Embed Size (px)
Citation preview
IntroductionNumerous basic and clinical studies on the reconstructivesurgery of the anterior cruciate ligament (ACL) with ten-don autograft have been performed in the last 2 decades.They have improved the clinical outcome after ACL recon-struction, although a number of problems remain unsolved.
Regarding the biological aspect, experimental studieshave demonstrated that the grafted tendon tissue changesinto ligament tissue in a new biological and physical envi-ronment. When autogenous patellar tendon is transplantedacross the knee joint to reconstruct the ACL, fibroblastnecrosis initially occurs during the early period aftersurgery [1, 2, 4, 10, 11]. Then the patellar tendon graft is
Abstract The purpose of this paperis to review scientific evidence thatgraft tension affects remodelling ofthe autograft in ligament reconstruc-tion. The in situ freezing model ofthe patellar tendon, an ideal patellartendon autograft model, demon-strated that subsequent cellular pro-liferation following fibroblast necro-sis reduces the mechanical propertiesof the autograft. Stress shielding en-hances reduction of the strength inthe once-frozen patellar tendon. Thestrength of the patellar tendon alsochanges depending on the degree ofstress shielding. Transmission elec-tron micrographs revealed that thenumber of small-diameter fibrils de-creases in the stress-shielded tendonscompared with non-stress-shieldedtendons after in situ freezing. Re-stressing essentially restores the me-chanical properties of patellar tendonautografts even if the strength hasbeen much reduced by completestress shielding. The effects of re-stressing may depend on the periodof stress shielding applied before re-stressing. Unphysiologically hightension significantly reduces the me-
chanical properties of the in situfrozen anterior cruciate ligament(ACL). Therefore, not only stress-de-privation but also stress-enhance-ment significantly affect the mechan-ical properties of tendon autografts.Results of in vivo and in vitro stud-ies suggest that cyclic tensile loadingmay inhibit the deterioration in me-chanical strength of the transplantedtendon. Clinically, our prospectiverandomized study demonstrated thata relatively high initial tension re-duces the postoperative anterior lax-ity of the knee joint after ACL re-construction using the doubled auto-genous hamstring tendons connectedin series with polyester tapes, whenthe tension applied is less than 80 N.Our experimental and clinical resultsindicate that the initial tension is oneof the significant factors that affectthe results of ACL reconstruction, al-though the optimal initial tension forthe other graft materials still remainsunknown.
Key words Anterior cruciate ligament · Graft tension · Remodeling
Knee Surg, Sports Traumatol, Arthrosc(1998) 6 [Suppl 1] :S30–S37
© Springer-Verlag 1998
Harukazu TohyamaKazunori Yasuda
Significance of graft tension in anteriorcruciate ligament reconstructionBasic background and clinical outcome
H. Tohyama (Y) · K. YasudaDepartment of Medical Biomechanics,Hokkaido University School of Medicine,Kita-15 Nishi-7, Kita-ku,Sapporo, 060-8638 JapanTel.: +81-11-706-7211Fax: +81-11-706-7822

enveloped with a vascular synovial tissue that initiates anintrinsic revascularization response [2, 4, 11]. This revas-cularization response is accompanied by cellular prolifer-ation in the graft. The revascularization of the patellar ten-don graft can be completed by 20 weeks, although evenmore time is required for the graft to obtain the structuraland mechanical characteristics of a ligament. Thesechanges are defined as “ligamentization” [2].
Concerning the biomechanical aspect, the autograft hasbeen extensively studied in animal ACL reconstructionmodels. Clancy et al. reconstructed the ACL with a freepatellar tendon autograft in the rhesus monkey. Theydemonstrated that the ultimate load of the patellar tendongraft was 52% of the control value at 12 months [11].McPherson et al. reported that the ultimate load of thepatellar tendon autograft was 45% of the control at 12months [18]. Butler et al. measured the mechanical prop-erties of patellar tendon autografts used to replace theACL in the cynomolgus monkey at four time periods upto 1 year [8]. The maximum stress and the ultimate loadreached 7% and 16%, respectively, of the control value at7 weeks, increasing to 26% and 39%, respectively, by 1year. Tohyama et al. demonstrated that the ultimate loadof the isometrically placed patellar tendon decreased to18% of the control value 18 months after reconstruction[32]. In these experimental studies, the mechanical andstructural properties of the graft were 20%–50% of thecontrol value of the ACL at 12 months after operation.
The success rate of ACL reconstruction has been re-ported to be between 75% and 90% [26]. However, theevaluation was made on the basis of the anterior trans-lation of the knee. The mechanical and structural proper-ties of the autografts have rarely been measured in humansubjects, although the animal experimental study sug-gested that anterior translation of the knee may reflect thestructural properties of the ACL graft [6]. An opposingview was proposed by Oakes, who observed collagen fi-brils of the patellar tendon autograft biopsied from humanpatients using transmission electron microscopy [22]. Themost significant feature of all the specimens was the in-variant predominance of small-diameter fibrils among afew larger, probably original, patellar tendon fibrils. Thelarge cross-section occupied by small-diameter fibrils per-sisted in grafts of all ages, although the cross-sectional areaof fibrils larger than 100 nm seemed to increase in the oldgrafts, those of 5–9 years. This suggests that the cross-sectional area of small fibrils slowly decreases with time.
