Embed Size (px)
Citation preview

Fig. 1
Fig. 2
VOL. 66-B, No. 4, AUGUST 1984 551
CLINICAL ASSESSMENT OF INSTABILITY OF THE SHOULDER
WITH SPECIAL REFERENCE TO ANTERIOR AND POSTERIOR DRAWER TESTS
CHRISTIAN GERBER, REINHOLD GANZ
From University of Berne
Anterior and posterior drawer tests of the shoulder are described. Their purpose is to detect anterior andposterior shoulder instability and thereby to eliminate some of the failures of operative treatment. Their valuein assessing unidhectional and mullidirectional instabifity both before and after operation is discussed.
The treatment of chronic instability of the shoulder hasreceived far more attention in the medical literature thanits clinical diagnosis. Most accounts tend to focus onoperative procedures without presenting clinical methods
ofdetecting glenohumeral instability accurately, let alonegrading it (Moseley 1969 ; Trillat and LeClerc-Chalvet
1973; Rockwood 1975; Bateman 1978; Post 1978; Saha
1981 ; Kessel 1982).The diagnosis of the direction of instability of the
shoulder is often based on radiographic findings, andmay be difficult if no dislocation is present when the
patient is seen (Patte et al. 1980; Rowe 1980). It istherefore not surprising that the surgeon is often facedwith posterior subluxations which have erroneously been
interpreted as anterior instabilities, or with so-called“loose shoulders” in which anterior or posterior recon-structions have failed because multidirectional instabilitywas not recognised before operation (Du Toit and Roux1956 ; Trillat, Dejour and Roullet 1965 ; Rowe, Pate! andSouthmayd 1978 ; Neer and Foster 1980).
For the unstable knee, clinical testing of the capsuleand ligaments is universally accepted ; it provides the
basic information for determining treatment as well as
for grading the results after operation. In this paper wedescribe a set of comparable, relatively simple, clinical
tests which we have used successfully to determine thedirection or directions of shoulder instability ; the testshave proved helpful in deciding the appropriate treat-ment and in evaluating the results.
ANTERIOR INSTABILITY
The diagnosis of anterior dislocation is obvious if thepatient has been seen with the joint dislocated, or if ithas been demonstrated radiographically. Anterior sub-
Professor R. Ganz, MD, DirectorCh. Gerber, MD, Resident in Orthopaedic SurgeryDepartment of Orthopaedic Surgery, University of Berne, Inselspital,3010 Berne, Switzerland.
Requests for reprints should be sent to Professor R. Ganz.
© 1984 British Editorial Society of Bone and Joint Surgery0301 -620X/84/4140 $2.00
luxations are often suspected from their characteristichistory which has been well described in many publica-
tions (Blazina and Satzman 1969 ; Rockwood 1975 ; Patteet al. 1980 ; Hastings and Coughlin 1981 ; Rowe andZarins 1981 ; DePalma 1983). However, about half thepatients with anterior subluxation never experience
The apprehension test.
/1
‘rb,
/
Fig. 3
..�. #{149} _._.4-----.---.
