Embed Size (px)
DESCRIPTION
Why Essential Newborn Care? What is Essential Newborn Care?. Subodh S Gupta MGIMS, Sewagram. “Fate has allowed humanity such a pitifully meagre coverlet that in pulling it over one part of the world, another has to be left bare … ” Rabindranath Tagore. 4 million newborns die each year. - PowerPoint PPT Presentation
Citation preview

Why Essential Newborn Care?
What is Essential Newborn Care?
Subodh S GuptaMGIMS, Sewagram

“Fate has allowed humanity such a pitifully meagre coverlet that in pulling it over one part of the world, another has to be left bare
… ” Rabindranath Tagore

4 million newborns die each year
1.5 million (38% of all newborn deaths) occur in 4 countries of South Asia

Inequity in maternal and newborn healthThe health of the mother and newborn is inseparable

0
20
40
60
80
100
1983 2000 1983 2000
Post-neonatal mortality
Late neonatal mortality
Early neonatal mortality
Developing Regions
Developed Regions
Source: RHR/WHO, 2003
Deaths among infants under 7 days are decreasing more slowly than among older infants

Infant and Neonatal Mortality
0
20
40
60
80
100
120
140
1976 1980 1982 1984 1986 1988 1990 1992 1994 1995 1997 1998
Year
Per
100
0 liv
e b
irth
s
IMR NMR

SEARCH Study• Trained VHW/1000
population• Intervention
– Birth asphyxia– LBW– Temp. maintenance. – promotion of breast
feeding– prevention of
superficial infection– Management of sepsis – Health education
0
10
20
30
40
50
60
70
Baseline 1st year 2nd year 3rd year
intervention control area

4 million newborn deaths – Why?almost all are due to preventable conditions
Two thirds of all neonatal deaths are in LBW infants

Prematurity15%
Asphyxia20%
Sepsis52%
Others13%
Causes of Neonatal MortalityCauses of Neonatal Mortality

When do they die?Up to 50%
of neonataldeaths are in
the first 24 hours
75% of neonatal deaths are in
the first week – 3 million deaths

Newborn Deaths from Asphyxia:the tip of an iceberg
0.9 million asphyxia deaths
1-2 million suffer medium to long–term impairment
Stillbirths from intrapartum hypoxia(~ 1 million deaths)

Three dimensions of poverty
• Poverty of means and access• Poverty of Hope!• Poverty of Imagination

REASONS FOR NOT SEEKING CARE (n=31)
13%
3%
6%
16%
23%
33%
6%
BABY NOT CONSIDERED ILL ENOUGH TO SEEK CARE
MONEY UNAVAILABLE
TRANSPORTATION UNAVAILABLE
POOR OPINION/ PREVIOUS NEGATIVE EXPERIENCE OF HEALTH SYSTEM
FATALISM (BELIEF THAT CHILD WILL DIE ANYWAY)
NO PERMISSION FROM HUSBAND/ IN LAWS/ NOBODY AT HOME TO TAKE CARE OF OTHER CHILDREN
DIED TOO SOON AFTER BIRTH
39%Fatalism Past experience
30%Empowerment Support structures

What can be done?

Evidence-based Interventions to Reduce Newborn Deaths
Infection36%
Sepsis/PneumoniaTetanusDiarrhea
Asphyxia23%
Other7%
Complications of Prematurity
27%
Cong. Anom
7%
Low birth weight is a significantcontributor in 40–70% of neonatal deaths.
Tetanus Toxoid Immunization of MotherClean DeliveryCord CareEarly & Exclusive BreastfeedingAntibiotics for mother and baby
Warming ResuscitationSkilled Birth Attendants
Syphilis Control Folate Supplementation
Adapted from Lancet 2005
Malaria ControlAntenatal CorticosteriodTreatment of Bacteriuria
Kangaroo Mother CareBirth SpacingMaternal Nutrition

