Shoulder Instability
Shoulder InstabilityDR Harpreet Singh
BhatiaDMCH,Ludhiana,Punjab
DEFINITION:
Instability:Inability to maintain the humeral head in the
glenoid fossa.Includes a spectrum of disorders
Dislocation Complete loss of glenohumeral
articulationSubluxation Partial loss of glenohumeral articulation
with symptomsLaxity Incomplete loss of glenohumeral articulation
unassociated with pain
STABILITY Static FactorsArticular CongruenceArticular
VersionGlenoid LabrumCapsule and Ligament
Dynamic FactorsRotator CuffBiceps TendonScapulothoracic
MotionNegative PressurePropioception
3
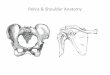
OSTEOLOGYGlenoid fossaPear shaped7 deg. of retroversion5 deg. of
sup tiltGlenoid version30o anteriorHumerusNeck-shaft 130o to
140oRetrotorsion 30o
Normal glenoid is about 7 degrees retroverted
If the retroversion is excessive, it leads to posterior
instability of shoulderSTATIC FACTORS
GLENOHUMERAL JOINTHumeral head 3x larger than glenoid fossaBall
and socket with translation3 degrees of
freedomFlex/ExtAbd/AddInt/Ext rotPlus Cricumduction
GLENOID LABRUMStatic stabilizercontributes 20% to GH
stabilityFibro cartilaginous tissueDeepens
glenoid(50%)3purposes:Inc. surface contact areaButtressAttachment
site for GH ligaments
The labrum increases the superoinferior diameter of the glenoid
by 75% and the anteroposterior (AP) diameter by 50%
CAPSULE AND LIGAMENTS CapsuleAttached medially glenoid
fossalaterally to anatomical neck of humerusAnt cap thicker than
post.2-3 mm of distractionLittle contribution to joint
stabilityStrengthened by GHLs and RC tendons
LIGAMENTS
GLENOHUMERAL LIGAMENTS (Superior, Middle , Inferior)SGHLO =
tubercle on glenoid just post to long head bicepsI = upper end of
lesser tubercleResists inf. subluxation and contributes to
stability in post and inf. directions
MGHLO= sup glenoid and labrumI = blends with subscapularis
tendonLimits ant. instability especially in 45 deg abduction
position Limits ext rotation
IGHLO= ant. glenoid rim and labrumI= inf. aspect of humeral
articular surface and anatomic neck3 bands, anterior, axillary and
posteriorActs like a sling ,the most important single ligamentous
stabilizer .Primary restraint is at 45-90 deg abduction.
Coracoacromial ligamentsecondary stabilizer.Coracohumeral
ligamentContribute to restraining inferior subluxation with arm at
side,
Dynamic FactorsRotator CuffBiceps TendonNegative
PressureScapulothoracic motionProprioception
ROTATOR CUFFCompression enhances conformityGreater than static
stabilizersCoordinated contractions/steering effectSupraspinatus
most important Dynamization
Biceps long head, Deltoid secondary stabilizer head depressor
Periscapular Muscles help position scapula and orient glenohumeral
joint contributes compressive force across joint
SCAPULOTHORACIC MOTION2:1 glenohumeral to scapulothoracic
motionScapulothoracic muscle (trapezius, serratus anterior, teres
major, levator scapulae)less stable platform
NEGATIVE INTRA-ARTICULAR PRESSURE-42 cm H2O in cadaverSecondary
to high osmotic pressure in interstitial tissuesOnly clinically
important in the arm at rest in adductionLost with lax capsule or
defect
INSTABILITYClassification:FrequencyCause DirectionDegree
Classification of instability
SPECTRUM Traumatic Microtrauma Atraumatic
Less laxity More laxity
Unidirectional Multidirectional
PATHOANATOMY OF SHOULDERINSTABILITYLaberal Lesions Bankart
Reverse Bankart SLAP lesionsCapsular Injury Intrasubstance Tear
HAGL Capsular Laxity Bone Loss Glenoid Humeral Head-Hill-Sachs
Lesion
BANKART LESION. The traumatic detachment of the glenoid labrum
has been called the Bankart lesion. 85%
BANKART LESION-labral tear at anterior half of glenoid rim
Reverse Bankart lesion
Anchor used for repair
HILL-SACHS LESION This is a defect in the posterolateral aspect
of the humeral head.
