis are found among patients who died of SAH even those without prior history of coronary artery disease. Abnormal left ventricu- lar function is seen most commonly among patients with elevated creatine kinase levels.53 Severe left ventricular dysfunction after SAH may necessitate a delay in aneurysm surgery.” In addition, the reduction of cardiac output after severe SAH might increase the risk of cerebral ischemia secondary to v a s ~ s p a s m . ~ ~
The frequency of electrocardiographic changes can be predicted from (1) the severity of bleeding detected on CT and (2) the patient’s neurologic status. The changes are most common among seriously ill patients with diffuse subarachnoid blood, intraventricular hemorrhage, or a large intracerebral h e m a t ~ m a . ~ ‘ , ~ The presence of a large clot in the right sylvian cistern and fissure is associated with
Table 14.6 Electrocardiographic Abnormalities after Subarachnoid Hemorrhage
Prominent P waves Prolonged/shortened PR interval Broadhnvertedlflattened T waves Prolongedkhortened QT interval Elevatioddepression ST segment Proininenthnverted U waves Pathologic Q waves S in V, and R in Vs combined >35 mm Rhythm disturbances
electrocardiographic changes. Although Brouwers and associatess5 correlated elevated plasma levels of norepi- nephrine with a poor outcome after SAH, they could not find a relationship between norepinephrine and cardiac ischemia. Still, it is assumed that the release of cate- cholamines by the posterior hypothalamus is key to the development of the car&ovascular complications of SAH. Presumably, the markedly elevated levels of norepineph- rine lead to hypokalemia, systemic hypertensive effects, left ventricular strain, coronary artery vasospasm, a “stunned myocardium, or cardiac t o x i ~ i t y . ~ ~ ~ ~ ~ . ~ ‘ Adminis- tration of a P-blocking medication might reduce the number and severity of cardiac s e q ~ e l a e . ~ ~ ~ ~ ~
Further study on the potential value of cardioprotective agents in reducing the cardiac complications of SAH is needed. The risk of cardiac causes of death seems to be low.= There may be a group of patients who are particularly vulnerable to such complications. Pending more definitive data, P-blockers can be given on a case-by-case basis. The first 24 to 48 hours are the period of highest risk for cardiac complications, so there is little reason to start treatment with cardioprotective medications after that time.
Neurogenic pulmonary edema is a rare, but often fatal complication that occurs in critically ill patients. Markedly increased extravascular lung water and an intrapulmonary shunt lead to hypoxia. This complication is frequently ascribed to greater sympathetic activity resulting in acute cardiac changes.31 Treatment is difficult but consists of oxygen and positive-pressure ventilatory assi~tance.~~ Dobutamine (5 to lOpg/kg/hr) increases both the cardiac index and left ventricular stroke work index and decreases the total peripheral vascular resistance, leading to diuresis and a reduction in pulmonary congestion; this agent is now recommended for the treatment of neurogenic pulmonary edema after SAH.31,59
ANTIHYPERTENSIVE TREATMENT Arterial hypertension is common in SAH, resulting from elevations of catecholamines and renin produced by hypo- thalamic disturbances (see Table 14.5).60,61 Additionally, increased intracranial pressure can induce arterial hyper- tension as a means to maintain adequate cerebral perfu- sion pressure. Arterial hypertension also can be secondary to seizures, vomiting, agitation, or pain. In adhtion, the patient may have preexisting hypertension.
Hypertension after SAH has been found to correlate with increases in the risk of vasospasm and rnortality.‘l Arterial hypertension also puts patients at high risk for recurrent hemorrhage. Administration of antihypertensive agents is a traditional component of early medical man- agement of SAH.30,31 However, rapid or steep reductions in blood pressure might be dangerous. Patients with vas- ospasm or increased intracranial pressure may experience a drop in cerebral perfusion in conjunction with a decline in blood pressure; neurologic deterioration can result. Some antihypertensive agents (nitroglycerin, sodium nitro- prusside, fenoldopam) are potent cerebral vasodilators, and enlargement of the cerebrovascular bed secondary to their administration could further increase intracranial pressure.

Chapter 14: Aneurysmal Subarachnoid Hemorrhafle 383
The blood pressure often returns to normal after the patient with SAH is admitted to the hospital or when symp- toms such as headache are treated; thus, aggressive anti- hypertensive therapy might be avoided in some cases. The level of arterial hypertension that mandates treatment is not known. Patients with moderate hypertension (mean arterial blood pressure lower than 120 mm Hg) probably do not need to be treated. On the other hand, patients whose mean blood pressure is 120mmHg or higher or whose systolic blood pressure is higher than 180 mm Hg should receive medication. The goal should be to cautiously lower the blood pressure to levels normal for the patient and to avoid inducing hypotension.
Although alert patients with elevated blood pressures can receive oral medications, parented agents have the advantage of a prompt response. Antihypertensive agents that were used before SAH are usually continued, and they should not be stopped abruptly. Short-acting antihyper- tensive agents are desirable because of the rapid resolu- tion of the unwanted effects of an excessive decline in blood pressure. Because patients are often dehydrated or hyponatremic, diuretics are avoided. P-blockers, calcium channel blockers, and angiotensin-converting enzyme inhibitors are the oral agents most commonly prescribed. Nimodipine or nicardipine may be useful antihypertensive agents in the patient with SAH.
The patient with a markedly elevated or unstable arterial blood pressure reading may require a continuous intravenous infusion of labetalol, sodium nitroprusside, or fenoldopam. The rate of infusion is adjusted in response to blood pressure values. Intravenous infusions of antihy- pertensive agents should be given only if intra-arterial or frequent noninvasive blood pressure monitoring can be achieved. The dosage must be individualized, because a patient may be very sensitive to a medication, and the resulting drop in blood pressure may exceed expectations. Doses required in patients with SAH can be lower than those required for other hypertensive emergencies.
Drug-induced hypotension might help prevent early rebleeding in SAH. This regimen was compared with absolute bed rest in a randomized triale6' Mortality and rebleeding rates were similar in the two groups. Although the study was performed more than 25 years ago and older antihypertensive medications were prescribed, there is no evidence that induced hypotension should be part of the acute management of patients with SAH. The potential for low arterial blood pressure to aggravate the ischemic effects of vasospasm is another reason to avoid vigorous lowering of blood pressure. If a patient does experience ischemic symptoms secondary to vasospasm, antihyper- tensive agents are usually discontinued to help efforts to increase cerebral perfusion pressure.
MANAGEMENT OF ELECTROLYTE AND FLUID BALANCE Disturbances in water and sodium balance occur in approximately one third of patients with SAH.@' These complications are most likely to develop in critically ill patients with large hemorrhages. Hyponatremia and volume depletion correlate with a poor prognosis and the
subsequent development of hydrocephalus, vasospasm, and ischemic stroke.M Severe hyponatremia can cause con- vulsions and is a potential cause of coma.
The primary indication for rapid correction of hypona- tremia is the development of seizures in a patient without neurologic disease; however, this indication becomes blurred in patients with recent SAH. In the past, hypona- tremia after SAH was attributed to the syndrome of inap- propriate secretion of antidiuretic hormone (SIADH) and was treated with fluid restriction. It is now recognized, however, that a more common cause of hyponatremia in patients with SAH is cerebral salt wasting (CSW). The mechanism of water and sodium loss in CSW has been correlated with disturbances in levels of atrial natriuretic peptide, brain natriuretic peptide, and c-type natriuretic peptide as well as with direct neural effects on renal func- t i ~ n . ~ ~ The key to diagnosis of this syndrome is the urinary excretion of large amounts of sodium and chloride at a time when the extracellular fluid volume is contracted. Declines in plasma volume, red blood cell mass, and total blood volume occur;63,68 these findings are unlike those in SIADH, in which the patient is euvolemic or hyper- volemic. In contrast to therapy for SIADH, the appropri- ate therapy for CSW is replacement of salt and water rather than fluid restriction. Assessment of volume status by means of careful recording of inputs and outputs to cal- culate sodium and chloride balance, daily body weights, or laboratory test results su esting dehydration, such as ele- vated hematocrit or bloo ?? urea nitrogen-creatinine ratio, can be useful in choosing the rap^.^.^'
Fluid restriction to control hyponatremia or to reduce the course of brain edema was tested in a randomized study, but no improvement in outcomes was noted.?' Fluid restriction is dangerous in CSW because it leads to a contracted blood volume, increased blood viscosity, and hemoconcentration-ffects that might increase the risk of ischemia among patients with vasospasm.64 The best strat- egy is to give at least maintenance volumes of colloid and crystalloid solutions. The usually daily administration of liquids, including dietary and intravenous fluids, should be approximately 2.5 to 3.5 L.31,71 Adjustments may be required, depending on urinary or insensible water losses. Central venous pressure or pulmonary artery wedge pres- sure monitoring might be needed to monitor the car- diac status of patients given large volumes of fluids. Increased volumes of sodium-containing fluids will over- come the volume contraction but may not reverse the hyponatremia."
If the serum sodium concentration does not normalize despite a euvolemic status, modest fluid restriction or an infusion of a hyperosmolar solution containing sodium can be started. The serum sodium concentration should be corrected no more rapidly than 0.7 mEqhour to avoid central pontine myelinolysis.65 In 39 patients with recent SAH, Wijdicks and associates73 administered 0.2 mg of flu- drocortisone twice a day, combined with daily fluid intake of at least 3 L, and noted improvements in plasma volume and sodium balance. As a result, these investigators rec- ommend that fludrocortisone be added to the fluid man- agement regimen if the serum concentration of sodium is less than 125 mmoVL. Hypokalemia after SAH probably results from vomiting but can be secondary to elevated

