Embed Size (px)
Citation preview
Short Course Report
Nutrition and Food Security - approaches to
improving the health of women and children
Nutrition for infants and young children
module pilot
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
2
Participants
Albertina Maria Domingas Belo Ermera District Hospital, Timor Leste
Amelia Huddlestone Sunrise Health Service, Ngukkurr Community
Crispin da Costa Araujo World Health Organisation, Timor Leste
Dirce Maria Soares Ministry of Health, Timor Leste
Emily Mooka Northern Territory Department of Health, Darwin
Filomeno Joao da Silva Baucau Referral Hospital,Timor Leste
Gloria Dalywater The Fred Hollows Foundation, Katherine
Joao Bosco da Costa Ministry of Health, Timor Leste
Maria Bower Sunrise Health Service, Katherine
Patricia O'Donoghue Anyinginyi Congress, Tennant Creek
Priscilla Martin Anyinginyi Congress, Tennant Creek Facilitators and presenters
Translators Expedito Belo Norman Piressva Monitoring and evaluation
Jenne Roberts Menzies School of Health Research Technical advisory group Jennifer Busch-Hallen Independent nutrition consultant Danielle Aquino The Fred Hollows Foundation Tracy Leon Boab Health Services, Western Australia Dympna Leonard Queensland Department of Health Heather Grieve Menzies School of Health Research
Developed by Menzies School of Health Research (Menzies), representing Compass: Women's and Children's Knowledge Hub for Health and funded by the Australian Agency for International Development (AusAID; the Australian Government’s international aid agency) and The Fred Hollows Foundation (TFHF).
Heather Grieve Menzies School of Health Research
Danielle Aquino The Fred Hollows Foundation
Cecily Dignan Independent nutrition consultant
Kate Mellor Menzies School of Health Research
Anna Roesler Menzies School of Health Research
Jodi Phillips Menzies School of Health Research
Gill Farlow The Fred Hollows Foundation (nutrition student)
Judith Myers Menzies School of Health Research
Tina McKinnon Northern Territory Department Health
Anne Neubauer Northern Territory Department of Health
Joshua Heath Northern Territory Department of Health
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
3
Executive Summary
The pilot of the Nutrition for infants and young children module of the Nutrition and Food Security - Approaches to
improving the health of women and children short course was delivered over five days in October 2011 to six
Indigenous health workers from the Northern Territory and five nutritionists from Timor Leste.
The module was delivered in a participatory, activity-based manner, with learnings reinforced through activities and
games. Data and case studies from Timor Leste and the Northern Territory were used throughout the module, and
participants were encouraged to consider and discuss how the learnings could be applied in their contexts and
roles.
Participants were introduced to the definitions, causes and consequences of the different types of malnutrition,
and the importance of addressing these conditions. The role of macro and micro nutrients was presented, as were
the causes and consequences of common micronutrient deficiencies. Key messages for appropriate nutrition
practices, including breastfeeding, complementary feeding, the management of malnutrition and food safety and
hygiene were discussed; and the evidence to support these messages and examples of appropriate approaches to
improving nutrition for infants and young children were presented and analysed.
Field trips provided opportunities for participants to observe the learnings of the course in practice. With ongoing
support from the facilitators, the individual action plans developed during the course will assist the participants to
apply the learnings of the course in their work roles.
Participants reported that the activity-based, participatory approach optimised their understanding of the
learnings, and that the case studies were ‘’well mixed, interesting, not too much from any one context, just a good
mix’’. As with the Nutrition planning and programming module, participants reported that bringing the two
country groups together had been beneficial, stating that they “found it interesting to learn from each other and
learn examples from different places”.
The positive feedback was reflected by a substantial increase in the number of correct responses submitted to a
quiz undertaken at baseline and again at endline, and an increase in the number of correct responses for six of the
seven learning areas in the quiz.

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
4
Introduction
This report documents the process and results of the pilot of the Nutrition for infants and young children module of
the Nutrition and Food Security - Approaches to improving the health of women and children short course, which
was delivered over five days from the 10th to the 14th of October 2011 at Menzies School of Health Research,
Darwin, Australia.
This module followed the Nutrition planning and programming module, which was delivered in May/June 2011;
and is the first of three elective modules to be piloted. The two remaining elective modules, Nutrition for
adolescent girls and women throughout the lifecycle and Food security and livelihoods, will be piloted in 2012.
Nutrition for infants and young children builds on the learnings of the Nutrition planning and programming module,
and is designed to provide participants with an understanding of the importance of appropriate nutrition for infants
and young children. Content includes the key messages regarding appropriate nutrition practices, the evidence to
support these messages and examples of evidence based, comprehensive and multi-stakeholder approaches to
improving the nutrition of infants and young children. Participants were encouraged to consider how the theory
presented related to their context, and how the learnings could be applied in their own work roles.
As with the Nutrition planning and programming module, this module was delivered in a participatory, activity-
based manner. Where possible, data and case studies from Timor Leste and the Northern Territory were used to
support the theory, and presentations were given by nutrition experts from these areas. Learnings were reinforced
through role-plays and games†.
Participants included six Indigenous health workers and community workers from the Northern Territory and five
nutritionists from Timor Leste‡.
† Refer to Appendix 1 for the course timetable ‡ Course materials, including presentations and factsheets were translated into Tetun for the participants from Timor Leste
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
5
178 9
0
4
8
12
Definition of the 1,000 Days
Definition of "Infants and young
children"
Number of participants who correctly answered "general"
questions (n=11)
Baseline Endline
Gloria from The Fred Hollows Foundation with her doll, Freddie
Day 1: Introduction and macro and micro nutrients
Learning objectives
The role of macro and micro nutrients in promoting normal growth and development in infants and young
children
The role and food sources of micronutrients most at risk of deficiency (such as iron, iodine and vitamin A),
international cut offs that define a public health problem, and the causes and consequences of common
micronutrient deficiencies
Essential skills and knowledge
List the macronutrients required for normal growth and development. Outline their function and common
food sources
List the common micronutrients required for normal growth and development. Outline their function and
common food sources
Identify the role and one food source of the micronutrient most at risk of deficiency in their local context
(such as iron, iodine or vitamin A)
Recognise the causes and consequences of the most common micronutrient deficiencies (such as iron, iodine
or vitamin A) in their local context
Theory presentations, activities and evaluation results
Following a welcome and an acknowledgment of the Larrakia
(Gulumbringin) people as the traditional custodians of the land;
participants were invited to reflect on the Nutrition planning and
programming module, and asked how they had integrated components
of the theory into their work roles. This session was noted to be
particularly valuable to the three participants who did not attend the
Nutrition planning and programming
module, and revealed that the concept of
the “upstream causes and downstream consequences of malnutrition” and the
planning cycle had been particularly valuable in participants’ work roles.
Participants made individual life size baby dolls. This activity served as an ice-breaker,
and the dolls were used to demonstrate theory throughout the course.
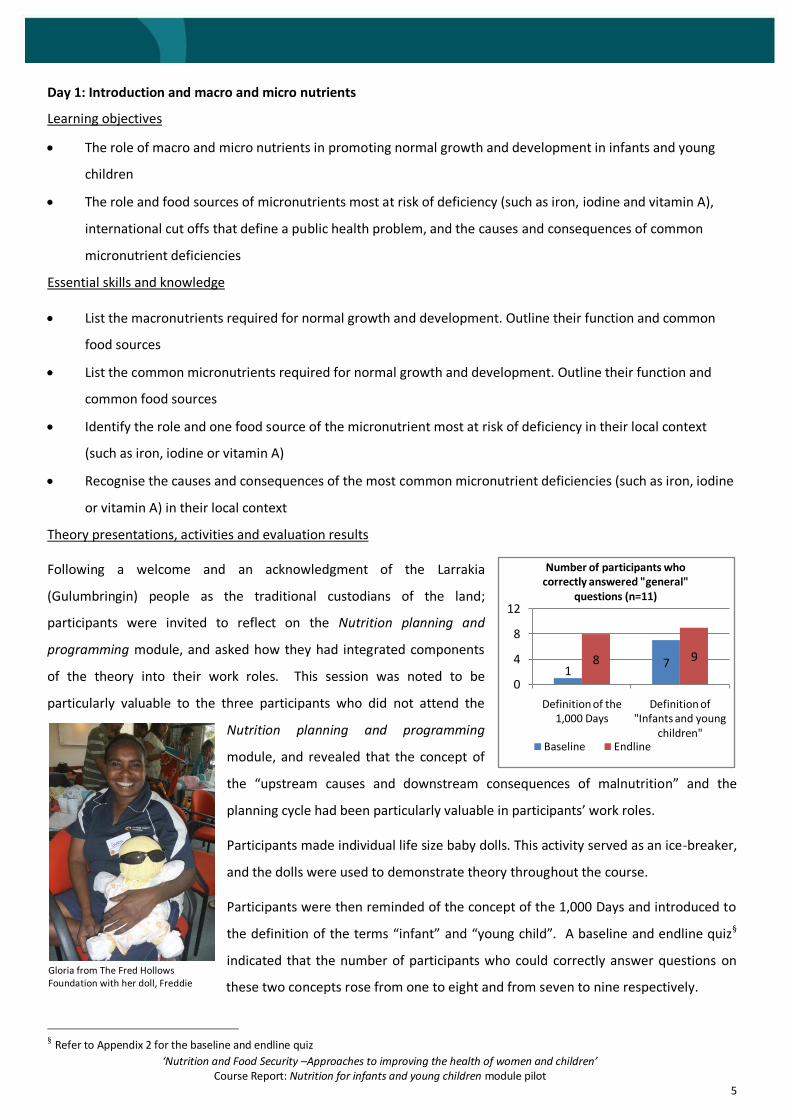
Participants were then reminded of the concept of the 1,000 Days and introduced to
the definition of the terms “infant” and “young child”. A baseline and endline quiz§
indicated that the number of participants who could correctly answer questions on
these two concepts rose from one to eight and from seven to nine respectively.
§ Refer to Appendix 2 for the baseline and endline quiz
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
6
The group brainstormed the role of macro and micro nutrients before the theory on this subject was presented. An
activity allowed participants to discuss local food sources of macro and micro nutrients in their context, and to
write or draw the “average” diet of a child aged 12 months in their context. Based on local food guides,
participants made recommendations to improve this diet. Participants from Timor Leste added fish, koto beans and
eggs to the diet of rice in order to increase the protein content, and noted that children in Timor Leste often
consume too much “unhealthy sugar”. The Indigenous Australian group added fruit and yoghurt to wheat biscuit
cereal, substituted the standard pie for spaghetti with meat and vegetables for dinner, and identified the need to
remove tea, soft drinks and undiluted cordial from the diet of a 12 month old child.
The role and food sources of micronutrients at risk of deficiency, including
iron, iodine and vitamin A, as well as the causes and consequences of
these deficiencies and the international cut offs that define a public
health problem, were presented. Mixed-country groups completed a
table of details related to each nutrient prior to the theory presentation,
and amended these tables following the presentation.
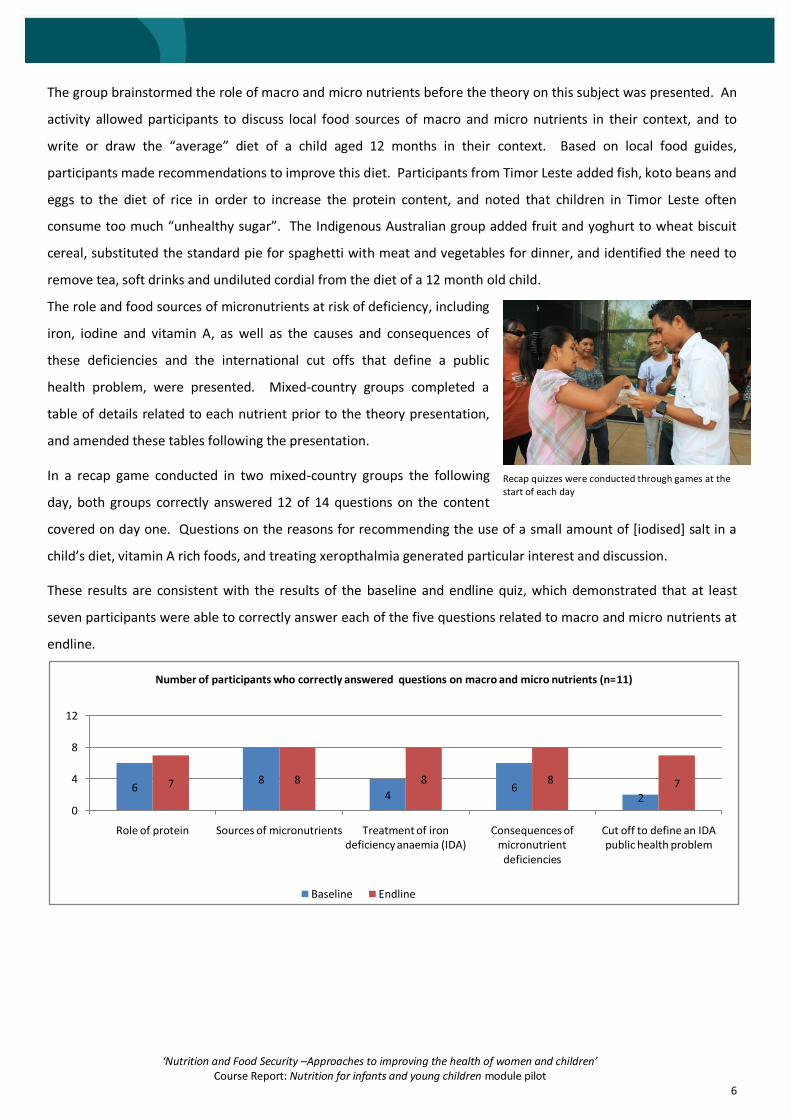
In a recap game conducted in two mixed-country groups the following
day, both groups correctly answered 12 of 14 questions on the content
covered on day one. Questions on the reasons for recommending the use of a small amount of [iodised] salt in a
child’s diet, vitamin A rich foods, and treating xeropthalmia generated particular interest and discussion.
