Embed Size (px)
Citation preview

Available online at www.sciencedirect.com
ScienceDirect
Journal of Electrocardiology xx (2015) xxx – xxxwww.jecgonline.com
Smartphone ECG for evaluation of STEMI: Results of the ST LEUISPilot Study
Joseph Boone Muhlestein, MD, a, b Viet Le, PA, a David Albert, MD, c Fidela Ll. Moreno, MD, a
Jeffrey L. Anderson, MD, a, b Frank Yanowitz, MD, a, b Robert B. Vranian, MD, d
Gregory W. Barsness, MD, e Charles F. Bethea, MD, f Harry W. Severance, MD, g
Barry Ramo, MD, h John Pierce, MD, i Alejandro Barbagelata, j
Joseph Brent Muhlestein, MDa, b,⁎a Intermountain Heart Institute, Salt Lake City, UT
b The University of Utah, Department of Internal Medicine, Salt Lake City, UTc AliveCor™ Corporation, San Francisco, CA
d Mary Washington Hospital, Fredericksburg, VAe Mayo Clinic, Rochester, MN
f Integris Heart Hospital, Oklahoma City, OKg Erlanger Institute for Clinical Research, UT College of Medicine, Chattanooga, TN
h New Mexico Heart Institute, Albuquerque, NMi Duke University, Durham, NC
j Buenos Aires, Argentina
Abstract Background: 12-lead ECG is a critical component of initial evaluation of cardiac ischemia, but has
⁎ CorrespondingCottonwood Street, Sa
E-mail address:
http://dx.doi.org/10.100022-0736/© 2014 El
traditionally been limited to large, dedicated equipment inmedical care environments. Smartphones provide apotential alternative platform for the extension of ECG to new care settings and to improve timeliness of care.Objective: To gain experience with smartphone electrocardiography prior to designing a largermulticenter study evaluating standard 12-lead ECG compared to smartphone ECG.Methods: 6 patients for whom the hospital STEMI protocol was activated were evaluated with traditional12-lead ECG followed immediately by a smartphone ECG using right (VnR) and left (VnL) limb leads forprecordial grounding. The AliveCor™ Heart Monitor was utilized for this study. All tracings were takenprior to catheterization or immediately after revascularization while still in the catheterization laboratory.Results: The smartphone ECG had excellent correlation with the gold standard 12-lead ECG in allpatients. Four out of six tracings were judged to meet STEMI criteria on both modalities asdetermined by three experienced cardiologists, and in the remaining two, consensus indicated a non-STEMI ECG diagnosis. No significant difference was noted between VnR and VnL.Conclusions: Smartphone based electrocardiography is a promising, developing technology intended toincrease availability and speed of electrocardiographic evaluation. This study confirmed the potential of asmartphone ECG for evaluation of acute ischemia and the feasibility of studying this technology further todefine the diagnostic accuracy, limitations and appropriate use of this new technology.© 2014 Elsevier Inc. All rights reserved.
Keywords: ECG; STEMI; Heart attack; Myocardial infarction; Smartphone; iPhone; Ischemia
Introduction
Annually, one in six deaths is due to cardiovasculardisease. The American Heart Association has reported that405,309 Americans died of cardiovascular disease (CVD) in2008, and that annually an estimated 785,000 Americans
author at: Intermountain Heart Institute, 5121 Southlt Lake City, UT [email protected]
16/j.jelectrocard.2014.11.005sevier Inc. All rights reserved.
will experience a first time coronary event, 470,000 willsuffer a recurrent event, and 195,000 will have a silent firstmyocardial infarction[1].
Urgent revascularization is indicated in patients withST-elevation myocardial infarction (STEMI) which is diag-nosed largely on electrocardiographic criteria [2]. Themajorityof STEMI deaths occur within the first 1–2 hours [3]. Manybarriers have been identified preventing early recognition ofSTEMI including lack of the patient's ability to identify thatthey are experiencing an MI, misattributing symptoms of

2 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
STEMI to some other disease, fearing embarrassment of falsealarm, not fitting a “stereotype” for heart attack, and lack ofrecognition by bystanders of a STEMI event [3,4].