384 Stroke: Patbopbysiology, Diagnosis, and ManaBement
levels of corticosteroids, renin, or catecholamines. Because cardiac arrhythmias can be associated with hypokalemia, this imbalance should be corrected promptly.
TMATMENT OF OTHER MEDICAL COMPLICATIONS Gastrointestinal bleeding can result froin hemorrhagic gas- tritis, stress gastric ulcers, or an esophageal tear secondary to vomiting. Because of the risk of bleeding, patients are often given intravenous histamine*-receptor antagonists or proton pump inhibitors via nasogastric tube.3” Sucralfate does not have central nervous system side effects, so it has potential advantages in preventing gastrointestinal side effects among critically ill patients prone to depression in consciousness.73
Obtunded patients are at high risk for adult respiratory distress syndrome, atelectasis, pulmonary hypoventilation, and aspiration pneumonia. Gruber and colleagues,2’ evaluating pulmonary function among 207 patients with SAH, noted that severe lung dysfunction was uncommon but that its presence was correlated with a greater likeli- hood of poor outcome. Securing of the airway, careful bronchopulmonary management, and ventilatory assis- tance may be required. Events such as renal failure, hepatic dysfunction, and urinary tract infections as well as other illnesses should be treated. Measures to avoid pres- sure sores or orthopedic complications also are important.
Using data from a large multicenter randomized trial, Solenski and associates7 found a frequency of 40% for life- threatening medical complications in patients with SAH. Careful monitoring to avoid systemic complications is important in these critically ill patients. Patients with SAH who have evidence of an acute systemic inflammatory response with elevations in temperature, heart rate, respi- ratory rate, and white cell count have worse outcomes.20,21 The central nervous system injury may predispose such patients to systemic inflammation, so therapies to modu- late cytokine-induced inflammation may have potential to reduce these systemic complications.
TREATMENT OF INCMASED INTRACRANIAL PRESSURE A decline in consciousness is the hallmark of increased intracranial pressure, which, in turn, can result from a large intracerebral or intraventricular hematoma, the mass effect of a secondary ischemic lesion, cerebral edema, or hydrocephalus. SAH also causes vasoparalysis and loss of autoregulation; secondary dilation of intracranial vessels might aggravate intracranial pressure by expanding the vascular compartment. Intracranial pressure is markedly elevated within a few minutes of aneurysmal rupture; the sudden increase in pressure may help halt the bleeding. In adchtion, the elevated intracranial pressure may transiently equal mean arterial blood pressure. A massive rise in intracranial pressure is probably one of the causes of sudden death after SAH. High intracranial pressure may also lead to hypoperfusion, which induces brain ischemia. Prompt aggressive treatment of increased intracranial pres- sure is one of the keys to successful management of SAH.31
Several medical and surgical measures are available to treat brain edema or increased intracranial pressure. Con- tinuous monitoring of intracranial pressure is indicated for many patients; the results might guide the timing of sur- gical or medical interventions. Continuous intraventricular drainage combined with monitoring is an option if the patient has intraventricular hemorrhage or acute hydro- cephalus. Treatment of increased intracranial pressure consists of (1) elevation of the head of the bed to pro- mote venous drainage,(2) fluid restriction, ( 3 ) correction of hyponatremia, (4) treatment of fever or agitation, and ( 5 ) prevention of hypoventilation and secondary hypercarbia.
Intubation and hyperventilation are indicated if a patient’s condltion is deteriorating. There is no evidence that dexamethasone is useful in managing brain edema after intracranial hemorrhage. Furosemide, which can reduce intracranial pressure by limiting the production of CSF, can be given in an emergency. However, the diuretic effects of furosemide can lead to electrolyte disturbances and hypovolemia. Mannitol is an osmotic agent that can be given to control increased intracranial pressure. A response is noted within minutes, and the duration of effect is approximately 4 to 6 hours. The dosage can be repeated as needed. Secondary dehydration, hyperosmolarity, and a rebound increase in brain edema are possible complica- tions. Measurements of serum osmolality and serum elec- trolytes should be performed often, especially if repeated doses of mannitol are prescribed. Measurement of central venous or pulmonary artery wedge pressure might be needed. Hypertonic saline has also been used in refractory cases to lower intracranial pressure and has the advantage of expanding intravascular volume.74 In a small retrospec- tive study, hypertonic saline did not produce adverse effects in patients with SAH and vasospasm.’”
Increased intracranial pressure may be caused by large intracerebral hematomas, which are usually located in the basal ganglia and adjacent white matter and are most commonly seen with ruptured aneurysms of the internal carotid or middle cerebral arteries. Surgical evacuation of the hematoma can be lifesaving in a rapidly deteriorating patient. Some patients can recover and return to inde- pendent a~tivity.”.’~.’~ Stereotactic aspiration combined with the thrombolysis has also been performed success- fully.” This approach might be better than direct surgical exploration if the hematoma is located deep within the hemisphere. Patients with CT evidence of very large hematomas, extensive intraventricular bleeding, or shifts of midline structures have the poorest postoperative out- comes. In general, patients who are in better clinical con- dition and those who have a ruptured aneurysm of the middle cerebral artery are most likely to benefit.
Patients with intraventricular extension of bleeding might benefit from the combination of ventricular drainage and instillation of fibrinolytic agent^.'^ However, no ran- domized trials have tested this approach. Shimoda and coworkers8’ reported that direct surgical evacuation of major intraventricular hemorrhages is not successful. Unfortunately, patients who are in poor condltion are the ones most commonly referred for operation. Although data are lacking to support a recommendation for surgical removal of a large hematoma associated with a ruptured aneurysm, operation is an option for a patient showing no

Chapter 14: Aneurysmal Subarachnoid Hemorrhage 385
response to medical measures. Still, both the physician and the family must be aware that the patient’s life might be saved but the neurologic sequelae might be considerable.
MANAGEMENT OF HYDROCEPHALUS Hydrocephalus is a common complication of SAH, result- ing from the massive collections of blood that fill the ventricles, block the aqueduct of Sylvius, or obstruct the fourth ventricle. Blood can fill the subarachnoid cisterns or coat the arachnoid villi. The prolonged presence of exten- sive subarachnoid clots is strongly associated with the appearance of hydrocephalus; thus, an intervention that extends the presence of these clots might promote devel- opment of hydrocephalus. Conversely, therapies that stimulate clot lysis might lessen the risk of hydrocephalus.
Sheehan and associates” reported that hydrocephalus developed in approximately one fourth of their patients during the acute treatment period. Hydrocephalus is more common among patients who, upon admission, have severe neurologic impairments or CT evidence of ventricular ddation or intraventricular hemorrhage. In addition, women, patients with preexisting hypertension, and patients with a history of alcohol abuse have higher rates of hydrocephalus.”
The hydrocephalus after SAH may be classified accord- ing to its time of appearance as (1) acute-appearing within 12 hours after aneurysmal rupture, (2) subacute- developing a few days after the ictus, or (3) delayed- noted as ventricular dilation weeks to years later.R2.83 Acute hydrocephalus is an important cause of increased intracra- nial pressure and coma. Subacute hydrocephalus is a cause of a gradual decline in consciousness that can occur approximately 7 to 10 days after SAH. In this situation, intracranial pressure may be modestly elevated. Delayed hydrocephalus often manifests as a subacute dementia, gait apraxia, and bladder incontinence. In this setting, intracra- nial pressure often fluctuates and may not be consistently elevated.
Approximately 16% to 34% of patients have CT findings consistent with acute hydrocephalus. Some patients with ventricular enlargement may be asymptomatic, but most have decreased consciousness. Symptoms of acute hydro- cephalus in addition to decline in alertness are bilateral motor signs, miosis, and downward deviation of the eyes. Acute hydrocephalus predicts increased mortality and morbidity and is correlated with subsequent development of vasospasm and ischemic stroke. A patient with acute hydrocephalus can be observed, medcally managed, monitored with sequential CT studies, and treated with serial lumbar punctures. Although acute hydrocephalus may resolve spontaneously, most cases require placement of a temgorary ventriculocaval or ventriculoperitoneal catheter.”. Insertion of a ventricular catheter may be dfficult in a patient with an intraventricular clot, because blood can occlude the catheter. Continuous cisternal drainage might relieve intracranial pressure and expedite lavage of blood from the subarachnoid space.
Placement of a shunt is recommended for any patient with depressed consciousness and enlarging ventricles.
Some patients require only temporary shunting. If neces- sary the shunt can be made permanent later. Shunting is not always effective, however. Hasen and colleaguesM reported a high rate of shunt-related complications, includng intracranial infections, among their patients with SAH and acute hydrocephalus.
PREVENTION OF RECURRENT HEMORRHAGE Recurrent hemorrhage is a feared complication of SAH because it is a leading cause of death or neurologic morbimty during the first 2 weeks after SAH.l””s In the series reported by Broderick and associates: rebleedmg accounted for half of the deaths that occurred more than 2 days after SAH. Mortality rates among patients who have rebleeding are approximately twice those of patients who have a single hemorrhage. Even in centers performing early surgery, rebleeding remains a major cause of poor outcome after SAH.86
Preventing recurrent hemorrhage is a major goal of the medical management of SAH. Torner and colleaguesx7 found that the period of greatest risk for rebleeding is the first 24 hours after the ictus; the risk peaked at approxi- mately 4% during that time. These results are supported by other studies. In a Swedish series, 9.6% of all patients admitted within 24 hours of SAH had very early rebleed- ing; most of these patients died.a5 Fujii and coworkersXH found that rebleeding occurred within 24 hours of admis- sion in 31 of 174 patients (17.3%)-most of whom were waiting for surgery. Steiger and associatesxg found a low rate of recurrent hemorrhage between 5 and 13 days after SAH. The cumulative rate of rebleeding during the first 2 weeks after SAH is approximately 15% to 20%.87 The high rate of early recurrent hemorrhage has implications for the choice of treatment. Bleeding might recur even before a surgical team can be mobilized or before a medication can reach “therapeutic” levels in the blood and CSF.
Several clinical features identify those patients at the highest risk for early rebleeding. The most important is the level of consciousness at admission; patients admitted in coma are at the greatest risk. Rebleeding is also more common among older people, women, and people whose systolic blood pressure exceeds 170 mm Hg. The results of the baseline CT do not predict recurrent hemorrhage.
Recurrent hemorrhage usually causes a sudden head- ache and a rapid change in neurologic condition, including a drop in consciousness. Extensor spasms and posturing are important early signs. A “convulsion” that occurs im- mediately after SAH also can mark a recurrent hemor- rhage.40 However, rebleeding in a comatose patient may be overlooked. It may be manifested only by a sudden change in respiratory pattern or vital signs. Recurrent hemorrhage should be sought whenever a patient experiences a new headache or worsens neurologically.
The differential diagnosis of rebleeding is listed in Table 14.7. The clinical diagnosis of rebleeding can be incorrect in as many as a third of cases. Other causes of the worsening are seizures, ischemia, and medical complica- tions. The diagnosis of rebleeding should not be made solely on clinical features, because this approach leads to

