Embed Size (px)
Citation preview


Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 2 of 39
1. About the Department: Scope of services
Timings
Types of patients served
2. Organogram
3. Quality Policy
4. Quality Objectives

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 3 of 39
5. Patient registration and admission S.No Activity Responsibility Record
1. Registration & Admission for walk –in cases
- Registration shall be done at registration counter during OPD
hours and at emergency department during non OPD hrs.
- Every patient who is registered shall be provided with a unique
identification number mentioned in the OP case paper and
directed either towards the OPD/emergency department based
on the working hours.
- A written order for hospitalization by the doctor at the paediatric
OPD during OPD hours or the Medical officer at the emergency
department shall be provided at the registration desk for
initiating admission formalities.
Doctor / Casualty
Medical Officer
OP ticket & Admission
slip
2. Registration and admission of referral cases
- Referred-in cases for out born admission shall be directly guided
to SNCU.
- As per physical assessment of the baby the doctors shall either
advice for hospitalization or prescribe medication/stabilizes and
send back.
- In case of advice for hospitalization, the admission formalities
shall be fulfilled at the SNCU itself.
SNCU - Incharge,
Doctor
Admission slip &
Infant case sheet
3. Inborn cases
- For inborn babies, they shall be transferred to SNCU from the
ward and no separate admission formalities shall be required,
only a separate case sheet for the baby will be developed. The
order for admission shall be given by the concerned doctor on
the mother’s case sheet.
SNCU- Incharge,
Doctor
Infant case sheet at
SNCU
4. Criteria for admission in SNCU
General criteria
- Birth weight < 1800g or gestation < 34 weeks
- Large baby (> 4.0 kg)
- Perinatal asphyxia
SNCU nursing
staff and doctor
Nil

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 4 of 39
- Apnea or gasping
- Refusal to feed
- Respiratory distress(Rate > 60/minute or grunt/retractions)
- Sever jaundice (Appears > 24 hours/stains palms & soles/lasts >
2 weeks)
- Hypothermia < 35.40 C or hyperthermia > 37.50 C
- Central cyanosis
- Shock ( Cold periphery with CFT > 3 seconds and weak and fast
pulse)
- Coma,convulsion,encephalopathy
- Abdominal distension
- Diarrhoea / Dysentery
- Bleeding major malformation
5. For observation after delivery
The following infants should be observed in the SNCU for at least 24
hours after delivery:
- Infants depressed at birth
- Meconium - stained infants
- Infants born after a traumatic delivery
- Infants of diabetic mother
- Infants small for gestational age, and / or < 2.4 kg
- Large for gestational Age > 4.0kg
- Infants born by emergency LSCS
Nursing staff &
Incharge of
Labour room &
SNCU
Mother’s case sheet,
SNCU register
6. Immediate admission after delivery
The following infants are immediately admitted after delivery
- Infants severely depressed at birth, e.g. APGAR score less
than or equal to five at five minutes.
- Any respiratory distress.
- Infants less than 34 weeks gestation or less than 1800g at
birth or SGA.
Nursing staff &
Incharge of
Labour room &
SNCU
SNCU admission
register, Infant case
sheet, Inter-dept
transfer register

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 5 of 39
- Infants with meconium aspiration.
- Infants with major or severe congenital anomalies (does not
include, for e.g. Down Syndrome)
7. Admission from postnatal ward to SNCU
The following signs and symptoms signify a sick infant and should
therefore be admitted from postnatal ward
- Delayed or persistent respiratory distress
- Apnoeic or cyanotic spells
- Abnormal behaviour or activity including recurrent vomiting,
abdominal distention, lethargy, hypotonia, Seizures
- Suspected sepsis
- Evidence of bleeding or excessively pale infants.
- Jaundice if it occurs before 24 hours of age or bilirubin is
equal to or exceeds a level of 15 mg/dl before 48 hours or if
considered to be in phototherapy range according to
reference charts.
- Persistent hypothermia not responding to simple measures.
- Hypoglycaemia –severe / recurrent / non- responding to
feeds alone.
Nursing staff &
Incharge of
maternity ward &
SNCU
SNCU admission
register, Infant case
sheet, Inter-dept
transfer register
In any of the above situations, the concerned doctor needs to be
contacted at the earliest.
Nursing staff
SNCU
Nil
Reference standard - ME E1.1, ME E1.3

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 6 of 39
6. In-case of non-availability of beds S.No Activity Responsibility Record
1. All efforts shall be made to accommodate the baby, extra baby
bassinets and baby warmers shall be available to accommodate the
new admissions.
Management ,
S.N.C.U – Incharge
Nil
2. In case of non-availability of beds, limited refer-in cases shall be
accepted or baby stabilized and referred to another centre.
S.N.C.U – Incharge S.N.C.U register
3. On phone calls received for refer-in cases, the problem of lack of beds
should be clearly intimated to the caller at the other end.
S.N.C.U –
Incharge, Nursing
staff
Nil
Reference standard - ME E1.4
7. Patient receiving, initial assessment, regular re-assessment S.No Activity Responsibility Record
1. Baby receiving from labour room/ward/OT
- For sending the baby to SNCU, prior information to the SNCU-
Incharge shall have to be sent.
- The SNCU nursing staff shall take handover of the baby, complete
necessary formalities in the SNCU register and receive the baby
covered in a sterile towel in the baby receiving tray for transfer to
SNCU.
- Baby bassinets whenever available shall be used for transfer
purpose.
Nursing staff of labour room, ward, OT, SNCU
Inter-dept
transfer register ,
SNCU register
2. Initial assessment
Initial assessment of the baby shall be done on the following
parameters
- Weight, Temperature , general condition
- Airway & breathing
- Circulation
- Convulsion
Nursing staff , duty doctor, specialist
Initial asessment form
Initial assessment and treatment should be provided immediately and
timely documented, preferably within 2 hours
Nursing staff , duty doctor, specialist
Initial asessment form
3. Re-assessment
Re-assessment shall be done by treating doctor at least once a day. Treating doctor Infant case sheet