Given that earlier treatment of STEMI reduces mortalityand morbidity, it is important to increase the speed ofdiagnosing a STEMI event. As ECG is the method fordiagnosing STEMI and is also the most simple andaccessible diagnostic modality, it is possible that byextending the availability of reliable ECGs to a high-riskoutpatient population, delays to early recognition andsubsequent treatment could be reduced and more promptlifesaving revascularization achieved.
Smartphones provide a possible platform for the extensionof the ECG as they have become common across world,including poorer nations. A report on a 2012 survey by theNielsen group ofUSmobile consumers estimates that over halfof USmobile consumers use a smartphone or smart device [5].Smart devices do not have voice capability but are otherwisesimilar to smartphones with comparable hardware andsoftware. Differences exist among operating systems andhardware specifications, but a standard set of featuresincluding a touch screen, Internet connectivity and the abilityto run 3rd party applications have become ubiquitous.
With the development of smartphones, independentsoftware developers have created applications or “apps” formultiple uses. One such app works in tandem with a phonecase with embedded sensors and provides a single channellead for accurate rate and rhythm assessment [6,7]. Thisdevice has been shown capable of distinguishing betweennormal sinus rhythm and atrial fibrillation when used by atrained medical professional. The device has been validatedagainst 12-lead ECGs in a small number of patients foraccurately identifying atrial fibrillation with sensitivitiesfrom 87% to 100%, specificities from 90% to 97%, and totalaccuracies from 94% to 97%. The ECG readings includedindependent blinded assessments by three different cardiol-ogists as well as an automated algorithm analysis [8]. Morerecently, the device has been shown reliable in assessingQTC intervals compared to standard 12-lead ECG [9].
While this device has been shown to provide a singlechannel lead reading that is diagnostic for normal sinusrhythm and atrial fibrillation, it has not been validated in itsability to provide readings during an acute MI, includingtime sensitive STEMI events, for accurate assessment anddiagnosis at point of care or even patient-applied application.
Following the success of single lead smartphone basedrhythm evaluation, interest has developed in more compre-hensive electrocardiographic evaluation using smartphoneswhich can assess ischemic ST-T wave changes. A preliminarystudy was recently published using the original single leaddevice attached to typical 12-lead ECG leads and thencompared to a standard 12-lead reading. A non-acute patientpopulation was studied and the authors noted good concor-dance between the two modalities [10]. At present, a testdevice has been created with two wire leads, designed to beusedwith traditional ECG stickers and connect wirelessly witha smart device. It differs from a 12-lead ECG in that thetracings are taken serially rather than simultaneously, it usescomputer averaging to give a single representative tracing
rather than raw voltage data, and it uses a single extremity leadfor grounding of the precordial leads instead of an average.How these differences affect its ability to diagnosis STEMIand non-STEMI has not previously been determined.
Objectives
The primary objective of this study was to assess theoperational feasibility of using a smartphone to obtain“12-lead equivalent” ECG recordings in patients suspectedto have acute MI, with particular focus on STEMI. Our intentwas to use results from this pilot study to design a largermulti-center study, the objective of which is to determine ifthe smartphone ECG is an acceptable substitute for astandard ECG in the identification of STEMI.
Specific goals of this pilot study included: to obtainsimultaneous standard 12-lead ECG and the smartphone“12-lead equivalent” ECG recordings on patients for whomthe STEMI protocol was activated; to determine theoperational feasibility of obtaining these simultaneousrecordings; to make preliminary assessment of diagnosticaccuracy; to make recommendations for the conduct of theplanned multi-center study that will determine if thesmartphone ECG is an acceptable replacement for a standardECG in the identification of STEMI.