386 Stroke: Patbopbysiology, Diagnosis, and Management
Table 14.7 Differential Diagnosis of Neurologic Worsen- ing after Subarachnoid Hemorrhage ~
Recurrent hemorrhage Vasospasm-induced brain ischemia Subacute hydrocephalus Seizures Hyponatremia Hypocdcemia Hypotension Hypoxia Hyperglycemia or hypoglycemia Medication effects Systemic complication (pneumonia, renal failure, etc.)
overdiagnosis. Recurrent hemorrhage can be proved most easily by the detection of additional blood on CT scans (see Table 14.7 and Fig. 1 P l B ) Changes in the CSF may be difficult to interpret.
Measures to ameliorate recurrent hemorrhage are not effective; therefore, treatment is aimed at prevention. Choices include prolonged bed rest, induced hypotension, antifibrinolytic agents, carotid ligation, intracranial clip- ping of the aneurysm, and endovascular obliteration of the aneurysm. Occlusion of the aneurysm is the best method for preventing rebleeding.” Neither absolute bed rest nor induced hypotension has been successful in improving outcomes after SAH or in reducing the risk of recurrent hemorrhage. Carotid ligation can be performed to prevent rebleedmg from aneurysms of the distal internal carotid artery, but because of the advances in intracranial opera- tive techniques and development of invasive neuro- radiologic procedures, carotid ligation now is rarely performed.9o
ANTIFIBRINOLYTIC THERAPY The rationale for the use of antifibrinolytic agents (amino- caproic acid or tranexamic acid) is that the perianeurysmal clot that formed the initial hemorrhage abuts and supports the aneurysm, thus helping to prevent its re-rupture. Treatment would be given before surgery, to prevent rebleeding while the patient was recovering from the acute effects of SAH. Antifibrinolytic agents cross the blood- brain barrier, but peak CSF levels of these agents are lower than plasma levels and are also delayed. When the agents are administered as a constant intravenous infusion, a steady state in CSF is reached only after 36 hours. There- fore, the possible therapeutic level of agent in the CSF may not be achieved during the period of highest risk for recur- rent hemorrhage.
Clinicians are concerned about the safety of antifibri- nolytic agents. A fulminant myopathy, rhabdomyolysis, or myoglobulinuria can complicate prolonged use of these medications?’ Antifibrinolytic agents accentuate the devel- opment of h y d r o c e p h a l ~ s . ~ ~ ~ ~ ~ Ischemic stroke is the most feared side effect. The higher risk of ischemia might be the result of (1) a persistent subarachnoid clot that induces vasospasm, (2) an intravascular change in coagulation that potentiates intra-arterial thrombosis, or (3) a change in blood viscosity that impairs perfusion. The high rate of
ischemic stroke is the primary reason that antifibrinolytic agents are not established as effective in the acute man- agement of SAH.92.93
A randomized trial of tranexamic acid showed a consid- erable reduction in the risk of rebleeding with treatment, but these effects were negated by a higher risk of ischemic complications; as a result, outcomes were not impr~ved.’~ These results were buttressed by those of a large, nonran- domized trialg2 The combination of an antifibrinolytic agent and nimodipine has been used as a medical regimen to prevent both rebleeding and ischemia while a patient waits for delayed operation. Some success has been reported using this approach.94 However, a placebo- controlled trial of tranexamic acid combined with calcium antagonists and hypervolemia did not find a net benefit from the combination of intervention^.^^ Although the antifibrinolytic agent reduced the risk of rebleeding, the occurrence of ischemic stroke and other complications was similar in the two treatment groups. Meta-analyses found that antifibrinolytic agents do not have a positive effect on improving outcomes after SAH.g6.9’
Antifibrinolytic agents are the only effective mehcal therapy to reduce the risk of early rebleedmg after SAH. These medications remain a part of the preoperative man- agement of patients scheduled for delayed surgery. This therapy should not be started for a patient who is sched- uled for early operation or in whom diagnosis of SAH was delayed, because patients surviving 7 to 14 days after SAH have already passed the period of highest risk for recur- rent hemorrhage. There is little indication to give these agents to patients with nonaneurysmal SAH.
INTRACRANIAL OPERATION Surgery is an important component of management of SAH. Indications for surgery are the need to clip the aneurysm to prevent rebleeding and evacuation of a hematoma. Currently, surgery is the preferred treatment for the aneurysm, but the recommendation for surgery must still be made on a case-by-case basis. For example, the patient’s age, the severity of neurologic injury, or the presence of a serious comorbid disease may weigh against an intracranial operation. Although people older than 60 years tolerate intracranial operation less well than younger people, age alone is not a reason for excluding surgery from the treatment regimen, because outcomes in the elderly have improved over time.’4
For most patients, the question is not whether the aneurysm should be clipped but, rather, when is the ideal time for the operation. Some neurosurgeons advocate delaying surgery until a patient’s condition has stabili~ed,’~ but most neurosurgeons now favor early ~peration.~’ Early operation is preferred because the risk of rebleeding is eliminated and the operation is performed before vasospasm appears. The primary reason for delaying surgery has been that a lag permits the patient’s condition to recover from the initial event before the patient is subjected to the stresses associated with early surgery. Delayed surgery leaves the aneurysm untreated during the period of highest risk of rebleeding. In addition, the poten- tial of recurrent rupture of an unsecured aneurysm can

Chapter 14: Aneurysmal Subarachnoid Hemorrhage 387
complicate hypervolemic hernodilution and induced hypertension for treatment of ischemia secondary to vasospasm. Surgeons rightfully point out that the overall results of management, and not just postoperative statis- tics, should be compared. The overall results of early medical treatment followed by a delayed operation are not satisfactory.
Several groups describe favorable results of early oper- ation combined with a variety of interventions, including calcium channel blockers.% A small trial in Finland demonstrated better outcomes for early operation."' Although the data favored early operation, the results were distorted by a simultaneous random assignment of patients to receive either placebo or active treatment with calcium channel blocking agents. Miyaoka and associates'" reported better management results with early surgery in patients who were in good condition and better results with delayed operation in patients who were seriously ill. A large international epidemiologic study evaluated out- comes of 3521 patients hospitalized within 3 calendar days of SAH.lo4.10s Although it was not a randomized trial, the large numbers assured that prognostic factors were similar in the groups that underwent early and delayed operations. Overall management results (favorable outcomes) were similar in the two treatment groups, but early surgery &d reduce the overall risk of rebleeding. Early surgery was not associated with a high rate of intraoperative complication, such as re-rupture of the aneurysm or worsening of brain edema.
Early operation reduces the mortality and morbidity from rebleeding. However, early operation does not seem to prevent the development of vasospasm or to facilitate the treatment of secondary ischemia enough to lower the mor- bidity and mortality from ischemia. Early operation (sooner than 3 days after SAH) is effective, but the results of early operation are not so overwhelming that it should be recom- mended for all cases. Plans for surgery should continue to be made on a case-by-case basis. For example, Deruty and colleagues'06 restrict early operation to only alert patients younger than 50 years. An important consideration is the skill of the neurologic surgeon, who must have demon- strated success in operating on these acutely ill patients. If all these criteria are not met, the patient may not be best served by an early emergency operation to clip the aneurysm. Still, the potential utility of early operation emphasizes the importance of a prompt, accurate diagnosis.
ENDOVASCULAR TREATMENT Endovascular obliteration of the aneurysm or the parent artery is used to treat aneurysms of the intracavernous or proximal portions of the internal carotid artery, even in patients who have a carotid-cavernous fistula. Tandem placement of balloons in the parent artery (trapping) can shrink the aneurysm or lead to its occl~sion.'~ This proce- dure is relatively effective, and the risk of ischemic stroke is However, detachable balloons can be relatively difficult to place within the aneurysm. The sizes and shapes of the balloons might not correspond to the contour of the aneurysmal sac. Occasionally, the balloons can be lost and migrate into distal arteries. In addition, the balloons can
deflate, and the aneurysm can become recanalized. Finally, the balloons might place pressure on the aneurysm's wall and promote recurrent rupture.
Endovascular placement of adhesive materials can be used to occlude smaller intracranial aneurysms. Kinugasa and associates"' reported success with the placement of cellulose acetate polymer for occlusion in 9 of 12 patients with aneurysms. Obliteration of the aneurysmal sac expe- dited treatment of vasospasm and allowed the patients to become stable before the aneurysm was surgically repaired.
Development of microcatheters and detachable coils has stimulated greater interest in direct endovascular treat- ment of intracranial aneurysms.lW Aneurysms that are not easily approached for direct cli ing might be occluded with endovascular treatment.'"'' In particular, aneu- rysms of the posterior circulation and the basilar bifur- cation can be treated with placement of coils."2 In one multicenter trial comprising 150 patients, basilar tip aneurysms were treated with detachable platinum coils; approximately 75% of the aneurysms were successfully treated.'13 The periprocedural mortality rate was 2.7%. Complications included rupture of the aneurysm and occlusion of the parent artery. Cognard and colleague^'^^ treated 208 patients with aneurysms (150 with SAH), achieving total occlusion of the aneurysms in 81% of cases, and subtotal occlusion in 17%. In another study, 75 seri- ously ill patients with ruptured aneurysms were treated with coil^."^ Success was achieved in most patients, although procedure-related mortality and morbidity occur- red in 8% of cases. Lefkowitz and coworkers116 placed coils in wide-necked aneurysms in 23 patients; complete or nearly complete occlusion was achieved in all cases. Three patients had complications. Although the usefulness of endovascular placement of coils has not been compared with that of surgery, this therapy has gained popularity and likely will continue to increase in popularity in the future.
VASOSPASM AND ISCHEMIC STROKE Although early intracranial operation and the use of antifibrinolytic agents reduce the risk of recurrent hemor- rhage after SAH, these advances have not been associated with declines in mortality or morbidity, primarily because of vasospasm-induced ischemic stroke."' Brain infarction accounts for approximately one third of all unfavorable outcomes after SAH.
The term vasospmm is used to describe the luminal nar- rowing detected by arteriography performed approxi- mately 7 to 10 days after SAH. Abnormalities may be restricted to one artery or may involve several vessels. Although vasospasm can complicate intracranial bleeding from other sources, including trauma, it is most commonly associated with a ruptured aneurysm. Autopsy examination of patients dying from the effects of acute vasospasm reveals morphologic changes in the capillaries, veins, small arteries, and larger arteries. Changes include disruption of the internal elastic lamina, swelling of the arterial media, smooth muscle necrosis, and infiltration of the adventitia by macrophages, lymphocytes, and plasma cells. Smith and colleagues"' noted endothelial desquamation, intimal proliferation, necrosis and fibrosis of the me&a, and

388 Stvoke: Patbopbysiology, Diagnosis, and Management
intramural deposits of type V collagen in their study of vasospasm. They concluded that the lumen of the vessel can remain constricted for weeks after SAN. Degenerative changes in the medal and intimal layers of the arteries can persist for at least 2 weeks.
The amount of blood in the subarachnoid space correlates with the development of vasospasm. A normal component of blood is presumably released at the time of or shortly after SAH. This substance or combination of factors, once liberated into the subarachnoid space, causes the vasospastic proce~s."~ Oxyhemoglobin may be the most important factor.'"^"' Vasospasm has been ascribed to prolonged arterial contraction, inhibition of vasodilation, an immunoreactive or inflammatory process, a mechanical phenomenon, or depressed arterial nietabolism."x~llg~'"' Nagatani and associates'" proposed that the breakdown products of blood lead to impaired mitochondria1 function and reduced energy levels in cerebral arteries. Elevations of platelet-activating factors that may mediate inflamma- tory responses and that have a close link to eicosanoids are common and are linked to infarction after SAH.1"2 Distur- bances in arachidonate metabolism and elevations of endothelin, a potent vasoconstrictor, may also be impor- tant in the development of vasospasm.'2~'2s Disturbances in levels of D dimer and fibrinogen also correlate with the
development of delayed ischemic neurologic impairments after SAH."' It is likely that vasospasm is the result of a complex process involving several metabolic and vascular derangements.
The arterial narrowing cause by vasospasm raises cere- bral vascular resistance and impairs cerebral autoregula- tion. As a result, perturbations in blood pressure can lead to declines in perfusion pressure and blood flow, resulting in brain ischemia. Yundt and coworkerslz6 showed that regional oxygen extraction is increased and cerebral blood volume reduced in the presence of vasospasm. Elevated intracranial pressure or increased viscosity secondary to hemoconcentration or dehydration can aggravate the impairments in flow. The end result is infarction in the arterial beds of the involved arteries. Infarctions are usually cortical and in border zone regions between the anterior, middle, and posterior cerebral arteries.
Major arterial narrowing can be detected arteriograph- ically 1 week after SAH in approximately 70% of patients (Figs. 14-4 to 14-6). Vasospasin causes symptoms in approximately 20% to 30% of patients. The severity of the arterial narrowing correlates with the likelihood of ischemic signs and an unfavorable outcome. Vasospasm is seen most commonly in the distal portion of the internal carotid artery and the proximal portions of the middle and
FIGURE 14-4 Anteroposterior oietv of a right carotid cirteri- ogrmn obtained with the use of srrhtractioti techriiqrie clerruw .str(ites ari nrieunjstn of the right middle cerebral ~ r t e r t j (ai-ron~) atid oasospasrn of the mirllle cerebral ar teq ( ~ K K O W ~ I ~ S ) .
FIGURE 14-5 Lnterrrl oieic .fa certebral arteriogram shows a lobrilatcd anenrrjsin a t the junction of the Gertebral and pos- teroinjerior cerebellar cirteries (large arrow) arid onsospnsiri of the contralriterd oertebral a r t e q (small ~LKKOWS).