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 7 of 39
The frequency can be augmented based on the clinical condition.
The following parameters shall be reassessed in routine for all the
patients by the staff nurse.
- Temperature, Pulse and Respiration
- Airway and breathing,
- Any feeding problems
- Any signs & symptoms of infection or any other developing
illness
Staff nurse Nursing note,
Infant case sheet
The treating doctor shall regularly check and scrutinize the notes
made on the case sheet to ensure that all the relevant information
about the sign and symptoms, daily progress or detoriation, notes of
investigations are entered on the case papers and evaluate the baby’s
condition accordingly.
Treating doctor Infant case sheet
The re-assessment done shall faithfully reflect the patient’s clinical
condition, response to treatment and inputs to plan further line of
treatment or discharge.
Treating doctor Infant case sheet
All clinical re-assessments shall be recorded and signed with name,
date and time in the medical record by the staff making entry
Nursing staff,
doctor
Infant case sheet
Reference standard – ME E2.1
8. Criteria for transfer to step down
S.No Activity Responsibility Record
1. The following criteria shall be used for baby transfer to step down unit
- Babies whose respiratory distress is improving and do not require
oxygen supplementation to maintain saturation
- Babies on antibiotics for completion of duration of therapy
- Low birth weight babies (less than 1800g) who are otherwise
stable 9for adequate weight gain)
- Babies with jaundice requiring phototherapy but otherwise stable
- Babies admitted for any condition but are now thermodynamically
and hemodynamically stable
SNCU nursing staff
and doctor
Reference standard – ME E2.1

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 8 of 39
9. Triage of new born
- Hypothermia
(temp< 360C)
- Apnea or gasping
respiration
- Severe respiratory
distress (rate > 70,
severe retractions,
grunt)
- Central cyanosis
- Shock (cold
periphery, CFT>3
secs, weak & fast
pulse)
- Coma, convulsions
or encephalopathy
- Cold stress (temp
36.40C- 360C)
- Respiratory distress
(rate > 60, no
retractions)
- Irritable/restless/jittery
- Abdominal distension
- Severe jaundice
- Severe pallor
- Bleeding from any sites
- Major congenital
malformations
- Weight less than 1800 g
or more than 4 kg
- Transitional stools
- Posetting
- Minor birth trauma
- Superficial
infections
- Minor
malformations
- Jaundice
- All cases not
categorized as
Emergency/Priority
Emergency signs
Priority signs Non-urgent
signs Classify Initiate
Emergency
treatment
Assess and act
rapidly
Assess and
act rapidly
Act
Triage of a sick newborn or at-
risk newborn who presents at
SNCU
Reference standard: ME.11.1

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 9 of 39
10. Assessment and treatment of newborns displaying emergency
signs
ASSESS FOR EMERGENCY SIGNS
(In all cases)
TREAT EMEREGNCY SIGNS
TEMPERATURE Cold to touch (Abdomen) Rewarm hypothermic babies
Rapidly re-warm if there is sever
hypothermia(<320C) upto 350C and
then gradual re-warming
Make sure young infant is warm
IF + ve
AIRWAY &
BREATHING
Not breathing or gasping or
Central synopsis or
Severe respiratory distress
- Respiratory rate 70/min
- Severe lower in-chest
drawing
- Apnoeic spells
- Grunting
- Unable to feed
ANY SIGN
+ ve Manage airway
Provide tactile stimulation if apnoeic
If still apnoeic or gasping – provide PPV
Give oxygen
Make sure neonate is warm
Capillary refill longer than 3
seconds and
Weak and fast pulse (>160)
Convulsions
CIRCULATION
CONVULSIONS
IF + ve
IF CONVULSING
Give oxygen
Insert IV line and give 20ml/kg normal
saline over 30 min
Proceed immediately to full assessment
and treatment
Make sure neonate is warm
Manage airway
Check and correct hypoglycemia
Give anticonvulsant
Make sure neonate is warm
Reference standard: ME.G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 10 of 39
11. Neonatal transportation and referral from unit
S.No Activity Responsibility Record
1. Criteria for referral
2. Referral of Patients
If the baby requires further care or any surgical intervention that
cannot be provided at the hospital then the patient shall be referred to
a higher centre for specialist care.
Doctor,
Staff nurse
Referral slip
Ambulance shall be provided by the hospital for quick transportation
of patients.
Nursing staff ,
ambulance driver
Nil
An advance telephonic communication with the referral centre shall
be done to ensure the required service is available and intimate the
staff of the higher centre about the referral.
Staff Nurse List of contact details
of ambulance
The staff nurse shall document the referral details and coordinate for
the referral process.
Staff Nurse Refer In-Out register
The baby along with the referral slip and case sheet shall be referred
to the higher centre.
Staff Nurse Referral slip
The nursing staff shall also contact the referral centre and follow up
about the condition of the patient post referral.
Staff Nurse Refer In-Out register
Reference standard - ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 11 of 39
12. Requisition for diagnostics, collection & transfer of samples and
receiving of reports
S.No Activity Responsibility Record
1. Treating doctor shall prescribe the investigations in the requisition
form/doctor’s note and counter sign the same with name, date and
time.
Doctor Investigation requisition
form/doctor’s note
2. For laboratory test, the sample shall be collected by Nursing staff
following aseptic procedure. The sample shall be transported to
the lab by the ward boy/aaya by the use of transportation boxes.
The samples shall be labelled with the patient name, ID and test
name.
Nursing staff Sample dispatch register
3. For emergency test requisitions the labels shall be marked with
EM. and lab staff shall be intimated over the phone too.
Nursing staff Sample dispatch register
4. After all tests are done, reports shall be received from the
concerned diagnostic area as per the turnaround time for test.
Nursing staff Test Report
5. The reports received should be discussed with the doctor during
his/her rounds. In case of any critical results the doctor shall be
immediately intimated through phone or by a messenger
Nursing staff Test Report
Reference standard - ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 12 of 39
13. Thermoregulation of newborns
S.No Activity Responsibility Record
1. Prevention of hypothermia
Baby must be kept warm at all times , the following measures
should be followed for maintaining the warm chain
- Ensuring warm transportation during receiving at SNCU
- Warm resuscitation
- Adequate temperature maintenance inside the SNCU
- Ensuring timely Breast feeding
- Appropriate clothing and bedding
Skin-to skin contact with mother when required
Nursing staff Nil
2. Assessment of temperature and grading of hypothermia
Normally axillary temperature : 36.5 - 37.50C
Cold stress : 36.4 - 36.00 C
Moderate hypothermia : 35.9 - 320C
Severe hypothermia : < 320C
The warm and pink feet of the baby indicate that the baby is in
thermal comfort, but when the feet are cold and abdomen warm, it
indicates that the baby is in cold stress. In hypothermia, both feet
and abdomen are cold to touch.
Nursing staff Infant case sheet
3. Management of hypothermia
A hypothermic baby has to be re-warmed as quickly as possible
Set radiant warmer at 37- 380 C
Once baby’s temperature reaches 340C the re-warming process
should be slowed down.
Continue re-warming till temperature reaches normal range.
Monitor every 15-30 minutes
Monitor B.P, heart –rate, temperature and glucose
In addition
- Take measure to reduce heat loss
- Start IV 10% dextrose
- Give inj Vit K 1 mg I/M to term neonates & 0.5 mg I/M to
preterm
Nursing staff Infant case sheet