These results are consistent with the results of the baseline and endline quiz, which demonstrated that at least
seven participants were able to correctly answer each of the five questions related to macro and micro nutrients at
endline.
68
46
27 8 8 8 7
0
4
8
12
Role of protein Sources of micronutrients Treatment of iron deficiency anaemia (IDA)
Consequences of micronutrient deficiencies
Cut off to define an IDA public health problem
Number of participants who correctly answered questions on macro and micro nutrients (n=11)
Baseline Endline
Recap quizzes were conducted through games at the start of each day
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
7
Day 2: Defining malnutrition; breastfeeding, complementary feeding and the management of acute and severe
malnutrition
Learning objectives
Definitions of malnutrition, including overnutrition and undernutrition
The causes and consequences of undernutrition, including the intergenerational cycle of stunting, mortality,
morbidity and the risk of adult chronic disease
Appropriate breastfeeding practices, and the evidence to support these practices
The causes and consequences of inappropriate breastfeeding practices
Evidence based approaches and strategies to protect, promote and support appropriate breastfeeding
practices
Appropriate complementary feeding practices, and the evidence to support these practices
The causes and consequences of inappropriate complementary practices
Evidence based approaches and strategies to promote and support appropriate complementary feeding
practices
The key components of an integrated approach to the management of acute malnutrition
Essential skills and knowledge
Define and describe malnutrition
Define and describ the types of undernutrition (acute and chronic)
Describe the causes and consequences of undernutrition (acute and chronic), mortality, morbidity, the risk of
adult chronic disease and the intergenerational cycle of stunting; and identify these in their local context
Describe methods of identifying acute and chronic undernutrition
Describe appropriate breastfeeding practices and the evidence to support these practices
Identify inappropriate breastfeeding practices and the causes of these practices in their local context
Identify one evidence based approach to protect, promote and support appropriate breastfeeding practices
Describe appropriate complementary feeding practices and the evidence to support these practices
Identify inappropriate complementary feeding practices and the causes of these practices in their local
context
Identify one evidence based approach to promote and support appropriate complementary feeding
practices
Identify the key components of an integrated approach to the management of acute malnutrition
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
8
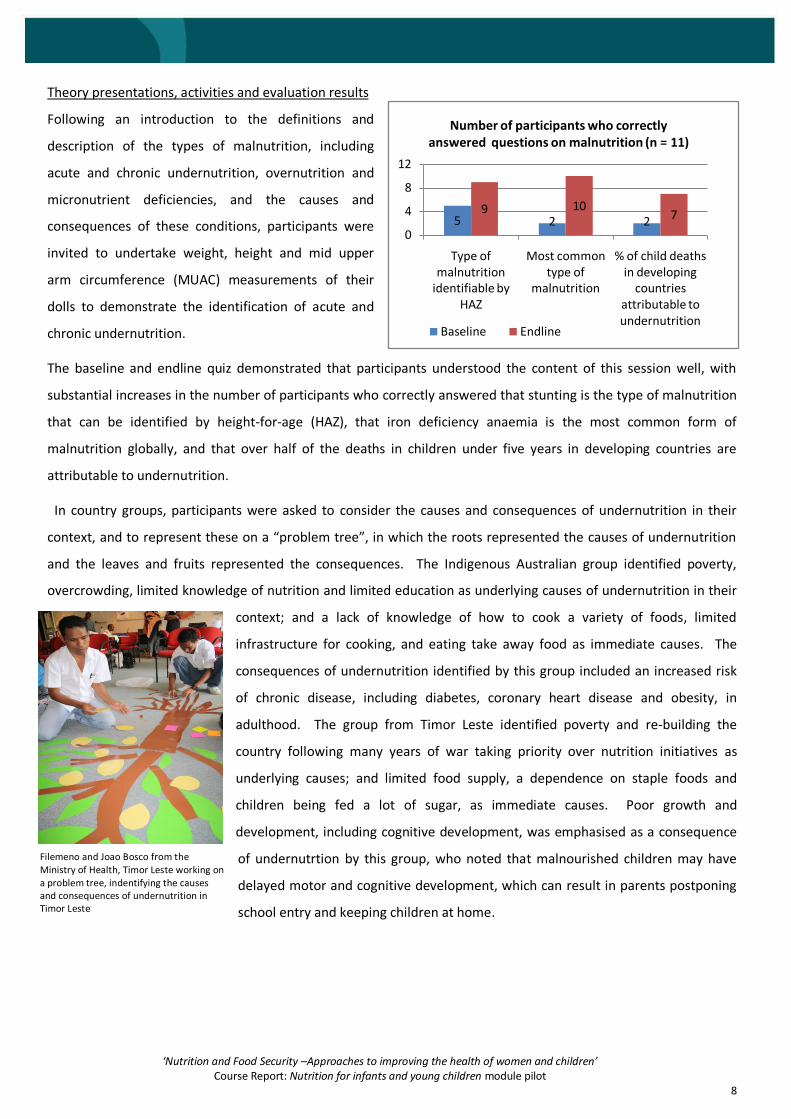
5 2 29 10
7
0
4
8
12
Type of malnutrition
identifiable by HAZ
Most common type of
malnutrition
% of child deaths in developing
countries attributable to undernutrition
Number of participants who correctly answered questions on malnutrition (n = 11)
Baseline Endline
Theory presentations, activities and evaluation results
Following an introduction to the definitions and
description of the types of malnutrition, including
acute and chronic undernutrition, overnutrition and
micronutrient deficiencies, and the causes and
consequences of these conditions, participants were
invited to undertake weight, height and mid upper
arm circumference (MUAC) measurements of their
dolls to demonstrate the identification of acute and
chronic undernutrition.
The baseline and endline quiz demonstrated that participants understood the content of this session well, with
substantial increases in the number of participants who correctly answered that stunting is the type of malnutrition
that can be identified by height-for-age (HAZ), that iron deficiency anaemia is the most common form of
malnutrition globally, and that over half of the deaths in children under five years in developing countries are
attributable to undernutrition.
In country groups, participants were asked to consider the causes and consequences of undernutrition in their
context, and to represent these on a “problem tree”, in which the roots represented the causes of undernutrition
and the leaves and fruits represented the consequences. The Indigenous Australian group identified poverty,
overcrowding, limited knowledge of nutrition and limited education as underlying causes of undernutrition in their
context; and a lack of knowledge of how to cook a variety of foods, limited
infrastructure for cooking, and eating take away food as immediate causes. The
consequences of undernutrition identified by this group included an increased risk
of chronic disease, including diabetes, coronary heart disease and obesity, in
adulthood. The group from Timor Leste identified poverty and re-building the
country following many years of war taking priority over nutrition initiatives as
underlying causes; and limited food supply, a dependence on staple foods and
children being fed a lot of sugar, as immediate causes. Poor growth and
development, including cognitive development, was emphasised as a consequence
of undernutrtion by this group, who noted that malnourished children may have
delayed motor and cognitive development, which can result in parents postponing
school entry and keeping children at home.
Filemeno and Joao Bosco from the Ministry of Health, Timor Leste working on a problem tree, indentifying the causes and consequences of undernutrition in Timor Leste

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
9
Participants were introduced to the key messages for
appropriate breastfeeding and complementary feeding
practices, and the evidence to support these messages. Prior
to the theory presentations, country groups were invited to
construct a table indicating the current breastfeeding and
complementary feeding practices in their respective contexts.
Following the theory, participants were asked to consider
which of the practices they had identified were consistent
with the key messages and those which required improving.
The Indigenous Australian group reported that many young
mothers exclusively breastfeed only while in hospital and provide other foods such as formula, cows’ milk, ice-
cream, fruit juice, custard or cereal thereafter; while other young mothers exclusively breastfeed for more than six
months, delaying the introduction of complementary foods.
These inappropriate practices were attributed by the group to a lack of available breastfeeding education and
inappropriate food labeling. The group from Timor Leste noted that many children in Timor Leste receive diets with
inadequate nutrients during the complementary feeding phase, and attributed this to acute poverty, noting that
many families can often only afford to feed their children rice.
Feedback indicated that the sessions on breastfeeding and complementary feeding were particularly useful, with
one participant from Timor Leste reporting that “we [now] know about the kind of food that can be consumed by
the baby ... In Timor Leste porridge is only made from rice, but ... we learnt about mixing other foods with the rice
for children over six months, so they get the right macro and micro nutrients. We think about more things now, not
just if the baby is hungry, but also about the quality of what they eat, if it is appropriate for their age”.
A recap activity the following day in which participants worked together to develop a timeline of appropriate
breastfeeding and complementary feeding practices demonstrated that the group was able to recall the
recommendation that infants should be exclusively breastfed until six months of age, key messages about what
proportion of the daily nutritional requirements that can be met by breastmilk for infants and young children of
different ages and the importance of adding more energy to the diet as the child grows. Participants reported that
working as a single group was enjoyable: “it was fun and we could work together… we were all on the same page
on the nutrition issues”.
The number of participants who correctly answered questions on breastfeeding and complementary feeding rose
between baseline and endline for all but one question, for which there was no change (however, the high number
of correct responses at baseline for this question left little room for improvement), indicating that these sessions
were well understood.
Participants enjoyed working together to create a timeline for breastfeeding and complementary feeding

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
10
5 86 70
4
8
12
Outpatient management of SAM
Management of SAM with complications
Number of participants who correctly answered questions on the managament
of acute malnutrition (n=11)
Baseline Endline
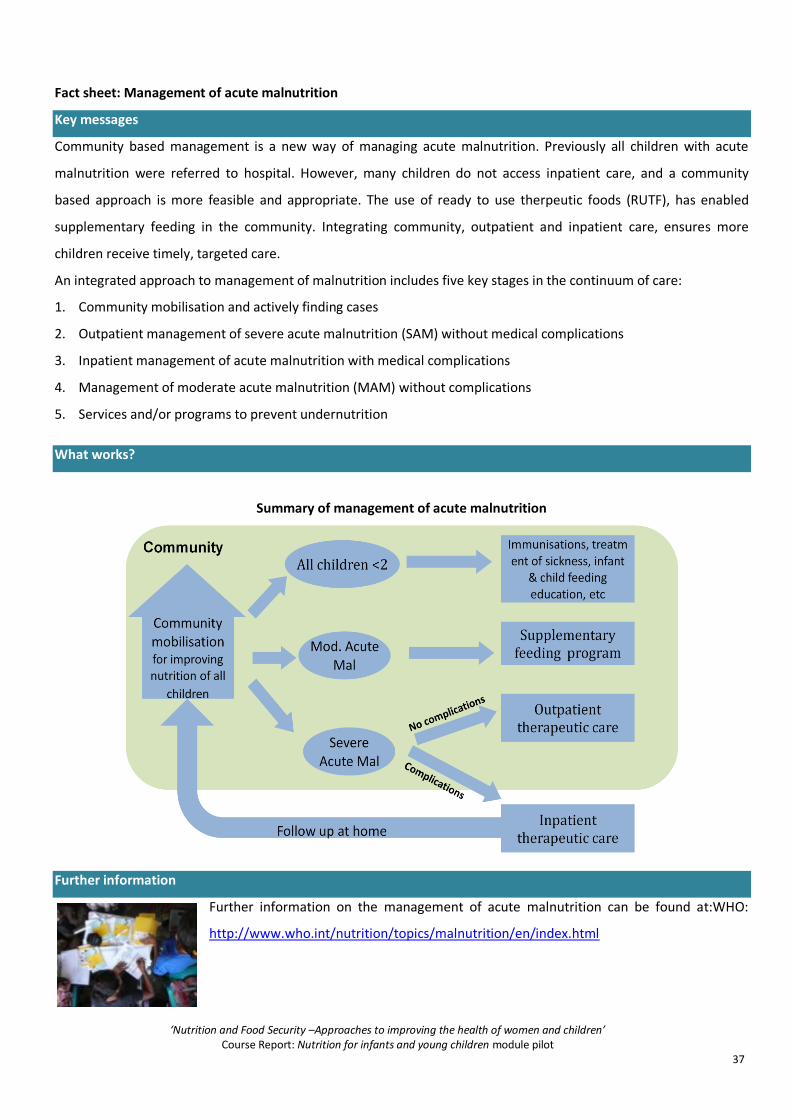
A presentation on evidence based approaches to the integrated management of acute malnutrition (IMAM)
recapped the importance of addressing malnutrition and introduced participants to the five key components of
IMAM. The recommendation that acute malnutrition without medical complications can be managed in the
community using ready to use therapeutic foods was presented, and the advantages of this approach were
discussed. A participant from Timor Leste then presented on IMAM practices in Timor Leste, which closely
reflected the key messages highlighted in the theory presentation.
Baseline and endline quiz results demonstrated a slight
increase in the number of participants who could correctly
answer one of the two questions pertaining to the
integrated management of severe acute malnutrition
(SAM), and a slight decrease in the number of participants
who could correctly answer the second.