Chapter 14: Aneurysmal Subavachnoid Hemorrhage 389
FIGURE 14-6 Anteroposterior ijieiu of a left carotid arteri- ograni obtained with the use of subtraction technique demon- strates a large fusifonn aneuysin arising from the middle cerebral artenj (arrowhead). In addition, vasospasm is present in the proximal anterior cerebral arte y (small arrows) and middle cerebral arte y (large arrows).
anterior cerebral arteries. The site of the ruptured aneurysm does not influence the development of vasospasm, but a common location for the narrowing is adjacent to the clot and aneurysm. Vasospasm also can be generalized or can be localized to an area of the brain remote from the aneurysm. Vasospasm is detected rarely before 48 hours after SAH, peaks at 5 to 10 days, and usually abates by 14 to 21 days. Predictors of poor out- comes from vasospasm include older age, poor condition on admission, large amount of blood on baseline CT, lack of improvement with hypervolemic treatment, and intracranial complications from hypervolemic therapy.lgi
Vasospasm is more likely to occur in young patients, women, patients with a prolonged duration of uncon- sciousness, patients in poor neurologic condition, patients with acute hydrocephalus, and patients with an abnormal electro~ardiogram.~"J~~ Qureshi and associate^'^^ reported that the risk of vasospasm was highest among patients with
thick subarachnoid clot on CT, an early rise in flow velocity detected by transcranial Doppler ultrasonography, decreased consciousness, or ruptured aneurysms of the anterior or middle cerebral artery.
Juvela13' found that the use of aspirin before SAH less- ened the likelihood of vasospasm and ischemia. This obser- vation prompted a pilot study of aspirin as prophylaxis against vasospasm after surgical treatment of the aneurysm.'32 Neurologic deterioration was noted in 15 of 26 patients given placebo and in 10 of 24 patients given aspirin. Four other antiplatelet agents have also been tested, and a systematic overview of all trials of antiplatelet therapy did not show benefit." The presence of fever (>38.3OC for 2 consecutive days) also predicts vasospasm independently from the severity of hemorrhage and the presence of infe~tion. '~ The amount of subarachnoid blood as seen on early CT is an important predictor, as is the presence of blood in both lateral ventricles.'33.'34 Ischemic complications of vasospasm are also more likely to occur among patients who have hyponatremia, dehydration, or hypotension. Recent cocaine use has also been associated with increased risk of ~asospasm."~
The symptoms of vasospasm usually begin insidiously.'x Findings can wax and wane over several hours or evolve suddenly. Increased headache, low-grade fever, increased meningismus, seizures, and disturbances of consciousness are usually followed by the appearance of focal neurologic impairments that primarily reflect ischemia in the vascular territories of the anterior and middle cerebral arteries. The process can progress to infarction, leading to neurologic residuals and hypodense lesions detected by CT. The dif- ferential diagnosis of vasospasm as a cause of neurologic worsening after SAH is the same as that of rebleeding (see Table 14.7). Alternative diagnoses should be excluded before vasospasm-induced ischemia is dagnosed.
Arteriography is the most definitive way to establish a firm diagnosis of vasospasm. Cerebral blood flow meas- urements detect local or generalized hypoperfusion. Single-photon emission computed tomography (SPECT) has a strong concordance with transcranial Doppler ultra- sonography, and SPECT measurements of cerebral blood flow could be used to screen for vasospasm.'37 Sequential transcranial Doppler studies are used to monitor for the development of vasospasm. 138~139 Progressive narrowing of the lumen can be accompanied by increased velocity in the arteries. Changes in flow velocity are uncommon during the first 48 hours after SAH.13' Transcranial Doppler ultra- sonography is particularly useful in patients with narrow- ing in the middle cerebral artery.138 Changes in velocity may precede the development of ischemic symptoms, and increases in velocity are highest among patients with ischemic deficits. 13* Disturbances in flow velocity are influ- enced by the patient's age as well as the presence of hyper- tension or tissue hyperemia.'4s'42 The extent of peripheral arteriolar resistance vessels, the presence of arterial anas- tomoses, or the use of nimodipine also can affect flow velocit ie~. '~~ Current evidence supports the use of trans- cranial Doppler ultrasonography as an adjunctive means of monitoring patients for the development of vasospasm. With future experience and with refinement and develop- ment of the technology, the need for arteriography may in time be eliminated.

390 Swoke: Patbophysiology, Diagnosis, and Management
REMOVAL OF THE SUBARACHNOID CLOTS Early intracranial operation and lavage of the subarachnoid space can remove clots and might prevent development of vasospasm. The rationale for this procedure is that evacu- ation of the clots might prevent the release of substances that induce the arterial narrowing. Surgical removal of the clots can be difficult in critically ill patients, however, and some of the blood collects in areas far from the operative field. Extensive manipulation of the brain to remove the subarachnoid clots may also injure penetrating vessels, leading to ischemic deficits. Despite promising preliminary studies of clot removal, a large international study &d not show an reduction in the severity or incidence of vasospasm."'It appears that vigorous lavage of the sub- arachnoid space is not a feasible way to prevent vasospasm in most patients.
Several small studies report the potential usefulness of intrathecal thrombolyhc therapy in the settin of acute surgical treatment of a ruptured Most of these studies treated only patients judged to be at very high risk for vasospasm and ischemia. Outcomes were gen- erally favorable, consisting of a lower frequency of severe vasos asm and ischemic impairments."' Kodama and asso- ciateJ4' performed cisternal irrigation with urokinase and ascorbic acid in 217 high-risk patients, and observed sub- sequent symptomatic vasospasm in 6 patients. Throm- bolytic agents can be instilled safely into the basal cisterns. The risk of major bleeding complications, in particular brain hemorrhage, appears to be low. Because of the risk of hemorrhage, thrombolytic agents should not be administered until the aneurysm has been occluded. The optimal timing of treatment, the duration of treatment, the best agent, and the best dose are not known. Consid- erable research, including prospective controlled trials, is needed before intrathecal thrombolyhc agents are added to the usual care of patients with recently ruptured aneurysms.
CALCIUM CHANNEL BLOCKING AGENTS Influx of extracellular calcium, an important component in sustaining contraction of smooth muscle, is critical in the process of cellular ischemia. An agent that inhibits calcium entry might prevent vasospasm or its cerebral ischemic consequences. The dihydropyridine derivatives nimodip- ine and nicardipine have been tested. Although these agents can reduce the arterial blood pressure, they also increase cerebral blood flow, including in ischemic regions. Small studies testing the utility of oral nimodipine found that the medication reduced mortality and morbidity but it did not prevent vasospasm.149~150 A British trial estab- lished the utility of nimodipine to improve outcomes after SAH.lS1 The rate of favorable outcome was increased from 67% to 80.2% with treatment. Meta-analyses confirm the efficacy of nimodipine in treating patients with recent SAH.15%-'" Although a significant reduction in mortality is not achieved, the calcium channel antagonists reduce the proportion of patients with ischemic deficits secondary to vasospasm.
Table 14.8 Management Options in Prevention or Treat- ment of Vasospasm and Brain Ischemia after Subarachnoid Hemorrhage
Prevention Nimodipine
Symptomatic medical Maintain adequate hydration Treat elevated intracranial pressure
treatment Discontinue antihypertensives and antifibrinolytic therapy
Hemodilution, hypewolemia, and hypertension (triple-H therapy)
Monitor with central venous pressure or pulmonary artery wedge pressure and electrocardiography
Administer isotonic crystalloids, colloid or blood
Venesection if necessary to keep hematocrit at 3035%
Use of vasopressors or positive inotropic agents
Symptomatic Intra-arterial papaverine neurointerventional Angioplasty therapy
In general, nimodipine is safe, and complications of its use are few. Hypotension is a potential side effect. The exact mechanism of nimodipine's efficacy is unclear, but it may be neuroprotective. Patients with recently ruptured aneurysms should receive nimodi ine as part of their
Drug Administration have approved the use of nimodip- ine for this indication. The usual oral dosage of nimodp- ine is 60mg every 4 hours. Comatose patients can receive the medication via a nasogastric tube. The usual duration of treatment is 3 weeks after SAH, although a shorter course (10 to 14 days) may be all that is needed. If the SAH is not diagnosed until 10 to 14 days after it has occurred, the patient has already survived the period of greatest risk for ischemia, and nimodipine might not be needed.
Nicardipine has similar potential therapeutic actions, and it can be given parenterally. Use of this agent in SAH was tested in a large clinical trial.'55,'56 At 3 months, the actively treated and control groups had comparable rates of favorable outcomes, but the frequency of symptomatic vasospasm was reduced with the use of nicardipine. In another study comparing two different doses of nicardip- ine, the same investigators found that the lower dose of medication was associated with a slightly higher rate of severe vasospasm but that outcomes were similar in the two groups.157 Shibuya and colleagues,'" who administered nicardipine intrathecally to 50 patients with SAH, noted declines in both symptomatic and arteriographic vaso- spasm. These stu&es suggest that nicardipine is effective in preventing ischemic sequelae of SAH but that the combination of aggressive volume expansion and induced hypertension is also effective. These additional data sup- port the use of calcium channel blockers supplemented by hypervolemic hemodilution and induced hypertension for prevention of ischemic stroke after SAH.
general medical care (Table 14.8).3 B ,71 The U.S. Food and

