Embed Size (px)
Citation preview

Slide 1
Shoulder InstabilityMechanical or Neurological
John Zavala, M.D.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 2 Shoulder Instability
Anterior
Posterior
MDI
Neurological
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3 Ligamentous and labrum
restraints
Capsulolabral complex
“Bumper”- deepens glenoid
Glenohumeral ligaments
Inferior GHL
• Ant and post bands
• Axillary pouch
Middle GHL
Superior GHL
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 4 Ligamentous and labrum
restraints
Rotator Interval
SGHL
CHL
Borders of
supraspinatus and
subscapularis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 5 Shoulder Instability
Instability: An increase of the normal
translation of the humeral head over the
glenoid in one or multiple directions
which has become disabling to the patient.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 6 Shoulder Instability
Traumatic
Unidirectional
Anterior
Posterior
Bankart (labral)
lesion
Surgery
Atraumatic
Multidirectional
Bilateral (?)
Rehab
Inferior capsular shift
Interval closure
Thomas and Matsen: JBJS, 1989
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 7 Shoulder Instability
Defining the problem
Direction - anterior, posterior, ± inferior
Degree – dislocation or subluxation
Onset – traumatic or atraumatic
Volition
Acute or Chronic (recurrent)
Hawkins
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 8 Shoulder Instability
Defining the problem
Direction - anterior, posterior – or both
Degree – dislocation or subluxation
Onset – traumatic or atraumatic
Volition
Acute or Chronic
Disabling ?
Past treatments and outcomes
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 9 Shoulder Instability
Making the diagnosis
HISTORY of problem
EXAM
Studies – x-ray, MRI
“Anterior
Instability”
99-100%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 10 Shoulder Instability
Exam
Observation, palpation, AROM, PROM,
strength
Special testing
• Glenohumeral translation
• Provacative tests
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 11 Shoulder Instability - Exam
Glenohumeral (GH) translation
“normal” = up to 1 cm in each direction: anterior, posterior and inferior
• 17-29% translation Humeral Head over glenoid. Hawkins: JSES, ‘96
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12
ASES
Grades
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 13 Shoulder Instability
GH translation - Grading
Anterior-posterior: Load and Shift Hawkins
• Up the face – grade 1= “normal”
• To the rim, perch – grade 2
• Over the rim – grade 3
Inferior – sulcus
• HH to acromion distance
– centimeters, grade 1-3
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 14
Laxity or
Excessive
Translation
Does Not
Equal
Instability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15 GH translation Anterior and Posterior
Load and Shift –
sitting or supine
Grade 1- up face
Grade 2- to rim
Grade 3- over rim
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 16 GH translation – Inferior “Sulcus Sign”
Inferior translation
Interval lesion
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 17 GH translation – Inferior
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18 Provocative Testing: Instability
ANT: Apprehension-Relocation
Abduction - ER reproduces
symptoms
Posterior force relieves symptoms
POST:
Jerk test
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 19
Apprehension Relocation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 20 Beware
Multi-Directional Instability
Hyperflexibility
• Palms to floor
• Thumb to wrist
• Hyperextension of elbows
• Patellar hypermobility
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21 Imaging
Plain Film
Bony Bankart
Orthogonal views
Hill Sachs lesion
Axillary lateral view
A
P
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 22 Imaging
MRI
Labral tear
• Bankart, SLAP
Glenoid insufficiency,
version (CT better)
Hill Sachs
Interval lesion
Rotator cuff integrity
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 23 Abnormal Glenoid Version
ANT
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24
Anterior Shoulder Instability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 25 Anterior Instability: Mechanism of Injury
FOOSH
AbER injury
Direct Trauma
Subtle Overuse
“Microinstability”
Throwers
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 26
Anterior Instability - History
Subluxation vs
Dislocation
ER reduction
“Popped it in
myself”
“Went in and out”
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27 Anterior Instability
Pathoanatomy
Bankart Lesion
Capsulolabral complex
off glenoid
Classic lesion
Not present in all patients
ALPSA lesion
Medialized anteroinferior
capsulolabral attachment
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 28 Anterior Shoulder Instability
Bankart: The British Medical Journal, 1923• humeral “head shears off the fibrous capsule of the joint
from its attachment to the fibro-cartaliginous glenoid
ligament….there is no tendency for the detached capsule to unite spontaneously with the fibro-
cartilage… the defect in the joint is therefore permanent, and the head of the humerus is free to move forwards over the anterior rim of the
glenoid cavity on the slightest provocation.”
“The Essential Lesion”
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 29 Anterior Instability Superior Lesion
Tear/deficiency of
interval capsule
± SLAP
Restraint to inferior
translation
Sulcus sign
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 30 Anterior Instability HAGL Lesion
Humeral Avulsion
of Glenohumeral
ligaments
Pre-op MRI
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 31 Anterior Instability – Treatment Decision
Operative vs Non-operative Management
Multi-factorial and Controversial
Acute, first time
Recurrent
Concomitant injuries
Age and Activities
Risk of future problems-with or without surgery
Timing
Degree of Disability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 32
Anterior Instability
Recurrence Rates - AGE
Skeletally immature:
near 100%
< 22: 85-95%
23-40 ?