Evidence of effectiveness Evidence of effectiveness of Home Based Neonatal of Home Based Neonatal
CareCareStudy Place NNMR/1000 LB
Risk approach strategyin neonatal care
Puneexperience(WHO study)
52 to 39
Rural neonatal care Dahanuexperience
57 to 34
Home based neonatalcare and sepsismanagement
Gadchiroliexperience
62 to 25

SEARCH StudySEARCH Study• Trained VHW/1000 Trained VHW/1000
populationpopulation• InterventionIntervention
– Birth asphyxiaBirth asphyxia– LBWLBW– Temp. maintenance. Temp. maintenance. – promotion of breast promotion of breast
feedingfeeding– prevention of prevention of
superficial infectionsuperficial infection– Management of Management of
sepsis sepsis – Health educationHealth education
0
10
20
30
40
50
60
70
Baseline 1st year 2nd year 3rd year
intervention control area

Effective interventions for Newborn CareLancet Series on Newborn Survival
Paper 2 (2005)
• 16 interventions identified with adequate evidence of effect on neonatal deaths (e.g., tetanus toxoid immunization, clean delivery, obstetric care, breastfeeding, antibiotics for infections)
• All are highly cost-effective especially if packaged and delivered within other programmes (e.g., maternal and child health)
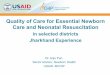
Referral HospitalTertiaryUniversity Hospital
SecondaryDistrict General HospitalTaluka Hospital
PrimaryRural Health Center
Basic Health Units
Clinical or Facility-based care
Outreach
Family and Community
Packages

Intervention PackagesSkilled obstetric and immediate newborn care including resuscitation
Emergency obstetric care to manage complications such as obstructed labour and hemorrhage
Antibiotics for preterm rupture of membranes#
Corticosteroids for preterm labour#
Emergency newborn care for illness, especially sepsis management and care of very low birth weight babies
Cli
nic
al
care
Folic acid #
Counseling and preparation for newborn care and breastfeeding, emergency preparedness
Healthy home care including breastfeeding promotion, hygienic cord/skin care, thermal care, promoting demand for quality care
Extra care of low birth weight babies
Case management for pneumonia
Fam
ily
-co
mm
un
ity
Clean home delivery
Simple early newborn care
15 - 32%
4-visit antenatal package including tetanus immunisation,detection & management of syphilis, other infections, pre-eclampsia, etc
Malaria intermittent presumptive therapy*
Detection and treatment of bacteriuria#
Ou
trea
ch
serv
ices
Postnatal care to support healthy practices
Early detection and referral of complications6 - 9%
23 - 50%NMR effect
InfancyNeonatal periodPre- pregnancy PregnancyBirth
Administering basic community-based intervention packages at full coverage can save ~ 37% of all newborn deaths!

Coverage rates are low!
How can these be scaled-up much faster?

Know ….Do gap Don’t know….Don’t do gap

30% reduction in neonatal mortality!Major impact on maternal mortality!

Shivgarh (India) Trial Community Mobilization and Behavior Change Communication
1. Birth preparedness for essential newborn care
2. Clean delivery, cord and skin care
3. Immediate wiping, drying and keeping the baby warm
4. Skin-to-Skin Care
5. Promotion of immediate and exclusive breastfeeding
6. Recognition and management of hypothermia

Shivgarh (India) Trial Community Mobilization and Behavior Change Communication
1. Birth preparedness for essential newborn care
2. Clean delivery, cord and skin care
3. Immediate wiping, drying and keeping the baby warm
4. Skin-to-Skin Care
5. Promotion of immediate and exclusive breastfeeding
6. Recognition and management of hypothermia
0
20
40
60
80
100
120
Control Intervention 1 Intervention 2
Perinatal Mortality Rate Neonatal Mortality Rate

27 Normal Newborn Care
Essential Newborn Care Interventions
• Clean childbirth and cord care– Prevent newborn infection
• Thermal protection– Prevent and manage newborn hypo/hyperthermia
• Early and exclusive breastfeeding– Started within 1 hour after childbirth
• Initiation of breathing and resuscitation– Early asphyxia identification and management

