Embed Size (px)
Citation preview

Skilled Care at BirthExperience from Afghanistan
Women Deliver Conference June -7-9- 2010
Pashtoon Azfar, PresidentAfghan Midwives Association (AMA)

2
Presentation Outline
• Overview of the context and challenges• Overview of the methods employed to address the challenge
– Creating the policy environment– Establishing an accreditation system– Estimating needs and employing a workforce planning approach– Ensuring quality education
• Ensuring deployment, supervision and support• AMA and its role in:
– Strengthening Midwifery Profession– Improving maternal Health in Afghanistan– Results and Achievements
• Remaining challenges• Lessons learned and recommendations

3
The challenges – after 23 years conflict
Challenging Health Indicators: Maternal Mortality Ratio
– 1,600 / 100,000
Neonatal Mortality – 60/1000 live births– Less than 9% of deliveries
attended by SBA
Few female health workers– 467 midwives in 2002– 21% health facilities had female
staff– Socio-cultural demand for female
providers

4
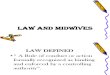
Maternal Health in Afghanistan
• Estimated 26,000 women dying from pregnancy related causes per year
• 1 woman dying every 27 minutes
• 78% of deaths are preventable
38%
26%
10%
5%
4%
9%
8%
Haemorrhage
Obstruction
PIH
Sepsis
Other direct
Indirect
Unclear
Source: Bartlett et al 2005

5
Policy Environment
• Development of Basic Package of Health Services
• Maternal mortality reduction strategy included improving coverage of SBA and an Intrapartum care strategy
• Policy statement on cessation of TBA training issued (2003); focus on training SBAs
• Midwifery curriculum existed; out of date, focused on training midwives for hospitals

6
Creating the Policy Environment
GOAL: To prepare qualified and competent midwives, to work in underserved areas of Afghanistan•Competency-based curriculum and
training materials developed • midwives job description developed (2004) •18-month competency-based curriculum re-designed•Knowledge and skills of clinical preceptors updated•Assessment conducted and curriculum revised
and extended to 24-months•National program of community midwifery education
began 2004; one pilot program started in 2002•Testing and certification process of previously
trained midwives established•Midwifery Education Policy endorsed (2005)

7
Estimating the Need for Midwives
• Calculation of required number of midwives based on number of health facilities (actual and planned) and population
• Approximately 5,000+ midwives needed to staff the expected ideal distribution of health facilities
• Human resource database established in Ministry of Health

8
Selection According to Human Resource Needs
• Mostly from rural areas• Commitment to work post-
graduation in the community where a need was identified and where student is from
• Collaboration with national, provincial, local health authorities and communities in selection and recruitment
• Follow selection policies of MoPH

9
Deployment, Supervision & Support
• Deployment – Midwives deployed to community
facility that they were recruited from
– Working within a defined Basic Package of Health Services
– Supportive supervision • Supervision
– Supervision teams established and checklists used.

10
Quality Education
• Education is focused on competencies and required clinical skills
• Standards & accreditation to ensure quality of teaching
• Residential programs addressed cultural concerns about women being away from families & provided supportive learning environments with almost zero attrition
• Babies and toddlers stayed with their mothers …and new babies arrived during the training!

11
Establishing the Accreditation System to Ensure Quality in Midwifery Education
1. Unified, national system built based on education standards
2. All programs initially “encouraged” to implement standards
3. National Midwifery Education Accreditation Board established
4. Standards and accreditation became mandatory
5. Improvements extended to clinical areas

12
Performance Standard Example
PERFORMANCE STANDARDS
SCORE VERIFICATION CRITERIA YES NO N/A1 COMMENTS
Verify whether the provider determines if the woman has had any danger signs during her pregnancy:
Vaginal bleeding
Respiratory difficulty
Fever, severe headache/blurred vision
Severe abdominal pain
Convulsions/loss of consciousness
Blurred vision
1. The provider asks about and records danger signs that the woman may have or has had.
Assures immediate attention in the event of any of the above symptoms
N/A = Not Applicable

13
CME Paktya, Binding Assessment

14
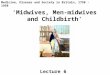
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Badak
hsha
n
Bamya
nG
hor
Hirat
Jawzja
nKab
ul
Kanda
har
Khost
Paktiy
a
Takhar
Baseline Non-binding Binding Re-binding (After 2 years)
Accreditation 2006-2009