Hill Sach Lesion
EVALUATION OF INSTABILITYHistoryAgeTrauma-DurationAssociated
Pain Sports, throwing or overhead activitiesVoluntary
subluxationClunk or knockFear-Limitation of MovementsHx
dislocationsand energy associatedHx 1st dislocation or
injurySubsequent dislocations/ subluxations
Physical Examination Inspection Palpation ROM Winging
Neurovascular testing Generalized ligamentous laxity Instability
tests
Sulcus signDrawer testsLoad & Shift test
Apprehension testJobes Relocation Jerk testFulcrum Grade = 1 -
4
DIAGNOSISX-raysCT ScanMRIArthroscopy
RADIOLOGYX-RaysIdentify Bankart or Hill-Sachs Lesion
AP VIEW
Normal Shoulder AP view
Axillary View
Scapular Y-View
Stryker viewHumeral Head Defect
Apical Oblique view
Glenoid rim lesion
West Point Axillary view Anteroinferior glenoid rim
ANTERIOR DISLOCATION 97% of recurrent dislocation abduction,
extension and external rotationsubcoracoid subglenoidsubclavicular
Associated Injuries: Fractures Head & Neck Rotator Cuff Tears
> 40 y/o = 30 % > 60 y/o = 80%
Neurologic InjuryAxillary nerve10-25% incidence 1st time.2-5% in
recurrent dislocatorsTx: watchful expectancyPoor prognosis if no
recovery by 10 wksVascular Injury Axillary artery 2nd part
thoracoacromial trunk
POSTERIOR DISLOCATION
Incidence: < 5% all shoulder dislocations Axial load
Flexed/Adduction Bench press-lock out Swimming- pull thru Rowing
Football Offensive Lineman
Examination Shift & load test Post. Apprehension test Jerk
test Kim test Imaging studies X-ray CT MRI
53
TREATMENT Non Operative Immobilization Protection Rehabilitation
70-90% improve Functional disability improved Instability not
eliminated
Operative Management
Overall 50-95 % successHigher recurrence vs ant. instability
procedures
Soft Tissue Procedures Posterior Capsulorrhaphy Reverse
Putti-Platt (IS Capsular Tenodesis) McLaughlin Bone Procedures
Posterior Glenoid OsteotomyPosterior Bone Block
MATSEN'S CLASSIFICATION TUBS: Traumatic Unidirectional Bankart
lesion Surgery is often necessary.AMBRI: Atraumatic
Multidirectional Bilateral Rehabilitation is the primary mode of
treatment.Inferior capsular shift & internal closure often
performed.
OPERATIVE TREATMENT:Capsulolabral RepairBankartModified Bankart
Subscapularis Procedures Putti-Platt Magnuson-Stack Coracoid
Transfer Procedures Bristow Latarjet
TREATMENT OPTIONSTYPE OF INSTABILITYPREFERRED SURGERYTraumatic
anterior, with Bankart LesionOpen / arthroscopic Bankart
repairTraumatic anterior , with no labral lesion, just capsular
laxityOpen / arthroscopic capsular imbricationAMBRI lesionsLateral
capsular shift( modified Neer and Foster ) with closure of rotator
intervalRecurrent posterior dislocation in association with a
reverse Hill-Sachs lesionmodified McLaughlin procedure Head defect
> 30 45 % > 45 % Acute disimpaction / Weber
osteotomyProsthetic replacementGlenoid defectBristow Latarjet
coracoid transferStructural bone graft
Procedures
ProcedureDescriptionResultsNeers CapsulorrraphyPosterior
capsular tighteningGenerally unsatisfactory, upto 50 %
recurrenceStaple capsulorraphyTightening done with staplesSmall
study groupTieborne and bradley procedureCapsular Imbrication with
a horizontal T approachUpto 20 % recurrenceHawkins and Janda
procedureSubscapularis advancement and shortening0 5 %
recurrenceRockwood Glenloid Plasty with Biceps Tenodesis to the
posterior capsuleCombined bony and soft tissue procedureNot often
done
OPEN BONY PROCEDURES FOR ANTERIOR INSTABILITY
Bristow procedure
Latarjet procedure
Helfet first described the Bristow procedure in 1958 and named
it after his late mentor .