Fig. 4
Fig. 5 Fig. 6
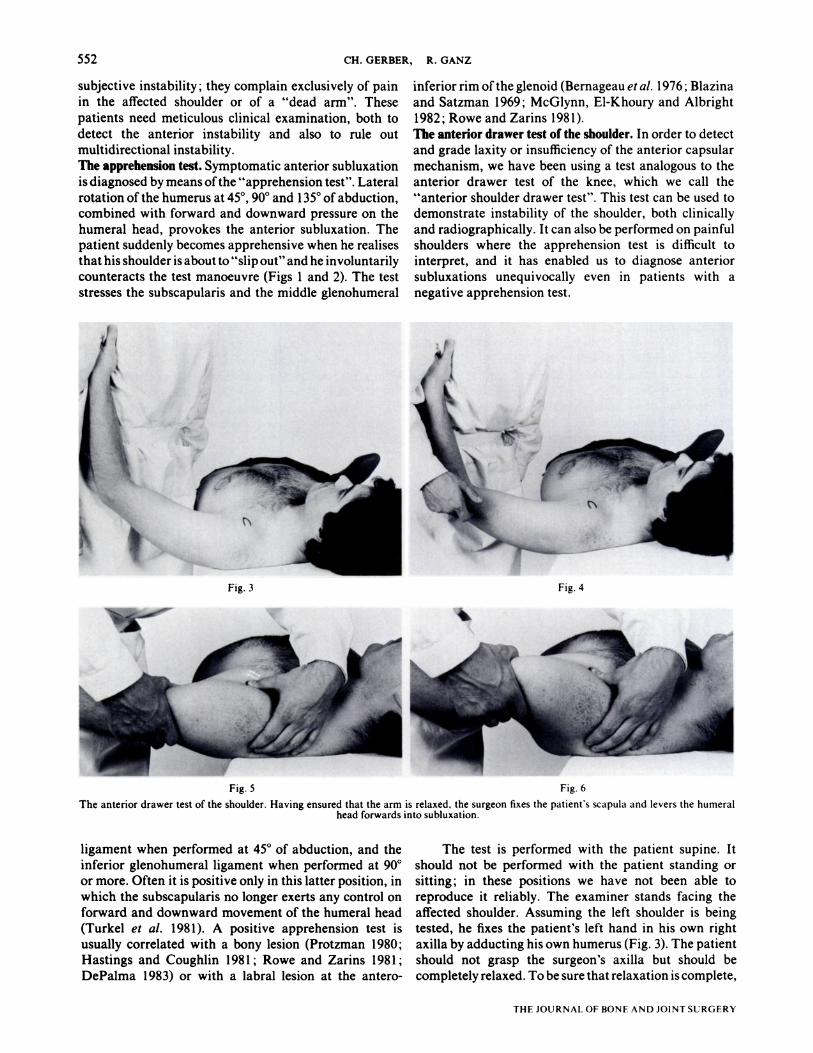
The anterior drawer test of the shoulder. Having ensured that the arm is relaxed, the surgeon fixes the patient’s scapula and levers the humeralhead forwards into subluxation.
552 CH.GERBER, R.GANZ
THE JOURNAL OF BONE AND JOINT SURGERY
subjective instability ; they complain exclusively of painin the affected shoulder or of a “dead arm”. These
patients need meticulous clinical examination, both todetect the anterior instability and also to rule out
multidirectional instability.The apprehension test. Symptomatic anterior subluxation
is diagnosed by means ofthe “apprehension test”. Lateral
rotation of the humerus at 45#{176},90#{176}and 135#{176}of abduction,combined with forward and downward pressure on thehumeral head, provokes the anterior subluxation. Thepatient suddenly becomes apprehensive when he realisesthat his shoulder is about to “slip out” and he involuntarilycounteracts the test manoeuvre (Figs 1 and 2). The teststresses the subscapularis and the middle glenohumeral
ligament when performed at 45#{176}of abduction, and theinferior glenohumeral ligament when performed at 90#{176}
or more. Often it is positive only in this latter position, inwhich the subscapularis no longer exerts any control on
forward and downward movement of the humeral head(Turkel et a!. 198 1). A positive apprehension test isusually correlated with a bony lesion (Protzman 1980;Hastings and Coughlin 1981 ; Rowe and Zarins 1981;
DePalma 1983) or with a labral lesion at the antero-
inferior rim ofthe glenoid (Bernageau et a!. 1976 ; Blazinaand Satzman 1969; McGlynn, El-Khoury and Albright
1982; Rowe and Zarins 1981).The anterior drawer test of the shoulder. In order to detectand grade laxity or insufficiency of the anterior capsular
mechanism, we have been using a test analogous to theanterior drawer test of the knee, which we call the
“anterior shoulder drawer test”. This test can be used todemonstrate instability of the shoulder, both clinically
and radiographically. It can also be performed on painfulshoulders where the apprehension test is difficult tointerpret, and it has enabled us to diagnose anterior
subluxations unequivocally even in patients with a
negative apprehension test.
ii
The test is performed with the patient supine. Itshould not be performed with the patient standing orsitting ; in these positions we have not been able toreproduce it reliably. The examiner stands facing theaffected shoulder. Assuming the left shoulder is beingtested, he fixes the patient’s left hand in his own rightaxilla by adducting his own humerus (Fig. 3). The patientshould not grasp the surgeon’s axilla but should be
completely relaxed. To be sure that relaxation is complete,

Fig. 9 Fig. 10
The anterior drawer test of the shoulder. Diagrams and radiographs illustrating the change in position of the head of the humerus in relation tothe scapula.
