Embed Size (px)
Citation preview

Scientificreport2013-2015
1
Intermediatesyntheticscientificreport
RegardingtheimplementationoftheprojectfromSeptember2013toDecember2015
Projectcode:PN-II-ID-PCE-2012-4-0067
Project title: In silico modelling of biological processes in hypoxic tumourstowardsanindividualizedtreatmentprotocol
I. ObjectivessetforSeptember2013–December2014timeperiod
Oct2013–Dec2013
The major objective: Growth of a virtual head and neck tumour using Monte Carlocomputationaltechniquesbasedonbiologicallyrealisticparameters.Plannedactivitiestoachievetheobjective:1. Tocollatetherequiredbiologicaldatabasedontheexistentscientificliteratureto
serveasinputparametersforthevirtualtumourgrowthmodel.2. Tobuildthemodelbasedontheinputparameters.Expectedresult:Abasicvirtualtumourrepresentativeforheadandneckcancers(resultdissemination:conferencepresentation).
Jan2014–Dec2014
Objective1.ModeladjustmentusingspatialcomponentscorrelatedwithPET/CTdata.Plannedactivitiestoachievetheobjective:
1.1. ToincorporatePET/CTdatainacomplexparametertodefinethespatialdistributionoftumourhypoxia.
1.2. To adjust the basicmodel’s input parameters as a function of patient-basedhypoxicandmetabolicfactors.
The expected result for this phase of the project: A complex head and neck tumourmodelbasedonrealimagingdata.
Objective2.Radiotherapysimulationofrealtreatmentschedules.
Plannedactivitiestoachievetheobjective:
1.1. To implement the mechanisms that are responsible for tumourrepopulationduringradiotherapy.
1.2. To simulate real treatment protocols using the linear quadraticformalismoffractionatedradiotherapy.
The expected result for this phase of the project: Results of radiotherapy treatmentsimulation(resultdissemination:conferencepresentation,ISIarticlepublication).

Scientificreport2013-2015
2
Jan2015–Dec2015
Objective1.Modeladjustmentaccordingtoclinicalresults.Plannedactivitiestoachievetheobjective:
1.1. Tocompareclinicaldatawithsimulationdataconsideringtumoursize,distributionofhypoxiaandmetabolicbehaviour.
1.2. Radiotherapymoduleadjustment.
Objective2.Modelvalidation.Plannedactivitiestoachievetheobjective:
1.1. Torecruita largernumberofpatientswithheadandnecktumoursforPET/CTimagedatacollection.
Theexpectedresultforthisphaseoftheproject:Optimisedmodelbasedonclinicaldata(resultdissemination:conferencepresentation,ISIarticlepublication).
II. ResearchresultsfromOctober2013toDecember2014
II.1.ArticlespublishedinISIjournals
1. L.Marcu,ThefirstRsofradiotherapy-orstandingontheshouldersofgiantsAustralasianPhysEngSciMed,38(4)(2015)(IF=0.882)(invitedarticle)
2. M.Jennings,L.Marcu,E.Bezak,PET-specificparametersandradiotracersintheoreticaltumourmodellingComputationalandMathematicalMethodsinMedicineArticleID415923(2015)(IF=1,08)
3. L. Marcu,W.Harriss-Phillips, S. Filip,Hypoxia inheadandneckcancer in theoryandpractice:aPET-basedimagingapproachComputationalandMathematicalMethodsinMedicine,ArticleID624642(2014)(IF=1,08)
4. L. Marcu, Tumour repopulation and the role of abortive division in squamous cellcarcinomasduringchemotherapyCellProliferation47(4):318-325(2014)(IF=3,28)
5. L. Marcu, Improving therapeutic ratio in head and neck cancer with adjuvant andcisplatin-basedtreatmentsBiomedResearchInternational2013:817279(2013)(IF=2.880)
II.2.PublicationsindexedinInternationalDatabases
1. L.Marcu,D.Marcu,S.Filip,Insilicorepopulationmodelofvarioustumourcellsduringtreatmentbreaksinheadandneckcancerradiotherapy