Thus, there is great discrepancy in the results of ACLreconstruction between experimental and clinical studies.We have hypothesized that some of it can be explained byeffects of the mechanical environment. Graft tension hasbeen regarded as one of the important factors. However,the significance of graft tension has not been establishedon the basis of empirical data. The purpose of this paper isto review the scientific evidence that graft tension affectsremodelling of the autograft in ligament reconstruction.
Effects of graft tension on free autograft in ACL reconstruction
Yoshiya et al. investigated the effects of 1 and 39 N initialtensions on a patellar tendon graft using a canine modeland detected no significant difference in the values for thefailure load of the graft 3 months after reconstruction[39]. Conversely, Arms et al. demonstrated in a caninemodel that local elongation of a bone-patellar tendon-bone graft at the time of operative fixation can affect itsultimate failure strength 1 year after reconstruction of theACL [3]: grafts that had had high local elongation valuesat the time of fixation had inferior values for ultimate fail-ure strength compared with those that had had lower localelongation values. Tohyama et al. also demonstrated thatinitial graft elongation, which reflects initial graft ten-sion, significantly affected the stiffness of the graft at 18 months after reconstruction in a canine model [32].Therefore, there is disagreement on the effects of initialgraft tension among these experimental studies. The di-vergence in results may be explained, in part, by varioussurgical and postoperative factors. To understand pre-cisely the effects of tension on the autograft, we shoulddistinguish the essential effect of tension from the effectsof other factors.
Effects of stress deprivation on the in situ frozen patellar tendon
Development of an autograft model
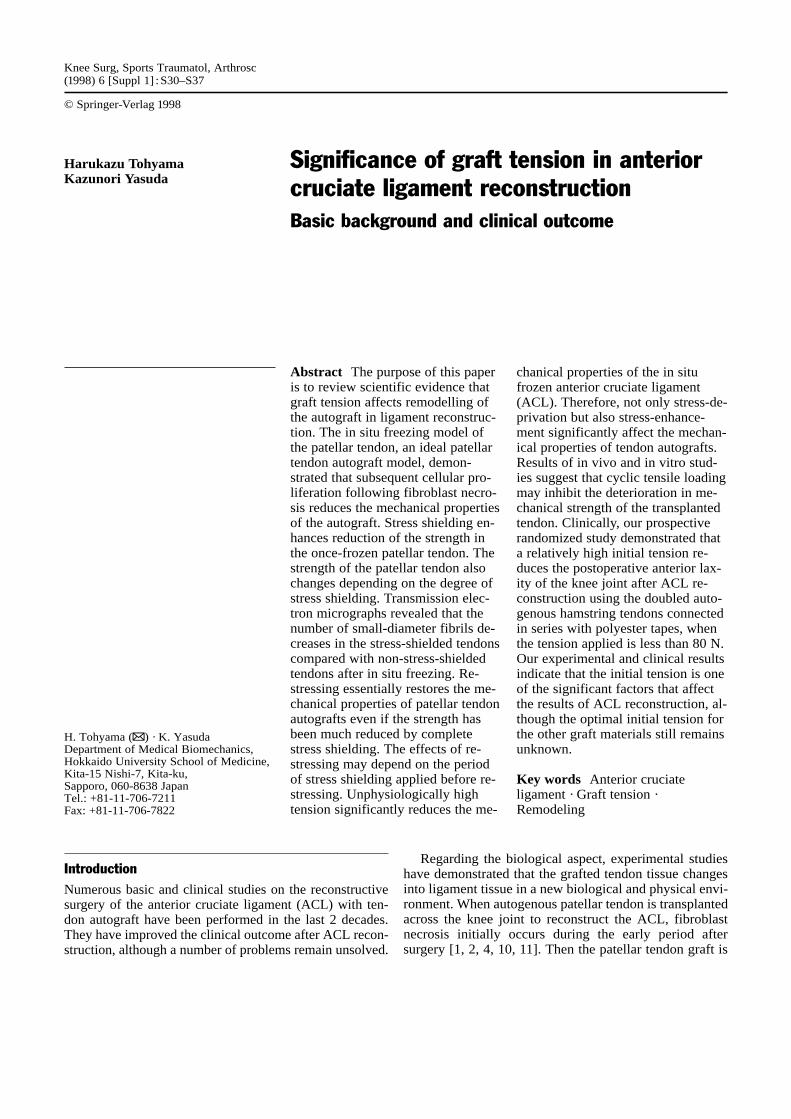
To improve understanding of the remodelling of auto-grafts, it is necessary to isolate the effects of each implan-tation variable from the effects of the other variables. Fi-broblast necrosis has been considered to be the most es-sential change in autografts transplanted for ACL recon-struction. We developed a patellar tendon autograft modelby necrotizing fibroblasts in the tendon with the in situfreeze-thaw technique in rabbits [23, 25]. This model sim-ulates an extra-articular patellar tendon autograft model asan alternative to intra-articular ACL reconstruction usinga patellar tendon autograft. A silicone rubber sheet wasinserted between the patellar tendon and the fat pad, andthe edges of the sheet were clamped with four graspers tomake a bath with the patellar tendon inside it. Liquid ni-trogen was poured into the bath; the patellar tendon wasfrozen in situ for 1 min (Fig. 1). The frozen patellar ten-don was then thawed by pouring physiological saline so-lution into the bath. In this model, fibroblast necrosis iseasily and quickly stimulated without disturbance of thetendon attachment sites or alteration of the mechanical en-vironment of the patellar tendon.