15

16

17
Results: IHSs &CME Schools
1. Badakhshan2. Badghis3. Baghlan4. Bamyan 5. Daykundi6. Farah7. Faryab (2
schools)8. Ghazni9. Ghor10. Helmand11. Jawzjan12. Khost
13. Kunar14. Kunduz15. Laghman16. Logar17. Nangarhar (2 schools)18. Nimroz19. Paktika20. Paktiya21. Parwan22. Samangan23. Sari Pul24. Takhar25. Urozgan26. Wardak27 Zabul
Newly graduated community midwives in Badakhshan province take midwifery pledge

18
Results: Institute of Health Sciences- Hospital Midwives
1. Kabul 2. Herat3. Nangarhar4. Kandahar5. Balkh
Students in skills lab in Takhar CME

Support to/from the Afghan Midwives Association
• Built capacity of AMA • AMA promotes and
strengthens the midwifery profession through– Organizational
development and sustainability, leadership programs, advocacy, and in-service trainings

20

Output and Achievement of MWE Programs
Type of Program
Currently studying
Enrolled
Graduated
Drop-outs
% Graduated
Deployed/Employed
% Deployed/ Employment of graduated
Currently working (as of May, 2009)
% currently working of graduated
Currently working of deployed/employed
IHS 167 1232
1103 129 90% 890 81% 754 68% 85%
CME 509 886 858 28 97% 785 91% 694 81% 88%
TOTAL 676 2118
1961 157 93% 167
5 85% 1448 74% 86%

22
Achievements
Before: – 8% of births attended
by a skilled provider in 2003
– Skilled ANC at 4.6% in 2003
– 5 midwifery education programs in 2002
– Outdated midwifery education curriculum with a focus on training hospital midwives
– 467 midwives in the country in 2002
– Few female staff in health facilities
After: – Birth attendance by
skilled provider increased to 19% in 2006
– Skilled ANC increased to 32% in 2006
– 34 midwifery education programs in 2010
– Competency-based training curriculum developed to train hospital & community midwives
– By May 2009, 2,200 competent midwives have graduated, 1,675 deployed (85%)
– 59% of BPHS health facilities (BHC, CHC, DH) staffed with at least 1 midwife

23
Are Women Getting the Services they Need?
“Before there was no midwife in our health center and we had to travel over one hour to the nearest town. I had all my babies at home before because of this. But now Midwife Hadia is at the health centre and because of this more women are seeing a midwife. I will have my next baby with Hadia in this health center, she is very nice and makes me feel safe”
Woman in Takhar province who was delivered by Midwife Hadia

24
Remaining Challenges
• Planning the HR needs for midwives nationally – how many do we need?
• Supervision post-graduation – are midwives under worked? Or over burdened and not able to focus on maternal and newborn health?
• Tracking deployment nationally
• Retention for remote and insecure areas
• Focusing on quality of existing programs
• Cultural isolation of women and female literacy rates

25

26
Lessons Learned & Recommendations
• Increasing skilled attendance at birth requires political will and commitment
• Focus should be on establishing and supporting a national accreditation system and processes
• Build on previous successes and approaches• Selection & recruitment of midwives linked to deployment is key to
success; think about the quality and deployment at the beginning• Involve the community and think about creative and culturally
appropriate approaches to attract students and the support of the community and families
• Midwives must be continuously supported in maximizing their potential• A professional association, such as AMA, is important to providing
advocacy for the profession, support for the midwives, and contributes to sustainability
• Success of community midwifery programs has created demand• Professional development and CME .

27
Remaining Challenges
• Planning the HR needs for midwives nationally – how many do we need?
• Supervision post-graduation – are midwives under worked? Or over burdened and not able to focus on maternal and newborn health?
• Tracking deployment nationally
• Retention for remote and insecure areas
• Focusing on quality of existing programs
• Cultural isolation of women and female literacy rates

28
Final Words
• “I am happy with the midwife. Previously there was no midwife in our village and women were suffering bleeding and their children were dying. Now thanks to God, we have got a midwife and since have not seen a pregnancy death.”
• “In the beginning, people thought that I might be a dayee (traditional birth attendant) and would not be effective. At present, they know me as a women’s specialist and they respect me and say that I solve their women’s problems.”

THANK YOU