Scientificreport2013-2015
3
WorldAcademyofScience,EngineeringandTechnology, InternationalScience Index,MedicineandHealthSciences9(3)(2015)
II.3.Internationalconferencepresentations
1. L. Marcu, D. Marcu, In silico evaluation of radiobiological hypoxia and its effect ontumourcontrolduringradiotherapyProceedingsofthe39thARACongress,Frascati,Rome,Italy,28-31July(2015)
2. L.Marcu,D.Marcu,S.Filip,CancerstemcellsinahierarchicalmodeloftumourregrowthinfiveheadandneckcarcinomasWorldCongressonMedicalPhysics&BiomedicalEngineering,Toronto,Canada,7-12June(2015)
3. L.Marcu,Medicalphysics–orhowachangeincareerpathbecomesapassion
WorldCongressonMedicalPhysics&BiomedicalEngineering,Toronto,Canada,7-12June(2015)
4. L.Marcu,Theimpactofcancerstemcells(CSCs)onradiotherapyoutcome:aninsilicoapproachACPESMWABranchMeeting,Perth,Australia,17-22May(2015)(Invitedtalk)
5. L.Marcu,D.Marcu,MonteCarlosimulationofpersonalisedradiotherapyforheadandneckcancerdrivenbytumourgrowthkineticsICRR2015,The15thInternationalCongressofRadiationResearch,Kyoto,Japan,25-29May(2015)
6. L.Marcu,D.Marcu,S.Filip,InsilicorepopulationmodelofvarioustumourcellsduringtreatmentbreaksinheadandneckcancerradiotherapyIEEE,InternationalConferenceonRadiationMedicine,Dubai,UAE,11-12March(2015)
7. D.Marcu,L.Marcu,InsilicogrowthofahypoxicheadandnecktumourincludingangiogenicprocessesThe60thAnnualMeetingoftheRadiationResearchSociety,LasVegas,21-24Sept(2014)
8. L.Marcu,TheinfluenceofrepopulationmechanismsontreatmentgaptiminginheadandneckcancerradiotherapyWorkshop:Biologicalbasisofradiotherapy–wheredowestand?Stockholm,4-5Sept(2014)
9. L.Marcu,D.Marcu,InsilicosimulationoftumourradiobiologytowardsindividualisedtreatmentThe3rdInternationalCongressonPersonalisedMedicine(UPCP),Prague,26-29June(2014)
10. L.Marcu,Theeffectofabortivedivisionasarepopulationmechanismonheadandneckcancerradiotherapy

Scientificreport2013-2015
4
ESTRO33,Vienna,Austria,4-8April(2014)
11. L. Marcu, D. Marcu, S. Filip, O. Straciuc, The implementation of tumour-specificradiobiologicalparametersinahead&necktumourgrowthmodel,InternationalConferenceonSciences,BăileFelix,8-9November(2013)
12. O. Straciuc, C. Oncu, Zs. Lengyel, Modern diagnostic imaging of prostate cancer,
International Conference on Urology, Gynaecology and Urogynaecology UroGyn,Oradea14-17November(2013)
II.4.Nationalconferencepresentations
1. A.Dinu,O.Straciuc,FDG-PETasanimagingbiomarkerinheadandneckcarcinomasThe2ndNationalCongressonMedicalOncologyandRadiotherapy,Sinaia,23-25Oct(2014)
2. O.Straciuc,C.Oncu,Themoderndiagnosticimagingofcancer,Ar-MedicaConference,Arad,2-4November(2013)
II.5.Books/bookchaptersandspecialissuejournals
1. L.Marcu(editor),ContemporaryIssuesinHeadandNeckCancerManagementInTechPublishing,ISBN:978-953-51-2135-0(2015)
2. L. Marcu, E. Bezak, I. Toma-Dasu, A. Dasu (editors), Predictive Models Of TumourResponseToTreatmentUsingFunctionalImagingTechniques(Specialissuejournal)ComputationalandMathematicalMethodsinMedicine,ISSN:1748-670X(2015)
3. L.Marcu, I.Toma-Dasu,A.Dasu,The6Rsofheadandneckcancerradiotherapy(book
chapter)In:ed. L.Marcu,Contemporary issues inheadandneckcancermanagement, InTechPubl.,ISBN978-953-51-2135-0(2015)
II.6.Submittedarticles
1. L. Marcu, Futuretreatmentdirections forHPV-associatedheadandneckcancerbasedonradiobiologicalrationaleandcurrentclinicalevidenceCriticalReviewsinOncology/Hematology(2015)(submitted)
2. R.Chirla, L.Marcu,PET-basedquantificationofstatisticalpropertiesofhypoxictumorsubvolumesinheadandneckcancerPhysicaMedica(2015)(submitted)
3. L.Marcu,D.Marcu,S.Filip,Cancerstemcelldynamicsandradiobiologicalhypoxiawith
treatmentimplicationsinaheadandnecktumourmodelCellProliferation(inpreparation)

Scientificreport2013-2015
5
II.7. MSc thesis, University of Oradea, The Physics of Biomedical Explorations andTherapies(July2014)
Thesistitle:FDG-biomarkerinthediagnosticimagingofheadandneckcancerMasterstudent:AncuțaDinuScientificcoordinators:Prof.dr.LoredanaMarcu&A/Prof.dr.OresteStraciuc