2
7 7 710
26
10 10 9 10 9
0
4
8
12
Appropriate duration of breastfeeding
Appropriate complementary
feeding practices
Appropriate feeding practices for infant under six months
Evidence for early initiation of
breastfeeding
Evidence for exclusive
breastfeeding
Introduction of milks other than breastmilk
Number of participants who correctly answered questions on breastfeeding and complementary feeding (n = 11)
Baseline Endline
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
11
Day 3: Best practice in nutrition programming, the Healthy Under 5 Kids program and a field visit
Learning objectives
The importance of taking multi-stakeholder and comprehensive approaches to improving nutrition for
infants and young children
Essential skills and knowledge
Describe the importance of taking multi-stakeholder and comprehensive approaches to improving nutrition
for infants and young children
Using case studies, identify the multi-stakeholder and comprehensive components of programs to improve
nutrition for infants and young children
Theory presentations, activities and evaluation results
A facilitator and a participant from Timor Leste co-presented theory on best-practice programmatic approaches,
and provided examples of how a variety of stakeholders had been engaged and a variety of evidence based
strategies incorporated into a program addressing malnutrition in Timor Leste.
A case study on anaemia prevention in Burma was presented, and participants were encouraged to critique this
case study against the recommended programmatic approaches presented earlier in the day. When asked to
consider the strengths of the program, participants noted that the program was based on “good data” and “looked
at the underlying causes”; the “target group was fully considered and well defined”; the program “addressed the
multiple causes of anaemia”; the “community and other stakeholders worked together”; the program was adapted
to the local context and the education component “made the women feel more empowered”. Participants
suggested that the program’s weaknesses included a failure to address “poor hygiene in the home” and “the high
rate of goiter”; and “not thinking enough about ongoing funding”.
A guest presenter from the Northern Territory Department of Health introduced the Healthy Under 5 Kids (HU5K)
program, a comprehensive monitoring and surveillance program which incorporates a variety of strategies to
prevent undernutrition in children under five years.
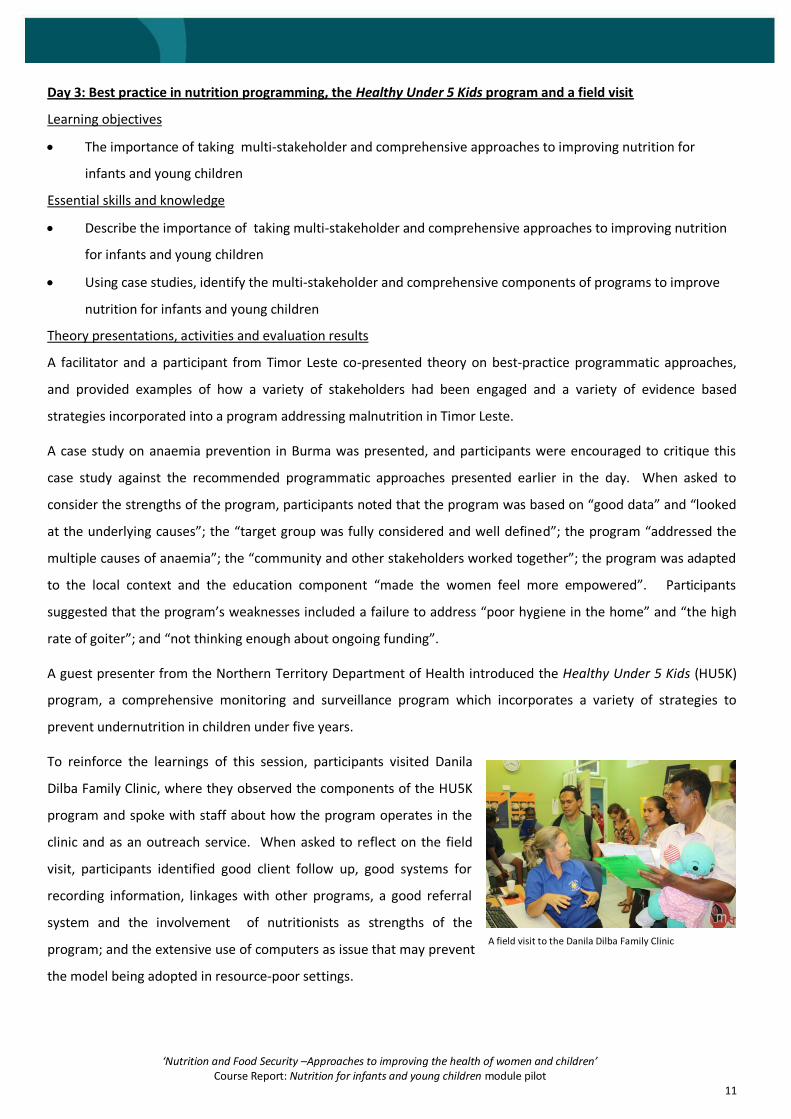
To reinforce the learnings of this session, participants visited Danila
Dilba Family Clinic, where they observed the components of the HU5K
program and spoke with staff about how the program operates in the
clinic and as an outreach service. When asked to reflect on the field
visit, participants identified good client follow up, good systems for
recording information, linkages with other programs, a good referral
system and the involvement of nutritionists as strengths of the
program; and the extensive use of computers as issue that may prevent
the model being adopted in resource-poor settings.
A field visit to the Danila Dilba Family Clinic
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
12
Albertina from the Ministry of Health, Timor Leste, washing her hands as a part of the food safety and hygiene session
Day 4: Food safety and hygiene, an introduction to action planning and a field trip
Learning objectives
The importance of taking multi-stakeholder and comprehensive approaches to improving nutrition for
infants and young children (continued)
The importance of the Five Keys to Safer Food, and personal and environmental hygiene measures for
promoting appropriate nutrition
The causes and consequences of inappropriate Five Keys to Safer Food, and personal and environmental
hygiene practices
Essential skills and knowledge
Using case studies, identify the multi-stakeholder and comprehensive components of programs to improve
nutrition for infants and young children (continued)
Name the Five Keys to Safer Food, and identify personal and environmental hygiene measures for supporting
good nutrition
Theory presentations, activities, and evaluation results
A case study of the Early Childhood Nutrition and Anaemia Prevention Project in
remote Indigenous Australian communities in the Northern Territory, northern
Queensland and the East Kimberly region of north-western Australia was presented,
and participants were encouraged to critique this case study against recommended
programmatic approaches. Participants noted that the strengths of the program
included undertaking formative research in the planning phase to identify the causes
of the problem, using reliable data, involving the community, the health sector and
non government organisations, educating key family members and using a variety of
integrated strategies to prevent anaemia. The group suggested that a remaining
challenge is to “get the belief of the community” in the program.
Participants were invited to re-visit a pre-course “Action Planning
Part 1” work sheet**, which required participants to identify nutrition
or food safety issues affecting infants and young children in their
contexts, the causes of these issues, and which of these causes they
can contribute to addressing in their work role. With the assistance
of facilitators, participants were invited to further consider the
nutrition or food safety issue they selected in the pre-course
worksheet (or another issue), the causes of this issue; and to identify
which cause or causes they are able to address in their work roles.
** Refer to appendix 3 for the Action planning part 1 - pre-course worksheet
Facilitator Danielle from the Fred Hollows Foundation discusses the “Action Planning Part 1” worksheet with Priscilla and Patricia from Anyinginyi Congress
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
13
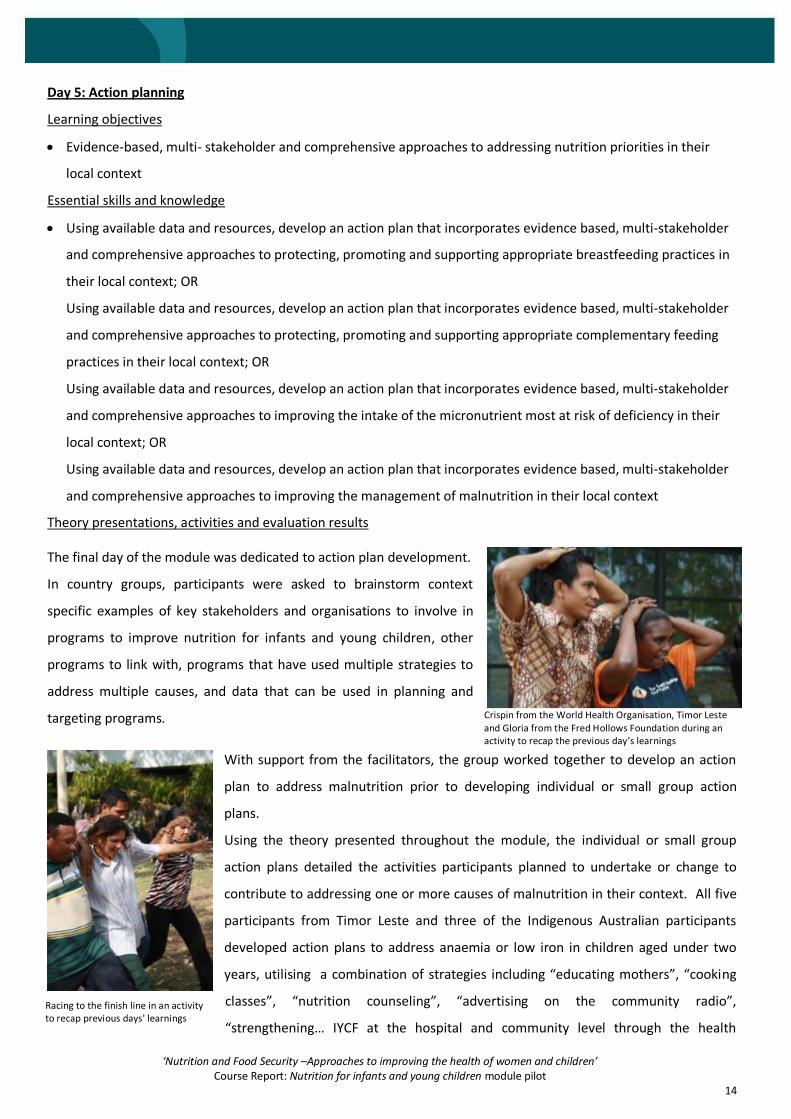
7910 11
0
4
8
12
Ensuring food safety WHO Five Keys to Safer Food
Number of participants who correctly answered questions on food safety
(n=11)
Baseline Endline
Environmental health officers from the Northern Territory Department of Health presented key messages on food
safety and hygiene (based on the World Health Organisation Five Keys to Safer Food) and the evidence to support
these messages.
The learnings were reinforced with a field trip to the Mindil Beach Markets, where participants were given the
opportunity to view the food preparation areas of two food stalls, and invited to observe how the stall holders
implement food safety guidelines and how these are monitored. Participants were encouraged to identify practices
that were and were not consistent with the Five Keys to Safer Food, and investigated whether raw and cooked
foods were stored separately, separate utensils were used for handling raw foods, foods were thoroughly cooked,
and foods were stored and served at the correct temperatures.
During a verbal quiz, participants demonstrated a sound understanding of food safety, and listed storing food at the
wrong temperature, cross-contamination (transferring “bugs” from one food surface to another), and poor
personal hygiene as inappropriate food handling practices. In
a recap session the following day, participants could recall
four of the Five Keys to Safer Food, but were unable to recall
“use clean water and safe materials”. Consistent with these
results, the number of correct responses to the two baseline
and endline quiz questions on food safety rose between
baseline and endline, and all participants were able to identify
“keep food at safe temperatures” as one of the Five Keys to
Safer Food.
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
14
Racing to the finish line in an activity to recap previous days' learnings
Day 5: Action planning
Learning objectives
Evidence-based, multi- stakeholder and comprehensive approaches to addressing nutrition priorities in their
local context
Essential skills and knowledge
Using available data and resources, develop an action plan that incorporates evidence based, multi-stakeholder
and comprehensive approaches to protecting, promoting and supporting appropriate breastfeeding practices in
their local context; OR
Using available data and resources, develop an action plan that incorporates evidence based, multi-stakeholder
and comprehensive approaches to protecting, promoting and supporting appropriate complementary feeding
practices in their local context; OR
Using available data and resources, develop an action plan that incorporates evidence based, multi-stakeholder
and comprehensive approaches to improving the intake of the micronutrient most at risk of deficiency in their
local context; OR
Using available data and resources, develop an action plan that incorporates evidence based, multi-stakeholder
and comprehensive approaches to improving the management of malnutrition in their local context
Theory presentations, activities and evaluation results
The final day of the module was dedicated to action plan development.
In country groups, participants were asked to brainstorm context
specific examples of key stakeholders and organisations to involve in
programs to improve nutrition for infants and young children, other
programs to link with, programs that have used multiple strategies to
address multiple causes, and data that can be used in planning and
targeting programs.
With support from the facilitators, the group worked together to develop an action
plan to address malnutrition prior to developing individual or small group action
plans.
Using the theory presented throughout the module, the individual or small group
action plans detailed the activities participants planned to undertake or change to
contribute to addressing one or more causes of malnutrition in their context. All five
participants from Timor Leste and three of the Indigenous Australian participants
developed action plans to address anaemia or low iron in children aged under two
years, utilising a combination of strategies including “educating mothers”, “cooking
classes”, “nutrition counseling”, “advertising on the community radio”,
“strengthening… IYCF at the hospital and community level through the health
Crispin from the World Health Organisation, Timor Leste and Gloria from the Fred Hollows Foundation during an activity to recap the previous day’s learnings

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
15
promotion program” and “giving out ‘Sprinkles’”. The remaining participants developed action plans to address
wasting through strategies such as “education on hygiene *and+ cooking classes”; and to improve low
breastfeeding rates by holding workshops at biannual women’s camps††.
