Embed Size (px)
DESCRIPTION
lung protective tools in servo i
Citation preview
POCKET GUIDE
LUNG RECRUITMENT CRITICAL CARE
3
3 Content 4 Ventilator-Induced Lung Injury (VILI) 7 Pressure Control Ventilation 8 Golden Moment: Late Inspiratoy Recruitment 9 The Open Lung Tool®
10 Open Lung Tool Parameters 11 Cursor Function 12 Zoom Function 13 Clinical Application of Cdyn i 13 Opening of collapsed airways and alveoli 14 PEEP titration 15 Evaluation of intervention 15 Monitoring 16 Clinical Application of VTCO2 17 Opening of collapsed airways and alveoli 17 PEEP titration 18 A Lung Recuitment maneuver 19 References
CONTENT
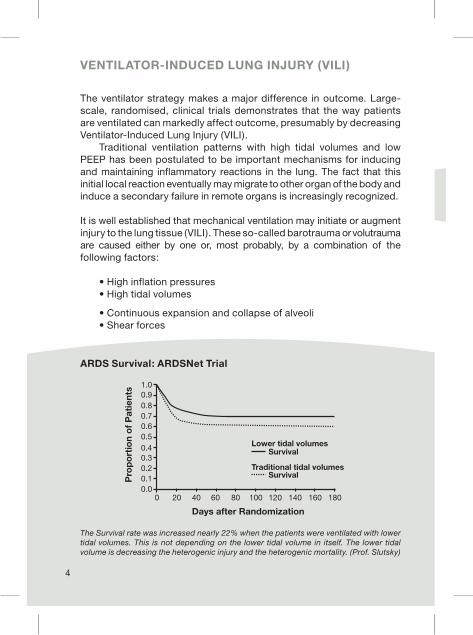
The ventilator strategy makes a major difference in outcome. Large-scale, randomised, clinical trials demonstrates that the way patients are ventilated can markedly affect outcome, presumably by decreasing Ventilator-Induced Lung Injury (VILI). Traditional ventilation patterns with high tidal volumes and low PEEP has been postulated to be important mechanisms for inducing and maintaining inflammatory reactions in the lung. The fact that this initial local reaction eventually may migrate to other organ of the body and induce a secondary failure in remote organs is increasingly recognized.
It is well established that mechanical ventilation may initiate or augment injury to the lung tissue (VILI). These so-called barotrauma or volutrauma are caused either by one or, most probably, by a combination of the following factors:
• High inflation pressures • High tidal volumes
• Continuous expansion and collapse of alveoli • Shear forces
VENTILATOR-INDUCED LUNG INJURY (VILI)
The Survival rate was increased nearly 22% when the patients were ventilated with lower tidal volumes. This is not depending on the lower tidal volume in itself. The lower tidal volume is decreasing the heterogenic injury and the heterogenic mortality. (Prof. Slutsky)
4
ARDS Survival: ARDSNet Trial

The inflammatory reaction induced by the mechanical insult on the lung, may further aggravate the injury by production of a multitude of pro-inflammatory substances. Migration of these inflammatory mediators to other organ systems may induce secondary organ dysfunction (biotrauma).
VILI
5
What Causes Ventilator Induced Lung Injury? • Volutrauma/ Barotrauma / Shear Force • Leaky Alveolar Capillary Membrane • Surfactant Deactivation • Cytokine and Mediator Release • “RACE” Repetitive Alveolar Collapse and Expansion
Mechanical Ventilation can lead to Biophysical injury • Shear force • Overdistention • Cyclic Stretch • Intrathoracic pressure
The hemodynamic consequences • Increased Alveolar-Capillary Permeability • Decreased Cardiac Output • Decreased Organ Perfusion
Biochemical Injury Pro-inflammatory mediators migrating to other organ systems through the sys-temic circulation may induce second-ary organ dysfunction and potentially increase mortality.