> 40: low
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33 Anterior Instability Non-Op Treatment
Indications
In season / pre-
season athlete
Low risk of
recurrence
Player decision
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 34
Surgery
Significant disability
Failure of cons Rx ??
“Essential”
Pathology for
recurrence
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 35 Arthroscopic Reconstruction
Immobilization
2-4 weeks
Rehabilitation
Return to full
activity 4-6
months
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 36 Anterior Instability Outcomes
Non-operative vs Operative
USMA – 1st time Anterior dislocation, 3 yr f/up
12 Non-op
4 weeks immobilization, then rehab
9/12 (75%) recurrence. 6/9 onto scope repair.
9 Scope, Bankart repair
1/9 recurrence (11.1%)
Bottoni, CR. AJSM July 2002
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 37
Arthroscopic Bankart Repair
10 % recurrence
2 years
72 patients
Mean age 26
Carreira DS, et al AJSM,
May 2006
4% recurrence
3 ½ years
167 patients
> 90% RTPLP
Kim, SH, et al AJSM, Aug
2003
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 38 Anterior Instability
Arthroscopic vs Open
4 ½ years, 59 patients
Surgery procedure bias
Scope-EUA only Ant
Open- EUA Ant + Inf.
Recurrence
24 % scope
18 % open
All re-injuries w/contact sport
Cole, BJ. JBJS Aug 2000
No recurrence either group
2 groups of 30 patients
2 years
Prospective/randomized
Increased loss of motion
Open group
Fabbriciani, C. JBJS. Nov 2003
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 39 Anterior Instability
Arthroscopic vs Open
64 consecutive patients prospective/randomized to Open
(32) or Scope (32) stabilization.
Had failed 6 months rehab
At avg. 32 months: No recurrent anterior dislocations
either group
OPEN: OR time 159 minutes, slightly less ROM.
• 2 “failed” (1-recurrent ant. Instability, 2-traumatic post. d/l)
SCOPE: OR time 59 minutes. 1 “failed” -Painful
Bottoni, CR. AJSM, Nov. 2006
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 40 Arthroscopic Bankart Repair
Contact and Collision Athletes
11 % recurrence
2 of 18 patients, both
collision - football
3 years
Mean age 20
± RI closure
Mazzocca, AD, AJSM Jan 2005
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 41 Anterior Instability – Collision
Arthroscopic vs Open
Recurrence
25% Scope (4/16)
12.5% Open (4/32)
Mean f/up at 6 years
Mean age 20
Rhee YG. AJSM June 2006
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 42 Anterior Instability: Questions
Non-op sling/brace position: IR or ER?
Decision for Surgery—
Analogous to ACL in the active patient?
Justified to repair 1st time dislocation in younger patients with “essential” pathology?
Prophalaxis for future disability?
Is Scope now the gold standard? Ability to address SLAP
Rotator Interval repair only for chronic/recurrent?
When to open?
Bony Bankart: Size (25%) –Screws or Anchor tech.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 43
Posterior Shoulder Instability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 44 Posterior Instability
Rare in isolation
2-4% of instability
Much more common:
Multidirectional with
predominant
posterior component
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 45 Posterior Instability Classification
Acute Posterior Dislocation
Chronic Locked Dislocation
Recurrent Subluxation
Voluntary
• Habitual- ? psychiatric issues
• Muscular Control
Involuntary
• Positional- can demonstrate
• Non-positional- “can’t show you”
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 46 Posterior Instability Mechanism
Traumatic
Football linemen
• Recurrent subluxation
“microinstability”
Seizures
Electrocution
Subluxation or dislocation
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 47 Posterior Instability Recurrent (rare?)