CLINICAL ASSESSMENT OF INSTABILITY OF THE SHOULDER 553
VOL. 66-B. No. 4. AUGUST 1984
the examining surgeon gently taps the patient’s elbow(Fig.4).
The affected shoulder is held in 80#{176}to 120#{176}ofabduction, 0#{176}to 20#{176}of forward flexion, and 0#{176}to 30#{176}oflateral rotation ; this position should be quite comfortable.
The examiner holds the patient’s scapula with his lefthand, pressing the scapular spine forward with his indexand middle fingers ; his thumb exerts counter-pressure onthe coracoid process. The scapula is now held firmly inthe examiner’s left hand (Figs 5 and 7). With his right
hand, he grasps the patient’s relaxed upper arm in itsresting position and draws it anteriorly (Figs 6 and 8)with a force comparable to that used at the knee in
Lachman’s test.The relative movement between the fixed scapula
and the movable humerus can easily be appreciated andcan be graded as with knee instability. Ifnecessary it can
be demonstrated by radiography (Figs 9 and 10), and bycineradiography using an ordinary axillary projection(Gerber, Ganz and R#{252}fenacht 1983). An occasionalaudible click on forward movement of the humeral
head-probably due to labral pathology-is usuallyassociated with apprehension. Its presence should benoted in addition to recording the degree of anterior
displacement of the humeral head.
POSTERIOR INSTABILITY
Posterior dislocations of the shoulder are often over-looked, both clinically and radiographically (McLaughlin1952; Rowe 1956; Rockwood 1975).
Recurrent posterior subluxations occur either spon-taneously or after significant trauma. They are oftencombined with anterior instability or with inferior
instability, or with both (Rockwood 1975 ; Tibone et a!.
1981 ; Neer and Foster 1980; DePalma 1983) and they
account for a large proportion of voluntary shouldersubluxations (Boyd and Sisk 1972 ; Rowe, Pierce andClark 1973; Rockwood 1975; DePalma 1983).
The history of unidirectional posterior instability isoften revealing : the patient either voluntarily subluxateshis shoulder in forward flexion and medial rotation, orhe complains of weakness and instability on combinedflexion and medial rotation (for example, when doingpress-ups). Some patients, however, cannot tell in whichposition the shoulder feels unstable or, if they havemultidirectional instability, they are apprehensive in
several different positions.We could find no reliable test for posterior instability
in the literature. The apprehension test mentioned by
Kessel (1982) was not consistent in detecting posteriorsubluxation in our patients. We feel it is this absence of

554 CH. GERBER, R. GANZ
THE JOURNALOF BONE AND JOINT SURGERY
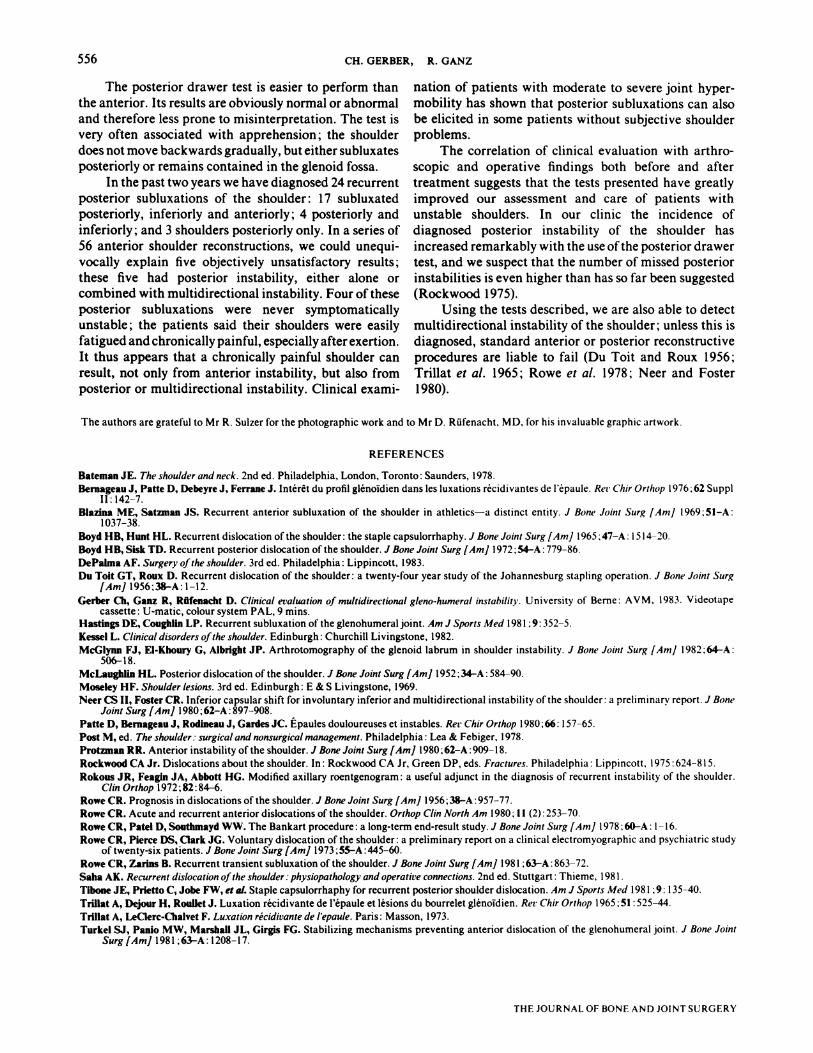
The posterior drawer test of the shoulder. The thumbslides along the lateral aspect of the coracoid process asthe head of the humerus is pushed backwards into
subluxation.
any reliable clinical test to identify posterior shouldersubluxation with certainty which may have contributed