“Open up the lung and keep the lung open” from Professor Lachmann´s editorial (1) has been quoted many times. The Open lung is characterized by an optimal gas exchange (1). The intrapulmonary shunt is ideally less than 10%, which corresponds to a PaO2 of more than 450mmHg on pure oxygen (4-6) at the same time airway pressure are at the minimum to ensure the required gas exchange. Hemodynamic side effects are thus minimized (1,7).
Approaches to Lung Protective Ventilation • Recruitment Maneuvres • PEEP> Critical Closing Pressure (CCP) • Low tidal Volumes • Pressure Control Ventilation
Lung recruitment has gained widespread interest as a procedure for the opening of closed lung units. The widespread use of low tidal volumes may increase the risk of generation of atelectasis in the basal parts of the lung, which eventually may lead to consolidation of the affected areas. Further deterioration is caused by high inhaled oxygen concentrations resulting in reabsorbtion atelectasis. In certain patients, the use of a recruitment maneuvre may provide a long-term improvement in oxygenation. If proper PEEP level can be determined and set, the effect will stabilize and further protect the lung by avoiding cyclic opening and closing of lung units. It is important to choose a mode of ventilation that minimizes the stress of the lung tissue.
VILI
6

7
Pressure control ventilationPressure control ventilation is recommended, as in this mode of ventilation the ventilator delivers a flow that maintains the preset pressure during the preset inspiratory time. The pressure is constant during the inspiratory time and the flow is decelerating. If for any reason pressure tends to decrease during inspiration the flow from the ventilator will immediately increase to maintain the set inspiratory pressure. The Servo-i will sense the smallest deviations in pressure. If it appears that previously collapsed units of the lung are starting to open in the late phase of inspiration the pressure tends to decrease, this is compensated by a precise increase in flow and the alveoli are opened.
PRESSURE CONTROL VENTILATION

8
LATE INSPIRATORY RECRUITMENT
Golden Moment: Late Inspiratory RecruitmentTerminal airway resistance decreases in discrete steps when the pressure is applied. The behavior of lung opening is comparable to a multitude of pressure- and time-dependent avalanches. By immediately sensing the pressure drop induced by an opening avalanche, Servo-i provides proper flow to balance and further enhance the opening process.
A minute pressure drop induced by a fractional opening of closed airways is immediately sensed by Servo-i, resulting in a correspond-ing increase in inspiratory flow delivery. This promotes gas dis-tribution to potentially recruitable areas and gives a gentle opening of previously collapsed areas. A low sampling rate during this situation will result in a larger pressure drop with a resultant over-shoot in flow delivery. This may rip the airways open and give an immediate rebound by the then induced tissue stress in adjacent areas. Late Inspiratory Recruitment

9
The Open Lung Tool®
The Open Lung Tool is a real-time monitoring option that looks at the changes in Lung Mechanics during the clinical application of a recruitment strategy. The Open Lung Tool (OLT) can be used for graphical visualization of measured and calculated values for easier interpretation of patient response to user controlled lung recruitment procedures. The OLT can also be used as a breath-by-breath trend monitor of collected and stored parameter data.
Open Lung Tool (option)This tool is reached and displayed via the Quick access fixed key. However, data are collected continuously at all times when the Servo-i is in operation. Upon selection, the three graph windows are auto scaled vertically. The scaling can be set manually via Quick access/Open Lung Tool scales.
THE OPEN LUNG TOOL®

10
OPEN LUNG TOOL PARAMETERS
OLT parametersOLT allows for a graphical breath-by-breath observation of End Inspiratory Pressure and PEEP, inspired and expired tidal volumes, dynamic compliance and Tidal CO2 elimination. Please observe when the CO2 Analyzer Servo-i is installed and connected. Three synchronous graphical trend windows are presented with a fixed set of parameters as a function of collected breaths over time. This alternative presentation may be used for immediate visualization of the effect of altered ventilator settings.
The following parameters are presented:• In the upper window, measured End Inspiratory Pressure (EIP) and Positive End Expiratory Pressure (PEEP) presented, breath-by-breath.• In the middle window, measured Inspiratory tidal volume (VTi) and Expiratory tidal volume (VTe) presented, breath-by-breath.• In the lower window, calculated dynamic Compliance (Cdyn i) and Tidal CO2 elimination (VTCO2) presented breath-by-breath.
Cdyn i =
It should be noted that calculation of Cdyn i as shown above results in the compliance of the whole respiratory system. Calculation of lung compliance requires the recording of transpulmonary pressure. That is airway pressure minus oesophageal pressure.
VTiEIP-PEEP