By validating the smartphone ECGs capacity to accuratelyassess the presence or absence of STEMI or non-STEMIcompared to gold standard 12-lead ECG, we may increase theaccessibility of electrocardiography and hasten the diagnosisand treatment of the life threatening events.
Materials and methods
This study was designed as a single center, prospective,non-randomized, open study,with a single-patient clinical design(i.e., the patients serve as their own control). Target enrollmentwas 5 patients and 6 patients were eventually enrolled over27 days. Inclusion criteria included age ≥18 years, ability ofpatient or legally-acceptable representative to provide writteninformed consent prior to study procedure, chest pain evaluatedin the emergency department, and activation of the STEMIprotocol based on clinical and preliminary ECG criteria.Exclusion criteria included inability to obtain legally-acceptableconsent or any condition that the principal investigator felt wouldincrease the risk to the patient or compromise the timing orquality of the trial. For inclusion, the smartphone ECG had to beobtained in the emergency department prior to revascularizationor in the catheterization laboratory before or after revasculari-zation, immediately following a comparison 12-lead ECG.
All smartphone ECGs were obtained by the research teamdirectly after being trained by the device company. Uponactivation of the STEMI protocol, the team was alerted andwent to evaluate and consent the patient as quickly as possible.One out of the six patients had consent and recordings taken inthe emergency department. All others were obtained in thecatheterization laboratory following revascularization.
The smartphone ECG was obtained following repeat12-lead ECG using the AliveCor™ Heart Monitor using aniPod Touch device with Wi-Fi connectivity (see Fig. 1). The

Fig. 1. AliveCor ™ Heart Monitor with 5th generation iPod Touch used forthis pilot study.
3J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
iPod Touch is a smart device running the iOS operatingsystem, similar to the iPhone smartphone. For this study,“smartphone ECG” and “smart device ECG” were consid-ered to be synonymous. The Heart Monitor was held near theiPod Touch to allow for a wireless connection. Electrodesattached to the AliveCor™ Heart Monitor were connected toECG stickers sequentially with a 15 second recordingobtained on each lead configuration. The tracings werewirelessly uploaded to the AliveCor™ servers where theywere processed with sequential averaging of QRS complexesand obtained by accessing their Web site and downloadingthe processed waveforms.
Two configurations were obtained for the precordialleads, VnL and VnR. VnL was obtained using the left armfor grounding and VnR with the right arm acting as ground.These were evaluated independently by the ECG reviewersalongside the gold standard 12-lead ECG.
The ECG reviewers comprised three experienced cardi-ologists who were provided no clinical context beyond theinclusion criteria of the study and tasked to evaluate theECGs based on waveform alone. Conflicting reads werediscussed among the reading panel and a consensus majoritywas achieved in each case to provide the final read of STEMIor not STEMI.
Table 1Characteristics of the six enrolled patients and description of reads.
Patient number Age Race Gender Time 12-lead read
P1 56 White Male 0931 Inferolateral MIP2 60 White Male 1410 Evolving inferior MIP3 64 White Male 1628 Marked precordial ST
depression suggesting posP4 62 White Male 2029 Diffuse non-specific ST cP5 85 White Male 1902 Evolving inferior-posterioP6 52 White Male 0846 Evolving anterior MI
Results
The study enrolled six patients for whom the STEMIprotocol was activated (Table 1). All 6 were white maleswith ages between 52 and 85 years. Expedited transfer to thecatheterization laboratory led to only one ECG beingobtained in the emergency department and all others beingperformed in the laboratory immediately post revasculariza-tion. All tracings obtained were felt to be of adequatetechnical quality for interpretation. Smartphone tracings andpaired 12-lead ECGs are shown in Figs. 2–14.
The reading panel found perfect correlation between thedifferent modalities with regard to STEMI criteria. FourECGs were judged to meet STEMI criteria and two did not inboth the 12-lead and smartphone ECG tracings. Three of thefour STEMI reads were inferior and one was anterior. Theother two reads were suggestive of myocardial ischemia butdid not meet STEMI criteria on either modality. See Table 1for full details of reads. All reads had a three out of threemajority after deliberation among the reading panel.