to its low rate of detection.The posterior drawer test. The patient must be supine.The examiner stands level with the affected shoulder.
Assuming the left shoulder is being tested, he grasps thepatient’s proximal forearm with his left hand, flexes theelbow to about 120#{176},and positions the shoulder into 80#{176}to 120#{176}of abduction and 20#{176}to 30#{176}of forward flexion.The examiner holds the scapula with his right hand, with
his index and middle fingers on the scapular spine ; his
thumb lies immediately lateral to the coracoid process,so that its ulnar aspect remains in contact with thecoracoid while performing the test (Figs 1 1, 1 3 and 15).With his left hand, the examiner slightly rotates theupper arm medially and flexes it to about 60#{176}or 80#{176};
during this manoeuvre, the thumb ofthe examiner’s righthand subluxates the humeral head posteriorly (Figs 12,
14 and 16). This posterior displacement can be appre-ciated as the thumb slides along the lateral aspect of the

1;
Fig. 17 Fig. 18
Inferior instability which can be demonstrated by applying downward traction on the upperarm.
CLINICAL ASSESSMENT OF INSTABILITY OF THE SHOULDER 555
VOL. 66-B, No. 4, AUGUST 984
coracoid process towards the glenoid, and the humeralhead abuts against the ring finger of the examiner’s right
hand. This manoeuvre is painfree but often associatedwith a slight to moderate degree of apprehension,
enabling the patient to identify the position of instability
with certainty.
INFERIOR INSTABILITY
Inferior instability (Figs 17 and 18) is almost always acomponent of multidirectional instability. The clinical
diagnosis is made by gentle traction on the relaxed upperarm (Neer and Foster 1980). This test is done with thepatient upright and the shoulder in the neutral position.It is important that the shoulder muscles are relaxed and
that the stress is applied to the upper arm and not to theforearm ; this eliminates the effect of the biceps andtriceps brachii. Subluxating the humeral head inferiorly
is the simplest of the tests described. Although wellestablished, it warrants restating, since a positiveresult invariably points to complex (multidirectional)instability.
DISCUSSION
Many authorities agree that the exact clinical diagnosisof multidirectional instability (as distinct from unidirec-tional subluxation or dislocation) is critical, since the
different conditions require different therapies (Boyd andHunt 1965 ; Rowe et a!. 1973 ; Bateman 1978 ; Neer andFoster 1980 ; DePalma 1983). Many reference texts,
however, do not provide guidelines for such clinicalassessment. Although each surgeon undoubtedly has hisown test, only DePalma(l983)gives a reasonably detailedaccount of a method of assessing shoulder instability.Neer and Foster (1980) test for inferior instability, butconsider that testing and grading of anteroposterior
instability is misleading if not performed under anaes-thesia. After two years’ experience with the tests
described in this paper, we feel that this view needs to bereconsidered.