28 Normal Newborn Care
Essential Newborn Care Interventions (continued)
• Eye care– Prevent and manage ophthalmia neonatorum
• Immunization– At birth: bacille Calmette-Guerin (BCG) vaccine, oral
poliovirus vaccine (OPV) and hepatitis B virus (HBV) vaccine (WHO)
• Identification and management of sick newborn• Care of preterm and/or low birth weight newborn

Cleanliness to Prevent Infection• Principles of cleanliness essential in both home and health
facilities childbirths• Principles of cleanliness at childbirth
– Clean hands– Clean delivery surface– Clean cord cut– Clean cord clamp– Clean cord care– Clean perineum– Nothing unclean introduced vaginally
• Infection prevention/control measures at healthcare facilities

Thermal Protection• Newborn physiology
– Normal temperature: 36.5–37.5°C– Hypothermia: < 36.5°C– Stabilization period: 1st 6–12 hours after birth
• Large surface area• Poor thermal insulation• Small body mass to produce and conserve heat• Inability to change posture or adjust clothing to respond to thermal
stress
• Increase hypothermia– Newborn left wet while waiting for delivery of placenta– Early bathing of newborn (within 24 hours)

31 Normal Newborn Care
Hypothermia Prevention
• Deliver in a warm room• Dry newborn thoroughly and wrap in dry, warm
cloth• Keep out of draft and place on a warm surface• Give to mother as soon as possible
– Skin-to-skin contact first few hours after childbirth– Promotes bonding– Enables early breastfeeding
• Check warmth by feeling newborn’s feet every 15 minutes
• Bathe when temperature is stable (after 24 hours)
Early and Exclusive Breastfeeding
• Early contact between mother and newborn – Enables breastfeeding– Rooming-in policies in health facilities prevents
nosocomial infection
• Best practices– No prelacteal feeds or other supplement– Giving first breastfeed within one hour of birth– Correct positioning to enable good attachment of the
newborn– Breastfeeding on demand– Psycho-social support to breastfeeding mother
33 Normal Newborn Care
Breathing Initiation and Resuscitation
• Spontaneous breathing (> 30 breaths/min.) in most newborns– Gentle stimulation, if at all
• Effectiveness of routine oro-nasal suctioning is unknown– Biologically plausible advantages – clear airway– Potentially real disadvantages – cardiac arrhythmia
– Bulb suctioning preferred
• Newborn resuscitation may be needed– Fetal distress
– Thick meconium staining– Vaginal breech deliveries
– Preterm
Hamilton 1999.

34 Normal Newborn Care
Eye Care To Prevent or Manage Ophthalmia Neonatorum
• Ophthalmia neonatorum– Conjunctivitis with discharge during first 2 weeks of life
– Appears usually 2–5 days after birth
– Corneal damage if untreated
– Systemic progression if not managed
• Etiology– N. gonorrhea
• More severe and rapid development of complications
• 30–50% mother-newborn transmission rate
– C. trachomatis
35 Normal Newborn Care
Eye Care To Prevent or Manage Ophthalmia Neonatorum (continued)
• Prophylaxis– Clean eyes immediately– 1% Silver nitrate solution
• Not effective for chlamydia
– 2.5% Povidone-iodine solution– 1% Tetracycline ointment
• Not effective vs. some N. gonorrhea strains
• Common causes of prophylaxis failure– Giving prophylaxis after first hour– Flushing of eyes after silver nitrate application– Using old prophylactic solutions

Immunization
• BCG vaccinations in all population at high risk of tuberculosis infection
• Single dose of OPV at birth or in the two weeks after birth
• HBV vaccination, wherever possible

37 Normal Newborn Care
Summary
The essential components of normal newborn care include:
• Clean delivery and cord care
• Thermal protection
• Early and exclusive breastfeeding
• Monitoring
• Eye care
• Immunization

Thank youThank you
![RESEARCH ARTICLE Open Access Is essential newborn care ... · essential newborn care [7-12]. Increased access to some components of newborn care for women giving birth at home without](https://img.dokumen.tips/doc/110x75/5fd7e7606465f95cbc178f5f/research-article-open-access-is-essential-newborn-care-essential-newborn-care.jpg)