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 13 of 39
- Provide oxygen
4. Fever
- Fever (temp > 37.50C) can be a sign of infection, In all febrile
neonates, a diligent search for possible infection should be
made.
- In summer, Hyperthermia may occur due to raised
environmental temperature. For treating the same, move the
baby into colder environment.
- When the temperature is 37.50C- 39
) C, undress and expose
the neonate to room temperature.
- If the temperature is above 390
C, the neonate should be
undressed and sponged with tepid water at approximately 350C
until the temperature is below 380C.
- Monitor the temperature every hour.
Nursing staff Infant case sheet
Reference standard – ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 14 of 39
14. Nursing care
S.No Activity Responsibility Record
1. Correct Identification of patient
The correct identification of the baby shall be ensured at all point
of care and especially before initiating any invasive procedure.
Nursing staff Nil
Identification tag enlisting name of mother, and id no shall be
placed near newborn feet.
Nursing staff Sure tag
2. Timely and accurate nursing care
Treatment charts shall be maintained and updated. Drugs given
shall be documented in case sheet. The drug dosage given
should Co-relate it with drugs, time and doses prescribed.
Nursing staff Infant case sheet
3. Ensuring accuracy of verbal/telephonic orders
Verbal or telephone orders shall be accepted only on emergency
when it is impossible or impractical for the physician to write
them.
Nursing
staff , doctor
verbal order register,
Infant case sheet
Abbreviations should not be used when an order is given or
received.
Nursing
staff , doctor
verbal order register
Read back the order to the physician including the patient’s
name, treatment order/drug name and spelling of the drug to
avoid an error due to sound alike drugs, Dosage, pronouncing it
in single digits (e.g. 15 mg should be read as one five), route,
frequency (e.g. three times daily, not TID).
Nursing
staff
verbal order register
Document the order immediately including the date, time, and
physician’s name. Receiver’s name and signature.
Nursing
staff
verbal order register
Ensure the order is countersigned by the same doctor within 24
hours of communication of the verbal order.
Nursing
staff , doctor
verbal order register,
Infant case sheet
4. Nursing Hand-over
The nursing staff shall follow handing over formalities after every
shift. A Nursing hand-over register shall be maintained for the
same.
Nursing staff Nursing hand-over
register
During change of each shift, patient handover shall be given; A
practice of giving bedside patient handover shall be carried out.
Nursing staff Nursing hand-over
register

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 15 of 39
All details of baby’s condition, treatment given and care to be
given next shall be explained to the next nursing staff on-duty.
Nursing staff Nursing hand-over
register
All details explained shall be documented in the nursing hand-
over register and signature of the nursing staff giving and taking
handover shall be documented in the register.
Nursing staff Nursing hand-over
register
Reference standard - ME .E 4

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 16 of 39
15. Safe Drug Administration
S.No Activity Responsibility Record
1. Drug orders should be in capital letters, with dose and frequency of
administration mentioned. Error prone medical abbreviations should be
avoided.
Nursing staff Drug chart
2. Following parameters shall be verified before administration of drugs by
the person administering the drug
Written medication order (For verbal order refer the document ‘written
orders for medications’
General appearance (physical incompatibility) of the medicine for
administration (for e.g. melting, clumping etc.)
Patient identification
Dosage of medication
Route of administration
Time of administration
Nursing staff Drug chart, Nursing notes
3. All the medications administered in In-patients shall be documented in
drug order sheet and nurses chart
Nursing staff Drug chart, Nursing notes
4. In case of any adverse reactions, the treating doctor shall be notified as
soon as possible and details of the event shall be documented in the
incident reporting form.
Nursing staff Drug chart, Nursing notes
5. Any high risk medication shall be administered by/under the supervision
of a senior Nursing staff only.
Nursing staff Drug chart, Nursing notes
6. Close monitoring of the patient after the drug administration shall be
carried out.
Nursing staff Drug chart, Nursing notes
7. Safety of high alert drugs
- High alert drugs available in department shall be identified and a list
displayed near the medication tray.
- Electrolytes like Potassium chloride, Opioids, Neuro muscular
blocking agent, Anti thrombolytic agent, insulin, warfarin, Heparin,
Adrenergic agonist etc. as applicable.
- The list displayed should enlist name of high alert drugs available in
department, value for maximum doses as per age and prescribed
for.
- A system of independent double check of drugs should be followed
before administration.
Nursing staff List of high alert drugs
Reference standard - ME E.7.1