Scientificreport2013-2015
6
III. Scientificachievements
Oct2013–Dec2013Theaimofthecurrentprojectistodevelopacomplexvirtualheadandnecktumourandtosimulatetheeffectofradiotherapyonthistumourbasedoninternationalprotocolsandtrialsdesigned for the management of advanced head and neck carcinomas. In our previousresearch we have developed a virtual tumour that encompassed several biological andradiobiological parameters that are specific for head and neck tumour growth anddevelopment.However,certainimportantprocesseshavenotbeenpreviouslyincludedinthebasic model, therefore the goal of the current project is to incorporate the majorradiobiologicalfactorsthatinfluencetumourresponsetoionizingradiation.Thiswillenabletheevaluationofradiotherapyanditseffectsonthevirtualheadandnecktumour.Cellular repopulation and tumour hypoxia are the key factors regarding tumour behaviourduring radiotherapy. Therefore, tumour repopulationmechanismsmust be incorporated inthebasicmodelinordertoanalysetumourevolutionduringtreatment.Animportantelementthatwasevaluatedatthisstagewasathoroughliteraturereviewregardingallrepopulationmechanismsspecificforheadandnecksquamouscellcarcinomas.Thefollowingrepopulationmechanismshavebeenidentifiedsofar,eitherexperimentallyorsemi-empirically:cellrecruitment,abortivedivision,accelerateddivisionofstemcellsandthelossofasymmetricaldivisionof stemcells (Withers1993,Dörr1997) (table1presents thedefinitionsoftherepopulationmechanisms).Table1.Repopulationmechanismsandtheireffectondifferentcelltypes
Repopulationmechanism
Effect/definition Typeofcellsaffected
Cellrecruitment Recyclingthequiescentcellsintothecellcycle
Quiescentcells
Acceleratedrepopulation
Shorteningofcellcycletime Proliferatingstemcells
Lossofasymmetricaldivision
Symmetricaldivisionofstemcellsinmitosis(i.e.twodaughterstemcells)
Proliferatingstemcells
Abortivedivision Limitednumberofproliferationsafterwhichthecellbecomessterile
Proliferatingdifferentiatedcells(finitelyproliferatingcellsordoomedcells)
In this phase of the project we have simulated the repopulation mechanisms duringradiotherapywith special focuson the least studiedmechanism in the literature–abortive

Scientificreport2013-2015
7
division of differentiated cells and the interplay between this mechanism and the othertumourrepopulationprocesses.Acceleratedstemdivisionandabortivedivisionarecontrolledbytissuehypoplasiawhereasthemechanismofasymmetrylossisdictatedbystemcelldepletion(Dörr2003).Cell recruitment is,perhaps, themostnatural repopulationmechanismdue to theavailablepool of quiescent cells in the G0 phase, which, under certain triggers such asradio/chemotherapy, can re-enter the cell cycle and restart proliferating. Despite thecommonnessofthismechanism,thereisveryfewquantitativedataintheliteratureregardingthe percentage and types of cells recruited during treatment and their effect on tumourcontrol.Tubiana(Tubiana1988)hasshownthatinanuntreatedtumourpopulationofhaemopoieticcells,theproportionofrecycledstemcellsisbelow2%ofthetotalnumberofcells.Giventhattheproliferativerateofhaematologicalcancersisgreaterthanthatofsolidmalignancies,thelimitof2%ofstemcellsrecruitedcouldrepresenttheupperlimitinthecaseofsolidcancers.Some insilicomodellingworkanalysingtheimpactofcellularrecruitmentonsolidtumourshasbeendoneinthepastbytheprojectdirector(Marcu2004).Itwasalsoshownthatinheadandneckcarcinoma, thismechanismis lesspowerful thanacceleratedrepopulationofstemcells or the loss of asymmetrical division of stem cells, irrespective of the number of cellsinvolvedinthere-cyclingprocess.In radiotherapy, the effect of accelerated repopulation and loss of asymmetrical division ofstemcellscanbeannihilatedbyincreasingtheradiationdose(Dörr2009).Abortivedivisioncan interact with the clinical outcome by counterbalancing the continuous cell loss due totreatment. Therefore a quantitative analysis in this directionwould be useful to assess theimpactofthismechanismontreatment-inducedoveralltumourregrowth.Todate,thereisnoquantitativedataintheliteratureregardingtheroleofabortivedivisioninradiotherapy,onlyonthosemechanismsthatarelinkedtostemcellrepopulation(Trott1999,Marcu2004,Marcu2010,Harriss-Phillips2011).Toassesstheroleofabortivedivision,an insilicomodelofaheadandneckcarcinomawasbuilt,withbiologicallyrealisticparameters,whichservesasabackgroundforthesimulationof tumour repopulation during radiotherapy. The three cell types studied in themodel arestem,finitelyproliferatingandnonproliferatingcells.Finitelyproliferatingcellsdivideoverafinitenumberofgenerations,aprocessknownasabortivedivision.Inordertogrowavirtualtumourwithsimilarbiologicalpropertiesofarealtumour,cancergrowthmustbeguidedbywell-definedkineticparameters,suchas:cellcycletime, the lengthofeachphaseof thecellcycle, growth rate, volume doubling time and also the percentage of each cell type whichdictates tumour composition. A study has been undertaken to determine the maximumnumberofdivisionsaproliferativecellcanundergowithoutalteringtumourkinetics.Themodelshowedthatthemaximumnumberofabortivedivisionstoleadtorealisticvolumedoublingtimes(i.e.anaverageof45days-characteristictoheadandnecktumours)is3,aslargernumberswouldresultinveryshortdoublingtimes.