The effects of the in situ freezing treatment were ob-served for 24 weeks [25]. The tensile strength of the ten-don did not change for 2 weeks, then began decreasing by
S31
3 weeks (Fig. 2). The strength decreased to approximately50% of the control value at 24 weeks. The cross-sectionalarea of the patellar tendon started to increase by 3 weeks,reaching a plateau at 12 weeks. Histologically, cells wereabsent until 2 weeks, while a large number of new fibro-blasts appeared by 3 weeks. Although the once frozenpatellar tendon had apparently normal cells at 24 weeks, itdid not contain dense collagen bundles like those seen inthe normal patellar tendon.
Recently, we inhibited extrinsic cell infiltration into theonce frozen patellar tendon by wrapping it with a nylonmembrane filter of 200 µm pore size [33]. The tensilestrength did not decrease in the frozen wrapped tendons,while it did decrease significantly at 3 weeks in the frozenwrapped tendons compared with the control tendons.Therefore, we can conclude that the fibroblast necrosis it-self does not affect the mechanical properties of the patel-lar tendon, but that the subsequent proliferation of extrin-sic cells changes them.
Effects of stress deprivation
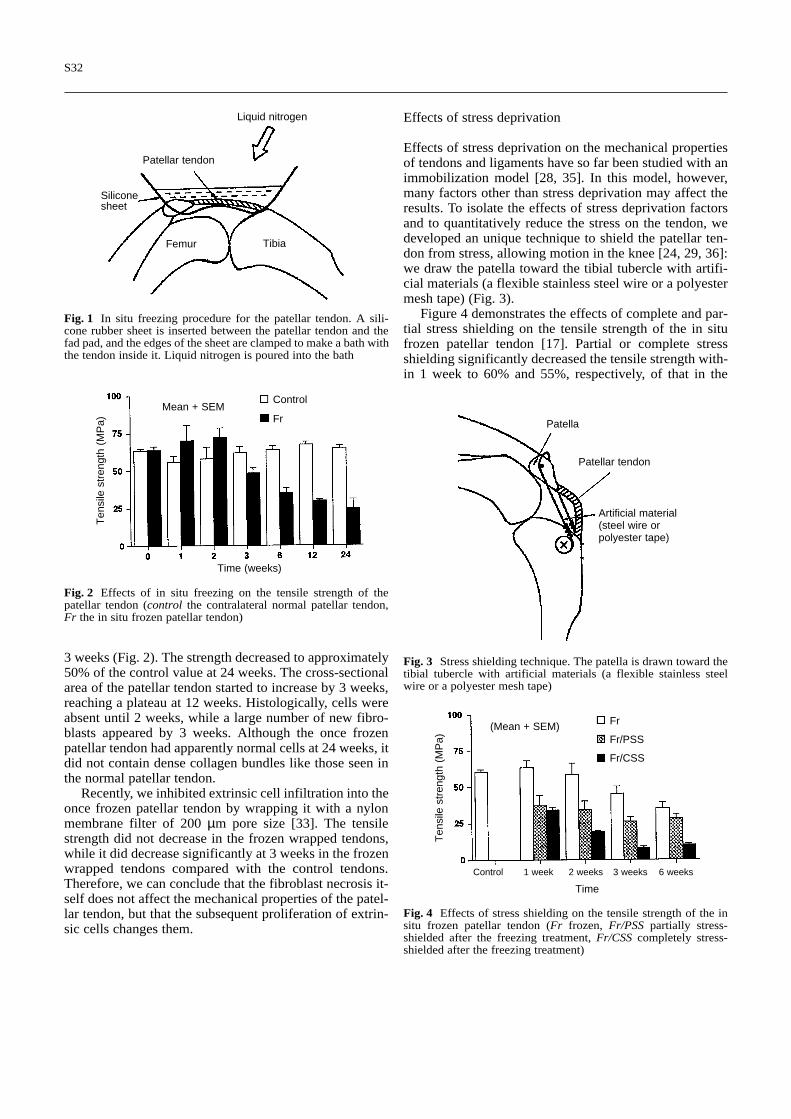
Effects of stress deprivation on the mechanical propertiesof tendons and ligaments have so far been studied with animmobilization model [28, 35]. In this model, however,many factors other than stress deprivation may affect theresults. To isolate the effects of stress deprivation factorsand to quantitatively reduce the stress on the tendon, wedeveloped an unique technique to shield the patellar ten-don from stress, allowing motion in the knee [24, 29, 36]:we draw the patella toward the tibial tubercle with artifi-cial materials (a flexible stainless steel wire or a polyestermesh tape) (Fig. 3).
Figure 4 demonstrates the effects of complete and par-tial stress shielding on the tensile strength of the in situfrozen patellar tendon [17]. Partial or complete stressshielding significantly decreased the tensile strength with-in 1 week to 60% and 55%, respectively, of that in the
S32
Liquid nitrogen
Patellar tendon
Femur
Siliconesheet
Tibia
Fig. 1 In situ freezing procedure for the patellar tendon. A sili-cone rubber sheet is inserted between the patellar tendon and thefad pad, and the edges of the sheet are clamped to make a bath withthe tendon inside it. Liquid nitrogen is poured into the bath
Control
FrMean + SEM
Ten
sile
str
engt
h (M
Pa)
Time (weeks)
Fig. 2 Effects of in situ freezing on the tensile strength of thepatellar tendon (control the contralateral normal patellar tendon,Fr the in situ frozen patellar tendon)
Patella
Artificial material(steel wire orpolyester tape)
Patellar tendon
Fig. 3 Stress shielding technique. The patella is drawn toward thetibial tubercle with artificial materials (a flexible stainless steelwire or a polyester mesh tape)
Fr
Fr/PSS
Fr/CSS
(Mean + SEM)
Control 1 week 2 weeks 3 weeks 6 weeks
Time
Ten
sile
str
engt
h (M
Pa)
Fig. 4 Effects of stress shielding on the tensile strength of the insitu frozen patellar tendon (Fr frozen, Fr/PSS partially stress-shielded after the freezing treatment, Fr/CSS completely stress-shielded after the freezing treatment)

frozen group. On the other hand, in the frozen group, thetensile strength started decreasing at between 2 and 3weeks. Histologically, no cells were observed within thefirst 2 weeks in any group; new cells appeared after 3weeks. There were essentially no differences in the lightmicroscopic structure between the partially stress-shieldedand frozen groups in this period; however, collagen fibreswere fragmented in the completely stress-shielded groupbut not in the other two groups.