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 17 of 39
16. Fluid Management
S.No Activity Responsibility Record
1. Babies requiring IV fluid therapy
- Neonates with lethargy and refusal to feed
- Moderate to severe breathing difficulty
- Babies with shock
- Babies with severe asphyxia
Abdominal distension with bilious or blood stained vomiting
Nursing staff Infant case sheet
2. Choice of fluids
Give 10% dextrose for the initial 48 hours of life
After the age of 48 hrs if the baby is passing urine 5-6 times a day,
use commercially available IV fluid, such as IsolyteP.
If the premixed solution is not available or baby requires higher GIR
(Glucose Infusion Rate).
- Add normal saline (NS) 20ml/kg body weight (which
contains 3 meq of Na/kg) to required volume of 10%
Dextrose. Add 1ml KCl/100ml of prepared fluid.
- To calculate the necessary fluid volume, determine the
volume of fluid required for day of life. Provide this as
20ml/kg of NS and the remaining as 10% dextrose.
Nursing staff Infant case sheet
3. Administration of IV fluid
Use of micro drip infusion set which has a micro dropper (where 1ml
= 60 micro drops)
In this device, number of drops per minute is equal to ml of fluid per
hour e.g. If a baby needs 6 mL/hr provide 6 microdrops/minute
Before infusing Iv fluid check
- The expiry date of the fluid
- The seal of the infusion bottle
Calculate the rate of administration, and ensure that the micro
dropper delivers the fluid at the required rate.
Change the IV infusion set and fluid bag every 24 hours; even if the
bag still contains IV fluids (this can be a major source of infection).
Nursing staff Infant case sheet
4. Volume of fluids
Fluid requirement of neonates (ml/per kg body weight)
Day of life Birth weight >1500g Birth weight <1500g
1 60 80
2 75 95
Nursing staff Infant case sheet