The anterior drawer test helps to grade anteriorinstability and gives information about the anteriorcapsular mechanism. The test was positive in all our
patients with recurrent dislocation. In post-traumaticcases it was occasionally necessary to abduct the humerusto more than 120#{176}and to exert considerably more forwardpressure to elicit an anterior drawer sign ; this was more
abduction than was needed in non-traumatic cases.Anterior subluxation was easily detected in the presenceof slight to moderate joint laxity, whereas the apprehen-sion test appeared more sensitive in tight shoulders with
truly post-traumatic antero-inferior subluxations.We have seen only two patients with post-traumatic
subluxation who had a negative anterior drawer signwhen tested up to about 135#{176}of abduction ; both thesepatients had a bony lesion at the antero-inferior glenoid
rim which was detected radiographically using a modified
axillary view (Rokous, Feagin and Abbott 1972). Rowe
and Zarins (1981) and DePalma (1983) stated thatanterior subluxation of the shoulder is always associatedwith a positive apprehension test. The anterior drawertest has enabled us to detect and demonstrate radiograph-ically anterior shoulder subluxation in five patients inwhom the apprehension test was negative. Four of these
had moderatejointlaxity and multidirectional instability;the other had slight to moderate joint laxity withoutdetectable posterior or inferior subluxation.
The anterior drawer test has to be performed exactly
as we have described it if reproducible results are to beobtained. When interpreting the results, it should beremembered that there is a significant range of laxity innormal individuals, just as there is in the knee.
556 CH. GERBER, R. GANZ
THE JOURNAL OF BONE AND JOINT SURGERY
The posterior drawer test is easier to perform thanthe anterior. Its results are obviously normal or abnormaland therefore less prone to misinterpretation. The test isvery often associated with apprehension ; the shoulder
does not move backwards gradually, but either subluxatesposteriorly or remains contained in the glenoid fossa.
In the past two years we have diagnosed 24 recurrentposterior subluxations of the shoulder : 17 subluxatedposteriorly, inferiorly and anteriorly ; 4 posteriorly andinferiorly ; and 3 shoulders posteriorly only. In a series of
56 anterior shoulder reconstructions, we could unequi-vocally explain five objectively unsatisfactory results;these five had posterior instability, either alone orcombined with multidirectional instability. Four of theseposterior subluxations were never symptomaticallyunstable ; the patients said their shoulders were easilyfatigued and chronically painful, especially after exertion.It thus appears that a chronically painful shoulder canresult, not only from anterior instability, but also from
posterior or multidirectional instability. Clinical exami-
nation of patients with moderate to severe joint hyper-mobility has shown that posterior subluxations can alsobe elicited in some patients without subjective shoulderproblems.
The correlation of clinical evaluation with arthro-scopic and operative findings both before and after
treatment suggests that the tests presented have greatlyimproved our assessment and care of patients withunstable shoulders. In our clinic the incidence of
diagnosed posterior instability of the shoulder hasincreased remarkably with the use ofthe posterior drawertest, and we suspect that the number of missed posteriorinstabilities is even higher than has so far been suggested(Rockwood 1975).
Using the tests described, we are also able to detectmultidirectional instability of the shoulder ; unless this isdiagnosed, standard anterior or posterior reconstructive
procedures are liable to fail (Du Toit and Roux 1956;Trillat et a!. 1965 ; Rowe et a!. 1978 ; Neer and Foster
1980).
The authors are grateful to Mr R. Suizer for the photographic work and to Mr D. ROfenacht, MD, for his invaluable graphic artwork.
REFERENCES
Bateman JE. The shoulder and neck. 2nd ed. Philadelphia, London, Toronto : Saunders, 1978.Bernageau J, Patte D, Debeyre J, Ferrane J. Int#{233}r�tdu profil gl#{233}noldiendans les luxations r#{233}cidivantes de l’#{233}paule.Ret Chir Orthop 1976 ; 62 Suppl
II : 142-7.Blazina ME, Satzman JS. Recurrent anterior subluxation of the shoulder in athletics-a distinct entity. J Bone Joint Surg [Am] 1969 ; 51-A:
1037-38.Boyd HB, Hunt HL. Recurrent dislocation ofthe shoulder: the staple capsulorrhaphy. J Bone Joint Surg [Am] 1965 : 47-A : 15 14-20.