Participants presented their action plans to the group, and received feedback from fellow participants and the
facilitators.
The action plans will be used for monitoring and evaluation purposes and participants will be supported to
implement their action plans in the months following the module.
†† Refer to Appendix 4 for participants’ action plans

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
16
3
11
11
8
4
9
11
11
6
6
11
11
4
3
7
2
3
5
4
2
0 11
Resources were clear and easy to understand
Presenters encouraged you to have your say and ask questions
Presenters made you want to learn
Presenters made topics interesting and engaging
Presenters were well organised
Presenters presented the material clearly
Presenters demonstrated a good knowledge/ understanding of
the content
Content coverved materials relevant to the learning
objectives
Content was useful for my work
Content was challenging enough
Content was informative
Content was interesting
Participant feedback (n=11)
Strongly agree Agree Disagree Stongly disagree
Discussion
Participant feedback
Participant feedback was generally positive.
Participants reported that the activity-based,
participatory approach consolidated their
understanding of the learnings, and that the
case studies were ‘’well mixed, interesting,
not too much from any one context, just a
good mix’’. As in the Nutrition planning and
programming module, participants reported
that bringing the two country groups together
had been beneficial, reporting that they
“found it interesting to learn from each other
and learn examples from different places”. It
was observed that both groups of participants
“are working to improve things for their own
people”; and that “there were people from
different places, departments and jobs, but
we all worked together”.
Working in groups, particularly for the daily
recap games, was reported to be beneficial,
as the groups could share information and
come to a consensus together.
Field trips were reported to be enjoyable and
a good opportunity to consolidate learnings.
Participants from Timor Leste found the field
visit to the Mindil Beach Markets particularly
useful, as there are plans to establish a similar
market in Timor Leste.

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
17
Expectations
Lear
nin
g
General
“Learn new things” “Learn more skills”
“Increase my knowledge about practices and how to improve practices”
“Learn new things and new information”
Nutrition “Hear more [about] nutrition and food safety” “Learn new things about young children so I can take it back to my community to get better view on good nutrition”
“Learn … how to develop the nutrition/ nutrition treatment at the hospital”
Food safety
“How to implement better food safety”
Food security
“Learn more on food security”
Ob
serv
atio
n
“Visit other areas around Darwin” “Visit to the hospital and clinics to closely observe the preparation process and treatment”
“Do more field trips out of the office to local communities”
“Go to other community to share good experiences”
“Visit to health care center in rural areas”
“Field trip to make a comparison of the situation between Timor and rural Australia”
Ne
two
rkin
g
and
sh
arin
g
“Share experience about nutrition intervention program”
“Sharing good ideas regarding food safety”
“Experience sharing between Timorese and Australian Aboriginals people”
“Sharing ideas with each other”
While all participants agreed or strongly agreed that the content was interesting, informative, and challenging
enough, two of the 11 participants (18%) disagreed with the statement that “the content is useful for my work”. All
participants agreed or strongly agreed that the
module covered material relevant to the learning
objectives, and that it was well planned and
organised. When asked about presenters, all
participants agreed or strongly agreed that the
presenters demonstrated a good knowledge and
understanding of the content, presented clearly, were
well organised, made topics interesting and engaging,
and encouraged participants to ask questions.
While seven participants (64%) agreed or strongly
agreed that the resources were clear and easy to
understand, four participants disagreed (36%), and it
was reported that participants would have found it
useful to receive a manual of the course notes,
factsheets, and the case studies on the first day of the
module.
Participants’ expectations
Participant expectations of this module were gathered on the first day of the course, and were generally aligned
with the content of the course. In summary, participants expected to gain knowledge and skills in nutrition, food
safety and food security; to observe nutrition programs in practices; and to share their experiences with other
participants.
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
18
Baseline and endline quiz results
Participants completed a 20 question quiz at the beginning
(baseline) and at the end (endline) of the module. At baseline,
a facilitator read each question aloud, and participants
recorded their response to each question on a square of paper
and handed it in before the next question was read out.
Participants noted that they preferred this method to a
written test because they felt less pressure and there was
plenty of opportunity to think through each option and seek
clarification. At endline, the quiz was conducted as a written
test, and participants were asked to circle the correct answer.
Comparison of the baseline and endline quiz results
demonstrates that while at baseline, participants answered an
average of 10 out of 20 questions correctly, by endline, this
had improved to 15 of the 20 questions.
Participants’ knowledge improved in 17 of the 20 questions.
For two questions - those relating to sources of micronutrients
and the evidence for exclusive breastfeeding - the number of
correct answers did not change from baseline to endline
(however, it is worth noting that the baseline correct response
rate was high for both of these questions, at eight out of 11
(73%)) and 10 out of 11 (91%) correct answers respectively,
leaving little room for improvement). For the question relating
to the management of severe acute malnutrition (SAM) with
complications, the number of correct answers fell slightly,
from eight out of 11 (72%) to seven out of 11 (64%).
At baseline, only one participant correctly answered a
question on the definition of the 1,000 days; and only two
participants correctly answered questions on the percentage of child deaths in developing countries attributable to
undernutrition, the most common type of malnutrition globally, the cut off to define an iron deficiency anaemia
public health problem, the appropriate duration of breastfeeding, and the appropriate time to introduce milks
other than breastmilk. These questions saw the greatest improvement between baseline and endline, with over
half of participants correctly answering each of these questions at endline.
Baseline and endline quiz results
Subject area/ question Baseline Endline
General
Definition of the 1000 Days 1 8
Definition of "Infants and young children" 7 9
Macro and micro nutrients
Role of protein 6 7
Sources of micronutrients 8 8
Treatment of IDA 4 8
Consequences of micronutrient deficiencies 6 8
Cut off to define an IDA public health
problem 2 7
Malnutrition
Type of malnutrition identifiable by HAZ 5 9
Most common type of malnutrition 2 10
% of child deaths in developing countries
attributable to undernutrition 2 7
Breastfeeding and complementary feeding
Appropriate duration of breastfeeding 2 6
Appropriate complementary feeding
practices 7 10
Appropriate feeding practices for infants
under six months 7 10
Evidence for early initiation of breastfeeding 7 9
Evidence for exclusive breastfeeding 10 10
Introduction of milks other than breastmilk 2 9
Management of acute malnutrition
Outpatient management of SAM 5 6
Management of SAM with complications 8 7
Food safety
Ensuring food safety 7 10
WHO Five Keys to Safer Food 9 11
TOTAL 107 169
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
19
77%
95%
59%
82%
79%
69%
77%
48%
73%
59%
53%
35%
64%
30%
0% 50% 100%
All questions
Food safety
Management of malnutrition
Breastfeeding and complementary
feeding
Malnutrition
Macro and micronutrients
General
Baseline and endline results by subject area
Baseline Endline
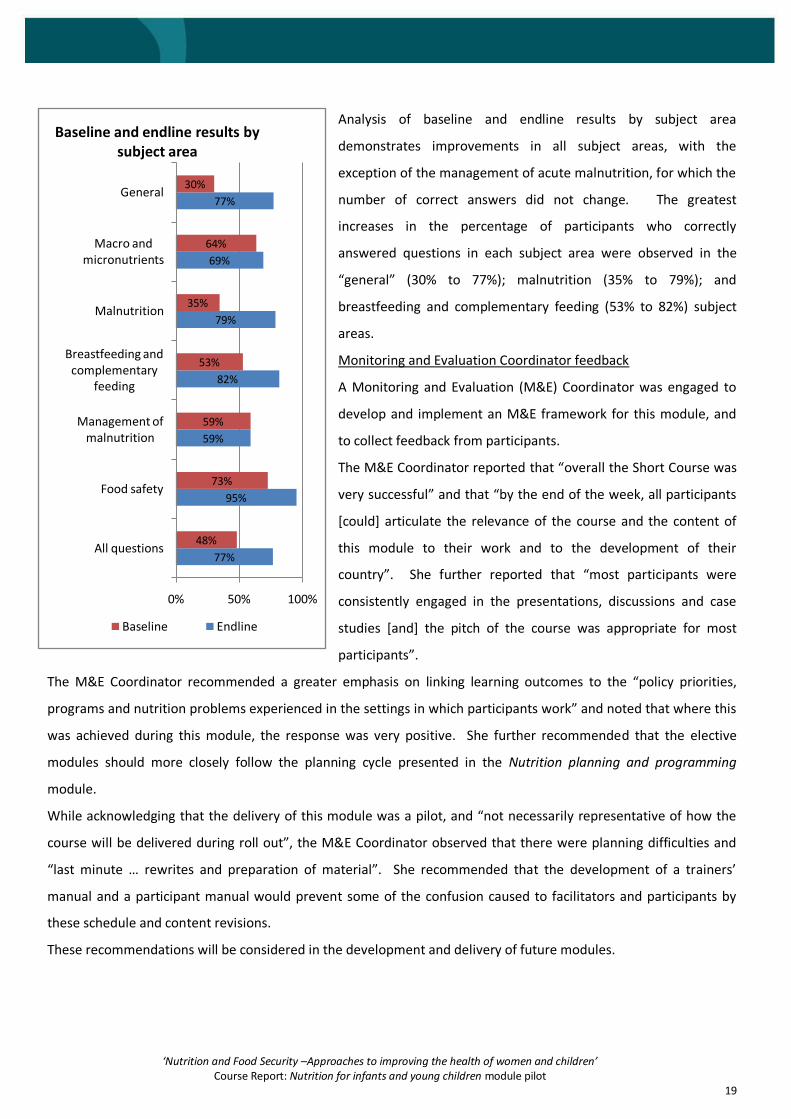
Analysis of baseline and endline results by subject area
demonstrates improvements in all subject areas, with the
exception of the management of acute malnutrition, for which the
number of correct answers did not change. The greatest
increases in the percentage of participants who correctly
answered questions in each subject area were observed in the
“general” (30% to 77%); malnutrition (35% to 79%); and
breastfeeding and complementary feeding (53% to 82%) subject
areas.
Monitoring and Evaluation Coordinator feedback
A Monitoring and Evaluation (M&E) Coordinator was engaged to
develop and implement an M&E framework for this module, and
to collect feedback from participants.
The M&E Coordinator reported that “overall the Short Course was
very successful” and that “by the end of the week, all participants
[could] articulate the relevance of the course and the content of
this module to their work and to the development of their
country”. She further reported that “most participants were
consistently engaged in the presentations, discussions and case
studies [and] the pitch of the course was appropriate for most
participants”.
The M&E Coordinator recommended a greater emphasis on linking learning outcomes to the “policy priorities,
programs and nutrition problems experienced in the settings in which participants work” and noted that where this
was achieved during this module, the response was very positive. She further recommended that the elective
modules should more closely follow the planning cycle presented in the Nutrition planning and programming
module.
While acknowledging that the delivery of this module was a pilot, and “not necessarily representative of how the
course will be delivered during roll out”, the M&E Coordinator observed that there were planning difficulties and
“last minute … rewrites and preparation of material”. She recommended that the development of a trainers’
manual and a participant manual would prevent some of the confusion caused to facilitators and participants by
these schedule and content revisions.
These recommendations will be considered in the development and delivery of future modules.
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
20
Thank you to all the participants for your active participation and your willingness to share
your knowledge, experiences and ideas.
Thanks also to the facilitators, presenters, translators, consultants, members of the
reference group and technical advisory group and Menzies support team; and to the
funders of this pilot, AusAID and The Fred Hollows Foundation.