11
Time displayed on the lower right hand area of the screen indicates remaining time at the current respiratory rate for the curve to fill the available screen space. Changing the scaling with the zoom in or out function will change the number of breaths needed for filling the available screen space.
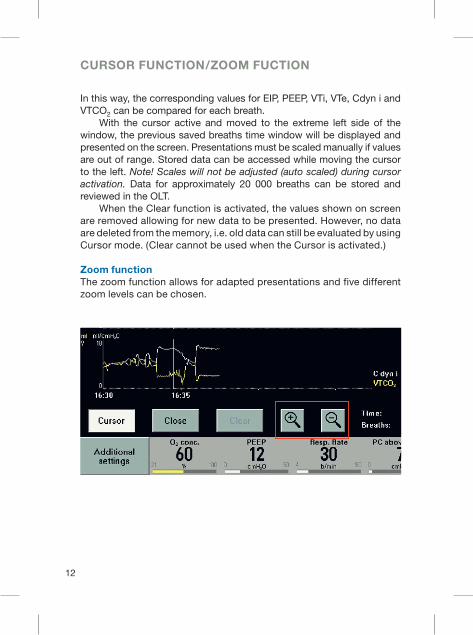
Cursor functionAn activated cursor can be moved with the Main Rotary Dial or via the soft keys. When moving it along the graph, the numeric parameter values valid for that particular moment will be shown at the right hand side of the graph.
CURSOR FUNCTION/ZOOM FUCTION
12
In this way, the corresponding values for EIP, PEEP, VTi, VTe, Cdyn i and VTCO2 can be compared for each breath. With the cursor active and moved to the extreme left side of the window, the previous saved breaths time window will be displayed and presented on the screen. Presentations must be scaled manually if values are out of range. Stored data can be accessed while moving the cursor to the left. Note! Scales will not be adjusted (auto scaled) during cursoractivation. Data for approximately 20 000 breaths can be stored and reviewed in the OLT. When the Clear function is activated, the values shown on screen are removed allowing for new data to be presented. However, no data are deleted from the memory, i.e. old data can still be evaluated by using Cursor mode. (Clear cannot be used when the Cursor is activated.)
Zoom functionThe zoom function allows for adapted presentations and five different zoom levels can be chosen.
CURSOR FUNCTION/ZOOM FUCTION

13
Clinical Application of Cdyn i
The Servo-i OLT provides a possibility to display and store patient/ventilator responses to a series of user-controlled patterns of changes in ventilator settings, typically applied during a lung recruitment procedure. The objective for such procedures is to open up airways and alveoli that currently are collapsed and to keep them aerated also throughout the expiratory part of the breath cycle.
Opening of collapsed airways and alveoliCurrently there are several different methods in clinical use to accom-plish an opening of collapsed alveoli and the common denominator for most of these methods is to intermittently apply an increased positive pressure in the lung for a limited time.
CLINICAL APPLICATION OF Cdyn i

14
CLINICAL APPLICATION OF Cdyn i
The graphical display of Cdyn i will indicate the response of the patients’ lung mechanics to each change in applied airway pressure and inspiratory tidal volume. For example, during a stepwise increase of the EIP a corresponding increase in tidal volume will occur.
As long as the relative increase in EIP and tidal volume are linear the Cdyn i will appear constant, reflecting the development of the pressure/volume relation in the lung over time. With a continued stepwise increase in EIP there will eventually be a slightly less increase in the corresponding tidal volume, which is indicated by a slight decrease in Cdyn i. Additional increase in EIP at this point may result in a gradually smaller increase in tidal volume accompanied by a decrease in Cdyn i. This pattern may illustrate that the relative frequency of opening of collapsed alveoli is reduced relative to increase in pressure and that further increase in EIP may result in overdistension of already opened alveoli.
PEEP titrationCdyn i may also be used to find the level of PEEP which prevents alveo-lar collapse during expiration (Critical Closing Pressure). Used for this purpose it may help guiding the titration of effective PEEP. This may be performed by a stepwise decrease of an initial high PEEP level, which should be assessed before the recruitment maneuvre is being per-formed. As PEEP is stepwise decreased, the Cdyn i will initially increase with each drop of the PEEP level indicating a relief of over distended areas in the lung. Subsequently the Cdyn i will reach a plateau where Cdyn i no longer increases when the PEEP level is decreased. After further decrease in the PEEP level, the Cdyn i will start decreasing indicating initial collapse of alveoli that no longer can be kept open at the current PEEP level.
The cursor may be used to help identify the maximum level of Cdyn i, and its corresponding PEEP level may be used as a reference for the closing airway pressure. Effective PEEP should be set 2-3 cmH2O above the indicated collapse pressure as a safety margin after a preceding recruitment maneuvre.