Boyd HB, Sisk TD. Recurrent posterior dislocation of the shoulder. J Bone Joint Surg [Am] 1972 54-A : 779-86.DePalma AF. Surgery ofthe shoulder. 3rd ed. Philadelphia : Lippincott, 1983.Du Toit GT, Roux D. Recurrent dislocation of the shoulder: a twenty-four year study of the Johannesburg stapling operation. J Bone Joint Surg
[Am] 1956;38-A: 1-12.
Gerber Cli, Ganz R, Rllfenacht D. Clinical evaluation ofmultidirectional gleno-humeral instability. University of Berne : AVM, 1983. Videotapecassette : U-matic, colour system PAL, 9 mins.
Hastings DE, Coughlin LP. Recurrent subluxation of the glenohumeraljoint. Am J Sports Med 1981 : 9: 352-5.
Kessel L. Clinical disorders ofthe shoulder. Edinburgh : Churchill Livingstone, 1982.
McGlynn FJ, El-Khoury G, Aibright JP. Arthrotomography of the glenoid labrum in shoulder instability. J Bone Joint Surg [Am] 1982 ; 64-A:506-18.
McLaughlin HL. Posterior dislocation of the shoulder. J Bone Joint Surg [Am] 1952 ;34-A : 584-90.
Moseley HF. Shoulder lesions. 3rd ed. Edinburgh : E & S Livingstone, 1969.
Neer CS II, Foster CR. Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder : a preliminary report. J BoneJoint Surg[Am] l980;62-A:897-908.
Patte D, Bernagesu J, Rodineau J, Gardes JC. Epaules douloureuses et instables. Rer Chir Orthop l980;66: 157-65.
Post M, ed. The shoulder: surgicaland nonsurgicalmanagement. Philadelphia : Lea & Febiger, 1978.
Protzman RR. Anterior instability of the shoulder. J Bone Joint Surg [Am] l980;62-A : 909-18.
Rockwood CA Jr. Dislocations about the shoulder. In : Rockwood CA Jr, Green DP, eds. Fractures. Philadelphia : Lippincott, 1975 :624-8 15.Rokous JR, Feagin JA, Abbott HG. Modified axillary roentgenogram : a useful adjunct in the diagnosis of recurrent instability of the shoulder.
C/in Orthop 1972;82:84-6.
Rowe CR. Prognosis in dislocations of the shoulder. J Bone Joint Surg [Am] l956;38-A : 957-77.
Rowe CR. Acute and recurrent anterior dislocations of the shoulder. Orthop Clin North Am 1980 : 1 1 (2) : 253-70.
Rowe CR, Patel D, Southmayd WW. The Bankart procedure : a long-term end-result study. J Bone Joint Surg [Am] 1978 :60-A : 1-16.Rowe CR, Pierce DS, Clark JG. Voluntary dislocation of the shoulder : a preliminary report on a clinical electromyographic and psychiatric study
of twenty-six patients. J Bone Joint Surg [Am] 1973 ;55-A : 445-60.Rowe CR, Zarins B. Recurrent transient subluxation ofthe shoulder. J Bone Joint Surg [Am] 1981 ;63-A : 863-72.
Saha AK. Recurrent dislocation ofthe shoulder : physiopathology and operative connections. 2nd ed. Stuttgart : Thieme, 1981.Tibone JE, Prietto C, Jobe FW, et al. Staple capsulorrhaphy for recurrent posterior shoulder dislocation. Am J Sports Med 1981 :9 : 135-40.Trillat A, Dejour H, Roullet J. Luxation r#{233}cidivantede l’#{233}pauleet lesions du bourrelet gl#{233}noIdien.Rev Chir Orthop 1965 :51 :525-44.
Trillat A, LeClerc-Cbalvet F. Luxation r#{233}cidivantede lepaule. Paris : Masson, 1973.Turkel SI, Paulo MW, Marshall JL, Girgis FG. Stabilizing mechanisms preventing anterior dislocation of the glenohumeral joint. J Bone Joint
Surg[AmJ 1981 ;63-A:1208-l7.