“This is a war on malnutrition and this knowledge is our weapon”
[Participant quote during the course]

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
21
Appendix 1: Course timetable Day 1 0800 – 0830 House keeping and pre-course survey (expectations) 0830 – 0840 Welcome and acknowledgement of the traditional landowners 0840 – 0920 Reflection on Core module 0920 – 1000 Baseline quiz 1000 – 1015 Morning tea 1015 – 1130 Course purpose, expectations management and ice breaker 1130 – 1245 The role of macro and micro nutrients 1245 – 1330 Lunch 1330 – 1430 Micronutrients at risk 1430 – 1445 Afternoon tea 1445 – 1600 Micronutrients at risk continued 1600 – 1630 Summary of the day/monitoring & evaluation Day 2 0815 – 0900 Recap quiz 0825 – 0830 Monitoring and evaluation 0900 – 1000 Malnutrition: definitions, measuring, causes and consequences 1000 – 1015 Morning tea 1015 – 1040 Malnutrition causes and consequences; problem tree exercise 1040 – 1200 Appropriate breastfeeding practices and evidence; causes of inappropriate practices and evidence based approaches and strategies to protecting, promoting and supporting appropriate breastfeeding practices 1200 – 1230 Lunch 1230 – 1430 Appropriate complementary feeding practices and evidence; causes of inappropriate practices and evidence based approaches and
strategies to promoting and supporting appropriate complementary feeding practices 1430 – 1500 The key components of an integrated approach to the management of acute malnutrition 1500 – 1515 Afternoon tea 1515 – 1545 The key components of an integrated approach to the management of acute malnutrition continued 1615 – 1630 Summary of the day/monitoring & evaluation Day 3 0800 – 0805 Monitoring and evaluation 0805 – 0845 Making a timeline: Appropriate breastfeeding and complementary feeding practices 0845 – 0900 Team photo 0900 – 1000 IMAM case Study: Healthy Under 5 Kids program NT 1000 – 1015 Morning tea 1015 – 1100 Multi-stakeholder comprehensive approaches to improving nutrition 1100 – 1200 Case study: Anaemia project in Burma 1200 – 1245 Lunch 1245 – 1400 Case Study: Anaemia project in Burma continued 1400 – 1630 Field visit to Danila Dilba Family Clinic Day 4 0800 – 0815 Feedback from field visit to Danila Dilba 0815 – 0820 Monitoring and evaluation 0820 – 0845 Recap quiz 0845 – 1000 Case study: Anaemia Prevention in Indigenous Australian Communities 1000 – 1015 Morning tea 1015 – 1100 Case study: Anaemia Prevention in Indigenous Australian Communities continued 1100 – 1200 Pre-course worksheet reflections 1200 – 1300 Lunch 1300 – 1330 Pre-course worksheet reflections continued 1330 – 1445 WHO Food Safety 5 key messages theory presentation 1445 –1600 Field visit to Mindil Beach markets 1600 – 1630 Recap quiz Day 5 0830 – 0825 Recap of WHO 5 keys to food safety and hygiene 0825 – 0930 Food safety and hygiene in Timor Leste case study 0930 – 1000 Action planning 1015 – 1030 Morning tea 1030 – 1115 Action planning continued 1200 – 1230 Daily recap activity quiz 1230 – 1315 Lunch 1315 – 1430 Action planning reporting back to the group 1430 – 1445 Afternoon tea 1445 – 1515 Post course/end line survey conducted 1515 – 1600 Post-course monitoring and evlaluation 1600 – 1645 Presentations of certificates, photos and thanks you to participants and facilitators 1645 – 1700 Presentation of the group monitoring and evaluation results

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
22
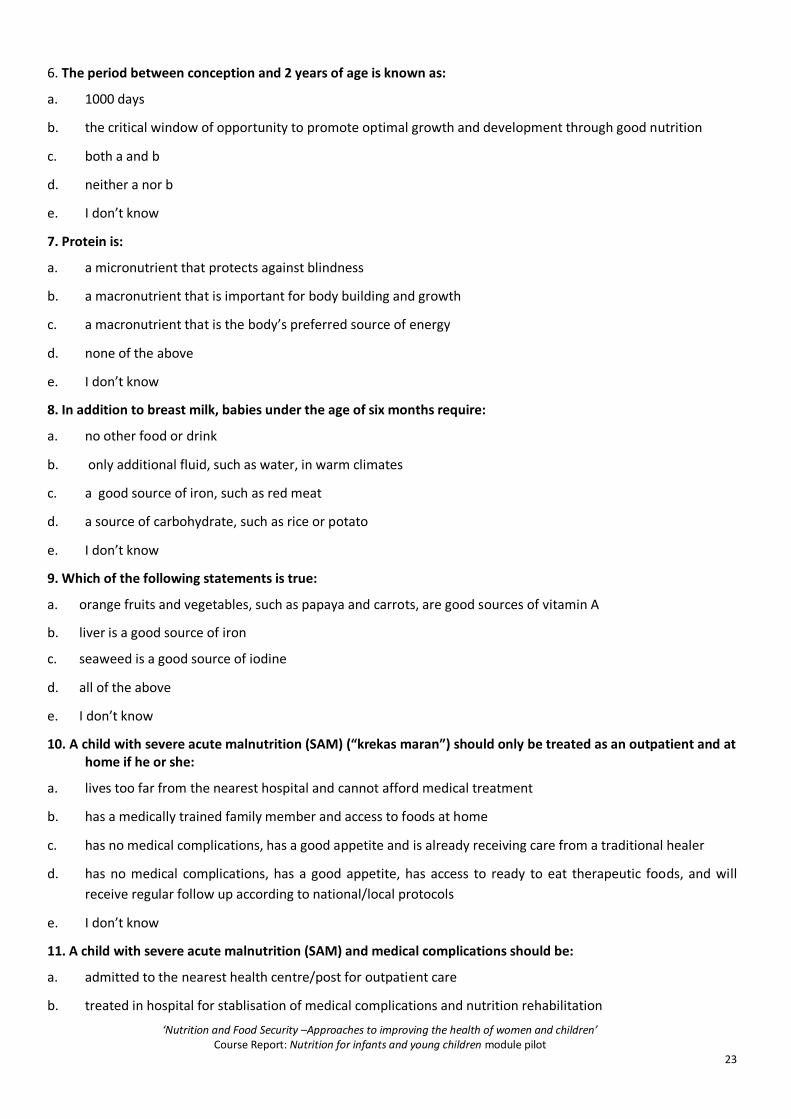
Appendix 2: Baseline and endline quiz
1. In developing countries what percentage of deaths of children under 5 years can be attributed to undernutrition:
a. more than a half
b. less than 2 %
c. almost a quarter
d. about 20 percent
e. I don’t know
2. Globally the most common type of malnutrition is:
a. stunting
b. wasting
c. iron deficiency anaemia
d. overweight
e. I don’t know
3. The term “infants and young children” refers to:
a. only children under 5 years
b. only children under 10 years
c. only children under 1 year only
d. only children under 18 months
e. I don’t know
4. Measuring height for age (HAZ) can be used to identify a child with:
a. severe acute malnutrition
b. moderately acute malnutrition
c. stunting
d. overweight
e. I don’t know
5. Breastfeeding should:
a. stop as soon as the child turns 2
b. stop as soon as the child is able to feed itself
c. continue until the child is at least 2 years
d. continue exclusively until the child is at least 2 years
e. I don’t know
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
23
6. The period between conception and 2 years of age is known as:
a. 1000 days
b. the critical window of opportunity to promote optimal growth and development through good nutrition
c. both a and b
d. neither a nor b
e. I don’t know
7. Protein is:
a. a micronutrient that protects against blindness
b. a macronutrient that is important for body building and growth
c. a macronutrient that is the body’s preferred source of energy
d. none of the above
e. I don’t know
8. In addition to breast milk, babies under the age of six months require:
a. no other food or drink
b. only additional fluid, such as water, in warm climates
c. a good source of iron, such as red meat
d. a source of carbohydrate, such as rice or potato
e. I don’t know
9. Which of the following statements is true:
a. orange fruits and vegetables, such as papaya and carrots, are good sources of vitamin A
b. liver is a good source of iron
c. seaweed is a good source of iodine
d. all of the above
e. I don’t know
10. A child with severe acute malnutrition (SAM) (“krekas maran”) should only be treated as an outpatient and at home if he or she:
a. lives too far from the nearest hospital and cannot afford medical treatment
b. has a medically trained family member and access to foods at home
c. has no medical complications, has a good appetite and is already receiving care from a traditional healer
d. has no medical complications, has a good appetite, has access to ready to eat therapeutic foods, and will
receive regular follow up according to national/local protocols
e. I don’t know
11. A child with severe acute malnutrition (SAM) and medical complications should be:
a. admitted to the nearest health centre/post for outpatient care
b. treated in hospital for stablisation of medical complications and nutrition rehabilitation

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
24
c. be treated in the home with ready to eat therapeutic foods at home
d. offered more breastmilk to increase appetite
e. I don’t know
12. Early initiation of breastfeeding has been shown to:
a. reduce neonatal mortality
b. cause breast engorgement
c. increase the risk of respiratory illness
d. delay wound healing after a caesarian section
e. I don’t know
13. Exclusive breastfeeding for six months reduces the risk of:
a. pneumonia and diarrhoea
b. allergies
c. infant mortality
d. all of the above
e. I don’t know
14. In order to ensure food safety:
a. cooked food should be kept at a temperature between 5 and 60 degrees Celsius
b. food should never be boiled
c. cooked and raw food should be stored separately
d. once cooked, food should never be re-heated
e. I don’t know
15. Intermittent iron supplementation is recommended in populations where
a. the soil is low in iron
b. red meat is not eaten
c. the prevalence of iron deficiency anaemia (IDA) is more than 20% in children under 5 or school age children
d. all of the above
e. I don’t know
16. Which of the following statements is true?
a. Children require other milks, in addition to breastmilk, at the age of six months as an additional source of
iron
b. Children require other milks, in addition to breastmilk, at the age of nine months to ensure good bone
development
c. It is recommended that milks other than breastmilk should not be given to a child before the age of five years
d. It is recommended that milks other than breastmilk should not given to a child before the age of 12 months
e. I don’t know

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
25
17. Which of the following statements is true?
a. iron deficiency can cause night blindness
b. vitamin A deficiency can cause goitre
c. iodine deficiency can cause anaemia
d. none of the above
e. I don’t know
18. An appropriate complementary feeding practice is to:
a. give thick mashed foods from the age of six months of age
b. give thin runny foods from the age of six months
c. replace breast milk with complementary foods when the child is weaned at the age of six months
d. stop complementary feeding when the child has a common illness
e. I don’t know
19. If a child has iron deficiency anaemia (IDA), he or she should?
a. seek treatment and drink tea with meals as tea helps with iron absorption
b. seek treatment and eat foods that are rich in vitamin C such as tomatoes and oranges with meals, as vitamin
C assists with iron absorption
c. seek treatment and stop breastfeeding until the iron deficiency is cured
d. all of the above
e. I don’t know
20. Which of the following is one of the WHO five keys to safer food?
a. freeze all left over food
b. keep food at safe temperatures
c. wear a hairnet when preparing food
d. shower every day
e. I don’t know
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
26
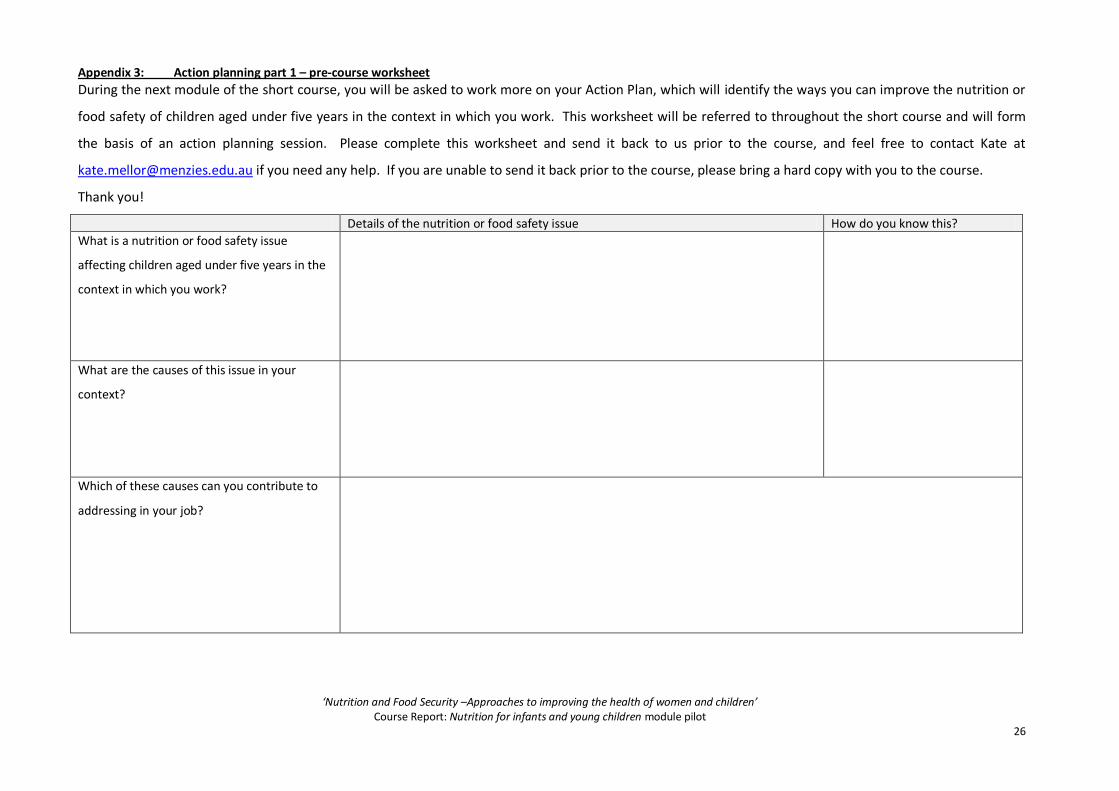
Appendix 3: Action planning part 1 – pre-course worksheet
During the next module of the short course, you will be asked to work more on your Action Plan, which will identify the ways you can improve the nutrition or
food safety of children aged under five years in the context in which you work. This worksheet will be referred to throughout the short course and will form
the basis of an action planning session. Please complete this worksheet and send it back to us prior to the course, and feel free to contact Kate at
[email protected] if you need any help. If you are unable to send it back prior to the course, please bring a hard copy with you to the course.
Thank you!
Details of the nutrition or food safety issue How do you know this?
What is a nutrition or food safety issue
affecting children aged under five years in the
context in which you work?
What are the causes of this issue in your
context?
Which of these causes can you contribute to
addressing in your job?