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 18 of 39
3 90 110
4 105 125
5 120 140
6 135 150
7 150 150
5. Monitoring of baby receiving IV fluid
- Inspect the infusion site every hour
- Look for redness and swelling around the insertion site of the
canula, which indicates that the canula is not in the vein and fluid is
leaking into the subcutaneous tissues.
- If redness or swelling is seen at anytime, stop the infusion, remove
the canula, and establish a new IV line in a different vein.
- Check the volume of fluid infused and compare to the prescribed
volume, record all findings.
- Measure blood glucose every nursing shift i.e.6-8 hours.
- If the blood glucose is less than 45mg/dl, treat for low blood glucose
- If the blood glucose is more than 150 mg/dl on two consecutive
readings, change to 5% dextrose solution and measure blood
glucose in three hours.
- Weigh the baby daily, if the daily weight loss is more than 5%
increase volume of fluid by 10ml/kg body weight for one day
- If there is no weight loss or weight gain in the initial 3 days of life, do
not give the daily increment, keep fluid rate same as previous
- In case of excessive weight gain (3-5%) decrease fluid intake by 15-
20 ml/kg/day.
- Check the urine output, normally a bay passes urine 5-6 times every
day.
Nursing staff Infant case sheet
Reference standard - ME G4.2
Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 19 of 39
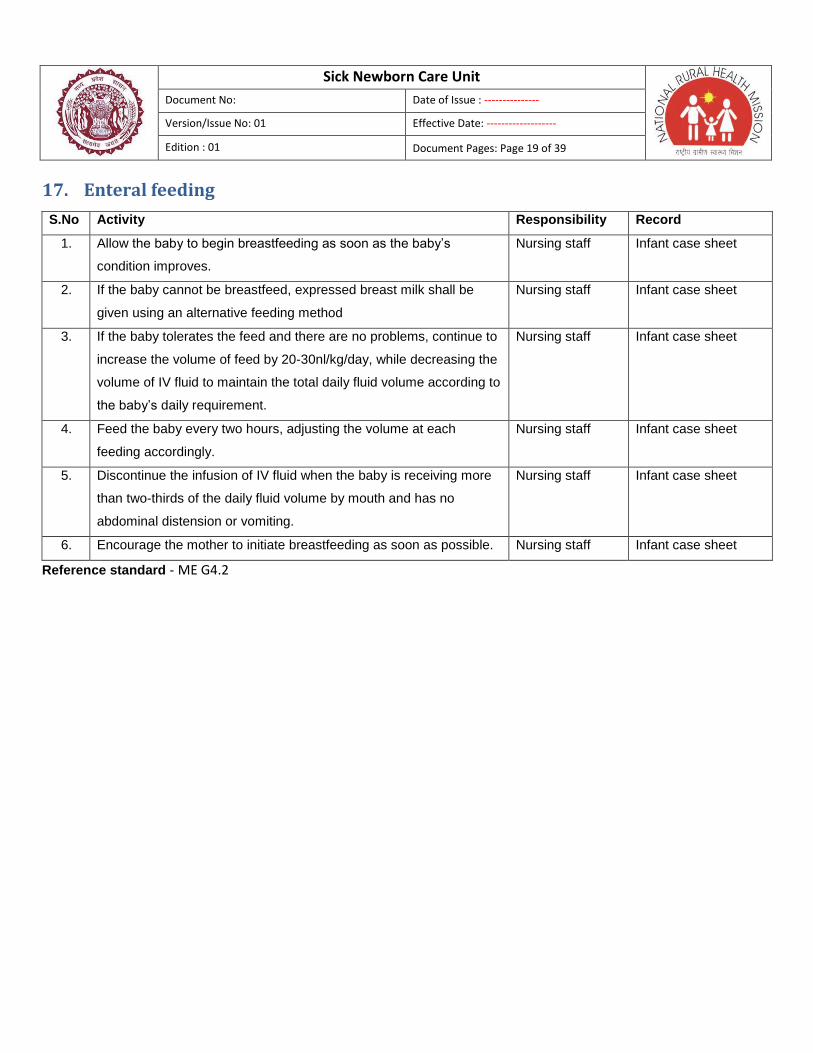
17. Enteral feeding
S.No Activity Responsibility Record
1. Allow the baby to begin breastfeeding as soon as the baby’s
condition improves.
Nursing staff Infant case sheet
2. If the baby cannot be breastfeed, expressed breast milk shall be
given using an alternative feeding method
Nursing staff Infant case sheet
3. If the baby tolerates the feed and there are no problems, continue to
increase the volume of feed by 20-30nl/kg/day, while decreasing the
volume of IV fluid to maintain the total daily fluid volume according to
the baby’s daily requirement.
Nursing staff Infant case sheet
4. Feed the baby every two hours, adjusting the volume at each
feeding accordingly.
Nursing staff Infant case sheet
5. Discontinue the infusion of IV fluid when the baby is receiving more
than two-thirds of the daily fluid volume by mouth and has no
abdominal distension or vomiting.
Nursing staff Infant case sheet
6. Encourage the mother to initiate breastfeeding as soon as possible. Nursing staff Infant case sheet
Reference standard - ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 20 of 39
18. Neonatal Resuscitation
S.No Activity Responsibility Record
1. - Transfer the baby to a warm clean, flat and dry surface.
- Provide warmth
- Position the baby
- Clear the airway
- Stimulate and reposition
For detailed procedure refer GoI’s work protocol for newborn
resuscitation.
Staff Nurse GoI’s work protocol for newborn resuscitation
2. Key to successful resuscitation Anticipation
Preparation
Call for help
Document /record
Be Fast
Be Gentle
Provide warmth
Maintain Hygiene
Staff Nurse GoI’s work protocol for newborn resuscitation
Reference standard - ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 21 of 39
19. Maintenance of Infrastructure of SNCU
S.No Activity Responsibility Record
1. SNCU shall have the following minimal infrastructure
- Waiting area
- Sitting area for patient relative
- Separate inborn & out born units
- Nursing station with receiving and examination room
- Ancillary areas like washing area, dirty & clean utiliy rooms, staff
room, staff and visitor changing area and breastfeeding room
Management, SNCU
In-charge
2. Safety of infrastructure
2.a. Seismic Safety
The SNCU shall ensure the seismic safety of the infrastructure.
Non structural components shall be properly secured.
SNCU In-charge, Nil
Fixtures and furniture like cupboards, cabinets, and heavy equipments, hanging objects shall be properly fastened and secured.
SNCU In-charge Nil
2.b. Safety of electrical establishment
SNCU shall not have temporary connections and loose hanging
wires
SNCU In-charge Nil
Periodical check / test of all electrical installation by electrical
Engineer/ maintenance staff shall be done once a week
SNCU In-charge &
maintenance staff
Maintenance
checklist
ICU shall have a dedicated earthling pit system available SNCU In-charge Nil
Wall mounted digital display shall be available in ICU to show earth
to neutral voltage
SNCU In-charge Nil
Quality output of voltage stabilizer will be displayed in each stabilizer
as per manufacturer guideline
SNCU In-charge Nil
Power boards shall be marked as per phase to which it belongs SNCU In-charge Nil
Floors of the ICU shall be non slippery and even and daily cleaning
done
SNCU In-charge &
housekeeping -Incharge
Nil
Windows/ ventilators if any shall be intact and sealed SNCU In-charge Nil
2.c. Fire safety
The I.C.U shall have a fire exit to permit safe escape to its occupant
at time of fire.
Management Nil
Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 22 of 39
Fire exits shall be clearly visible and routes to reach exit clearly
marked.
Management Nil
Smoke and heat detectors and fire extinguishers will be placed at
strategic locations in I.C.U for ensuring fire safety.
Management & SNCU
Incharge
Nil
3. Maintenance
The Incharge of the SNCU shall ensure the SNCU is adequately
maintained.
SNCU Incharge Nil
The in-charge shall check that there is no seepage, cracks, chipping
of plaster, window panes, doors and other fixtures are intact.
SNCU Incharge Nil
No condemned/Junk material in the SNCU SNCU Incharge Nil
For any infrastructural damage or problems like breakage, seepage
etc the maintenance staff & PWD shall be informed for repair
SNCU Incharge Nil
Reference standard - ME D4.1

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 23 of 39
20. Maintaining, updating of patients’ clinical records, their storage
and retrieval
S.No Activity Responsibility Record
1. Maintaining and updating of records
All the assessments, re-assessment, investigations, , treatment
and medication details shall be recorded and updated.
Nursing staff Associated forms and
formats
Standard forms and formats like treatment charts, surgery notes,
investigation chart, medicine register, nursing handover register,
referral register, transfer in-out register etc shall be maintained
Nursing staff Associated forms and formats
All records maintained shall be legible and complete in terms with
name and signature of staff making entry along with date and
time of entry.
Nursing staff Associated forms and formats
All registers/records shall be identified and numbered. Nursing staff Associated forms and
formats
2. Storage of records
All medical records of the patient shall be complete & legible with
proper name & signature of the author with date & time.
Nursing staff Infant case sheet
The patient information shall only be shared amongst the care
providers. While on use the files should be stored in nursing
station under the custody of the ward nursing staff.
Nursing staff Infant case sheet
On patient discharge the file shall be checked for completion and
sent to MRD for storage. Only copy of the discharge summary
shall be handed over to the patient during his discharge.
Nursing staff Infant case sheet
3. Retrieval of records
Access to clinical records of patient is allowed to entitled
personnel only on request. Whenever the clinical record of a
follow up patient is sought after by the treating doctor, he/she
shall fill in a record requisition register at MRD for availing the
same.
Nursing staff Record requisition
register
Reference Standard: ME.E8