In the Bristow procedure and its variants, the coracoid process
is transferredthrough the subscapularis tendon as a method of
treating recurrent anterior instability of the shoulder.
1) The coracoid tip is transferred to the anteroinferior glenoid
neck and likely serves as a bone block in front of the humeral
head. The transferred short head of the biceps and coracobrachialis
are placed so as to produce a strong dynamic buttress across the
anterior and inferior aspects of the joint when the shoulder is in
the vulnerable abducted and externally rotated position. The
transfer was held in place bysuturesthrough the conjoined tendon
and subscapularis.
2) Latarjet described a similar procedure in 1954, in which he
transferred the tip of the coracoid along with the conjoined tendon
through a horizontal slit in the subscapularis and fixed it with a
screw
The procedure involves transfer of the coracoid with it's
attached muscles to the deficient area over the front of the
glenoid.
This replaces the missing bone and the transferred muscle also
acts as an additional muscular strut preventing further
dislocations.
The procedure has a high success rate (recurrence rate of less
than 1%4) and this is due to the triple effect described by
Patte.
These are: Increase or restore the glenoid contact surface
area;
The conjoint tendon stabilises the joint when the arm is
abducted and externally rotated, by reinforcing the inferior
subscapularis and anteroinferior capsule
Repair of the capsule. This triple effect is why the Latarjet is
such a successful procedure.
Latarjet procedure
AMBRI Lesions-Idea of managementPrimary treatment
nonoperative
Operative management recommended for patients who have continued
pain or disability despite an adequate rehabilitation
The gold standard is open stabilization
Capsular shift( modified Neer and Foster )
OPEN ANTERIOR PROCEDURES FOR POSTERIOR INSTABILITY
McLaughlin procedure
Neers modification of McLaughlin procedure
McLaughlin technique
subscapularis
Neers modification
Putty Platt Operation
Surgical procedure for stabilizing the glenohumeral joint after
recurrent anterior shoulder dislocations. The subscapularis tendon
is detached near its insertion on the humerus, the joint opened,
and the stump of the tendon on the lesser tuberosity is sutured to
the glenoid labrum.
Sometimes the procedure is combined with reattachment of the
glenoid labrum.
Technically an easy procedure
Disadvantages:
The Putti-Platt procedure is not to be performed on throwers
because it can reduce the range of movement in the shoulder.
30 35 % incidence of late OA
Magnuson Stack procedure
ADVANTAGES AND DISADVANTAGES OF ARTHROSCOPIC
STABILIZATIONADVANTAGES DISADVANTAGES-Improved cosmesis
-Technically demanding -Shorter operative time -Difficult in
revision case-Short hospital stay -Difficult in altered
anatomy-Decreased morbidity -Cannot address bony defect-Decreased
complication-Lower cost
PHASES OF REHABILITATIONPhase I Rest and immobilization. Pain
control with nonsteroidal anti-inflammatory drugs and ice applied
to the shoulder Phase II Isometric strengthening Isotonic
strengthening. Begin exercises with shoulder in adducted, forward-
flexed position, progressing to abducted position Phase III
Endurance building along with strengthening exercises. Goal: the
patient reaches 90% strength in the injured shoulder compared with
the uninjured shoulder Phase IV Increase activity to sport- or
job-specific activities
THANKS