Scientificreport2013-2015
8
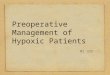
Figure1.Thenumberoftumourcellsasafunctionofthenumberoffinitelyproliferatingcellgenerations.Another observation indicates that the proliferative/stem (P/S) ratio increases with thelength of stem cycle time (supra-linear increase), meaning that repopulation via abortivedivision overcomes the one caused by stem cells (figure 2). On the other hand, for shortmitoticcycles(upto10h)theP/Sratiodecreasesovertreatmenttimewithupto12%,whichindicatesadropinabortivedivisionduringtreatmentascomparedtostemcellrepopulation.However,whenthecellcycletimehasanaveragevalueof33h(i.e.theaverageheadandneckcellcycletime)theP/Sratioisnearlyconstantthroughoutthetreatment(figure2).
Figure2.Theratioofproliferativeversusstemcells(P/S)asafunctionofstemcellcycletime.
Wehaveshownthatbesidestemcell-relatedrepopulationmechanisms,abortivedivisionoffinitelyproliferatingcells(ordoomedcells)contributestocellproductionwithinthetumourduringradiotherapy.The P/S ratio is strongly dependent on the stem cell cycle time suggesting that there is asynergisticeffectbetweenacceleratedrepopulationandabortivedivisionofcancercells.
1.E+01
1.E+03
1.E+05
1.E+07
1.E+09
1.E+11
1.E+13
0 1 2 3 4 5 6
Noofcells
Noofgenerations

Scientificreport2013-2015
9
This first phase of the project has lead to important research results regarding therelationship between various repopulationmechanisms that are specific to head and neckcancers,givingalsoaninsightonthepotentialeffectofrepopulationduringradiotherapyontumour control. In the next phasewe are continuing the simulation of tumour growth andresponsetotreatmentbystudyingthesecondmajorradiobiologicalparameterthatinfluencestreatmentoutcome,namelytumourhypoxia.Jan2014–Dec2014Inthissecondphaseoftheprojectwestudiedtheavasculartumourresponsetotheeffectofradiationwithandwithoutchemotherapy,followedbytheimplementationofhypoxia-relatedparameters,which further onwill enable the evaluation of a vascular and hypoxic tumourduringirradiation.
A. Therepopulationmechanisms thathavebeen identifiedso far,eitherexperimentallyorsemi-empiricallyarethefollowing:cellrecruitment,abortivedivision,accelerateddivisionofstemcellsandthe lossofasymmetricaldivisionofstemcells(Withers1993,Dörr1997).Acceleratedstemdivisionandabortivedivisionarecontrolledbytissuehypoplasiawhereasthemechanismofasymmetrylossisdictatedbystemcelldepletion(Dörr2003).In radiotherapy, the effect of accelerated repopulation and loss of asymmetrical division ofstemcellscanbeannihilatedbyincreasingtheradiationdose(Dörr2009).Abortivedivisioncan interact with the clinical outcome by counterbalancing the continuous cell loss due totreatment. Therefore a quantitative analysis in this directionwould be useful to assess theimpactofthismechanismontreatment-inducedoveralltumourregrowth.Until the startof thisproject, therewasnodata in the literature regarding the influenceofabortivedivisionontumourbehaviourduringtreatment,onlyonthosemechanismsthatarelinkedtostemcellrepopulation(Trott1999,Marcu2004,Marcu2010,Harriss-Phillips2011),reason why this type of repopulation (i.e. abortive division) has been comprehensivelystudied and the results published in the ISI journal Cell Proliferation (Marcu 2014a) andpresentedattheinternationalconferenceESTRO33,Vienna,2014.Therepopulationmechanismshaveamajorimpactontumourresponsetoradiotherapyandchemotherapy.Therefore,thenextstepwastostudytheeffectofrepopulationontreatmentgapsduringradiotherapy.Plannedtreatmentgaps(orbreaks)occurduringaggressiveheadand neck cancer treatment schedules to allow the surrounding normal tissue to repair thesublethaldamageandtoregrow/repopulatethetissuefromthesurvivingcells.Usingthelinearquadraticformalismofcellsurvival:
𝑆 = 𝑒! !"!!!! ,whereSrepresentsthesurvivingfraction,Drepresentsthetotaldoseofradiation,andαandβaretumour-specificcoefficientsthatcharacterisetissueradioresistance,wehavesimulatedalteredfractionation(non-standard)schedulesonthevirtualtumourbasedontheRTOGtrial(RadiationTherapyandOncologyGroup):1.6Gy/fraction,twiceaday,6hoursapart,5daysaweek, and a total of 42 dose fractions. Three different timings for treatment interruptionshave been simulated using the Linear Quadratic model: after 20, 24 and 28 fractions,respectively.Bothstemanddifferentiatedcellshavebeenmonitoredandtheircontributiontowards tumour growth analysed (results presented at theWorkshop: Biological basis of