Chapter 14: Aneurysmal Subarachnoid HemorrhaJe 391
OTHER MEDICATIONS TO PREVENT VASOSPASM OR ISCHEMIC STROKE Calcitonin gene-related peptide (CGRP), a potent vasoddator, was tested in a small clinical trial.'s9 Hypoten- sion was a common side effect, and two thirds of the treated patients dld not complete of the course of treat- ment. Although this study was reported as having negative results for the use of CGRP, largely because of its small size, favorable outcomes were noted in 66% of treated patients and 60% of controls.
Clinical studies of superselective intra-arterial adminis- tration of papaverine suggest that this potent vasodilator may be helpful.'60 Firlik and coworkersJ6' found that intra- arterial papaverine can reverse the arterial narrowing of vasospasm. In their series of 15 patients (32 treated arteries), papaverine therapy increased cerebral blood flow in 46% of cases and led to major clinical improvement in 26%. Kaku and associateP2 reported that this agent should be given before the arteries lose their ability to respond. Hypotension does not appear to be a complication of local intra-arterial infusions. Seizures have been reported as a complication of this therapy.'" Arakawa and colleagues'M reported that the vasoddator milrinone might be helpful in dilating vasospastic vessels.
Finfer and associates'6 used barbiturate-induced coma to protect the brain in 11 patients with severe vasospasm, 10 of whom had good outcomes. These investigators proposed this therapy for patients who show no response to other medical interventions. Although barbiturate-induced coma does offer benefit, it is a very vigorous therapy that requires intensive adjunctive care. Its u d t y has not been established.
The 21-aminosteroids can scavenge free radicals and inhibit lipid peroxidation, features that promote stabiliza- tion of the membranes of ischemic tissues. Clinical trials have been conducted to test intravenously administered tirilazad given as a supplement to oral nimodipine.'6'68 Although the medication was well tolerated, no major improvement in favorable outcomes was noted with treat- ment. The medwation has not been approved for man- agement of patients with SAH.
HYPERVOLEMIC HEMODILUTION AND INDUCED HYPERTENSION Increasing cerebral blood flow can ease ischemic symp- toms and can revent permanent neurologic sequelae (see Table 14.8).".p6g~170 Reduction in the diameter of the vas- cular lumen affects the bloods rheologic characteristics and, thus, influences flow. Severe losses of water and sodium result in hernoconcentration, which in turn increases viscosity and reduces blood flow. Measures to prevent infarction by correcting the losses of sodium and water are initiated upon the patient's admission to the hos- pital. A small randomized trial of prophylactic therapy with hypervolemic hypertensive hemoddution therapy did not demonstrate benefit in preventing vasospasm.
Because autoregulation is impaired, cerebral blood flow becomes pressure-dependent. Cerebral perfusion pressure is altered by changes in the mean arterial blood pressure and intracranial pressure. Improvement of venous drainage by positioning and elevation of the head, treatment of brain
edema, and control of hydrocephalus lowers intracranial pressure and improves perfusion. When feasible, antihy- pertensive agents are avoided. Nimodipine may have to be discontinued so that the blood pressure can be effectively raised. After the diagnosis of symptomatic vasospasm is made, more aggressive treatment of increased intracranial pressure, including hyperventilation and mannitol, might help. Antifibrinolytic agents should be discontinued.
Several groups report reversal of ischemic symptoms with the combination of volume expansion and drug- induced hypertensi~n. '~~~' '~ In some cases, neurolo 'c signs can reappear when the therapy is discontinued. Although no controlled trials of this regimen have been conducted, the previously described trial of nicardi ine demonstrates a benefit from this aggressive therapy. Qureshi and associate~''~ found that patients with a depressed level of consciousness at the initiation of volume expansion therapy had the poorest responses to treatment. Another trial compared the effects of hypervolemic or nor- movolemic therapy on blood flow and cardiac f~nction.'~' The investigators found that hypervolemic therapy raised cardiac filling pressures but it did not increase cerebral blood flow. A meta-analysis of published data found that there is no sound evidence for or against the use of volume expansion therapy in patients with SAH.'74
If improvement is not observed after volume expansion, a vasopressor (most commonly dopamine or phenylephrine) is added in an attempt to increase mean arterial blood pressure. Darby and coworker^"^ noted that the increase in cerebral blood flow after use of dopamine may be indepen- dent of changes in blood pressure, because the dopamine might have direct cerebrovascular effects. Although there is some disagreement about the utility of hypervolemic hemo- dilution and induced hypertension to prevent ischemia after SAH, the regimen is commonly p r e ~ c r i b e d . ' ~ ~ ~ ~ ~ ~ ' ' ~
This therapy is vigorous, and patients need intensive observation. Arterial pressure, cardiac rhythm, central venous pressure, or pulmonary artery wedge pressure should be continuously monitored. 170 Continuous intracra- nial pressure monitoring may also be needed. Frequent laboratory assessments of serum electrolytes, serum osmolarity, blood gases, and blood counts are needed. Complications of the therapy include congestive heart failure, pulmonary edema, acute myocardial infarction, and cardiac arrhythmias. Worsening of brain edema, hyperten- sive intracerebral hemorrhage, hemorrhagic transforma- tion of the infarction, and re-rupture of the aneurysm can also occur.169,'7* Shimoda and colleague^'^^ reported wors- ening of brain edema in 18 of their 94 patients undergo- ing hypervolemic hemodilution; 8 others had hemorrhagic infarctions. These investigators advised against the use of hypervolemic hemodilution if a patient's CT scan shows an ischemic lesion in the brain, particularly if the abnormal- ity is found within 6 days of SAH. Hetastarch is not used as a volume-expanding agent because it prolongs the acti- vated partial thromboplastin time and, hence, bleeding. '*'
$fi,
l!S,lS6
ANGIOPLASTY Transluminal angioplasty successfully dilates vasospastic arteries.'*' The development of microballoons allows for

392 Stroke: Patbopbysiology, Diagnosis, and Management
catheterization in small- to medium-sized arteries at the base of the brain. Angioplasty does stretch and disrupt the arterial wall.’s2 Bejjani and associate^'^^ performed angio- plasty at approximately 7 days after SAH in 31 patients, treating a total of 81 vessels. These investigators noted major clinical improvements in 12 cases and moderate improvements in another 11. They encountered no major neurologic complications and concluded that angioplasty is a potentially useful treatment for patients who show no response to other therapies. Polin and coworkers’84 found that angioplasty is effective in reversing angiographically confirmed vasospasm, but they did not observe clinical improvements with treatment. At present, angioplasty is usually reserved for treatment of SAH that does not respond to medical measures.
CONCLUSION Considerable progress is being made in the manage-
ment of SAH. Medical and surgical therapies that effec- tively prevent rebleeding and vasospasm are reflected by declines in mortality and morbidity. Still, there is consid- erable room for improvement. Several promising therapies are being tested; one or more of these interventions likely will be shown to further improve outcomes after SAH. However, most successful therapies are based on early treatment. Thus, the medical community must give greater attention to the early diagnosis of SAH and the acute care of patients with SAH who are critically ill.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
Rinkel GJE, Wijdicks EF, Vermeulen M: The clinical course of perimesencephalic non-aneurysmal subarachnoid haemorrhage. Ann Neurol 29:463, 1991. Velthuis BK, Rinkel GJ, Ramos LM, et al: Perimesencephalic hem- orrhage: Exclusion of vertebrobasilar aneurysms with CT angiogra- phy. Stroke 30:1103-1109, 1999. Arboix A, Marti-Vilalta JL: Predictive clinical factors of very early in-hospital mortality in subarachnoid hemorrhage. Clin Neurol Neurosurg 101:lOO-105, 1999. Broderick JP, Adam SA, Mann JI: Initial and recurrent bleeding are the major causes of death following subarachnoid hemorrhage. Stroke 25:1342-1347, 1994. Schievink WI, Wijdicks EFM, Parisi JE: Sudden death from aneurysmal subarachnoid hemorrhage. Neurology 45%-874, 1995. Edner 6, Ronne-Engstrom E: Can early admission reduce aneurys- mal rebleeds? A prospective study on the aneurysmal incidence, aneurysmal rebleeds, admission and treatment delays in a defined region. Br J Neurosurg 5:601, 1991. Solenski NJ, Haley EC Jr, Kassell NF: Medical complication of aneurysmal subarachnoid hemorrhage: A report of the multicenter, cooperative aneurysm study. Participants of the Multicenter Cooperative Aneurysm Study. Crit Care Med 23:1007-1017, 1995. Proust F, Hannequin D, Langlois 0: Causes of morbidity and mor- tality after ruptured aneurysm surgery in a series of 230 patients: The importance of control angiography. Stroke 26: 1553, 1995. Rosenorn J, Eskesen V, Schmidt K: Clinical features and outcome in females and males with ruptured intracranial saccular aneurysms. Br J Neurosurg 7287, 1993. Saveland H, Brandt L: WVhich are the major determinants for outcome in aneurysmal subarachnoid hemorrhage’? Acta Neurol Scand 90245, 1994. Johnston SC, Sehin S. Cress DR: The burden, trends, and demo- graphics of mortality from subarachnoid hemorrhage. Neurolog) 50:141%1418, 1998.
12. Roos YB, de Haan RJ, Beenen LF, et al: Complications and outcome in patients with aneurysmal subarachnoid haemorrhage: A prospec- tive hospital based cohort study in the Netherlands. J Neurol Neurosurg Psychiatry 68:337341,2000.
13. Cesarini KG, Hardemark H-G, Persson L: Improved survival after aneurysmal subarachnoid hemorrhage: Review of case management during a 12-year period. 1 Neurosurg 90:66p672, 1999.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
JohaGson M, Gidiana K, Contant EF, et al: Changes in interven- tion and outcome in elderly patients with subarachnoid hemor- rhage. Stroke 32:2845-2849, 2001. Adams HP Jr, Kassell NF, Torner JC: Usefulness of computed tomography in predicting outcome after aneurysmal subarachnoid hemorrhage. Neurology 35: 1263-1267, 1985. Roos EJ, Rinkel GJ, Velthuis BK, Algra A: The relation between aneurysm size and outcome in patients with subarachnoid hemor- rhage. Neurology 54323342336, 2000. Pobereskin LH: Influence of premorbid factors on suMval follow- ing subarachnoid hemorrhage. J Neurosurg 95:555-559, 2001. Kongable GL, Lazino G, Germanson TP: Gender-related dif- ferences in aneurysmal subarachnoid hemorrhage. J Neurosurg 84:43-48, 1996. Oliveira-Filho J, Ezzeddine MA, Segal AZ, et al: Fever in subarachnoid hemorrhage: Relationship to vasospasm and outcome. Neurology 56:1299-1304, 2001. Gruber A, Reinprecht A, Gorzer H, et al: Pulmonary function and radiographic abnormalities related to neurological outcome after aneurysmal subarachnoid hemorrhage. J Neurosurg 88:28-37, 1998. Yoshimoto Y, Tanaka Y, Hoya K: Acute systemic inflammatory response syndrome in subarachnoid hemorrhage. Stroke 321989- 1993, 2001. Fujii Y, Takeuchi S, Sasaki 0, et al: Serial changes of hemostasis in aneurysmal subarachnoid hemorrhage with special reference to delayed ischemic neurological deficits. J Neurosurg 863594402, 1997. Mack WJ, Mocco J, Hoh DJ, et al: Outcome prediction with serum intercellular adhesion molecule-1 levels after aneurysmal subarach- noid hemorrhage. J Neurosurg 96:71-75, 2002. Enblad P, Persson L: Impact on clinical outcome of secondary brain insults during the neurointensive care of patients with subarachnoid haemorrhage: A pilot study. J Neurol Neurosurg Psychiatry 62: 512-516, 1997. Camarata PJ, Heros PC, Latchaw RE: “Brain attack”: The rationale for treating stroke as a medical emergency. Neurosurgery 34:144- 158, 1994. Adams HP Jr, Jergenson DD, Kassell NF: Pitfalls in the recognition of subarachnoid hemorrhage. JAMA 2443794796, 1980. Edlow JA, Caplan LR: Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. N Engl J Med 342:2936, 2000. Neil-Duyer G, Lang D: ‘Brain attack-aneurysmal subarachnoid haemorrhage: Death due to delayed diagnosis. J R Coll Physicians Lond 31:49-52, 1997. Findlay JM: Current management of aneurysmal subarachnoid hemorrhage: Guidelines from the Canadian Neurosurgical Society. Can J Neurol Sci 24:161-170, 1997. Mayberg MR, Batjer HH, Dacey R: Guidelines for the management of aneurysmal subarachnoid hemorrhage. Circulation 90:2592- 2605, 1994. IVijdicks EFM: \\’orst case scenario: Management in poor-grade aneurysmal subarachnoid hemorrhage. Cerebrovasc Dis 5:163-169, 1995. Thonrson S, Ryan JM, Lyndon J: Brain attack:-how good is the early management of subarachnoid haemorrhage in accident and emergency departments? South Thames A&E Specialty Sub Committee Audit Group. Emerg Med J 17:17&179, 2000. Mitchell P, WVilkinson ID, Hoggard N, et al: Detection of sub- arachnoid haemorrhage with magnetic resonance imaging. J Neurol Neurosurg Psychiatry 70:205-211, 2001. Velthuis BK, Rinkel GJ, Ramos LM, et al: Subarachnoid hemor- rhage: Aneurysm detection and preoperative evaluation with CT angiography. Radiology 208:423430, 1998. Zouaoui A, Sahel M, Marro B, et al: Three-dimensional computed tomographic angiography in detection of cerebral aneurysms in acute subarachnoid hemorrhage. Neurosurgery 41: 125-130, 1997. Hashimoto H. Jim-Ichi I. Hironaka Y, et al: Use of spiral comp- uterized tomography angiography in patients with subarachnoid