VnR and VnL were read separately for each patient. In allcases they were felt to provide similar diagnostic informationwith only minor, diagnostically irrelevant differences. In twopatients VnR was felt to be slightly closer to the 12-lead thanVnL, and in one VnL was felt to be slightly closer (seeTable 1). No differences noted were sufficient to changewhether or not the ECG met STEMI criteria.
Discussion
This study importantly demonstrates that the smartphoneECG is capable of identifying an ST-segment myocardialinfarction using a technology platform that is now readilyavailable. The significance of this lies in its ability to extendelectrocardiographic evaluation into new use case scenarios,including personalized use by the owner or point-of-care,out-of-hospital first medical contact. These and otherimportant scenarios include settings where a standard12-lead ECG is not immediately available. Settings ofparticular need include rural areas with no nearby medicalfacilities, developing nations and regions, and travelscenarios such as cruise ships and tour buses. It would beunfeasible to provide standard 12-lead ECG devices in suchsettings, but smartphone penetration has already becomecommonplace and has the potential to provide a foundation
Correlation of 12-leadwith smartphone ECG
VnR vs VnL(compared to 12-lead
Excellent R = LExcellent R N L
terior ischemia, not MIGood R = L
hanges, not MI Good R b Lr MI Excellent R b L
Good R N L
)

Fig. 2. Subject P1: 12-lead ECG obtained just prior to smartphone ECG during a STEMI activation. This 12-lead ECG was read as concordant with thesmartphone ECGs. This was read as an inferolateral STEMI.
4 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
for the greater spread of electrocardiography.Additionally, hospitals and clinicswhereECGsmay already be
available might have increased penetration with this technologyallowing for prompt electrocardiographic evaluation without theexpense of additional dedicated ECG machines and staff.
There are limitations to this study. It was a small, white maleonly population at a single center. It did not extensively evaluateother, non-STEMI clinical settings. All but one patient hadtracings performed following revascularization. It used onlytrained individuals to perform the recordings and used prototypehardware. The device was somewhat cumbersome with longleads attached, and ECG stickers were required.
However, the excellent quality of tracings obtained (as notedabove), and the 100% correspondence between 12-lead andsmartphone ECG readings, are promising and encouraging. Thediscrepancies noted were subtle and not diagnosticallyimpactful. Reading cardiologists noted that concordance wasalways at least “good” and typically “excellent.” Possibleexplanations for minor differences include the small time delayrequired to perform the smartphone ECG, the averagingtechnique used in processing, and using a single groundinglead for the precordial measurements. Improvements in futureprototypes to allow for more rapid measurement as well as alarger study populationwill help furtherminimize the sources ofthese minor differences.
As the study could not interfere with the revascularizationprocess and the catheterization laboratory efficiency in treatingthese STEMI patients, all but one of the tracings were obtainedin the lab post revascularization. Since the evolution of ECGfindings is rapid after reperfusion, this may have limited thenumber of cases with truly acute STEMI findings. More oftenan evolving/resolving pattern was noted. However, concor-dance was not affected since a comparison ECGwas taken justprior to the smartphone ECG.
The amount of training to adequately perform smartphoneECGs is still unclear. This study used research associates whohad been trained by the device company to perform allrecordings. A previous study with a related product found thatreceptionists were uncomfortable performing a single leadrecording, whereas nursing staff were much more comfortable[11]. With the added complexity of obtaining a morecomplicated 12-lead tracing, the ability for this technology tobe utilized by non-medical personnel requires further study.