These observations indicate that stress shielding en-hanced the reduction of the strength in the once-frozenpatellar tendon. A significant reduction in the mechanicalproperties was already obvious at 1 week in both the par-tially and completely stress-shielded groups, although therewere no cells at this period. These results demonstrate thatthe mechanical response of the patellar tendon to stressshielding occurs independently of living cells, and there-fore that the remodelling occurring during stress shieldingis associated with non-cellular components, including col-lagen. With respect to the difference between completeand partial stress shielding, the tensile strength of thecompletely stress-shielded patellar tendon was generallylower than that of the partially stress-shielded patellar ten-don. Thus, the strength of the patellar tendon changes de-pended on the degree of stress shielding.
To clarify the effects of complete stress shielding on theultrastructure of the in situ frozen patellar tendon, trans-mission electron micrographs were obtained of the patellartendons completely shielded from stress for 3 and 6 weeksafter the freeze-thaw treatment [34]. At 3 weeks, we foundobvious differences in the diameter of collagen fibrils be-tween the frozen tendons and frozen stress-shielded ten-dons. The number of small-diameter fibrils decreased inthe stress-shielded tendons, while the unphysiologicallylarge fibrils increased. These results demonstrate that stressshielding affects the extracellar matrix of the tendon, inparticular, the collagen fibrils. These changes may lead tothe deterioration of tendon strength.
Effects of resumption of stress on the stress-shielded tendon
We also investigated the effects of restressing on the pre-viously frozen and completely stress-shielded patellar ten-don [14]. The artificial material installed in parallel to therabbit tendon for stress-shielding (Fig. 3) was cut and re-moved after stress-shielding for 1–6 weeks, and physio-logical stress was applied again to the tendon for the fol-lowing 3–12 weeks. When a frozen patellar tendon wascompletely shielded from stress for less than 3 weeks, re-stressing completely restored the reduced mechanical prop-erties to the normal level of the autograft, and 12 weeks ofrestressing was required for recovery. When a frozenpatellar tendon was completely shielded from stress for 6weeks, the mechanical properties of the patellar tendon
did not change between 3 and 6 weeks after restressingbut significantly increased by 12 weeks. This study sug-gests that stressing essentially restores the mechanicalproperties of patellar tendon autografts even if their strengthhas been greatly reduced by complete stress shielding.However, the effects of restressing may depend on the pe-riod of stress shielding applied before restressing.
Effects of stress enhancement on the in situ frozen ACL
The effects of graft tension should be evaluated not onlyin the extra-articular environment but also in the intra-ar-ticular environment. Therefore, we created an in situfrozen ACL model using the dog [15]. This is an ideal in-tra-articular model of ACL reconstruction. To kill the fi-broblasts in the canine ACL, we developed a mini-cry-oprobe. We coiled the spiral tube around the ACL andthen circulated liquid nitrogen through the tube. Thefreeze-thaw treatment was repeated three times. The cellculture technique demonstrated that the freeze-thaw treat-ment with this probe killed 100% of cells in the midsub-stance and tibial attachment of the ACL, and 95% of cellsin the femoral attachment [15].
Using this in situ frozen ACL model, we clarified theeffects of stress enhancement on the remodelling of thereconstructed ACL [15]. After the bilateral ACLs werefrozen in situ in each dog, the tibial insertion of the ACLwas freed from the tibia along with a cylindrical boneblock. In the right knee, a high tension of 20 N was ap-plied to the ACL by pulling the bone block in the distal di-rection with a tensiometer (the high tension group). In theleft knee, this bone block was reduced anatomically (thephysiological tension group). Then, each bone block wasfirmly fixed with an interference screw. We also measuredthe ACL tension of the high tension group using anarthroscopic force probe (Microstrain, Vt) for 72 h after
S33
Physiological
High
(Mean + SEM)
Ten
sile
str
engt
h (M
Pa)
6 weeks 12 weeksTime
Fig. 5 Effects of stress enhancement on the tensile strength of thein situ frozen ACL (physiological the physiological tension group,high the high tension group)
surgery. The precision and reproducibility of this trans-ducer have been confirmed [30].
Figure 5 shows the mechanical properties of the hightension and physiological tension groups at 6 and 12 weeks.The tensile strength decreased significantly between thetwo periods in the high tension group, but not in the phys-iological tension group. The strength in the high tensiongroup was significantly lower than in the physiologicaltension group at 12 weeks, but not at 6 weeks. Histologi-cally, we observed focal degenerative changes in the sub-stance of highly tensioned tendon at 12 weeks, whilethese changes were not found in the physiological tensiongroup. These findings demonstrate that unphysiologicallyhigh tension significantly reduces the mechanical proper-ties of the in situ frozen ACL.