Chapter 14: Aneurysmal Subarachnoid Hemorrhage 393
hemorrhage in whom subtraction angiography did not reveal cere- bral aneurysms. J Neurosurg 92:278-283,2000.
37. Lenhart M , Bretschneider T, Gmeinwieser J, et al: Cerebral CT angiography in the diagnosis of acute subarachnoid hemorrhage. Acta Radio1 38:791-796, 1997.
38. Black PM, Crowell RM, Abbott WM: External pneumatic calf com- pression reduces deep vein thrombosis in patients with ruptured intracranial aneurysms. Neurosurgery 18:25-28, 1986.
39. Nishioka H: Report of the Cooperative Study of Intracranial Aneurysms and Subarachnoid Hemorrhage. Section VII, Part I: Evaluation of conservative measurement of ruptured aneurysms. J Neurosurg 25:574, 1966.
40. Hart RG, Byer JA, Slaughter JR: Occurrence and implications of seizures in subarachnoid hemorrhage due to ruptured intracranial aneurysms. Neurosurgery 8:417, 1981.
41. Rhoney DH, Tipps LB, Muny KR, et al: Anticonwlsant prophy- laxis and timing of seizures after aneurysmal subarachnoid hemor- rhage. Neurology 55:258-265, 2000.
42. Sundaram MBM, Chow F: Seizures associated with spontaneous subarachnoid hemorrhage. Can J Neurol Sci 13:229-231, 1986.
43. Fisher CM: Clinical syndromes in cerebral thrombosis, hyperten- sive hemorrhage and ruptured saccular aneurysm. Clin Neurosurg 22:117, 1975.
44. Di Pasquale G, Andreoli A, Lusa AM, et al: Cardiologic complica- tions of subarachnoid hemorrhage. J Neurosurg Sci 42:33-36,1998.
45. Di Pasquale G, Pinelli G, Andreoli A Torsades de pointes and ven- tricular flutter-fibrillation following spontaneous cerebral subarach- noid hemorrhage. Int J Cardiol 18:163, 1988.
46. Manninen PH, Ayra B, Gelb AW: Association between electrocar- diographic abnormalities and intracranial blood in patient with acute subarachnoid hemorrhage. J Neurosurg Anesthesiol 7:lZ-16, 1995.
47. Oppenheimer SM, Hachinski V: Neurogenic cardiac effects of cere- brovascular disease. Curr Opin Neurol7:20-24, 1994.
48. Randell T, Tanskanen P, Scheinin M, et al: QT dispersion after sub- arachnoid hemorrhage. J Neurosurg Anesthesiol 11: 163-166, 1999.
49. Machado C, Baga JJ, Kawasaki R, et al: Torsades de pointes as a complication of subarachnoid hemorrhage: A critical reappraisal. J Electrocardiol30:31-37, 1997.
50. Gascon P, Ley TJ, Toltzis RJ, Bonow RO: Spontaneous subarach- noid hemorrhage simulating acute transmural myocardial infarction.
, Am Heart J 105:511, 1983. 51. Sakka SG, Huettemann E, Reinhart K: Acute left ventricular dys-
function and subarachnoid hemorrhage. J Neurosurg Anesthesiol 11:209-213, 1999.
52. Yuki K, Kodama Y, Onda J: C o r o n q vasospasm following subarachnoid hemorrhage as a cause of stunned myocardium. J Neurosurg 75:308-311, 1991.
53. Mayer SA, Lin J, Homma S, et al: Myocardial injury and left ventricular performance after subarachnoid hemorrhage. Stroke 30:78&786, 1999.
54. Zaroff JG, Rordorf GA, Newell JB, et al: Cardiac outcome in patients with subarachnoid hemorrhage and electrocardiographic abnormalities. Neurosurgery 44:34-39, 1999.
55. Brouwers PJAM, Westenberg HGM, van Gijn J: Noradrenaline con- centration and electrocardiographic abnormalities after aneurysmal subarachnoid hemorrhage. J Neurol Neurosurg Psychiatry 58:614, 1995.
56. Donaldson p, Pritz MB: Myocardial stunning secondary to aneurysmal subarachnoid hemorrhage. Surg Neurol 55:12-16, 2001.
57. Hamann G, Haass A, Schimrigk K: Beta blockade in acute aneurys- mal subarachnoid hemorrhage. Acta Neurochir (Wien) 121:119, 1993.
58. Neil-Dwyer G, Walter P, Cruikshank JM: Effect of propranolol and phentolamine on myocardial necrosis after subarachnoid hemor- rhage. Br Med J 2:990, 1978.
59. Levy ML, Rabb CH, Zelman V, Giannotta S L Cardiac performance enhancement from dobutamine in patients refractory to hyper- volemic therapy for cerebral vasospasm. J Neurosurg 79:494,1993.
60. Neil-Dwyer G, Walter P, Shaw HJH: Plasma renin activity in patients after a subarachnoid hemorrhage: A possible predictor of outcome. Neurosurgery 7:578, 1980.
61. Toftdahl DB, Torp-Pedersen C, Engel UH: Hypertension and left ventricular hypertrophy in patients with spontaneous subarachnoid hemorrhage. Neurosurgery 37:235, 1995.
62. Nibbelink DW: Considerations in the treatment of stroke: Cooper- ative Aneurysm Study: Antihypertensive and antifibrinolytic therapy following subarachnoid hemorrhage from ruptured intracranial aneurysm. In Whisnant JP, Sandok BA (eds): Cerebral Vascular Diseases. Orlando, Grune ti Stratton, 1975, p 155.
63. Wijdicks EFM, Vermuelen M, Ten Haaf JA: Volume depletion and natriuresis in patients with ruptured intracranial aneurysm. Ann Neurol 18:211-216, 1985.
64. Wijdicks EFM, Vermuelen M, Hijdra A: Hyponatremia and cere- bral infarction in patients with ruptured intracranial aneurysms: Is fluid restriction harmful? Ann Neurol 17:137-140, 1985.
65. Harrigan MR: Cerebral salt wasting syndrome. Crit Care Clin 17:125-138, 2001.
66. Sviri GE, Feinsod M, Soustiel JF: Brain natriuretic peptide and cerebral vasospasm in subarachnoid hemorrhage: Clinical and TCD correlations. Stroke 313118-122, 2000.
67. Wijdicks EF, Schievink WI, Burnett JC Jr: Natriuretic peptide system and endothelin in aneurysmal subarachnoid hemorrhage. J Neurosurg 87:275-280, 1997.
68. Sat0 K, Karibe H, Yoshimoto T: Circulating blood volume in patients with subarachnoid haemorrhage. Acta Neurochir 141: 1069-1073, 1999.
69. Carlotti APCP, Bohn D, Rutka JT, et al: A method to estimate urinary electrolyte excretion in patients at risk for developing cere- bral salt wasting. J Neurosurg 95:420424,2001.
70. Nibbelink DW, Torner JC, Burmeister LF: Fluid restriction in combination with antifibrinolytic therapy. In Sahs AL, Nibbelink DW, Torner JC (eds): Aneurysmal Subarachnoid Hemorrhage. Baltimore, Urban & Schwarzenberg, 1981, p 307.
71. van Gijn J, Rinkel GJE: Subarachnoid haemorrhage: Diagnosis, causes and management. Brain 124:249-278, 2001.
72. Diringer MN, Wu KC, Verbalis VG: Hypervolemic therapy prevents volume contraction but not hyponatremia following subarachnoid hemorrhage. Ann Neurol31:543-550, 1992.
73. Wijdicks EFM, Vermuelen M, Van Brummelen P The effect of flu- drocortisone acetate on plasma volume and natriuresis in patients with aneurysmal subarachnoid hemorrhage. Clin Neurol Neurosurg 90:209-214, 1988.
74. Qureshi AI, Suarez JI: Use of hypertonic saline solutions in treat- ment of cerebral edema and intracranial hypertension. Crit Care Med 28:33013313,2000.
75. Suarez JI, Qureshi AI, Parekh PD, et al: Administration of hyper- tonic (3%) sodium chloride/acetate in hyponatremic patients with symptomatic vasospasm following subarachnoid hemorrhage. J Neurosurg Anesthesiol 11:178-184, 1999.
76. Nowak G, Schwachenwald R, Arnold H: Early management in poor grade aneurysm patients. Acta Neurochir (Wien) 126:33, 1994.
77. Stachnick JB, Layon AJ, Day AL, Gdagher J: Craniotomy for intracranial aneurysm and subarachnoid hemorrhage: Is course, cost or outcome affected by age? Stroke 27:276, 1996.
78. Montes J, Wong J, Fayad P, Awad IA Stereotactic computed tomographic-guided aspiration and thrombolysis of intracerebral hematoma: Protocol and preliminary experience. Stroke 31:834- 840,2000.
79. Nieuwkamp DJ. de Gans K, Rinkel GJ, Algra A: Treatment and outcome of severe intraventricular extension in patients with sub- arachnoid or intracerebral hemorrhage: A systematic review of the literature. J Neurol247:117-121, 2000.
80. Shimoda M, Oda S, Shibata M, et al: Results of early surgical evacuation of packed intraventricular hemorrhage from aneurysm rupture in patients with poor-grade subarachnoid hemorrhage. J Neurosurg 91:408-414, 1999.
81. Sheehan JP, Polin RS, Sheehan JM, et al: Factors associated with hydrocephalus after aneurysmal subarachnoid hemorrhage. Neuro- surgery 45:112&1127, 1999.
82. Gr&-Radford NR, Torner J, Adams HP Jr: Factors associated with hydrocephalus after subarachnoid hemorrhage: A report of the Cooperative Aneurysm Study Arch Neurol46744-752, 1989.
83. Heros RC: Acute hydrocephalus after subarachnoid hemorrhage. Stroke 20:715, 1989.
84. Hasen D, Vermeulen M, Wijdicks EFM: Management problems in acute hydrocephalus after subarachnoid hemorrhage. Stroke 20747, 1989.
85. Hillman J, von Essen C, Leszniewski W, Johansson I: Significance of “ultra-early’’ rebleeding in subarachnoid hemorrhage. J Neurosurg 68401, 1988.