Looking to more widespread adoption, there are severaltechnological questions that should be addressed. Thecurrent implementation uses a remote server for processingthat requires an active Internet connection. Local processingon the smartphone would allow a tracing to be obtainedwithout an active Internet connection. A 15 second read oneach lead was required with the current implementation.Local processing could also allow for a lead to be attachedonly long enough for an accurate tracing, with the deviceproviding a signal when an adequate read is obtained andindicating when the leads can be advanced to the nextposition. Additionally, no automated reading is availablewithin the present system. Whether it would be beneficial tohave an automated read, with the inherent potential for errorbut potentially a much quicker response, or rely solely onremote expert readers, was not addressed in this study. Thecurrent technological iteration relies on traditional ECGstickers and leads with clips. A device not requiring stickersand leads also may facilitate more general adoption.
With these limitations of our current study in mind, we arecurrently planning a multi-center study to further evaluatethe concordance of smartphone ECG compared to 12-leadECG. The intention is to evaluate 100 patients for whom theSTEMI protocol is activated and 200 additional patients whopresent to the emergency department with a chief complaint

Fig. 4. VnL, smartphone ECG using the left arm for grounding. Tracing wastaken just following 12-lead ECG seen in Fig. 2.
Fig. 3. Subject P1: VnR, smartphone ECG using the right arm for grounding.Tracing was taken just following 12-lead ECG seen in Fig. 2.
5J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
of chest pain. The intent will be to verify the findings of thepilot study on a larger, more heterogeneous population, toextend the study to patients for whom the STEMI protocolwas not activated, and to assess overall diagnostic accuracyin a more general chest pain population.
Several modifications to the pilot protocol will be considered.Given the difficulty in obtaining research tracings prior torevascularization, we may look to include clinical staff such asECG technicians or emergency department nurses or aides toacquire some of the tracings. Additionally, given the excellentconcordance betweenVnRandVnL and the added time and effortrequired to obtain the separate tracings,wewill likely proceedwithVnR serving as the sole smartphone precordial measurement.
Conclusions
The AliveCor™ Heart Monitor, a smartphone device-basedECG system was found to generate “12-lead equivalent” ECGsthat demonstrated excellent concordance with standard 12-leadECGs for the detection of STEMI as well as non-STEMI
ischemic changes. These pilot results suggest that a low cost,convenient alternative to existing ECG technology using nowcommon smartphones and other smart electronic devices mayextend the availability of ECG beyond its current reach andfacilitate the early detection of STEMI (and possibly non-STEMI), including personalized use by the owner or bypoint-of-care, out-of-hospital first medical contact. The promiseof smart device diagnosis of acute coronary syndromes deservesfurther evaluation in larger, multi-center studies.