15
CLINICAL APPLICATION OF Cdyn i
Evaluation of interventionCdyn i may also be a good indicator of an intervention. An assessment of the relative improvement of Cdyn i, may be done by comparing the value before and after the intervention.
MonitoringThe breath-by-breath registration and storage of Cdyn i in the OLT will allow for a continuous monitoring, which with the help of the cursor can be reviewed and evaluated as an indicator of changes in the lung mechanics. A declining Cdyn i over time can be correlated to an ongoing process of alveolar collapse. In cases when a significant drop in Cdyn i can be observed, the need for a re-recruitment should be assessed.
Effect of a recruitment maneuver. Note the lack of effect with a step-wise increase in PEEP without the recruitment maneuver. Slide kindly provided by Fernando Sipman-Suarez: Alveolar and Airway Collapse. Preventive measures by best PEEP titration. Symposium: Iatrogenesis of mechanical ventilation: How to prevent it. Sydney, October 2001.

16
CLINICAL APPLICATION OF VTCO2
Clinical application of VTCO2The CO2 concentration in expired air depends mainly on alveolar ventilation, cardiac output and the metabolic state. A large difference between arterial and end-expiratory (end-tidal) CO2 can be caused by an alveolar dead space, as can be seen, for example, with a pulmonary embolus. Shunt and V/Q-mismatch impede CO2 elimination only to a minor degree and can be disregarded in this context (very large shunts transmit mixed venous blood to the arterial side, slightly raising arterial CO2). The elimination of CO2 via expired gas during normal conditions can be calculated from the Brody´s formula, which predicts CO2 production during resting condition:
VCO2 (elimination/minute) = V/Qx10xBW0.75
Using this formula for a person weighing 70 kg will give VCO2 elimination of approximately 200ml CO2/min. VTCO2 can be calculated by dividing VCO2 with the respiratory rate. In the OLT, VTCO2 is calculated by a direct integration of measured CO2 concentration over measured expiratory flow on a breath-by-breath basis. (See equations under OLT parameters above.)

17
Opening of collapsed airways and alveoliWhen a stepwise increase of EIP is applied to a collapsed lung, the VTCO2 will increase with each pressure step due to increased ventilation of already opened alveoli and recruitment of collapsed areas allowing for additional diffusion of CO2 from the blood into the alveolar space. With a continued stepwise increase of EIP, VTCO2 will keep increasing until a point when no additional alveoli may be possible to open without impeding circulation. Already opened alveoli could also be over distended at this point, resulting in an increase in the ventilation/perfusion ratio. At this point diffusion of CO2 into the alveoli will start decreasing, which primarily may be indicated as a drop in VTCO2 and by a fall in pulmonary blood flow with subsequent fall in systemic arterial blood pressure.
PEEP titrationVTCO2 will follow a similar pattern as described for the Cdyn i above, when the same technique for PEEP titration (see above) is applied.
CLINICAL APPLICATION OF VTCO2

A LUNG RECRUITMENT MANEUVRE
Corresponding Lung Recruitment Maneuvre shown in the ordinary OLT window: (See corresponding red circles from left to right in the picture)
1 The initial situation, with limited ventilated area within the lungs
2 The increased EIP, opens up closed compartments. VTCO2 (tidal elimination) increases, as previously unventilated compartments now take part in the gas exchange.
3 VTCO2 reaches a plateau as no additional alveoli opens up.
4 PEEP is slowly decreased, step-by-step to identify the maximum value of Cdyn i as a breaking point, where lung compartments may start to close again. Collapse pressure is identified as the corresponding plateau/max value of Cdyn i and VTCO2.
5 The lung is re-recruited at initially used opening pressure.
6 PEEP is set 2 cmH2O above the collapse pressure. The CO2 tidal elimination and Cdyn i were used here for evaluation and identification of the different phases in the maneuvre.
18