Scientificreport2013-2015
10
radiotherapy –where dowe stand? Stockholm, 2014). Due to the activation of repopulationmechanismsduringradiotherapy,thereisalargeincreaseinthepercentageofstem(%S)andalso differentiated cells (%P) that contribute to tumour development. While beforeradiotherapy the tumour consisted of 6% stem cells and 10% differentiated cells, duringaccelerated radiotherapy, both percentages increased drastically, depending also on thetimingof treatmentbreaks.Therefore, theaveragepercentofstemcellsvaried from41.3%(breakafter20 fractions) to36.6%(breakafter28 fractions),while theaveragepercentofdifferentiated cells varied from 30.5% (break after 20 fractions) to 33.7% (break after 28fractions) (figure1).An interestingobservation is the fact that thepercentageof stemcellsdecreaseswiththedelayoftreatmentgap.Thisisbecauseearlybreaks(after20fractions)donot allow sufficient cell kill among the continuously proliferating stem cells to control thetumour.Thebehaviourofdifferentiatedcells is justtheopposite,tokeepaconstantcellkillalongthetreatment.
Figure1.Theinfluenceoftreatmentgaptimingonpercentageofcelltype. The model has shown that not only stem cells but also differentiated cells, via abortivedivision, can contribute to malignant cell repopulation during treatment. This is observedfromthesurvivingfractionsillustratedinfigure2.Themaindifferencebetweenthetwocelltypesisthefactthatdifferentiatedcellsundergoingabortivedivisionare ‘doomed’cellsas theyeventuallyceasecreatingnewcellsanddieout,whilestemcellsareabletoregrowthetumour,evenfromonesinglecell.Asaconsequence,fortheireradicationthereisneedforfineadjustmentsoftreatmentparametersthattakeintoaccounttheacceleratedrepopulationofheadandneckcarcinomacells.
20
25
30
35
40
45
50
After20fx After24fx After28fx
Percentageofcells
Timingoftreatmentgap
%S %P

Scientificreport2013-2015
11
Figure2. Surviving curves of stemanddifferentiated cells under acceleratedRTwith treatment gap after 20fractions.
B. The in silico grown head and neck tumour (figures 3 and 3a) has been furtherdeveloped by including in the model those parameters that are related to hypoxia status(Marcu 2014b), represented by pO2 (partial oxygen tension), the oxygen gradient and thediffusion distance from the capillary to the cell. Themain tumour characteristics and theircorrespondingvaluesappliedtothevirtuallygrownhypoxictumourarepresentedintable1.Figure4isaflowchartofhypoxictumourdevelopment.
Figure3.Spatialdevelopmentofthevirtualtumourinthevicinityofabloodvessel.
Figure3a.Enlargedimageofatumoursection,wherestemcellsarerepresentedwithred,differentiatedcellswithgreenandwithorangethequiescentcells.
Inordertomodelthespatialdevelopmentofthetumour,endothelialcellshavebeenincludedaswell, thatarestimulatedby the lackofoxygentostart theangiogenicprocesswithin thetumour (results presented atThe60thAnnualMeetingof theRadiationResearchSociety,LasVegas,Sept.2014).
1.E+00
1.E+01
1.E+02
1.E+03
1.E+04
0 5 10 15 20 25 30 35 40 45
Num
berofcells
Treatmenttime(days)
Stemcells Differentiatedcells