Effects of cyclic loading on remodelling process
To clarify the effects of cyclic loading on the remodellingprocess of the tendon autograft, in vivo and in vitro stud-ies were examined. Muneta et al. performed an in vivo ex-periment using a rabbit model [21]. They transplanted thepatella-patellar tendon-tibia complex into a subcutaneoustissue on the back of the rabbit. Controlled cyclic loads (apeak load of 10 N, 60 times over a period of 5 min, 5 daysper week) were applied via transcutaneous sutures to halfof the graft, while the other half remained unloaded. Theyshowed that the loaded portions of the patellar tendonshad a significantly higher ultimate load and stiffness thanthe unloaded halves at 3 and 6 weeks. Histology demon-strated that cellularity had increased from 3 weeks to 6 weeks, with the loaded portion exhibiting a substantiallyhigher cell density than the unloaded half. Hannafin et al.investigated the effects of cyclic tensile loading on thematerial properties of canine flexor tendon using an invitro organ culture system [13]. They applied a cyclic ten-sile load (a peak load of 0.42 N, one cycle per minute for2 hour per day, 5 days per week) to canine flexor tendonsover a 4-week time period. The tensile modulus of cycli-cally loaded tendon (93% of the control) was significantlygreater than that of unloaded tendon (68% of the control).They also found that cyclic loading maintained the normalhistological pattern of the tendon, while there was a de-crease in the number of cells in the unloaded tendon. Theresults of these in vivo and in vitro studies suggest thatcyclic tensile loading may inhibit the deterioration of themechanical strength of the transplanted tendon.
Effects of initial graft tension on clinical outcome
An important question we should ask is if initial tension inthe autograft strongly affects the clinical outcome in hu-man ACL reconstruction. In 1991, we developed a newACL reconstruction procedure using doubled hamstring
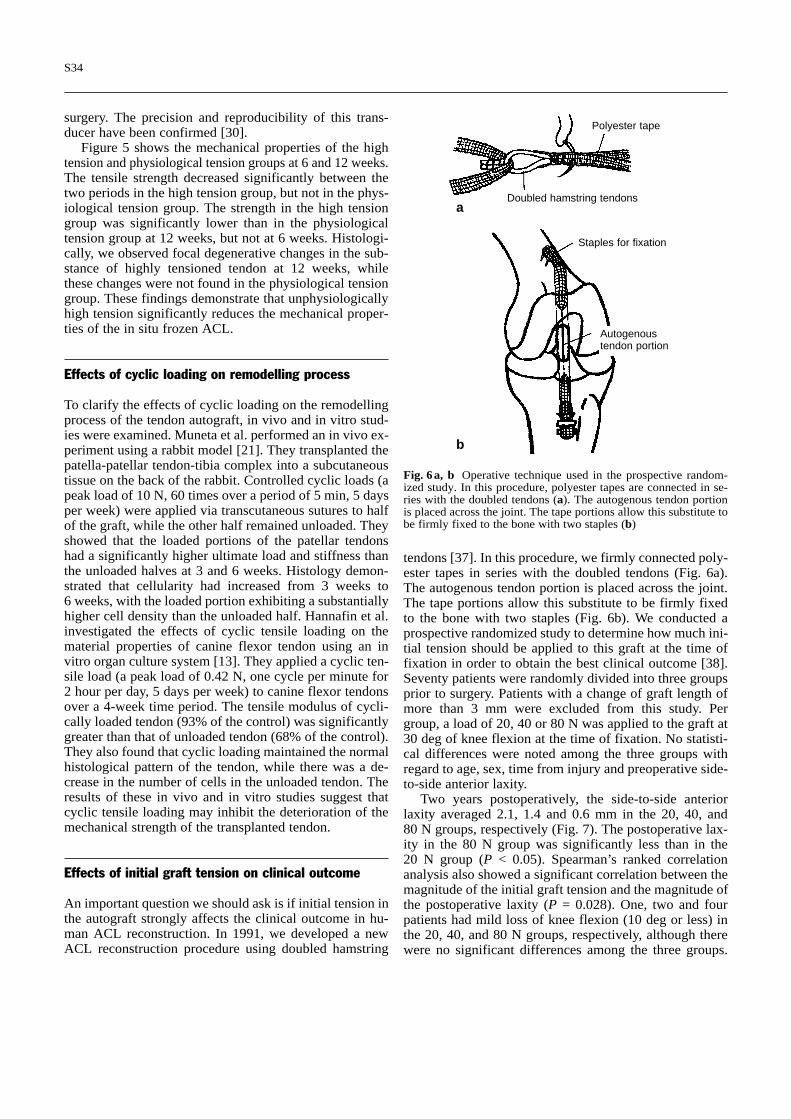
tendons [37]. In this procedure, we firmly connected poly-ester tapes in series with the doubled tendons (Fig. 6a).The autogenous tendon portion is placed across the joint.The tape portions allow this substitute to be firmly fixedto the bone with two staples (Fig. 6b). We conducted aprospective randomized study to determine how much ini-tial tension should be applied to this graft at the time offixation in order to obtain the best clinical outcome [38].Seventy patients were randomly divided into three groupsprior to surgery. Patients with a change of graft length ofmore than 3 mm were excluded from this study. Pergroup, a load of 20, 40 or 80 N was applied to the graft at30 deg of knee flexion at the time of fixation. No statisti-cal differences were noted among the three groups withregard to age, sex, time from injury and preoperative side-to-side anterior laxity.