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
27
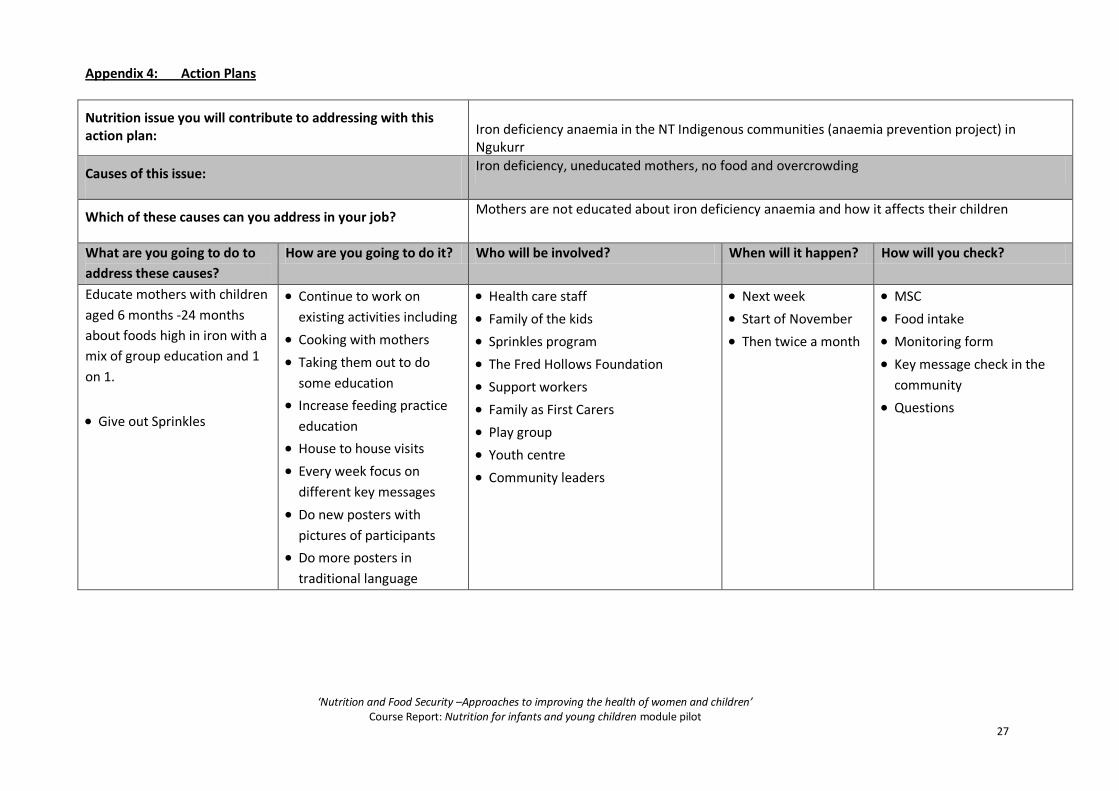
Appendix 4: Action Plans
Nutrition issue you will contribute to addressing with this action plan:
Iron deficiency anaemia in the NT Indigenous communities (anaemia prevention project) in Ngukurr
Causes of this issue: Iron deficiency, uneducated mothers, no food and overcrowding
Which of these causes can you address in your job? Mothers are not educated about iron deficiency anaemia and how it affects their children
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Educate mothers with children
aged 6 months -24 months
about foods high in iron with a
mix of group education and 1
on 1.
Give out Sprinkles
Continue to work on
existing activities including
Cooking with mothers
Taking them out to do
some education
Increase feeding practice
education
House to house visits
Every week focus on
different key messages
Do new posters with
pictures of participants
Do more posters in
traditional language
Health care staff
Family of the kids
Sprinkles program
The Fred Hollows Foundation
Support workers
Family as First Carers
Play group
Youth centre
Community leaders
Next week
Start of November
Then twice a month
MSC
Food intake
Monitoring form
Key message check in the
community
Questions
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
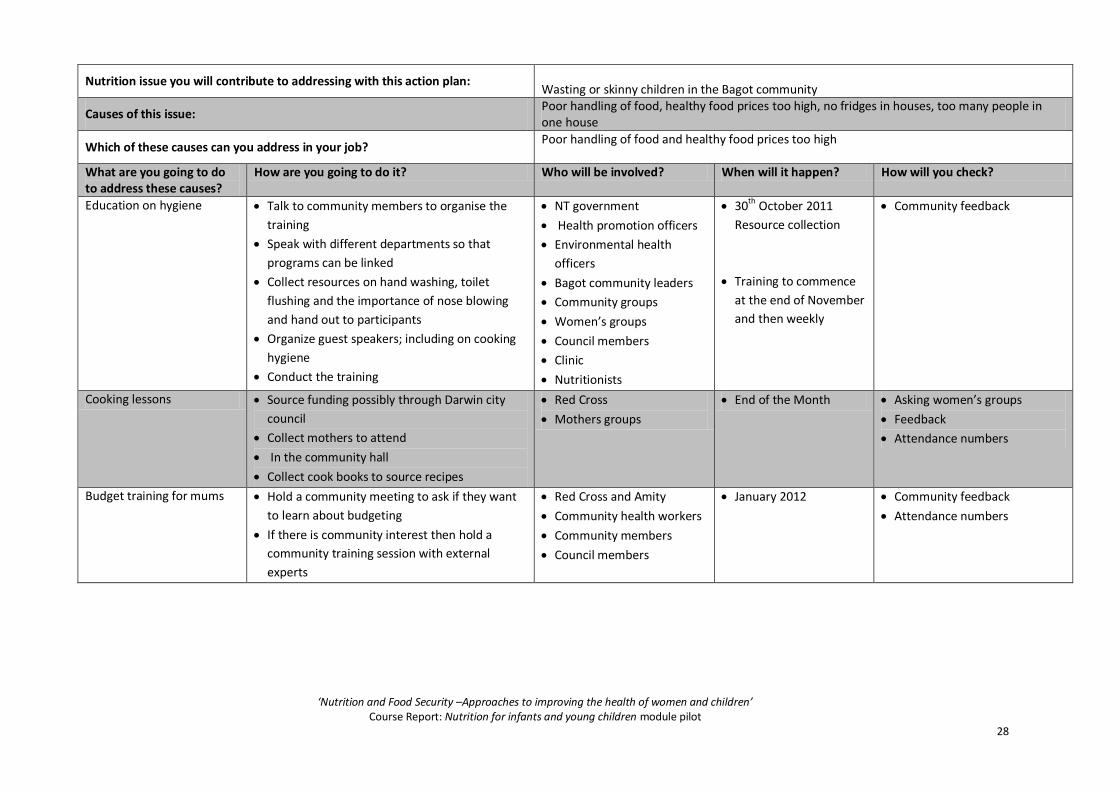
28
Nutrition issue you will contribute to addressing with this action plan: Wasting or skinny children in the Bagot community
Causes of this issue: Poor handling of food, healthy food prices too high, no fridges in houses, too many people in one house
Which of these causes can you address in your job? Poor handling of food and healthy food prices too high
What are you going to do to address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Education on hygiene
Talk to community members to organise the
training
Speak with different departments so that
programs can be linked
Collect resources on hand washing, toilet
flushing and the importance of nose blowing
and hand out to participants
Organize guest speakers; including on cooking
hygiene
Conduct the training
NT government
Health promotion officers
Environmental health
officers
Bagot community leaders
Community groups
Women’s groups
Council members
Clinic
Nutritionists
30th October 2011
Resource collection
Training to commence
at the end of November
and then weekly
Community feedback
Cooking lessons Source funding possibly through Darwin city
council
Collect mothers to attend
In the community hall
Collect cook books to source recipes
Red Cross
Mothers groups
End of the Month Asking women’s groups
Feedback
Attendance numbers
Budget training for mums Hold a community meeting to ask if they want
to learn about budgeting
If there is community interest then hold a
community training session with external
experts
Red Cross and Amity
Community health workers
Community members
Council members
January 2012 Community feedback
Attendance numbers
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
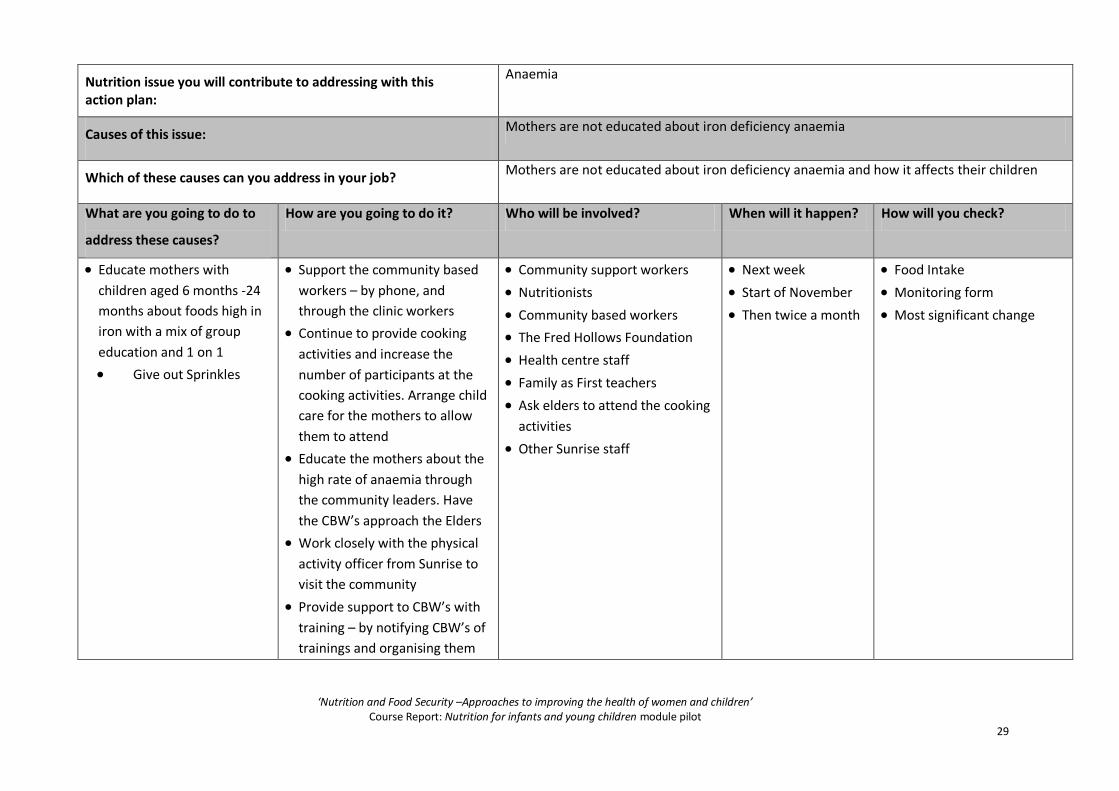
29
Nutrition issue you will contribute to addressing with this action plan:
Anaemia
Causes of this issue: Mothers are not educated about iron deficiency anaemia
Which of these causes can you address in your job? Mothers are not educated about iron deficiency anaemia and how it affects their children
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Educate mothers with
children aged 6 months -24
months about foods high in
iron with a mix of group
education and 1 on 1
Give out Sprinkles
Support the community based
workers – by phone, and
through the clinic workers
Continue to provide cooking
activities and increase the
number of participants at the
cooking activities. Arrange child
care for the mothers to allow
them to attend
Educate the mothers about the
high rate of anaemia through
the community leaders. Have
the CBW’s approach the Elders
Work closely with the physical
activity officer from Sunrise to
visit the community
Provide support to CBW’s with
training – by notifying CBW’s of
trainings and organising them
Community support workers
Nutritionists
Community based workers
The Fred Hollows Foundation
Health centre staff
Family as First teachers
Ask elders to attend the cooking
activities
Other Sunrise staff
Next week
Start of November
Then twice a month
Food Intake
Monitoring form
Most significant change
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
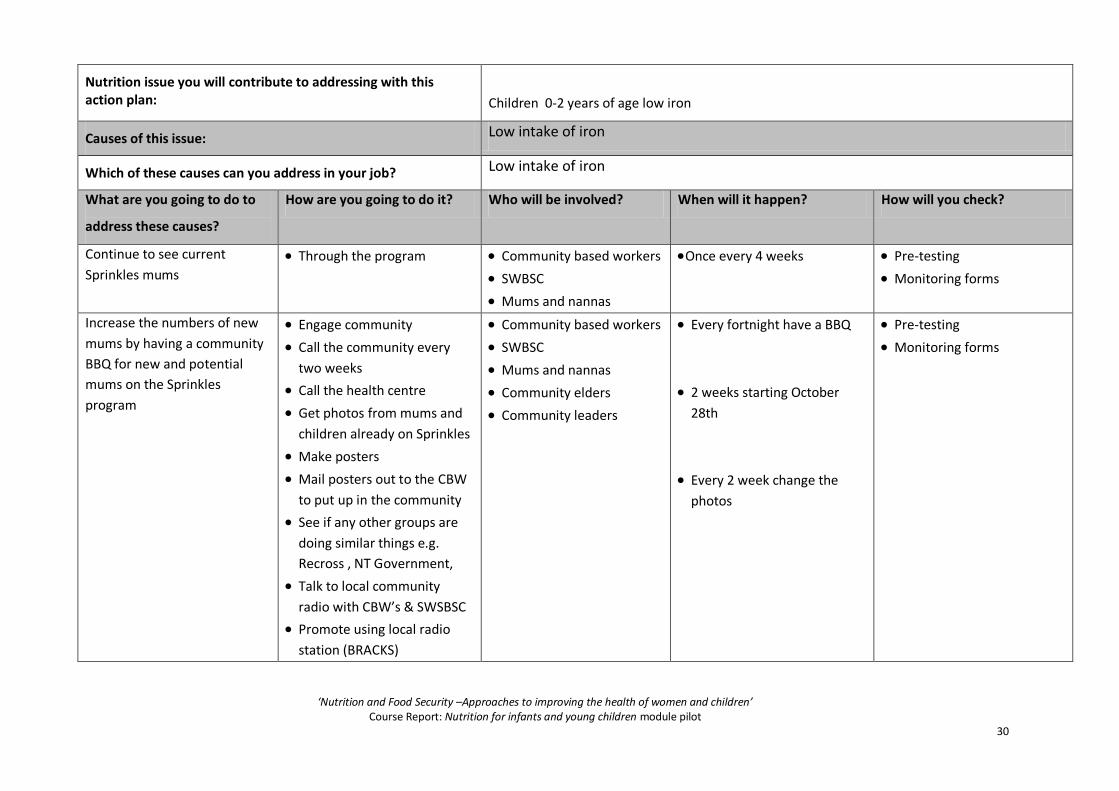
30
Nutrition issue you will contribute to addressing with this action plan:
Children 0-2 years of age low iron
Causes of this issue: Low intake of iron
Which of these causes can you address in your job? Low intake of iron
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Continue to see current
Sprinkles mums Through the program Community based workers
SWBSC
Mums and nannas
Once every 4 weeks
Pre-testing
Monitoring forms
Increase the numbers of new
mums by having a community
BBQ for new and potential
mums on the Sprinkles
program
Engage community
Call the community every
two weeks
Call the health centre
Get photos from mums and
children already on Sprinkles
Make posters
Mail posters out to the CBW
to put up in the community
See if any other groups are
doing similar things e.g.