Scientificreport2013-2015
12
Table1.Insilicoheadandneckcancerproperties
Property/Characteristics
Quantification(inaccordancewithliterature)
Cellularcomposition(qualitative)
Tumourcells Stem
DifferentiatedtumourQuiescent
Vascularcells Endothelial
Cellularcomposition(quantitative)
Tumourcells 2.6%stem
12%differentiated85.4%quiescent
Tumourcellkinetics
Meancellcycletime 33hours
Cellcycletimevariation ±10%ofmeancycletimeLength of various cellcyclephases
M(7%),G1(40%),S(30%),G2(23%)
Volumedoublingtime 53daysCelllossfactor 85%
Tumouroxygenation pO2 From20%(nexttobloodvessel)to0.3%
Figure4.Flowchartofhypoxictumourdevelopment

Scientificreport2013-2015
13
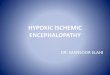
PET/CTimagingplaysacrucialrole inthemanagementofheadandneckcancerduetotheinformation that are supplied regarding malignant status and the aggressiveness of thetumour which very often is correlated with the oxygen content. In order to obtain suchdetails,forty(40)patientsdiagnosedatthePETDiagnosztikaCentre,Oradea,withmalignantlesionsoftheheadandneckareahavebeenstudiedandanalysed.PETimageassessmenthasshownthatmajorityofthediagnosedheadandneckcancersarelocallyadvanced(65%). Animportant parameter that has been investigated is SUV (Standardised Uptake Value). Thisquantity (SUV) is not equivalent with the CT-given radiodensity expressed with theHounsfield units. The quantity of the FDG (fluoro-deoxyglucose) that is uptaken by thetumour following the injection of the radiopharmaceutical strongly depends on theindividual’sglucosemetabolism,which,ontheotherhand,dictatesthechangesinSUV.ThisFDG-PET specific parameter is a biophysical index that offers information about theaggressivityoftumoursandtheirmetabolicactivity.Thisisalsoillustratedinfigure5,wheretheevolutionoftumoralSUVduringsuccessiveexaminations(4examinations)ofaheadandneckcancerpatienttreatedwithradio-andchemotherapyisrepresented.TheelevatedSUVvalues,which showed a continuously growing trend, illustrate the aggressive nature of thetumouranditsresistancetoradio-andchemotherapy.Suchtumoralbehaviourisoftenlinkedto the hypoxic status that hinders the efficacy of radiotherapy due the radioresistance ofhypoxiccellsandtheeffectivenessofchemotherapyduetopooragentperfusion.FDGcanbe,therefore,consideredaninvivobiomarkeroftumourproliferation.
Figure5.TheevolutionoftumoralSUVduringsuccessiveexaminationsofaheadandneckcancerpatienttreatedwithradio-andchemotherapy.
The high SUV values among patientswith radioresistant tumours also explain the effect oftumourhypoxiaonglucosemetabolism.Thisobservationisinaccordancewiththeresultsofclinical studiesreported in the literature,whichshowed thathypoxic tumours tend tohavehighSUVvalues(>9)(Zimny2006).Headandneckcarcinomasareoftenhypoxicandtheypresent,besidechronicallyhypoxicregions,areaswithacutehypoxiathatareduetotemporalblockage of tumour blood capillaries (Marcu 2014b). These blood vessels have abnormal-lookingshapesandstructures,andarandomdistributionwithinthetumourthatisgivenbythespatio-temporal instabilityofacutelyhypoxicregions.Takenthese intoaccount,cellularoxygenationwithintheinsilicomodeldependsonthedistancetotheclosestcapillaryandthepO2gradientstimulates theendothelial cells tocreatenewbloodvessels in thedirectionofthehypoxicregions.Duetocellkineticsandmovementwithinthetumour,thenewlyformedbloodvesselscanbeoccluded,momentwhenthatparticularareabecomesacutelyhypoxic.This hypoxic virtual tumour will serve, in the next phase of the project, as a model forradiotherapysimulation.Thedifferencesintumourcontrolbetweenoxygenatedandhypoxictumourswillalsobeanalysedinthetextphase.
0
5
10
15
0 1 2 3 4 5
SUV
NumberofPETexaminations