394 Stroke: Patbopbysiology, Diagnosis, and Management
86. Roos YB, Beenen LF, Groen RJ, et al: Timing of surgery in patients with aneurysmal subarachnoid haemorrhage: Rebleeding is still the major cause of poor outcome in neurosurgical units that aim at early surgery. J Neurol Neurosurg Psychiatry 63:49C493, 1997.
87. Torner JC, Kassell NF, Wallace RB: Preoperative prognostic factors for rebleeding and survival in aneurysm patients receiving fibrinolyhc therapy: Report of the Cooperative Aneurysm Study Neurosurgery 9:50&513, 1981.
88. Fujii Y, Takeuchi S, Sasaki 0: Ultra-early rebleeding in spontaneous subarachnoid hemorrhage. Neurosurgery 84:3542, 1996.
89. Steiger HJ, Fritschi J, Seiler RW: Current pattern of in-hospital aneurysmal rebleeds. Acta Neurochir (Wien) 127:21, 1994.
90. Perret GE, Nibbelink DW: Randomized treatment study: Carotid ligation. In Sahs AL, Nibhelink DW, Torner JC (eds): Aneurysmal Subarachnoid Hemorrhage. Baltimore, Urban & Schwamenberg, 1981, p 121.
91. Brown JA, Wollmann RL, Mullan S: Myopathy induced by epsilon-aminocaproic acid. J Neurosurg 57:130, 1983.
92. Kassell NF, Torner JC, Adams HP Jr: Antifibrinolytic therapy in the acute period following aneurysmal subarachnoid hemorrhage: Preliminary observations from the Cooperative Aneurysm Study. J Neurosurg 61:225230, 1984.
93. Vermuelen M, Lindsay Kw, Murray GD: Antifibrinolytic treatment in subarachnoid hemorrhage. N Engl J Med 311:432437, 1984.
94. Stroobandt G, Lambert 0, Meuard E: The association of tranex- amic acid and nimodipine in the pre-operative treatment of rup- tured intracranial aneurysms. Acta Neurochir 140: 148-160, 1998.
95. Rms Y: Antifibrinolytic treatment in subarachnoid hemorrhage: A randomized placebo-controlled trial. STAR Study Group. Neurol- ogy 54:77-82,2000.
96. Rms YB, Rinkel GJ, Vermeulen M , et al. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev CD00124, 2000.
97. Roos YB, Vermeulen M, Rinkel GJ, et al: Systematic review of antifibrinolytic treatment in aneurysmal subarachnoid haemor- rhage. J Neurol Neurosurg Psychiatry 65:942-943, 1998.
98. Maurice-Williams RS, Wadley JP: Delayed surgery for ruptured intracranial aneurysms: A reappraisal. Br J Neurosurg 11:10&109, 1997.
99. Juvela S, Kaste M, Hillbom M: The effects of earlier surgery and shorter bedrest on the outcome in patients with subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry 52:776, 1989.
100. LeRoux PD, Elliott JP, Downey L: Improved outcomes after rupture of anterior circulation aneurysms: A retrospective 10-year review of 224 good-grade patients. J Neurosurg 83:394, 1995.
101. Nishmoto A, Veta K, Onbe H: Nationwide cooperative study of intracranial aneurysm surgery in Japan. Stroke 16:48, 1985.
102. Ohman J, Heiskanen 0: Timing of operation for ruptured supra- tentorial aneurysms: A prospective randomized study J Neurosurg 7055, 1989.
103. Miyaoka M, Sat0 K, Ishii S: A clinical study of the relationship of timing to outcome of surgery for ruptured cerebral aneurysms: A retrospective analysis of 1,622 cases. J Neurosurg 79:373-378, 1993.
104. Kassell NF, Torner JC, Haley EC: The International Cooperative Study on the Timing of Aneurysm Surgery. 11: Surgical results. J Neurosurg 73:3436, 1990.
105. Kassell NF, Torner JC, Haley EC: The International Cooperative Study on the Timing of Aneurysm Surgery. I: Overall management results. J Neurosurg 73:18-33, 1990.
106. Deruty R, Mottolese C, Pecisson-Guyotat I, Soustiec JF: Manage- ment of the ruptured intracranial aneurysm: Early surgery, late surgery, or modulated surgery. Acta Neurochir (Wien) 11%3:1, 1991.
107. Larson JJ, Tew JM Jr, Tomsick T: Treatment of aneurysms of the internal carotid artery by intravascular balloon occlusion: Long-term follow-up of 58 patients. Neurosurgery 36:23-30, 1995.
108. Kinugasa K, Mandai S, Kamata I: Prophylactic thrombosis to prevent new bleeding and to delay aneurysm surgery, Neurosurgery 36:661, 1995.
109. McDougall CG, Halbach W, Dowd CF: Endovascular treatment of basilar tip aneurysms using electrolytically detachable coils. J Neurosurg 84:393, 1996.
110. Casasco AE, Aymard A, Gobin P: Selective endovascular treatment of 71 intracranial aneurysms with platinum coils. J Neurosurg 79:3, 1993.
111. Sinson G, Philips MF, Flamm ES: Intraoperative endovascular surgery for cerebral aneurysm. J Neurosurg 84:63, 1996.
112. Birchall D, Khangure M, McAuliffe W, et al: Endovascular treat- ment of posterior circulation aneurysms. Br J Neurosurg 153-3, 2001.
113. Eskndge J, Song J: Endovascular embolization of 150 basilar tip aneurysms with Guglielmi detachable coils: Results of the Food and Drug Administration multicenter clinical trial. J Neurosurg 89:81-86, 1998.
114. Cognard C, Weill A, Castings L, et al: Intracranial berry aneurysms: Angiographic and clinical results after endovascular treatment. Radiology 206:499510, 1998.
115. Raymond J, Roy D: Safety and efficacy of endovascular treatment of acutely ruptured aneurysms. Neurosurgery 41:12351245, 1997.
116. Lefkowitz MA, Gobin UP, Akiba Y, et al: Balloon-assisted Guglielmi detachable coiling of wide-necked aneurysms: Part II-clinical results. Neurosurgery 45531-537, 1999.
117. Treggiari-Venzi MM, Suter PM, Romand JA: Review of medical prevention of vasospasm after aneurysmal subarachnoid hemor- rhage: A problem of neurointensive care. Neurosurgery 48:249-261, 2001.
118. Smith RR, Clower BR, Grotendorst GM: Arterial wall changes in early human vasospasm. Neurosurgery 16: 171, 1985.
119. Dietrich HH, Dacey RG Jr: Molecular keys to the problems of cerebral vasospasm. Neurosurgery 46:517-530, 2000.
120. Nagatani K, Masciopinto J, Letarte PB: The effect of hemoglobin and its metabolites on energy metabolism in cultured cerebrovas- cular smooth-muscle cells. J Neurosurg 82:244, 1995.
121. Pasqualin A: Epidemiology and pathophysiology of cerebral vaso- spasm following subarachnoid hemorrhage. J Neurosurg Sci 42: 15-21, 1998.
122. IIirashima Y, Endo S, Ohinori T: Platelet-activating factor (PAF) concentration and PAF acetylhydrolase activity on cerebrospinal fluid of patients with subarachnoid hemorrhage. J Neurosurg 80:31, 1994.
123. Gaetani P, Rodriguez Y, Baena R: Endothelin and aneurysmal sub- arachnoid hemorrhage: A study of subarachnoid cistemal cere- brospinal fluid. J Neurol Neurosurg Psychiatry 66:57, 1994.
124. Pickard JD, Walker V, Brandt L: Effect of intraventricular haemor- rhage and rebleeding following subarachnoid haemorrhage on CSF eicosanoids. Acta Neurochir (Wien) 129:152, 1994.
125. Seifert V, Loffler BM, Zimmerman M, et al: Endothelin concentra- tions in patients with aneurysmal subarachnoid hemorrhage: Correlation with cerebral vasospasm, delayed ischemic neurologic defects and volume of hematoma. J Neurosurg 82:55, 1995.
126. Yundt KD, Gruhb RL Jr, Diringer M N , Powers WJ: Autoregulatory vasodilation of parenchymal vessels is impaired during cerebral vasospasm. J Cereb Blood Flow Metab 18:419424, 1998.
27. Shimoda M, Oda S, Tsugane R, Sat0 0: Prognostic Factors in delayed ischaemic deficit with vasospasm in patients undergoing early aneurysm surgery. Br J Neurosurg 11:210-215, 1997.
28. Charpentier C, Audibert 6, Guillemin F, et al: Multivariate analy- sis of predictors of cerebral vasospasm occurrence after aneurysmal subarachnoid hemorrhage. Stroke 30:140%1408, 1999.
29. Hop JW, Rinkel GJ, Algra A, van Gijn J: Initial loss of consciousness and risk of delayed cerebral ischemia after aneurysmal subarach- noid hemorrhage. Stroke 30:2268-2271, 1999.
30. Qureshi AI, Sung GY, Razumovsky AY, et al: Early identification of patients at risk for symptomatic vasospasm after aneurysmal sub- arachnoid hemorrhage. Crit Care Med 28:984990, 2000.
131. Juvela S: Aspirin and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. J Neurosurg 82:945, 1995.
132. Hop JW, Rinkel GJ, Algra A, et al: Randomized pilot trial of postoperative aspirin in subarachnoid hemorrhage. Neurology 54:872-878, 2000.
133. Claassen J, Bernardmi GL, Kreiter K, et al: Effect of cisternal and ventricular blood on risk of delayed cerebral ischemia after sub- arachnoid hemorrhage: The Fisher Scale revisited. Stroke 32:2012- 2020,2001.
134. Fisher CM, Kistler JP, Davis JM: Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery 6:l-9, 1982.
135. Conway JE, Tamargo RJ: Cocaine use is an independent risk factor for cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Stroke 32:2338-2343, 2001.
136. Fisher CM, Roberson GH, Ojemann RG: Cerebral vasospasm with ruptured saccular aneurysm: The clinical manifestations. Neurosurgery 1:245, 1977.