Recross , NT Government,
Talk to local community
radio with CBW’s & SWSBSC
Promote using local radio
station (BRACKS)
Community based workers
SWBSC
Mums and nannas
Community elders
Community leaders
Every fortnight have a BBQ
2 weeks starting October
28th
Every 2 week change the
photos
Pre-testing
Monitoring forms
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
31
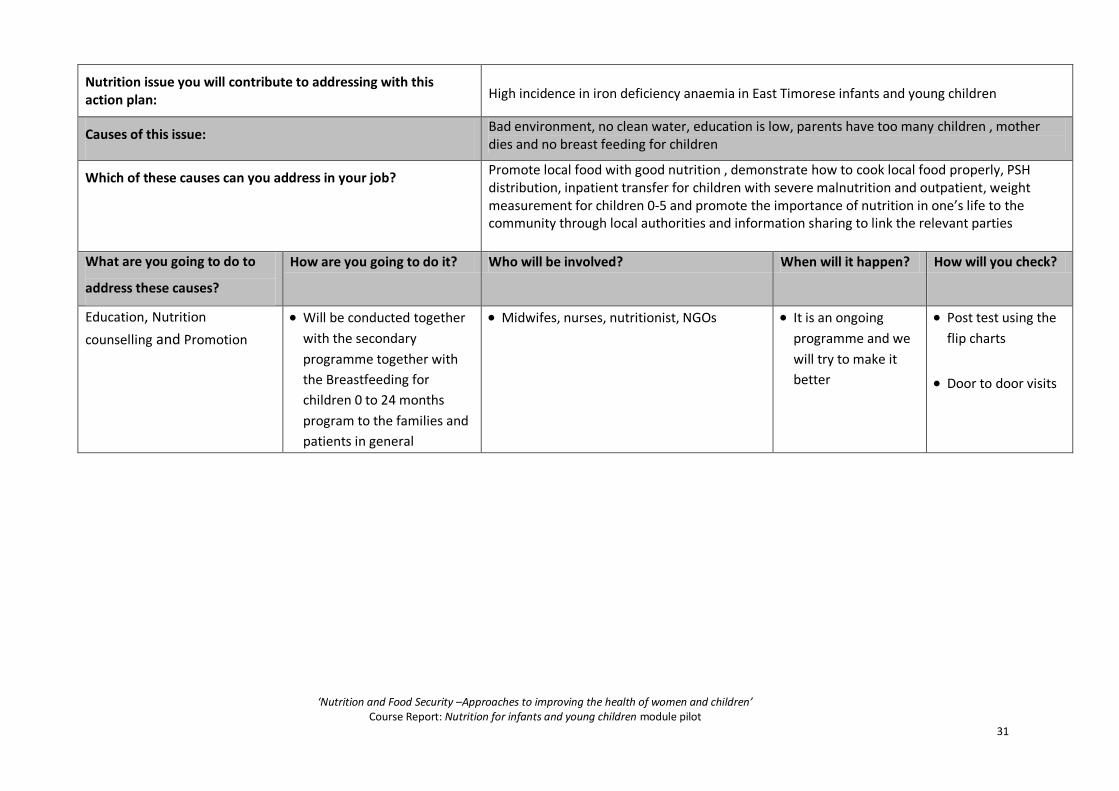
Nutrition issue you will contribute to addressing with this action plan:
High incidence in iron deficiency anaemia in East Timorese infants and young children
Causes of this issue: Bad environment, no clean water, education is low, parents have too many children , mother dies and no breast feeding for children
Which of these causes can you address in your job? Promote local food with good nutrition , demonstrate how to cook local food properly, PSH distribution, inpatient transfer for children with severe malnutrition and outpatient, weight measurement for children 0-5 and promote the importance of nutrition in one’s life to the community through local authorities and information sharing to link the relevant parties
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Education, Nutrition
counselling and Promotion
Will be conducted together
with the secondary
programme together with
the Breastfeeding for
children 0 to 24 months
program to the families and
patients in general
Midwifes, nurses, nutritionist, NGOs It is an ongoing
programme and we
will try to make it
better
Post test using the
flip charts
Door to door visits
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
32
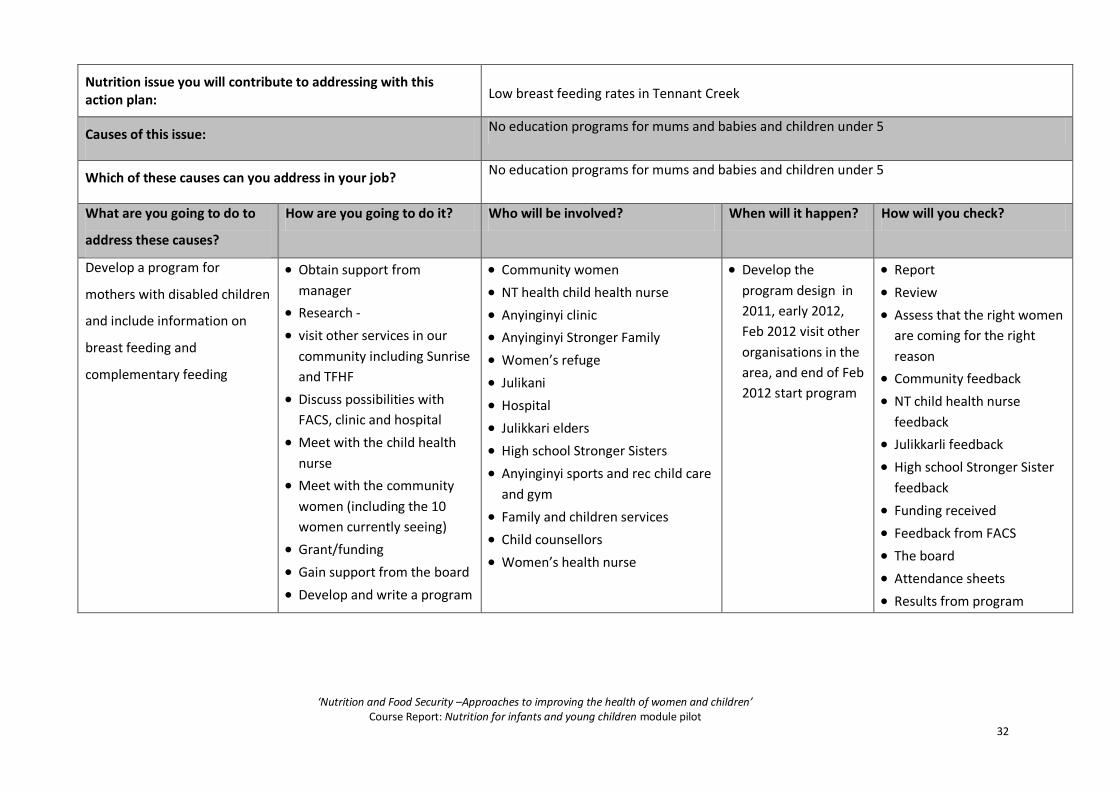
Nutrition issue you will contribute to addressing with this action plan:
Low breast feeding rates in Tennant Creek
Causes of this issue: No education programs for mums and babies and children under 5
Which of these causes can you address in your job? No education programs for mums and babies and children under 5
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Develop a program for
mothers with disabled children
and include information on
breast feeding and
complementary feeding
Obtain support from
manager
Research -
visit other services in our
community including Sunrise
and TFHF
Discuss possibilities with
FACS, clinic and hospital
Meet with the child health
nurse
Meet with the community
women (including the 10
women currently seeing)
Grant/funding
Gain support from the board
Develop and write a program
Community women
NT health child health nurse
Anyinginyi clinic
Anyinginyi Stronger Family
Women’s refuge
Julikani
Hospital
Julikkari elders
High school Stronger Sisters
Anyinginyi sports and rec child care
and gym
Family and children services
Child counsellors
Women’s health nurse
Develop the
program design in
2011, early 2012,
Feb 2012 visit other
organisations in the
area, and end of Feb
2012 start program
Report
Review
Assess that the right women
are coming for the right
reason
Community feedback
NT child health nurse
feedback
Julikkarli feedback
High school Stronger Sister
feedback
Funding received
Feedback from FACS
The board
Attendance sheets
Results from program
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
33
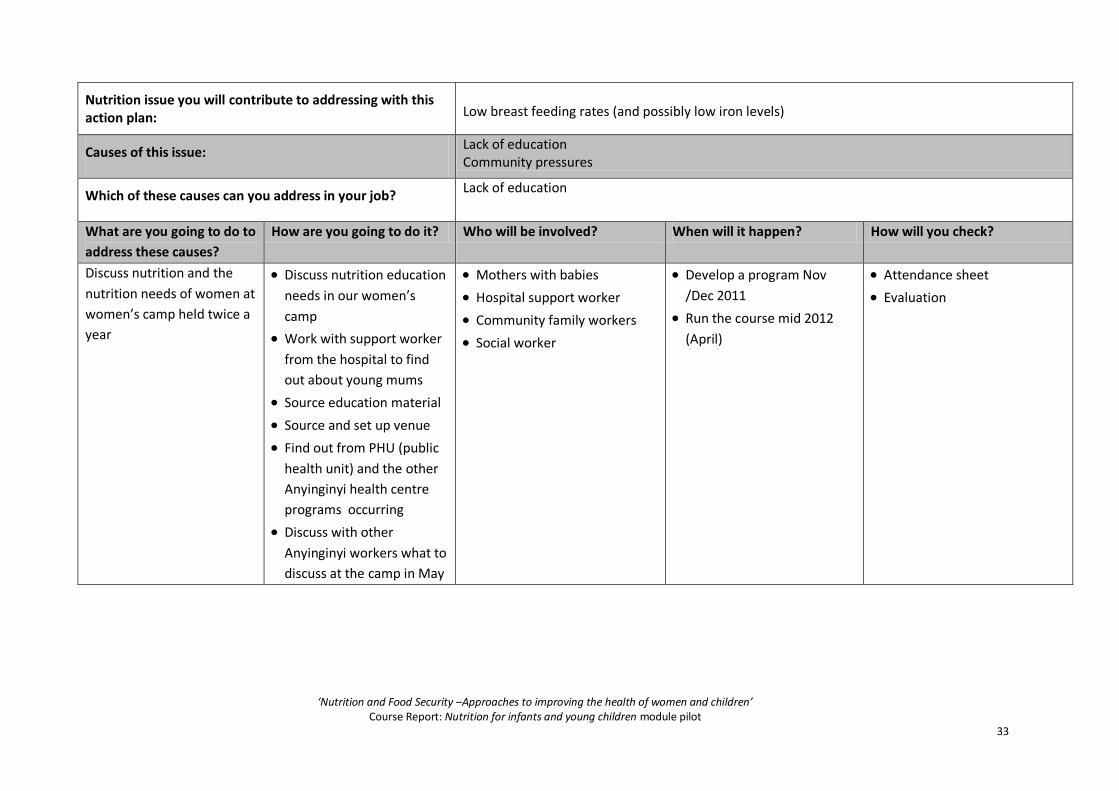
Nutrition issue you will contribute to addressing with this action plan:
Low breast feeding rates (and possibly low iron levels)
Causes of this issue: Lack of education Community pressures
Which of these causes can you address in your job? Lack of education
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Discuss nutrition and the
nutrition needs of women at
women’s camp held twice a
year
Discuss nutrition education
needs in our women’s
camp
Work with support worker
from the hospital to find
out about young mums
Source education material
Source and set up venue
Find out from PHU (public
health unit) and the other
Anyinginyi health centre
programs occurring
Discuss with other
Anyinginyi workers what to
discuss at the camp in May
Mothers with babies
Hospital support worker
Community family workers
Social worker
Develop a program Nov
/Dec 2011
Run the course mid 2012
(April)
Attendance sheet
Evaluation
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
34
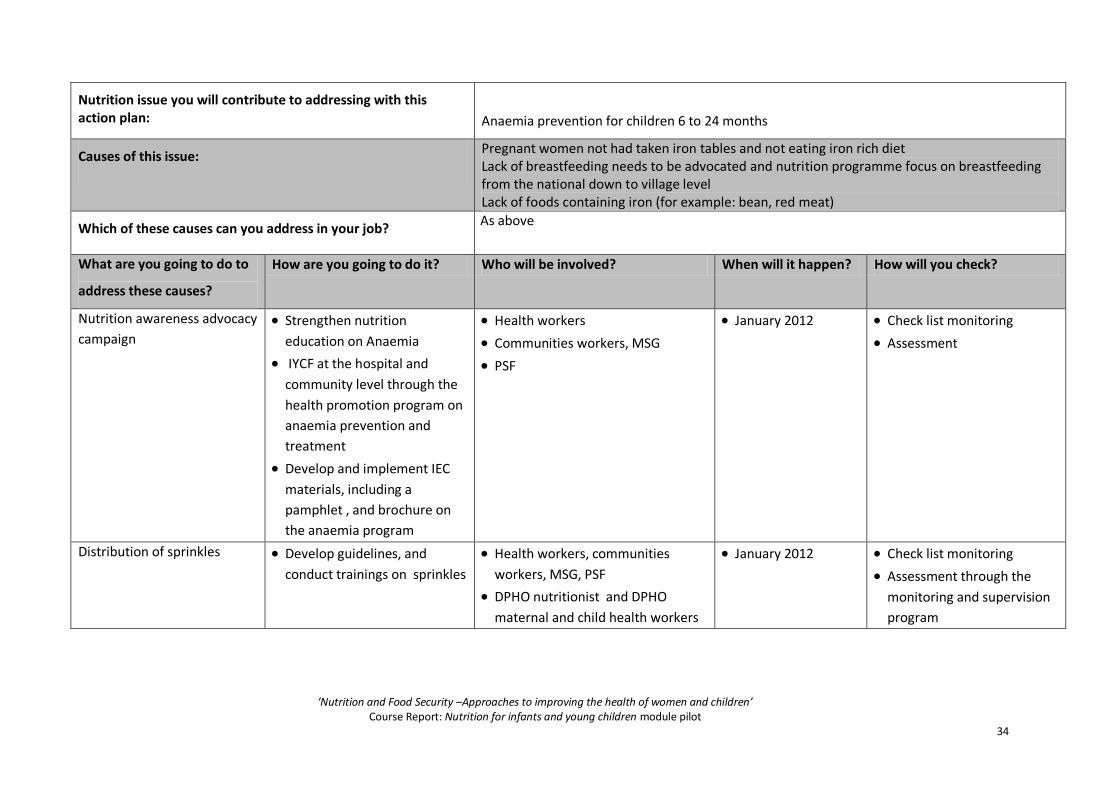
Nutrition issue you will contribute to addressing with this action plan:
Anaemia prevention for children 6 to 24 months
Causes of this issue: Pregnant women not had taken iron tables and not eating iron rich diet Lack of breastfeeding needs to be advocated and nutrition programme focus on breastfeeding from the national down to village level Lack of foods containing iron (for example: bean, red meat)
Which of these causes can you address in your job? As above
What are you going to do to
address these causes?