Scientificreport2013-2015
14
Jan2015–Dec2015Themajorobjectiveofthisprojectistheinsilicogrowthofavirtualheadandnecktumouraswell as the simulation of its response to radiation therapy. In order to simulate treatmentresponse there is need for the implementation of repopulation mechanisms that lead toacceleratedregrowthduringtreatmentandalsooftumouroxygenationstatus,twoimportantfactorsthatcanchangetheeffectofradiationonthetumour. The twokey factors– cellular repopulationandhypoxia,havebeen the focusof thisresearchandmodelling.Therefore,theevolutionoftheprojectfollowedtwopaths:
1. Onepaththatsimulatedtherepopulationmechanismsduringradiotherapy2. Another path that investigated and simulated the processes that are correlated to
hypoxiaanditsdistribution.In order to achieve this year’s objectives:model adjustment according to clinical data andvalidation, we have studied the effect of inter-patient variation (i.e. the impact of tumourgrowthkinetics,hypoxiaandrepopulation)ontreatmentresponse(objective1).Duetothefactthatheadandneckcancersaregreatlyheterogeneousregardingtheirhypoxiccontent anddistribution, anddue to the lackof F-FDG toquantitatively assesshypoxia,wehaveundertakenameta-analysisofallstudiesonhypoxia-specificPET/CTtracersconductedonheadandneckcancerandreportedintheliteratureoverthelastdecade(objective2).Theresults/conclusionshavebeenusedforfurthermodeloptimisationandvalidation.
TheneedforhypoxiaquantificationGiven that tumors are inhomogeneous entities, with subpopulations of hypoxic andradioresistantcells,doseadministrationduringradiotherapyshouldbenon-uniforminorderto allow for escalations in hypoxic regions and for dose reduction in areas of lowerradioresistance.Hypoxia-targetedradiotherapyusingdosepaintingisafeasibletechniquethathasthepotentialtoincreasetumorcontrolwithoutincreasingnormaltissuecomplications.Biological modeling using hypoxia-specific molecular imaging information is greatlyencouraged for the progress of individualized treatment planning and delivery and for theimplementation of biologically based treatment planning systems (Marcu 2014a, Jennings2015). In this sense, the need arises for finding quantitative associations between imagingparametersandtumor-specificcharacteristics.Thisobjectiveaimstoquantifythestatisticalpropertiesofhypoxictumorsubvolumesinheadandneckcancer(HNC)asmeasuredinPETscans,aswellastheirimpactonthefailureratetostandardchemoradiationtherapy,basedontheavailableliterature.Meta-analysisofPEThypoxia-imagingusinghypoxia-specifictracers(Chirla&Marcu2015)In head andneck cancer (HN), themost frequently used hypoxiamarkers are F-FMISO andmore recently, F-FAZA, while other markers used for these tumors, namely F-FETNIM, Cu-ATSM,F-EF3,F-EF5andF-HX4,arepoorlyrepresentedintheliterature.PEThypoxiamarkersshouldaccumulateinhypoxictissue,andwashoutfairlyquicklyfromnormoxictissue.F-FAZAscanshaveasomewhathighertumortobackgroundratiothanF-FMISOscansduetothemorerapidclearanceofthistracerfromnonhypoxictissue.Othertracersthatarepromisinginthis

Scientificreport2013-2015
15
respectareCu-ATSM,F-FETNIMandF-HX4.62-Cu-ATSMhassofarthebestcontrast,afterlessthan30minutespostinjection.EF3hasafasterclearancefromnormaltissueascomparedtoEF5,andthemetabolitesof these tracerscontribute far less to thesignal than in thecaseofFETNIM,FAZAandFMISO.CompilingthedataforhundredsofpreviouslyuntreatedpatientsinTable1,wefoundthatonaverage73%ofallHNcancerpatientsarehypoxicasmeasuredbyhypoxiaspecificPET.Sincemost patients have primary and/or nodal tumors, we have also calculated the fraction ofhypoxiasrelativetothenumberoftumors.Table1.Frequencyofhypoxiaanditsimpactonfailureafterstandardtreatment.Shownincurlybracketsisthenumberoftumorsorofpatientsconsidered.
PETtypeFractionhypoxicpatients
Fractionhypoxicprimarytumors
Fractionhypoxicnodaltumors
Fractionhypoxictumors*
Fractionfailuresinnon-
hypoxicpatients
Fractionfailuresinhypoxicpatients
Ratiofailureshypoxic/non-hypoxicpatients
Source
F-FMISO 0.74{207}
0.58{113}
0.66{58}
0.54{169} 0.141{65} 0.59{97} 4.1**
LeeetalTachibanaetalKikuchietalHendricksonetalRajendranetalDirixetalRischinetalYasudaetalSatoetalZipsetalNorikaneetal
F-FAZA 0.72{79}
0.69{68}
0.57{56}
0.63{124} 0.07{14} 0.40{26} 5.7
PostemaetalGrosuetalServagi-Vernat etalMortensenetal
62-Cu-ATSM - 0.60
{40} - - 0.14{16} 0.64{24} 4.7 MinagawaetalSatoetal
F-FETNIM - - - - - 0.63{19} - Lehtioetal
F-EF5 - 0.73{22} - - 0.0{6} 0.47{16} - Komaretal
F-HX4 0.70{10}
0.75{12} - - - - - Chenetal
ZegersetalOverall 0.73 0.63 0.61 0.58 0.12 0.55 4.6 Nr.tumors - 255 114 293 - - - Nr.patients
296 - - - 101 182 283
*Only studies that included both types of tumors **We excluded patients treated with tirapazamine. Hypoxic patients treated by standard chemoradiotherapywere on average 4.6 timesmorelikelytosufferafailurecomparedtononhypoxicones.