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 24 of 39
21. Discharge from S.N.C.U to home
S.No Activity Responsibility Record
1. Discharge planning involves the following activities:
- Development of a care plan for post discharge care.
- Arranging for the provision of services, including
patient/family education and referrals.
- The Nurse in charge as well as the duty doctor shall be
responsible for coordinating the discharge with other team
members.
Treating Doctor Infant case sheet ,
investigation results,
nurses notes etc.
2. The following criteria shall be met by baby for discharge
- Baby is able to maintain temperature without radiant warmer
- Baby is hemodynamically stable (normal CFT, strong
peripheral pulses)
- Baby accepting breast feeds well
- Baby has documented weight gain for 3 consecutive days
and the weight is more than 1.5 kg
- Primary illness has resolved
- In addition to the above, mother should be confident of
taking care of the baby at home.
Treating Doctor Infant case sheet ,
investigation results,
nurses notes etc.
3. The Discharge process shall be planned in consultation with the
family members.
Treating Doctor,
Nursing staff
Infant case sheet ,
investigation results,
nurses notes etc.
4. Discharge planning shall be initiated on the basis of assessment
of baby’s condition.
Treating Doctor Doctor’s notes
5. Assessment of the baby shall be made for being ‘medically
stable’ and fit for discharge. This may include assessment of
functional, medical, medication, and nutritional needs.
Treating Doctor Patient vital sheets,
investigation results,
nurses notes etc
6. The Treating doctor shall write the discharge orders in the case
paper to initiate the necessary formalities for discharge.
Treating Doctor Doctor’s note
7. A Discharge Summary shall be prepared and signed by the
treating doctor or doctor on duty (in case of non availability of
treating doctor) and given to the parents/family members.
Treating Doctor/
Medical officer on
duty
Discharge Summary

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 25 of 39
8. A copy of discharge summary shall be attached with IP case
paper
Nursing staff Patient case sheet
9. Details of the discharge shall be entered in the discharge register Nursing staff Discharge register
10. The discharge summary shall contain the following information
- Details of the patient including Hospital IP Number
- Date of admission and date of discharge
- Name of the doctor in charge of the case
- Patient history
- Reason for admission.
- Significant findings.
- Diagnosis
- Investigation results.
- Details of any procedure performed.
- Medication.
- Other treatment given.
- Course in the hospital
- Follow up
a. Advice.
b. Medication
- Instructions regarding when and how to obtain urgent care
Management Discharge summary
form
11. During discharge, the parents should be counselled on
Medication intake, care at home, diet & nutrition, any medical
precautions & infection control measures and identifying
symptoms requiring immediate medical care.
Nursing staff Patient discharge
checklist
Reference Standard: ME.9.1, ME.9.2, ME.9.3, ME.9.4

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 26 of 39
22. Equipment Management
S.No Activity Responsibility Record
Calibration of Equipments
1. All the measuring equipments/ instrument shall be
calibrated.
SNCU –Incharge Nil
2. An ISO certified calibration agency shall be identified to
calibrate the equipments/instruments.
SNCU –Incharge Nil
3. Calibration labels/stickers shall be placed on the
equipment denoting the date of calibration and indicating
the status of calibration/ verification when recalibration is
due.
SNCU –Incharge Equipment register
4. All calibration certificates shall be maintained by the
Incharge or centrally stored by the Store-Incharge of the
hospital.
SNCU –Incharge Calibration certificate
5. The ward shall maintain an equipment register to
document details of equipment and calibration status.
SNCU –Incharge Equipment register
6. It shall be the duty of the Incharge to ensure updation of
calibration for all equipments as per their schedule.
SNCU –Incharge Equipment register
General Maintenance
7. Up to date manufacturer’s instructions for operation and
maintenance of equipments shall be kept in the
department so that the same can be readily available to
staff when required.
SNCU –Incharge Manufacturer’s instruction
8. Defective/Out of order equipments shall be labelled and
stored appropriately away from traffic area, until it has
been repaired
SNCU –Incharge
9. Daily dusting/ dry wiping of equipments shall be done by
housekeeping staff. The laboratory technician shall do a
daily check on the functioning of equipments every
morning before commencement of testing procedure.
SNCU –Incharge Nil
10. An equipment register shall be maintained to document SNCU –Incharge Equipment register

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 27 of 39
details of equipment - name, hospital code, and date of
installation, name of manufacturer, maintained in A
house/maintained by external agency or manufacturer,
Warranty Period, under AMC/CMC.
Preventive and Breakdown Maintenance
Preventive Maintenance
11. All equipments shall be covered under AMC/CMC
including Preventive maintenance.
SNCU –Incharge Equipment register
12. The lab-Incharge shall maintain an updated record on
AMC & Preventive maintenance in equipment register this
should include details like :
o Frequency of Preventive Maintenance/Calibration
- As per manufacturer guidelines
- Presently being followed
o Preventive Maintenance/Calibration Done On
o Preventive Maintenance/Calibration Due On
o Expenditure with cost and details
o Remarks with Functional Status
SNCU –Incharge Equipment register
13. Preventive maintenance shall be carried out as per
Maintenance Schedule for each individual equipment
based on manufacturer’s recommendations.
SNCU –Incharge Equipment register
14. The following shall be checked during a preventive
maintenance-
Physical condition of the equipment/ facility
lubrication, calibration, cleaning or replacing parts that
are expected to wear or which have a finite life
Maintenance report verification
Maintenance / Service report shall be obtained from
service agency and after verification marked as O.K. /Not
O.K.
SNCU –Incharge Equipment Service Report
Breakdown Maintenance
15. Faulty or defective equipment shall not be used regardless
of how minor is the problem and must be reported in the
first instance to the in-house maintenance engineer
SNCU –Incharge Equipment register