Acknowledgments
Funding: Funds for this study were provided by AliveCor,Inc. in the form of an unrestricted research grant and byproviding the research device along with device training.AliveCor, Inc. did not contribute to the study design orexecution, data analysis, manuscript preparation, or thedecision to submit the manuscript for publication. Theauthors take full responsibility for manuscript content.
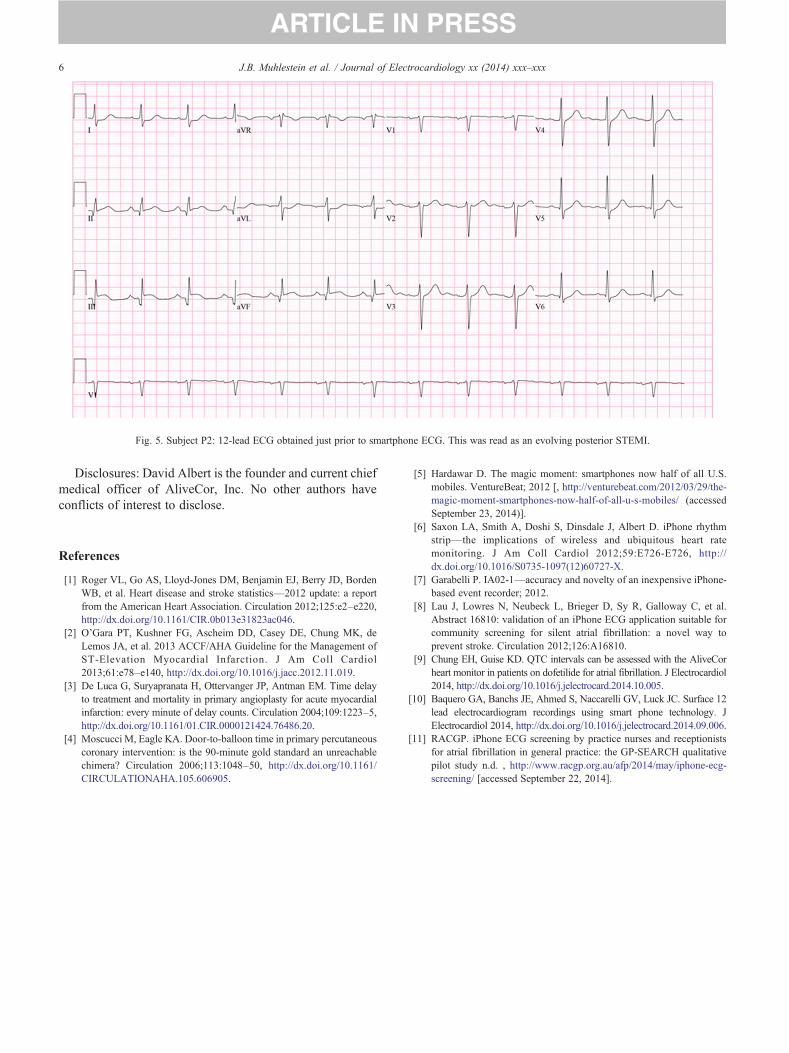
Fig. 5. Subject P2: 12-lead ECG obtained just prior to smartphone ECG. This was read as an evolving posterior STEMI.
6 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
Disclosures: David Albert is the founder and current chiefmedical officer of AliveCor, Inc. No other authors haveconflicts of interest to disclose.
References
[1] Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, BordenWB, et al. Heart disease and stroke statistics—2012 update: a reportfrom the American Heart Association. Circulation 2012;125:e2–e220,http://dx.doi.org/10.1161/CIR.0b013e31823ac046.
[2] O’Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, deLemos JA, et al. 2013 ACCF/AHA Guideline for the Management ofST-Elevation Myocardial Infarction. J Am Coll Cardiol2013;61:e78–e140, http://dx.doi.org/10.1016/j.jacc.2012.11.019.
[3] De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delayto treatment and mortality in primary angioplasty for acute myocardialinfarction: every minute of delay counts. Circulation 2004;109:1223–5,http://dx.doi.org/10.1161/01.CIR.0000121424.76486.20.
[4] Moscucci M, Eagle KA. Door-to-balloon time in primary percutaneouscoronary intervention: is the 90-minute gold standard an unreachablechimera? Circulation 2006;113:1048–50, http://dx.doi.org/10.1161/CIRCULATIONAHA.105.606905.
[5] Hardawar D. The magic moment: smartphones now half of all U.S.mobiles. VentureBeat; 2012 [, http://venturebeat.com/2012/03/29/the-magic-moment-smartphones-now-half-of-all-u-s-mobiles/ (accessedSeptember 23, 2014)].
[6] Saxon LA, Smith A, Doshi S, Dinsdale J, Albert D. iPhone rhythmstrip—the implications of wireless and ubiquitous heart ratemonitoring. J Am Coll Cardiol 2012;59:E726-E726, http://dx.doi.org/10.1016/S0735-1097(12)60727-X.
[7] Garabelli P. IA02-1—accuracy and novelty of an inexpensive iPhone-based event recorder; 2012.
[8] Lau J, Lowres N, Neubeck L, Brieger D, Sy R, Galloway C, et al.Abstract 16810: validation of an iPhone ECG application suitable forcommunity screening for silent atrial fibrillation: a novel way toprevent stroke. Circulation 2012;126:A16810.
[9] Chung EH, Guise KD. QTC intervals can be assessed with the AliveCorheart monitor in patients on dofetilide for atrial fibrillation. J Electrocardiol2014, http://dx.doi.org/10.1016/j.jelectrocard.2014.10.005.