1. Lachmann B. Open up the lung and keep the lung open. Intensive Care Med 1992; 118: 319-321.
2. Lichtwarck-Aschoff M, Nielsen JB, Sjöstrand UH, Edgren E. An experimental randomized study of five different ventilatory modes in a piglet model of severe respira-tory distress. Intensive Care Med 1992;18: 339-347.
3. Sjöstrand UH, Lichtwarck-Aschoff M, Nielsen JB, et al. Different ventilatory ap-proaches to keep the lung open. Intensive Care Med 1995; 21:310-8.
4. Kesecioglu J, Tibboel D, Lachmann B. Advantages and rationale for pressure control ventilation. In: Vincent JL (ed) Yearbook of intensive care and emergency medicine. Springer-Verlag; Berlin; Heidelberg, New York, 1994; 524-533.
5. Lachmann B, Danzmann E, Haendly B, Jonson B. Ventilator settings and gas exchange in respiratory distress syndrome. In: Prakash O (ed) Applied physiology in clinical respiratory care. Nijhoff, The Hague 1982; 141-176.
6. Tusman G et al. Alveolar recruitment strategy improves arterial oxygenation during general anesthesia. Br J Anaesth 1999; 8-13.
7. Tusman G et al. Alveolar recruitment strategy increases arterial oxygenation during one-lung ventilation. Annals of Thorac Surg 2002; 73: 1204-9.
8. Tusman G et al. Effects of recruitment maneuver on atelectasis in anesthetized chil-dren. Anesthesiology Jan 2003; 98(1): 14-22.
9. Suárez Sipmann F et al. Clinical experience from the open lung clinical trial in Spain. Jour-nal für Anästhesie und Intensivbehandlung 1998;1.Quartal:183-6.
10. Rimensberger PC, Pache JC, McKerlie C,Frndova H, Cox PN.Lung recruitment and lung volume mainte-nance: a strategy for improving oxygenation and preventing lung injury during both
conventional mechanical ventilation and high-frequency oscillation.Intensive Care Med.2000 Jun; 26(6):745-55.
11. Amato MB. Barbas CS, Medeiros MD, et al. Beneficial effects of the ”open lung approach” with low distending pressures in acute respiratory distress syndrome. A prospective randomized study on mechanical ventilation. Am J Respir Crit Care Med 1995; 152: 1835-46.
12. Amato MB. Barbas CS, Medeiros MD, et al. Effect of a protective-ventilatory strategy on mortality in the acute respiratory distress syndrome. N Engl J Med 1998; 338: 347-54.
13. Marini J J, Gattinoni L. Ventilatory management of acute respiratory distress syndrome: A consensus of two. Crit Care Med.2004 Vol.32, No1
Scientific Presentations and publications
14. Lung recruitment in patients with ARDS/ALI.Art. No: 65 88 888 E315E
15. Ventilator associated treatment and moni-toring of pediatric and neonatal cardiopulmo-nary disease. Art. No: 64 41 989 E315E
16. Iatrogenesis of Mechanical Ventilation: How to prevent it?Art. No: 65 88 367 E315E
17. Mechanical Ventilation in Anesthesia & Intensive Care. Art. No: 65 88 433 E315E
18. Biotrauma – A primer on ventilator-in-duced inflammatory reaction. Art. No: 65 88 938 E315E
18. Lung Recruitment PEEP and VT in ARDS. Art. No: 66 48 864 E315E
19. Mechanical Ventilation.Art. No: 66 48 872 E315E
20. CD collection box.Art. No: 65 88 862 E315E
REFERENCES
19

Maquet Critical Care ABSE-171 95 SOLNASwedenPhone: +46 8 730 73 00www.maquet.com/criticalcare
© Maquet Critical Care AB 2004. All rights reserved.
MAQUET reserves the right to modify the design and specifications contained herein without prior notice.
Order No. 66 61 271Printed in Sweden1104 10.Rev.01 English Price: Group 1