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 28 of 39
/outside agency hired for maintenance as soon as
possible and seen that the problem is attended to as soon
as possible.
16. A label of “out of order” shall be attached to the equipment
and information regarding breakdown shall be passed to
all staff including any shift changes.
SNCU –Incharge Nil
17. On restoration of the equipment, the Equipment
Breakdown Record should be updated. This indicates that
the breakdown/maintenance is performed of the
equipment.
The “out of order” sticker shall be removed after the
restoration of the equipment.
SNCU –Incharge Nil
18. All the breakdowns occurring in the department should be
maintained in the equipment register and include the
following
Breakdown Date and Time
Breakdown Details (Technical fault or other reasons)
Date and Time of Rectification
Total Time Taken (Rectification Time – Breakdown
Time)
Rectification Details with expenditure including cost (if
any)
Remarks with functional status
Reasons for delay if any
SNCU –Incharge Equipment register
Reference Standard: ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 29 of 39
23. Storage and Inventory management of drugs and consumables
S.No Activity Responsibility Record
Inventory Management
1. All drugs and consumables to be used shall be stored under the
supervision of ward Incharge in cupboards at ward store
room/nursing station.
SNCU -Incharge,
Nursing staff
Stock register
2. The stock stored shall be kept in original packages/labelled containers
on labelled racks.
SNCU -Incharge,
Nursing staff
Stock register
3. Stock level shall be daily checked and updated in a stock register. The
expiry date for each batch of drugs shall also be mentioned in the
register.
Ward-Incharge,
Nursing staff
Stock register
4. A system of timely forecasting and indenting of drugs and
consumables shall be practiced .The ward Incharge shall ensure there
is a buffer stock available for emergency use before putting an indent
for new stock.
Ward-Incharge Stock register
5. A crash cart for storage of emergency drugs equipment and
consumables shall be maintained and a crash cart checklist shall be
used for daily (in very shift) stock checking and updation of the same.
Ward-Incharge,
Nursing staff
Crash cart
checklist
Storage of drugs and consumables for daily use
6. All drugs and consumables required for daily use shall be kept neatly
arranged in a medicine trolley.
Nursing staff Nil
7. The all drug and consumable containers shall be labelled. Nursing staff Nil
8. A medicine trolley register shall be maintained to record details of
usage.
Nursing staff Medicine trolley
register
Reference Standard: ME D.2.1, ME D.2.5
24. Purchase of external services & supplies
Refer SOP in pharmacy & store manual

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 30 of 39
25. Infection control practices
S.No Activity Responsibility Record
1. Linen Management
For linen management refer SOP Auxiliary services Linen & Laundry
6.3.1,6.3.2,6.3.3
Nursing staff SOP Auxiliary
services
2. Hand Hygiene
- Availability of wash basin with running water, soap, clean
towel/tissue paper/hand dryer shall be ensured at the casualty.
- Poster depicting steps of hand washing shall be displayed near all
wash basins.
- All staff involved in patient care shall be trained on hand hygiene
practices.
- The Infection control nurse shall monitor for adherence to hand
hygiene practices.
- Alcohol based Hand rubs shall also be made available .
- Mothers shall be educated to practice hand washing with soap.
Nursing staff Hand hygiene
monitoring
checklist
3. Standard practices and materials for antisepsis
- Antiseptic solutions shall be made available at all patient care
points.
- Proper cleaning of procedure site with antisepsis like before giving
IM/IV injection, drawing blood, putting Intravenous lines.
Nursing staff Nil
4. Use of PPE
- The staff should always adhere to the use of PPE like gloves,
uniform. Apron, mask, shoe cover/sterile slipper & caps.
- No reuse of disposable gloves, masks, caps and aprons shall be
practiced.
- Compliance to correct method of wearing and removing the gloves
should be practiced
Nursing staff Nil
5. General cleaning
- Wet mop floor using detergent and standard
disinfectant/0.5%chlorine solution.
- Clean all furniture and lights using warm water, detergent and
Housekeeping
staff
Housekeeping
checklist
Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 31 of 39
disinfectant/0.5% chlorine solution every morning.
- Clean the toilets and corridor daily with detergent water and
disinfectant.
- Prepare cleaning solutions daily or as needed, and replace with
fresh solution frequently.
- Cleaning equipments like broom shall not be used in patient care
areas.
- Three bucket system for mopping should be used.
- Unidirectional mopping from inside out should be practiced.
- Any cleaning equipment leading to dispersion of dust particles in air
should be avoided.
Terminal cleaning
- Use vacuum cleaner to clean the AC Vent and ducts if available,
once in a month.
- Wet-dust horizontal surfaces by moistening a cloth with a small
amount of a recommended hospital detergent/disinfectant.
- Avoid dusting methods that disperse dust (e.g., feather-dusting).
Housekeeping
staff
Housekeeping
checklist
6. Waste Management
The following colour - coding system shall be used in waste
management segregation.
Blue Bag:
Syringes
Tubings
Saline bottles
Puncture Proof containers: White
Broken glass articles
Medicine vials
Needles (to be disposed only after burning)
Scalpels
Metal articles, like forceps to be disposed.
Yellow Bag:
Blood stained bandages, gauze, cotton, tissues, and gloves
Housekeeping
staff
Nil