[10] Baquero GA, Banchs JE, Ahmed S, Naccarelli GV, Luck JC. Surface 12lead electrocardiogram recordings using smart phone technology. JElectrocardiol 2014, http://dx.doi.org/10.1016/j.jelectrocard.2014.09.006.
[11] RACGP. iPhone ECG screening by practice nurses and receptionistsfor atrial fibrillation in general practice: the GP-SEARCH qualitativepilot study n.d. , http://www.racgp.org.au/afp/2014/may/iphone-ecg-screening/ [accessed September 22, 2014].

Fig. 6. Subject P2: VnR, smartphone ECG using the right arm for grounding.Tracing was taken just following 12-lead ECG seen in Fig. 5.
7J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx

Fig. 7. Subject P3: 12-lead ECG obtained just prior to smartphone ECG. This was read as posterior ischemia not meeting STEMI criteria.
8 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx

Fig. 8. Subject P3: VnR, smartphone ECG using the right arm for grounding.Tracing was taken just following 12-lead ECG seen in Fig. 7.
9J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
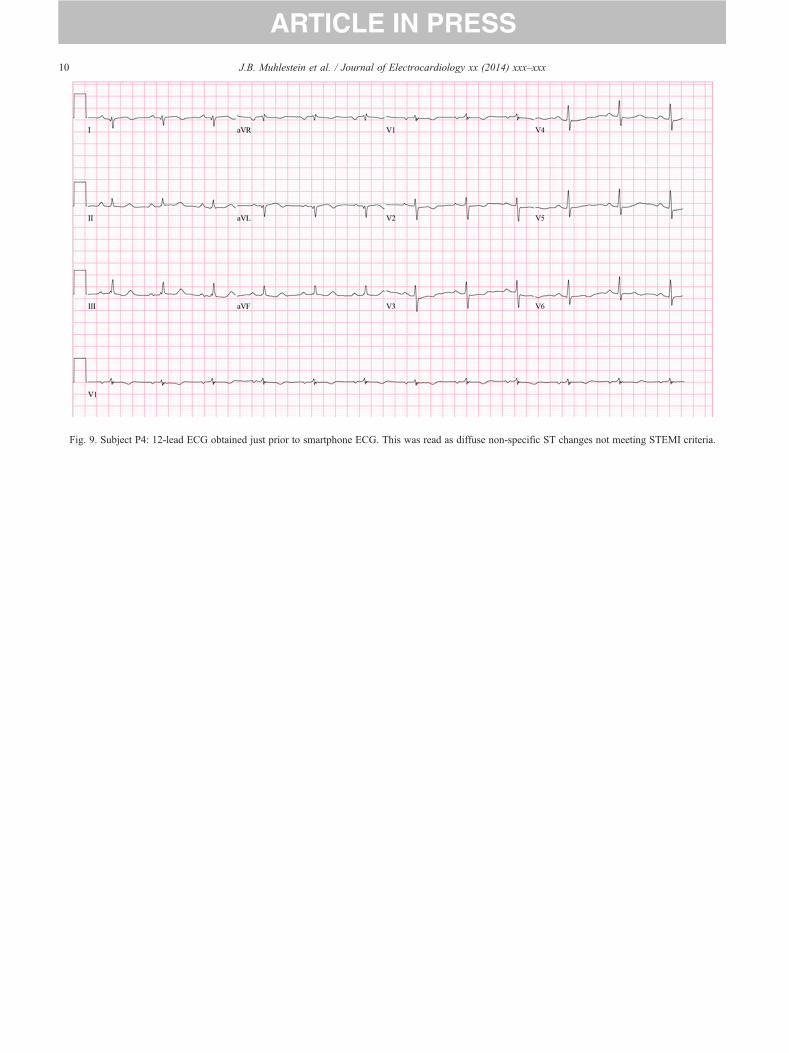
Fig. 9. Subject P4: 12-lead ECG obtained just prior to smartphone ECG. This was read as diffuse non-specific ST changes not meeting STEMI criteria.