Two years postoperatively, the side-to-side anteriorlaxity averaged 2.1, 1.4 and 0.6 mm in the 20, 40, and 80 N groups, respectively (Fig. 7). The postoperative lax-ity in the 80 N group was significantly less than in the 20 N group (P < 0.05). Spearman’s ranked correlationanalysis also showed a significant correlation between themagnitude of the initial graft tension and the magnitude ofthe postoperative laxity (P = 0.028). One, two and fourpatients had mild loss of knee flexion (10 deg or less) inthe 20, 40, and 80 N groups, respectively, although therewere no significant differences among the three groups.
S34
Polyester tape
Doubled hamstring tendons
Staples for fixation
Autogenoustendon portion
Fig. 6a, b Operative technique used in the prospective random-ized study. In this procedure, polyester tapes are connected in se-ries with the doubled tendons (a). The autogenous tendon portionis placed across the joint. The tape portions allow this substitute tobe firmly fixed to the bone with two staples (b)
a
b

There were no patients with loss of knee extension in eachgroup. This study demonstrates that a relatively high ini-tial tension (but less than 80 N) reduces the postoperativeanterior laxity of the knee joint after our ACL reconstruc-tion procedure using the hamstring tendons.
Discussion
In this paper, we have provided scientific evidence thatgraft tension affects remodelling of the autograft in liga-ment reconstruction. For example, many studies have sug-gested that excessive stress deprivation greatly influencesthe mechanical properties, histology and ultrastructure ofthe autograft. Our experimental study demonstrated thatexcessive stress enhancement also has adverse effects onthe mechanical properties of the previously frozen ACL.Therefore, we hypothesized that not only excessively lowtension but also excessively high tension may reduce themechanical properties of the autograft. Only adequate ten-sion within a relatively narrow range may prevent the de-terioration of the mechanical properties. However, we donot know the extent of this range at present. This hypoth-esis may explain the differences in the postoperative re-sults of ACL reconstruction using the patellar tendon au-tograft between humans and animals, because the me-chanical environment around the autograft is extremelydifferent.
Based on experimental studies, we considered the fol-lowing hypothesis on the effects of mechanical stimuli onthe tendon autograft. Cellular proliferation following fi-broblast necrosis causes essential remodelling of the auto-graft. This remodelling process may be significantly af-fected by the mechanical stimuli from the surrounding en-vironment. Especially concerning the effects of stress de-privation on the mechanical properties of the autograft,we propose two mechanisms. First, stress deprivation di-rectly affects the matrix, specifically collagen molecules.Second, it also affects fibroblasts, and subsequently the fi-broblasts change the structure of collagen. Both mecha-
nisms result in the reduction of the mechanical propertiesof the autograft. To clarify the mechanisms of these phe-nomena, further biomechanical, ultrastructural and bio-chemical studies should be conducted.
Clinically, our prospective randomized study demon-strated that a relatively high initial tension reduces thepostoperative anterior laxity of the knee joint after ACLreconstruction using the doubled autogenous hamstringtendons connected in series with polyester tapes, when thetension applied is less than 80 N. We should acknowledgethat the postoperative laxity is not determined solely bythe mechanical properties of the reconstructed ligamen-tous tissue. Two potential other mechanisms may explainthis phenomenon. Many studies have pointed out that anincrease of ACL tension decreases the degree of anteriortranslation of the tibia to the femur [7, 9, 12, 16, 20]. Be-cause the graft tension may decrease in the early and re-modelling phases after reconstruction surgery, low tensionapplied on the graft during surgery may result in slacknessof the reconstructed ligament tissue. Therefore, one po-tential mechanism is that the tension of a ligament graftwith a low initial tension may be insufficient at the finalfollow-up. Second, many experimental studies have sug-gested that tension significantly affects the mechanicalproperties and the tissue dimension of tendon autografts.Therefore, the other potential mechanism is that the stiff-ness and the strength of a reconstructed ligament tissuemay change during its remodelling process depending onthe degree of initial graft tension, if the initial tension ischosen from an adequate range.
Initial tension for the graft directly affects the postop-erative stress conditions. Both excessively low and hightension should be avoided. We cannot apply the recom-mendation obtained with our prospective randomizedstudy to other ACL reconstructive procedures, for severalreasons. First, the optimal initial tension may be graft-spe-cific [7]. Second, the load-deformation characteristics ofthe femur-graft-tibia complex at the time of implantationdepend not only on the mechanical properties of the auto-genous graft, but also on the artificial devices used for fix-ation [19, 27, 31]. Third, graft tension during the remod-elling process is considered to be affected by creep elon-gation of an autograft and its transposition in the bonetunnel [5]. The characteristics of the femur-graft-tibiacomplex concerning creep and transposition also dependon the characteristics of all artificial devices used for fix-ation [31]. Thus, we recommend applying an initial ten-sion of approximately 80 N for the doubled hamstring ten-dons with synthetic tapes. However, we have to say thatthe optimal initial tension still remains unknown for otherACL reconstructive procedures. It is necessary to deter-mine how much graft tension should be applied to the au-tograft in order to obtain the best clinical outcome by fur-ther clinical studies.