Pathoanatomy
Posterior-inferior labrum
/ ligaments
“reverse Bankart”
Rotator Interval tear /
laxity
Glenoid bone deficiency
inferior
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 48 Posterior Instability Acute Dislocation
Post-reduction:
ER Brace 4-6 weeks
• 5 degrees ext
• 20-30 deg ER
• Rehab
Recurrence
uncommon
Recurrent Instability
posterior repair /
reconstruction
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 49
Recurrent Posterior Instability Treatment
Usually Non-operative
Therapy
Surgical Repairs
Open vs Arthroscopic
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 50 Interval Closure
All posterior instability
procedures
Decreases inferior and
posterior translation
Harryman JBJS, ’92
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 51 Interval : Beach chair
J. Abrams, MD
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 52 Recurrent Posterior Instability
Surgical Outcomes
Generally good results
Open: Recurrence 11-36%
• Some studies included MDI patients and/or
osteotomy procedures
Arthroscopic: Recurrence 4-25%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 53
Multidirectional Instability
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 54 Multidirectional Instability
Disabling subluxation or dislocation
• At least 2 of 3 directions
• Always excessive inferior translation
(sulcus) Neer
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 55
Multidirectional Instability Sulcus Sign
ACROMION
HUMERAL
HEAD
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 56 Multidirectional Instability Etiology
Traumatic Atraumatic
LAXITY
Capsulolabral injuriesPlastic deformation capsule
MDI
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 57 Multidirectional Instability H & E
Young adults
Instability through mid-ROMIncapacitating for ADLs
Grade 2-3 GH translation in at least 2 directions, concurrent with symptoms in at least one direction
Hyperflexibility• Palms to floor, thumb to wrist
• Elbow hyperextension
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 58 Multidirectional Instability
Pathoanatomy
Redundant inferior capsule / ligaments
Resultant increase in capsular volume
Collagen (Ehlers-Danlos syndrome)
Abnormal bony morphology
Labral, capsule tears
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 59
Multidirectional Instability Treatment
Therapy, therapy, and more therapy
Dynamic shoulder stabilizers
• Rotator cuff, deltoid, scapular muscles
Surgical – fair to good results
Open – Gold standard
• Inferior Capsular Shift + Interval Closure
Arthroscopic Gaining
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 60 Multidirectional Instability
Treatment OutcomesNonoperative –
88% satisfactory Rockwood. JBJS, 1992
Operative – Inferior Capsular Shift
OPEN: 91% (ant), 100% (post) satisfactory 49 patients at 5 years
Bigliani, Ortho Trans, 1993
OPEN: 38/39 satisfactory results, b/w 1-2 years f/upNeer and Foster. JBJS, 1980
Arthroscopic: 97% (47/48) Good/Excellent results2-5 years
Gartsman. Arthroscopy, 2001
Arthroscopic: 22/25 (88%) satifactory at avg. 5 yearsTreacy. JSES, July 1999
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 61
Neurologic Instability
Brachial Plexus Injury
Cervical spine Injury
Stroke
Subclavian Cyst
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
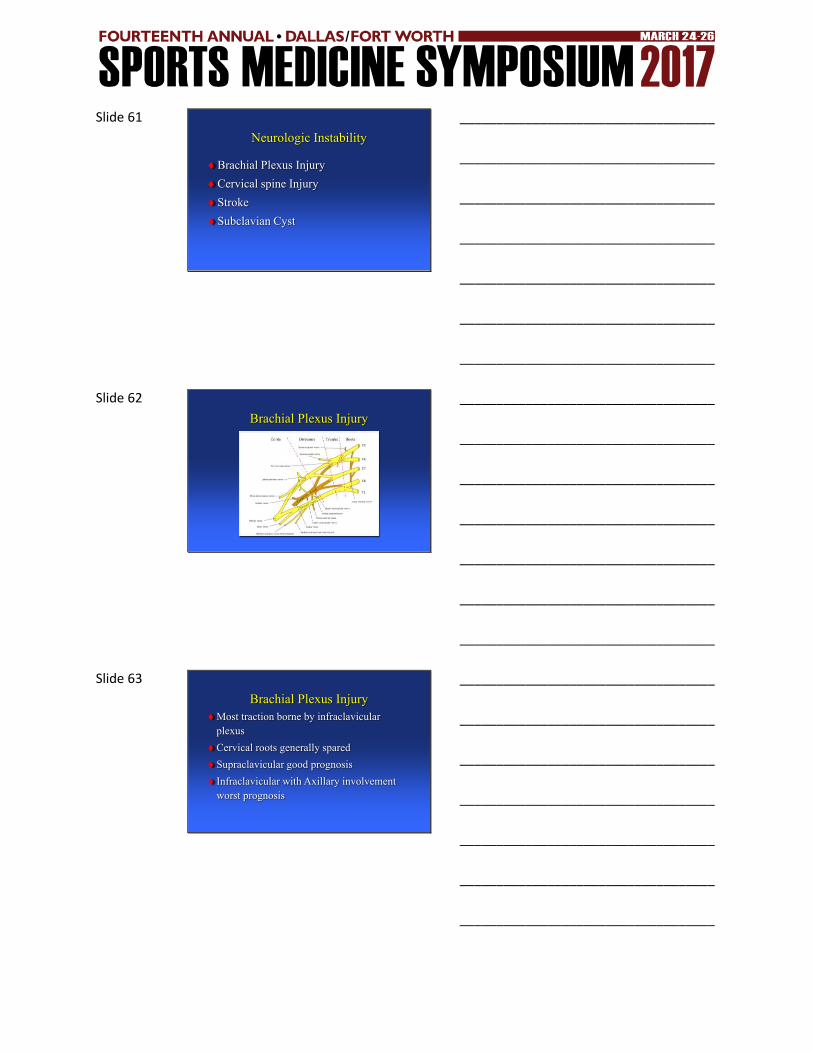
Slide 62
Brachial Plexus Injury
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 63
Brachial Plexus Injury
Most traction borne by infraclavicular
plexus
Cervical roots generally spared
Supraclavicular good prognosis
Infraclavicular with Axillary involvement
worst prognosis
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________

Slide 64
Axillary Nerve Injury
Most common
Neurovascular injury
13%
Deltoid weakness or
lateral numbness
Normal sensation doesn’t
exclude
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 65
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________





