10 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx

Fig. 10. Subject P4: VnR, smartphone ECG using the right arm forgrounding. Tracing was taken just following 12-lead ECG seen in Fig. 9.
11J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx

Fig. 11. Subject P5: 12-lead ECG obtained just prior to smartphone ECG. This was read as an evolving inferior-posterior STEMI.
12 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx

Fig. 12. Subject P5: VnR, smartphone ECG using the right arm forgrounding. Tracing was taken just following 12-lead ECG seen in Fig. 11.
13J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx
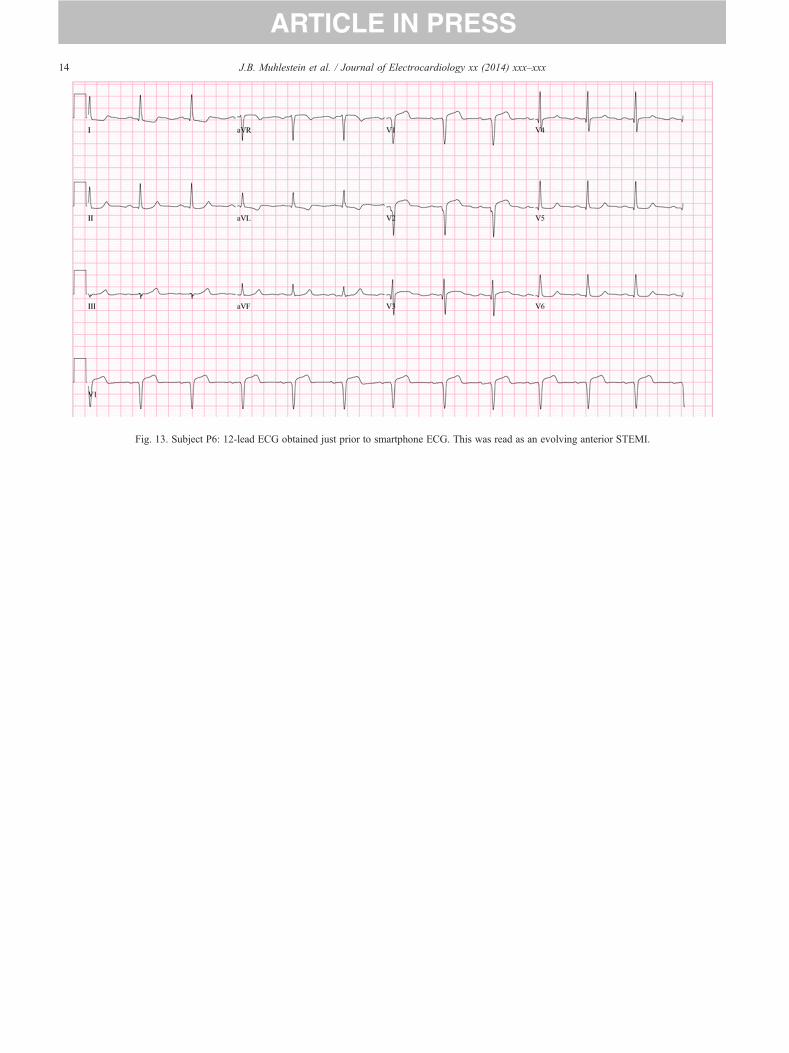
Fig. 13. Subject P6: 12-lead ECG obtained just prior to smartphone ECG. This was read as an evolving anterior STEMI.
14 J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx

Fig. 14. Subject P6: VnR, smartphone ECG using the right arm forgrounding. Tracing was taken just following 12-lead ECG seen in Fig. 13.
15J.B. Muhlestein et al. / Journal of Electrocardiology xx (2014) xxx–xxx





