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 32 of 39
Infectious wastes
Black Bag:
Paper
Plastic & other general waste
8. Microbiological surveillance
As an infection control measure to check the sterility of the environment
and surfaces in S.N.C.U, swabs shall be collected from patient care
surfaces,utilities,floor,instruments & A.C vent to be sent for
microbiological culture surveillance .
Infection control
nurse/
SNCU- Incharge
Culture
sensitivity report
9. Water testing
Once in a month overhead water tank cleaning and water testing shall
be done to check sterility of water.
Infection control
nurse/
SNCU-Incharge
Water testing
report
10. Processing of equipments and instruments
- Procedure surface like baby basiinets, warmers, phototherapy units,
laryngoscope, oxygen hood and other instruments used shall be
wiped with 5% chlorine solution.
- Instruments like ambubag, suction canula, Surgical Instruments
shall be decontaminated by Soaking in 0.5% Chlorine Solution/
Wiping with 0.5% Clorine Solution or 70% Alcohol as applicable.
- Contact time for decontamination shall be maintained to 10 minutes.
- The instruments should be cleaned after decontamination with
detergent and running water.
- Cleaned instruments shall be sent to TSSU/CSSD for autoclaving
and sterilization.
Infection control
nurse/
SNCU -Incharge
11. Use of standard disinfectants
- Standard disinfectants like chorine solution, sodium hypochlorite
solution, phenyl , formaldehyde/gluteraldehyde should be used
Infection control
nurse/
FP OT-Incharge
12. Restricted entry
- Taking into consideration infection control measures and prevention
of overcrowding only one attendant at a time shall be allowed to
meet the patient.
Incharge, nursing
staff
Nil

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 33 of 39
- Visitors shall be allowed entry only during visiting hours as per the
visiting policy
- Keeping in purview the infection control practices the attendant shall
have to change into sterile gowns, mask & slippers before entering
into the patient zone
- Hand washing shall be advocated before and after visiting the ICU
for the visitors.
Reference standard - ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 34 of 39
26. Prevention of Child Abduction
S.No Activity Responsibility Record
Restricted Entry in SNCU
1. The SNCU shall at all times ensure limited entry inside SNCU, i.e. only
identified SNCU staff shall be available at SNCU. The staff should
always wear their Id tag. No outsiders shall be allowed. In any
exceptional case if required, visitors are permitted entry only on
approval of Incharge/duty doctor and shall have to be accompanied by
a SNCU staff during the visit.
SNCU –Incharge,
Duty doctor
Staff duty roaster
Visitor register
2. The baby’s family members shall be allowed entry inside the SNCU
during visiting hours only.
SNCU –Incharge,
nursing staff
Visitor register
3. Aside from the visiting hours, only the baby’s mother can be allowed to
meet baby for feeding.
SNCU –Incharge Nil
4. Family members shall be allowed to visit the baby only when
accompanied by any one of the parent or if identified by the parents as
their family member. However entry of only one family member at a
time shall be allowed inside SNCU.
SNCU –Incharge Visitor register
Correct identification
Baby identification at labour room/OT
5. Correct identification of the newborn shall be initiated immediately
after birth at labour room/OT.
Labour room/OT
nursing staff
Labour room/OT
register , Patient
case sheet
6. Immediately after Baby birth details shall be entered in the case sheet,
(Recording date and Time of Birth, Weight of baby). An identification
tag shall be placed on baby’s ankle. Mother shall be shown the baby
and family members intimated about the baby’s birth and shown the
baby.
Labour room /OT
nursing staff
Labour room/OT
register, Patient
case sheet
Baby identification at SNCU
7. The SNCU staff should verify the details on the baby tag and that on
the mother’s case sheet during receiving the baby.
SNCU nursing
staff
SNCU register
8. The nursing staff at SNCU shall ensure the baby tag is intact at all times, if any damage the same shall be immediately replaced with a new one by verifying details with the baby’s case sheet.
SNCU nursing
staff
SNCU register,
infant case sheet
Reference standard - ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 35 of 39
27. Quality assurance
S.No Activity Responsibility Record
1. Department Incharge shall be vigilant about the key characteristics.
Based on the observation, every month Department-Incharge shall
record his / her remark against the key characteristics as to whether
the key characteristics meet the acceptance norms or not. Specific
comments for the key characteristics may also be written.
Incharge Nil
2. All reports shall be verified and signed by the radiologist/sonologist
and then dispatched.
Incharge Reports
3. These quality indicators relating to productivity, efficiency, safety,
service etc shall be maintained by the technicians and reviewed by the
Incharge:
- Inborn admission rate - Proportion of admissions which are out born - Bed Occupancy Rate - Proportion of female babies admitted - LAMA rate for female babies - Proportion of BPL Patients - Proportion of very low birth weight babies - Down time Critical Equipments - Bed Turnover Rate - Referral Rate - Survival rate - No. of drug stock out in SNCU - Average waiting time for initial assessment of newborn - Proportion of newborn deaths among inborn - Proportion of newborn deaths among outborn - Case Fatality Rates - Proportion of asphyxiated newborn babies admitted out of
deliveries conducted at facility - Average length of stay - No of Adverse events reported - % of environmental swab culture reported positive - Average length of stay
- Antibiotic use rate
Incharge Indicator register
4. Internal Audits
o Audits shall be conducted as per pre scheduled audit plan and
organized and carried out by designated internal auditors.
o While planning Audit it should be ensured that the internal
auditors do not audit their own activities.
Auditor & Auditee Internal Audit
report
CAPA report

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 36 of 39
o A Quality management system procedure for Internal Audit
shall include the following
Selection of Internal Auditors.
Criteria for Internal Auditors.
Audit Planning and methodologies.
Audit recording, non-conformance and summary report
preparation.
o Where audit findings indicate deficiencies or the opportunity for
improvement corrective or preventive action is promptly taken,
this is documented and carried out within an agreed upon time.
Note: Refer Internal Audit procedure in Lab Manual for details
Reference Standard: ME G4.2

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 37 of 39
Annexure:
I. Housekeeping protocol

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 38 of 39

Sick Newborn Care Unit
Document No: Date of Issue : ---------------
Version/Issue No: 01 Effective Date: -------------------
Edition : 01 Document Pages: Page 39 of 39
II. Clinical protcols