There are many transplantation variables that lead toACL reconstruction success. They are categorized into
S35
Initial graft tension
Sid
e to
sid
e an
terio
r la
xity
diff
eren
ce (
mm
) (Mean + SEM)
Fig. 7 Effects of initial graft tension on the side-to-side anteriorlaxity difference of the knee at 2 years after the operation

S36
two types, biological and mechanical. The biological onesinclude synovial environment condition, postoperativehaemorrhage, postoperative synovitis, cytokines, cell in-filtration and revascularization. The mechanical ones in-clude mechanical and structural properties of the graft,preconditioning of the graft, initial graft tension, graftisometry and fibre orientation, graft fixation to the bone,notchplasty and postoperative management. Biologicalvariables involve many essential factors in tendon trans-plantation. Unfortunately, however, most of them are notchecked by surgeons at present. On the other hand, themechanical variables are related to surgical techniquesand postoperative management, factors which are con-trolled by surgeons. Therefore, we can say that the me-chanical variables are the keys to success in ACL recon-
struction at present. Initial graft tension is an important el-ement of the mechanical environmental factors surround-ing the autograft. We do not believe that the initial tensionis the sole factor that determines success or failure in ACLreconstruction. However, we believe that the initial ten-sion is one of the significant factors affecting the results.It is necessary to establish quantitative guidelines for op-timal tension for each graft used in ACL reconstruction.
Acknowledgements We appreciate our collaborators, Drs. Kiyo-shi Kaneda, Kozaburo Hayashi, Noritaka Yamamoto, KazunoriOhno, Tokifumi Majima, Takamasa Tsuchida, Hirohide Ishida,Ryosei Katsuragi, Jun Tsujino, Koji Miyata and Ms. Yoshie Tan-abe. This work was supported financially in part by the Grant-in-Aids for Scientific Research (nos. 07558118 and 08671629) fromthe Ministry of Education, Science and Culture in Japan.
1.Alm A, Strömberg B (1974) Transpos-ed medial third of patellar ligament inreconstruction of the anterior cruciateligament: a surgical and morphologicstudy in dogs. Acta Chir Scand Suppl445:37–49
2.Amiel D, Kleiner JB, Roux RD, Har-wood FL, Akeson WH (1986) Thephenomenon of “ligamentization”: an-terior cruciate ligament reconstructionwith autogenous patellar tendon. J Or-thop Res 4:162–172
3.Arms SW, Pope MH, Johnson RJ,Renström P, Fischer RA, Järvinen M,Beynnon BD (1990) Analysis of ACLfailure strength and initial strains in thecanine model. Trans Orthop Res Soc15:524
4.Arnoczky SP, Tarvin GB, Marshall JL(1982) Anterior cruciate ligament re-placement using patellar tendon: anevaluation of graft revascularization inthe dog. J Bone Joint Surg [Am] 64:217–224
5.Beynnon BD, Johnson RJ, FlemingBC, Renstrom PA, Nichols CE, PopeMH, Haugh LD (1994) The measure-ment of elongation of anterior cruciateligament graft in vivo. J Bone JointSurg [Am] 76:520–531
6.Beynnon BD, Johnson RJ, Tohyama H,Renstrom PA, Arms SW, Fischer RA(1994) The relationship between ante-rior-posterior knee laxity and the struc-tural properties of the patellar tendongraft. A study in canines. Am J SportsMed 22:812–820
7.Burks RT, Leland R (1988) Determina-tion of graft tension before fixation inanterior cruciate ligament reconstruc-tion. Arthroscopy 4:260–266
8.Butler DL, Grood ES, Noyes FR, Olm-stead M, Hohn RB, Arnoczky SP,Siegel MG (1989) Mechanical proper-ties of primate vascularized vs. non-vascularized patellar tendon grafts;changes over time. J Orthop Res 7:68–79
9.Bylski-Austrow DL, Grood ES, HefzyMS, Holden JP, Butler DL (1990) An-terior cruciate ligament replacements: amechanical study of femoral attach-ment location, flexion angle at tension-ing, and initial tension. J Orthop Res 8:522–531
10.Chiroff RT (1975) Experimental re-placement of the anterior crucate liga-ment: a histological and microradio-graphic study. J Bone Joint Surg [Am]57:1124–1127
11.Clancy WG, Narechania RG, Rosen-berg TD, Gmeiner JG, Wisnefske DD,Lange TA (1981) Anterior and poste-rior cruciate ligament reconstruction inrhesus monkeys. J Bone Joint Surg[Am] 63:1270–1284
12.Fleming BC, Beynnon BD, Howe JG,McLeod W, Pope MH (1992) Effect oftension and placement of a prostheticanterior cruciate ligament on the an-teroposterior laxity of the knee. J Or-thop Res 10:177–186
13.Hannafin JA, Arnoczky SP, HoonjanA, Torzilli PA (1995) Effects of stressdeprivation and cyclic tensile loadingon the material and morphologic prop-erties of canine flexor digitorum pro-fundus tendon. An in vitro study. J Or-thop Res 13:907–914
14. Ishida H, Yasuda K, Hayashi K, Ya-mamoto N, Kaneda K (1996) Effectsof resumption of loading on stress-shielded autografts after augmentationprocedures. An experimental study.Am J Sports Med 24:510–517