How are you going to do it? Who will be involved? When will it happen? How will you check?
Nutrition awareness advocacy
campaign
Strengthen nutrition
education on Anaemia
IYCF at the hospital and
community level through the
health promotion program on
anaemia prevention and
treatment
Develop and implement IEC
materials, including a
pamphlet , and brochure on
the anaemia program
Health workers
Communities workers, MSG
PSF
January 2012 Check list monitoring
Assessment
Distribution of sprinkles Develop guidelines, and
conduct trainings on sprinkles
Health workers, communities
workers, MSG, PSF
DPHO nutritionist and DPHO
maternal and child health workers
January 2012 Check list monitoring
Assessment through the
monitoring and supervision
program

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
35
Appendix 5: Fact sheets Fact sheet: Breastfeeding
Key messages and the evidence
Breastfeeding is the natural and normal way of feeding babies from birth. Breastmilk provides an unequalled source
of nutrition and protection against infection. In addition, breastfeeding benefits the physical and mental health of
both mother and baby.
Initiation of breastfeeding within one hour of birth
Early initiation of breastfeeding reduces the risk of neonatal death by 19-22%
Colostrum, the first, yellowish milk, protects infants from illness
Breastfeed exclusively for the first six months – no teas, no water, no honey – nothing but breastmilk
Breastmilk contains all the energy, other nutrients and water infants need for the first six months of life
Exclusive breastfeeding reduces infant mortality and protects the infant from acute respiratory illness, diarrhoea
and other infections; and reduces the risk of chronic disease later in life
Continue to breastfeed until two years and beyond
Breastmilk continues to provide a significant proportion of energy and other nutrients into the second year of life
Breastfeed frequently, on demand, day and night
Baby-led feeding ensures baby’s cues are responded to
Frequent feeding helps stimulate and maintain milk production
Continue to breastfeed when the child or mother has a common illness
The nutrients and protective factors in breastmilk are important when the mother or infant is ill
Frequent breastfeeding meets additional fluid and energy requirements during illness and helps with recovery
Avoid artificial nipples – if the mother can not be with the baby, she should express milk and the baby should drink
from a cup
Artificial nipples increase the risk of illness, especially diarrhoea
Cup-feeding provides physical stimulation and closeness and does not interfere with the infant’s natural feeding
reflexes
Infants can be cup fed from any age
What works?
Several approaches have been found to improve breastfeeding practices, including: antenatal and postnatal
counselling by trained peers and health workers; targeted mass media promotion; and baby friendly hospital and
community initiatives. Successful programs use multiple strategies to address the multiple causes of inappropriate
breastfeeding practices, utilise relevant data, involve key stakeholders and build into other programs, plans and
policies.
Further information
Further information about breastfeeding can be found at: http://www.who.int/topics/breastfeeding/en/

‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
36
Fact sheet: Complementary Feeding
Key messages
Breastmilk alone provides enough energy and other nutrients for the first six
months of life. After six months of age, extra nutrients are required for healthy
growth and development. Complementary foods should be introduced, and
breastfeeding should be continued until two years and beyond.
Start to give foods when the baby is six months old and continue to
breastfeed until the child is two years or older
Feed baby responsively- allow baby to lead feeding and respond to cues
Practice good hygiene and proper handling of food
Increase the amount of foods as the child gets older, and continue to breastfeed
Change the texture and consistency to match the growing child’s needs and abilities
In addition to breastmilk, as babies get older feed frequently, and increasing the number of times a day the baby
is fed
Feed babies a variety of foods, in addition to breastmilk
Give babies fortified foods or micronutrient supplements when needed
Continue to breastfeed during illness and give extra food, more often after illness
What works?
Several approaches have been found to improve complementary feeding practices, including: behaviour change
counselling by trained peers and health workers; and increasing the energy and micronutrient density of
complementary foods at home and through simple technologies. In food insecure populations, provision of food
supplements should also be considered. Successful programs use multiple strategies to address the multiple causes of
inappropriate complementary feeding practices, utilise relevant data, involve key stakeholders and build into other
programs, plans and policies.
Further information
Further information on complementary feeding can be found at:
http://www.who.int/nutrition/publications/infantfeeding/9789241594745/en/index.html
http://www.who.int/nutrition/publications/infantfeeding/a85622/en/index.html
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
37
Fact sheet: Management of acute malnutrition
Key messages
Community based management is a new way of managing acute malnutrition. Previously all children with acute
malnutrition were referred to hospital. However, many children do not access inpatient care, and a community
based approach is more feasible and appropriate. The use of ready to use therpeutic foods (RUTF), has enabled
supplementary feeding in the community. Integrating community, outpatient and inpatient care, ensures more
children receive timely, targeted care.
An integrated approach to management of malnutrition includes five key stages in the continuum of care:
1. Community mobilisation and actively finding cases
2. Outpatient management of severe acute malnutrition (SAM) without medical complications
3. Inpatient management of acute malnutrition with medical complications
4. Management of moderate acute malnutrition (MAM) without complications
5. Services and/or programs to prevent undernutrition
What works?
Summary of management of acute malnutrition
Further information
Further information on the management of acute malnutrition can be found at:WHO:
http://www.who.int/nutrition/topics/malnutrition/en/index.html
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
38
Factsheet: Program approaches
Key Messages
When developing a nutrition or food security program, there are four
important programmatic approaches to consider:
1. Use data to plan and target
For example, review existing health data or collect new data to identify the
nutrition and food security issues for 0-5 year old, and identify the immediate
and underlying causes of these issues
Helps identify the issue
Helps identify the best way to address the issue
Ensures that the right people are targeted, with the right approaches
2. Link programs into existing systems, programs, plans or policies (Integrated)
For example, distribution of ready to use food supplements by an existing network of community health
volunteers/workers
Enables resource and information sharing
Prevents duplication
Improves reach
Ensures that all stakeholders are working towards a common goal
3. Involve a range of relevant key stakeholders (Multi-stakeholder)
For example, involving the community, the government, non-government organisations (NGOs), women’s groups
and health centres at all stages of planning, implementing and evaluating and reviewing the program
Ensures that the problem is well-understood and there is a shared understanding by everyone involved
Ensures that potential linkages are identified
Ensures that the right people are involved and the community has ownership of the program
Enables cooperation and resource sharing
4. Include multiple strategies, known to work, to address multiple causes (Comprehensive and Evidence Based)
For example, provide nutrition education along with vitamin
supplementation, to encourage dietary change whilst ensuring babies are
receiving the nutrients they need in the short term
Broader range of causes are addressed, in more a holistic way
Ensures that the results of the program are sustaina
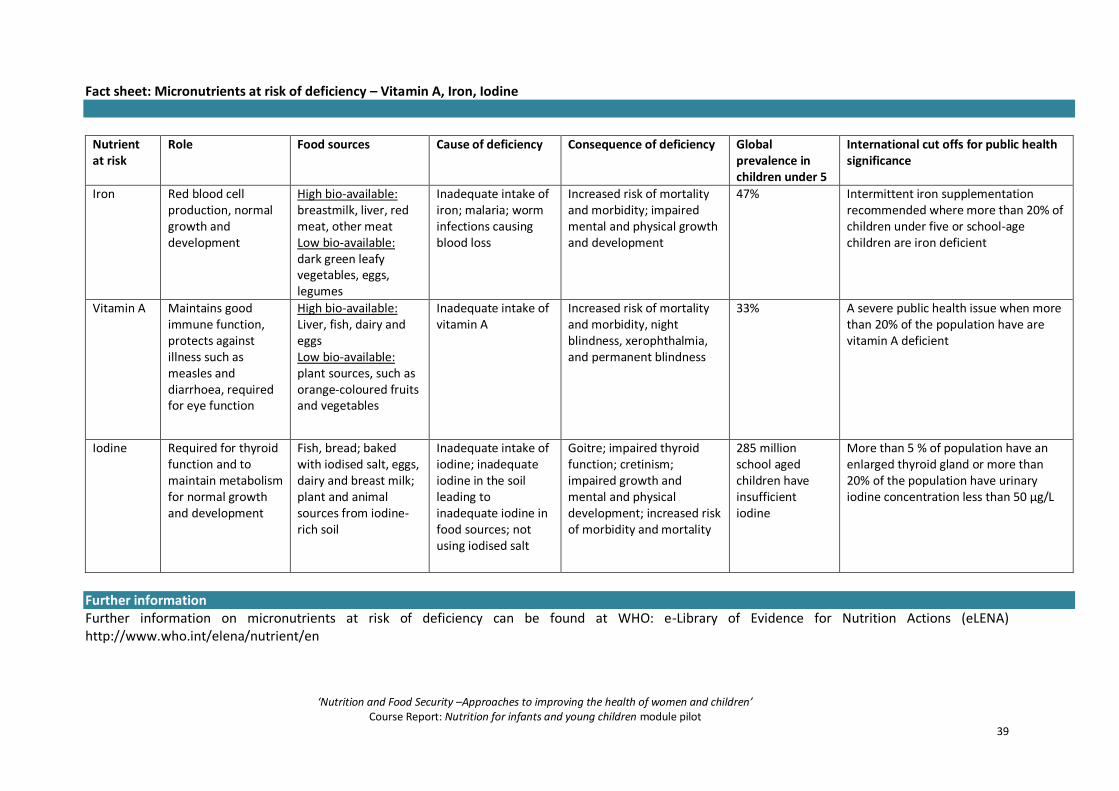
‘Nutrition and Food Security –Approaches to improving the health of women and children’ Course Report: Nutrition for infants and young children module pilot
39
Fact sheet: Micronutrients at risk of deficiency – Vitamin A, Iron, Iodine
Nutrient at risk
Role Food sources Cause of deficiency Consequence of deficiency Global prevalence in children under 5
International cut offs for public health significance
Iron Red blood cell production, normal growth and development
High bio-available: breastmilk, liver, red meat, other meat Low bio-available: dark green leafy vegetables, eggs, legumes
Inadequate intake of iron; malaria; worm infections causing blood loss
Increased risk of mortality and morbidity; impaired mental and physical growth and development
47%
Intermittent iron supplementation recommended where more than 20% of children under five or school-age children are iron deficient
Vitamin A Maintains good immune function, protects against illness such as measles and diarrhoea, required for eye function
High bio-available: Liver, fish, dairy and eggs Low bio-available: plant sources, such as orange-coloured fruits and vegetables
Inadequate intake of vitamin A
Increased risk of mortality and morbidity, night blindness, xerophthalmia, and permanent blindness
33%
A severe public health issue when more than 20% of the population have are vitamin A deficient
Iodine Required for thyroid function and to maintain metabolism for normal growth and development
Fish, bread; baked with iodised salt, eggs, dairy and breast milk; plant and animal sources from iodine-rich soil
Inadequate intake of iodine; inadequate iodine in the soil leading to inadequate iodine in food sources; not using iodised salt
Goitre; impaired thyroid function; cretinism; impaired growth and mental and physical development; increased risk of morbidity and mortality
285 million school aged children have insufficient iodine
More than 5 % of population have an enlarged thyroid gland or more than 20% of the population have urinary iodine concentration less than 50 μg/L
Further information Further information on micronutrients at risk of deficiency can be found at WHO: e-Library of Evidence for Nutrition Actions (eLENA) http://www.who.int/elena/nutrient/en





