Chapter 14: Aneurysmal Subarachnoid Hemorrhaae 395
137. Rajendran JG, Lewis DH, Newell DW, Winn HR: Brain SPECT used to evaluate vasospasm after subarachnoid hemorrhage: Corre- lation with angiography and transcranial Doppler. Clin Nucl Med 26:125-130, 2001.
138. Grosset DG, Straiton J, McDonald I: Angiographic and Doppler diagnosis or cerebral artery vasospasm following subarachnoid hemorrhage. Br J Neurosurg 7:291-298, 1993.
139. Laumer R, Steinmeier R, Gonner F: Cerebral hemodynamics in subarachnoid hemorrhage evaluated by transcranial Doppler sonog- raphy. Neurosurgery 33:ll-18, 1993.
140. Boecher-Schwarz HG, Ungersboeck K, Ulrich P, et al: Transcranial Doppler diagnosis of cerebral vasospasm following subarachnoid haemorrhage: Correlation and analysis of results in relation to the age of patients. Acta Neurochir (Wien) 127:32, 1994.
141. Ekelund A, Saveland H, Romner B: Transcranial Doppler ultra- sound in hypertensive versus normotensive patients after aneurys- mal subarachnoid hemorrhage. Stroke 26:2071-2074, 1995.
142. Giller CA, Purdy P, Giller A Elevated transcranial Doppler ultra- sound velocities following therapeutic arterial dilation. Stroke 26:123-127, 1995.
143. Steinmeier R, Laumer R, Bondar I: Cerebral hemodynamics in sub- arachnoid hemorrhage evaluated by transcranial Doppler sonogra- phy. Part 2: Pulsatility indices: Normal reference values and characteristics in subarachnoid hemorrhage. Neurosurgery 33:10, 1993.
144. Brinker T, Seifert V, Dietz H: Subacute hydrocephalus after exper- imental subarachnoid hemorrhage: Its prevention by intrathecal fibrinolysis with recombinant tissue plasminogen activator. Neurosurgery 31:306, 1992.
145. Mizoi K, Yoshimoto T, Takahashi A Prospective study on the pre- vention of cerebral vasospasm by intrathecal fibrinolytic therapy with tissue type plasminogen activator. J Neurosurg 78:430, 1993.
146. Sasaki T, Ohta T, Kikuchi H: A phase I1 clinical trial of recombinant human tissue-type plasminogen activator against cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Neuro- surgery 35:597-605, 1994.
147. Usui M, Saito N, Hoya K, Todo T Vasospasm prevention with post- operative intrathecal thrombolyhc therapy: A retrospective com- parison of urokinase, tissue plasminogen activator, and cistemal drainage alone. Neurosurgery 34:235, 1994.
148. Kodama N, Sasaki T, Kawakami M, et al: Cisternal imgation therapy with urokinase and ascorbic acid for prevention of vasospasm after aneurysmal subarachnoid hemorrhage: Outcome in 217 patients. Surg Neurol53:110-117, 2000.
149. Allen AS, Ahn HS, Preziosi TJ: Cerebral arterial spasm-a con- trolled trial of nimodipine in patients with subarachnoid hemor- rhage. N Engl J Med 308:619, 1983.
150. Ohman J, Servo A, Heiskanen 0: Long-term effects of nimodipine on cerebral infarcts and outcome effects after aneurysmal sub- arachnoid hemorrhage and surgery. J Neurosurg 74:8, 1991.
151. Pickard JD, Murray GD, Illingworth R: Effect of oral nimodipine on cerebral infarction and outcome after subarachnoid haemor- rhage: British Aneurysm Nimodipine Trial. Br Med J 298:63fX42, 1989.
152. Barker FGI, Ogilvy CS: Efficacy of prophylactic nimodipine for delayed ischemic deficit after subarachnoid hemorrhage: A meta-analysis. J Neurosurg 84:405414, 1996.
153. Feigin VL, Rinkel GJ, Algra A, et al: Calcium antagonists for aneurysmal subarachnoid haemorrhage. Cochrane Database Syst Rev CD000277,2000.
154. Tettenbom D, Dycka J: Prevention and treatment of delayed ischemic dysfunction in patients with aneurysmal subarachnoid hemorrhage. Stroke 21(Suppl):IV85, 1990.
155. Haley EC Jr, Kassell NF, Tomer JC: A randomized trial of nicardip- ine in subarachnoid hemorrhage: Angiographic and transcranial Doppler ultrasound results. A report of the Cooperative Aneurysm Study. J Neurosurg 78548553, 1993.
156. Haley EC Jr, Kassell NF, Torner JC, et al: A randomized, controlled trial of high-dose intravenous nicardipine in aneurysmal subarach- noid hemorrhage: A report of the Cooperative Aneurysm Study. J Neurosurg 78:537547, 1993.
157. Haley EC Jr, Kassell NF, Tomer JC, and the participants: A ran- domized trial of two doses of nicardipine in aneurysmal subarach- noid hemorrhage: A report of the Cooperative Aneurysm Study. J Neurosurg 80:788, 1994.
158. Shibuya M, Suzuki Y, Enomoto H: Effects of prophylactic intrathe- cal administration of nicardipine on vasospasm in patients with severe aneurysmal subarachnoid haemorrhage. Acta Neurochir (Wien) 131:19, 1994.
159. Effect of calcitonin-gene-related peptide in patients with delayed postoperative cerebral ischaemia after aneurysmal subarachnoid haemorrhage. European CGRP in Subarachnoid Hemorrhage Study Group. Lancet 339:831-834, 1992.
160. Clouston JE, Numaguchi Y, Zoarski GH: Intraarterial papaverine infusion for cerebral vasospasm after subarachnoid hemorrhage. Am J Neuroradiol 16:2, 1995.
161. Firlik KS, Kaufmann AM, Firlik AD, et al: Intra-arterial papaverine for the treatment of cerebral vasospasm following aneurysmal subarachnoid hemorrhage. Surg Neurol51:6&74, 1999.
162. Kaku Y, Yonekawa Y, Tsukahara T, Kazekawa K: Superselective intra-arterial infusion of papaverine for the treatment of cerebral vasospasm after subarachnoid hemorrhage. J Neurosurg 77:842, 1992.
163. Carhuapoma JR, Qureshi AI, Tamargo RJ, et al: Intra-arterial papaverine-induced seizures: Case report and review of the litera- ture. Surg Neurol56:159-163, 2001.
164. Arakawa Y, Kikuta K, Hojo M, et al: Milrinone for the treatment of cerebral vasospasm after subarachnoid hemorrhage: Report of seven cases. Neurosurgery 48:713-728, 2001.
165. Finfer SR, Ferch R, Morgan MK: Barbiturate coma for severe, refractory vasospasm following subarachnoid haemorrhage. Inten- sive Care Med 25:406-409, 1999.
166. Haley ECJ, Kassell NF, Apperson-Hansen C, et al: A randomized, double-blind, vehicle-controlled trial of tirilazad mesylate in patients with aneurysmal subarachnoid hemorrhage: A cooperative study in North America. J Neurosurg 86:467474, 1997.
167. Kassell NF, Haley EC Jr, Apperson-Hansen C: Randomized, double-blind, vehicle-controlled trial of tirilazad mesylate in patients with aneurysmal subarachnoid hemorrhage: A cooperative study in Europe, Australia, and New Zealand. J Neurosurg
168. Lanzino G, Kassell NF: Double-blind, randomized, vehicle- controlled study of high-dose tirilazad mesylate in women with aneurysmal subarachnoid hemorrhage. Part 11: A cooperative study in North America. J Neurosurg 90:10161024, 1999.
169. Kassell NF, Peerless SJ, Durward QJ, et al: Treatment of ischemic deficits from vasospasm with intravascular volume expansion and induced arterial hypertension. Neurosurgery 11:337-343, 1982.
170. Mori K, Arai H, Nakajima K: Hemorrheological and hemodynamic analysis of hypervolemic hemodilution therapy for cerebral vasospasm after aneurysmal subarachnoid hemorrhage. Stroke 26:1620-1626, 1995.
171. Egge A, Waterloo K, Sjoholm H, et al: Prophylactic hyperdynamic postoperative fluid therapy after aneurysmal subarachnoid hemorrhage: A clinical, prospective, randomized, controlled study. Neurosurgery 49:593-606, 2001.
172. Qureshi AI, Suarez JI, Bhardwaj A, et al: Early predictors of outcome in patients receiving hypervolemic and hypertensive therapy for symptomatic vasospasm after subarachnoid hemor- rhage. Crit Care Med 283824429,2000.
173. Lennihan L, Mayer SA, Fink ME, et al: Effect of hypervolemic therapy on cerebral blood flow after subarachnoid hemorrhage: A randomized controlled trial. Stroke 31:383-391, 2000.
174. Feigin VL, Rinkel GJ, Algra A, van Gijn J: Circulatory volume expansion for aneurysmal subarachnoid hemorrhage. Cochrane Database Syst Rev CD000483,2000.
175. Darby JM, Yonas H, Marks EC: Acute cerebral blood flow response to dopamine-induced hypertension after subarachnoid hemorrhage. J Neurosurg 80:857, 1994.
176. Oropello JM, Weiner L, Benjamin E: Hypertensive, hypervolemic, hemodilutional therapy for aneurysmal subarachnoid hemorrhage: Is it efficacious? No1 Crit Care Clin 12:709-730, 1996.
177. Ullman JS, Bedersom JB: Hypertensive hypervolemic, hemodilu- tional therapy for aneurysmal subarachnoid hemorrhage. Is it efficacious? Yes. Crit Care Clin 12:697-707, 1996.
178. Terada T, Komai N, Hayashi S: Hemorrhagic infarction after vasospasm due to ruptured cerebral aneurysm. Neurosurgery 18:415, 1986.
179. Shimoda M, Oda S, Tsugane R, Sat0 0: Intracranial complication of hypervolemic therapy in patients with a delayed ischemic deficit attributed to vasospasm. J Neurosurg 78:423, 1993.
84:221-221, 1996.

396 Stroke: Patbopbysiology, Diagnosis, and Management
180. Trumble ER, Muizelaar JP, Myseros JS: Coagulopathy with the use of hetastarch in the treatment of vasospasm. J Neurosurg 82:44, 1995. rhage. Neurosurgery 42:979-986, 1998.
181. C o p e TJ, Montanera WJ, Macdonald RL: Percutaneous translu- mind angioplasty for cerebral vasospasm after subarachnoid hemorrhage. Can J Surg 37:391396, 1994.
182. Honma Y, Fujiwara T, Irie K: Morphological changes in human cerebral arteries after percutaneous transluminal angioplasty for vasospasm caused by subarachnoid hemorrhage. Neurosurgery 36:1073, 1995.
183. Bejjani GK, Bank WO, Olan WJ, Sekhar LN: The efficacy and safety of angioplasty for cerebral vasospasm after subarachnoid hemor-
184. Polin RS, Coenen VA, Hansen CA, et al: Efficacy of transluminal angioplasty for the management of symptomatic cerebral vasospasm following aneurysmal subarachnoid hemorrhage. J Neurosurg 92: 284290,2000.
![Inflammation in human cerebral aneurysms: pathogenesis ... · aneurysmal subarachnoid hemorrhage (SAH) is higher in hypertensive patients, smokers, heavy drinkers, and females. [2,4]](https://img.dokumen.tips/doc/110x75/5ed55ef36933f508e973f11f/inflammation-in-human-cerebral-aneurysms-pathogenesis-aneurysmal-subarachnoid.jpg)


![Non-aneurysmal subarachnoid hemorrhage in a case of ... · associated with aneurysmal subarchnoid and intracranial hemorrhage [5]. In our case this was a primary subarchnoid hemorrhage](https://img.dokumen.tips/doc/110x75/5ed55eea6933f508e973f10c/non-aneurysmal-subarachnoid-hemorrhage-in-a-case-of-associated-with-aneurysmal.jpg)