15.Katsuragi R, Yasuda K, Tsujino J,Miyata K, Keira M, Kaneda K (1996)Unphysiologically high initial tensiondeteriorates the mechanical propertiesand histology of the in situ frozen ca-nine anterior cruciate ligament. TransOrthop Res Soc 21:76
16.Lewis JL, Lew WD, Engebretsen L,Hunter RE, Kowalczk C (1990) Fac-tors affecting graft force in surgical re-construction of the anterior cruciateligament. J Orthop Res 8:514–521
17.Majima T, Yasuda K, Yamamoto N,Kaneda K, Hayashi K (1994) Deterio-ration of mechanical properties in con-trolled stress-shielded augmentationprocedure. An experimental study withrabbit patellar tendon. Am J SportsMed 22:821–829
18.McPherson GK, Mendenhall HV, Gib-bons DF, Plenk H, Rottmann W, San-ford JB, Kennedy JC, Roth JH (1985)Experimental mechanical and histo-logic evaluation of the Kennedy liga-ment augmentation device. Clin Orthop196:186–195
19.Miyata K. Yasuda K, Ishida H, KimuraS, Hara N, Kaneda K (1995) Fixationstrength of the polyester tape-ham-string tendons-tape graft in anteriorcruciate ligament reconstruction. TransOrthop Res Soc 21:783
20.More RC, Markolf KL (1988) Mea-surement of stability of the knee andligament force after implantation of asynthetic anterior cruciate ligament. J Bone Joint Surg [Am] 70:1020–1031
21.Muneta T, Lewis JL, Stewart NJ(1994) Load affects remodeling oftransplanted, autogenous bone-patellartendon-bone segments in rabbit model.J Orthop Res 12:138–143
References

S37
22. Oakes BW (1993) Collagen ultrastruc-ture in the normal ACL and in ACLgraft. In: Jackson DW (ed) The ante-rior cruciate ligament. Current and fu-ture concepts. Raven Press, New York,pp 209–218
23. Ohno K, Yasuda K, Yamamoto N,Hayashi K (1991) Effects of stressshielding on the mechanical propertiesof normal and in situ frozen patellartendon. Trans Orthop Res Soc 16:134
24. Ohno K, Yasuda K, Yamamoto N,Hayashi K (1994) Effects of completestress shielding on the mechanicalproperties and histology of in situfrozen patellar tendon. J Orthop Res11:592–602
25. Ohno K, Yasuda K, Yamamoto N,Hayashi K (1996) Biomechanical andhistological changes in the patellar ten-don after in situ freezing. An experi-mental study in rabbits. Clin Biome-chanics 11:207–213
26. Ritchie JR, Parker RD (1996) Graft se-lection in anterior cruciate ligament re-vision surgery. Clin Orthop 325:65–77
27. Steiner ME, Hecker AT, Brown CH,Hayes WC (1994) Anterior cruciateligament fixation. Comparison of ham-string and patellar tendon grafts. Am J Sports Med 22:240–249
28.Tipton CM, Vailas AC, Matthes RD(1986) Experimental studies on the in-fluence of physical activity on liga-ments, tendon and joints: a brief re-view. Acta Med Scand Suppl 711:157–168
29.Tohyama H, Ohno K, Yamamoto N,Yasuda K, Kaneda K, Hayashi K(1992) Stress-strain characteristics ofin situ frozen and stress-shielded rabbitpatellar tendon. Clin Biomech 7:226–230
30.Tohyama H, Beynnon B, Fleming B,Peura G, Johnson R, Pope M (1994)Evaluation of the arthroscopic forceprobe. Trans Orthop Res Soc 19:644
31.Tohyama H, Beynnon B, Fleming B,Johnson R, Pope M (1994) Ultimatefailure strength is not the only criterionfor evaluation of tendon graft fixation.Trans Orthop Res Soc 19:641
32.Tohyama H, Beynnon BD, Johnson RJ,Renström PA, Arms SW (1996) Theeffect of anterior cruciate ligamentgraft elongation at the time of implan-tation on the biomechanical behaviorof the graft and knee. Am J SportsMed 24:608–614
33.Tohyama H, Yasuda K, Miyagi N,Ohno K, Kaneda K (1996) Inhibitionof extrinsic cell infiltration prohibitsreduction of the mechanical propertiesof the patellar tendon following intrin-sic cell necrosis. Trans Orthop Res Soc21:29
34.Tsuchida T, Yasuda K, Hayashi K,Majima T, Yamamoto N, Kaneda K,Miyakawa K, Tanaka K (1994) Effectsof stress shielding on the ultrastructureof the in situ frozen patellar tendon inthe rabbit. Trans Orthop Res Soc19:638
35.Woo SL-Y, Wang CW, Newton PO,Lyon RM (1990) The response of liga-ments to stress deprivation and stressenhancement: biomechanical studies.In: Daniel DM, Akeson WH, O’Con-nor JJ (eds) Knee ligaments: structure,function, injury, and repair. RavenPress, New York, pp 337–350
36.Yamamoto N, Ohno K, Hayashi K,Kuriyama H, Yasuda K, Kaneda K(1992) Effects of stress shielding onthe mechanical properties of rabbitpatellar tendon. J Biomech Eng115:23–28
37.Yasuda K, Tsujino J, Ohkoshi Y, Tan-abe Y, Kaneda K (1995) Graft sitemorbidity with autogenous semitendi-nosus and gracilis tendons. Am JSports Med 23:705–714
38.Yasuda K, Tsujino J, Tanabe Y,Kaneda K (1997) Effects of initial grafttension on clinical outcome of anteriorcruciate ligament reconstruction usingdoubled hamstring tendons. Am JSports Med 25 :95–106
39.Yoshiya S, Andrish JT, Manley MT,Bauer TW (1987) Graft tension in an-terior cruciate ligament reconstruction.An in vivo study in dogs. Am J SportsMed 15:464–470




