Scientificreport2013-2015
16
Considerablereoxygenationhappensduringstandardradiotherapy,seeTable2,inwhichweexcludedpatientswith nonhypoxic tumors and analyzed the data for patientswith at leastone hypoxic HN tumor. HV-P, HV-N and HV-all are respectively the hypoxic volumes forprimary,nodalandbothtypesoftumors.Themid-therapyscanswereactuallytakenbetweentheendofthesecondandfifthweekofradiotherapy,andthusalargevariabilityofresultsisexpected.
Table2.Thehypoxicvolumepre-andmid-therapyinpatientswithhypoxictumors(excludingbaselinenormoxictumors).Shownincurlybracketsisthenumberoftumorsorofpatientsconsidered.
PETtype
HV-P(ml)
baselineaverage(median)*
RatioHV-P
mid/pretherapyaverage(median)
HV-N(ml)
baselineaverage(median)
RatioHV-N
mid/pretherapyaverage(median)
HV-all(ml)
baselineaverage
(median)**
RatioHV-all
mid/pretherapyaverage.(median)
Ratiohypoxicpatients
mid/pretherapy
Source
F-FMISO 8.2 (3.4) {44} - - - 15.2 (8.1)
{18} 0.07
(0.004) {8}
0.27 {92}
Choi et al Lee et al Hendrickson et al Chang et al Dirix et al Rischin et al Figueiredo et al Zips et al Bittner et al Okamoto et al Lin et al
F-FAZA 9.8 (4.5) {46}
0.23 (0.08) {14}
11.5 (3.4) {32}
0.11 (0.0) {5}
10.5 (3.8) {78}
0.17 (0.03) {23}
0.52 {23}
Grosu et al Servagi-Vernat et al Mortensen et al Bollineni et al
F-FETNIM
14.3 (4.5) {18} - 3.6 (1.4)
{9} - 10.7 (3.6) {27} - - Lehtio et al
F-EF5 6.0 (1.2) {16} - - - - - - Komar et al
F-HX4 6.5 (2.3) {6} Zegers et al
Overall 9.6 (3.6) 0.23 (0.08) 9.8 (2.5) 0.11 (0.0) 11.0 (4.0) 0.15
(0.01) 0.32 Standard deviation 14.1 0.30 18.6 0.16 16.5 0.24 -
Range 0.1 - 78.6 0.0 - 0.91 0.1 - 96.5 0.0 - 0.35 0.02 – 96.5 0.0 – 0.91
0.11 – 0.67
Nr. tumors 121 14 41 5 129 31 - Nr. patients - - - - - - 115
* Two outlier patients with an HV-P > 157 ml were excluded ** Only studies that included both types of tumors. Some studies may list only the tumor with largest HV.
In Figures 1 and 2 we have plotted the statistical distribution of hypoxic fraction (HF)(excludingnormoxictumors)compiledfromalargenumberofsources.Thereisaclearbiastowardssmallerfractions,whenthegrosstumorvolume(GTV)isdelineatedviaCT,withthedistributionsshowinganexponentialdecay,regardlessofthetracerusedandthetypeofthetumor(primaryornodal).

Scientificreport2013-2015
17
Figure 1. Statistical distribution of the hypoxic fraction (HF), as measured from PET and CT, excludingnonhypoxic tumors, for: (a)F-FMISOscansof all reported tumors, (b)F-FAZAscansof all tumors, (c)F-FAZAscansofprimarytumorsand(d)F-FAZAscansofnodaltumors.
Figure2.Statisticaldistributionofthehypoxicfraction(HF),asmeasuredfromhypoxiaspecificPETandF-FDGPET,excludingnonhypoxictumors,for:(a)F-FMISOscansand(b)F-FETNIMscansofalltumors.

Scientificreport2013-2015
18
No significant correlation between the maximum SUV and the fractional hypoxic volume(using CT tumor delineation) has been observed in F-FAZA PET. We found a strongcorrelation (r=0.96)between themedian tumor tomuscleSUVvalueandHF,asshown inFigure3,wherethemedianistakenoverthewholetumor.
Figure3.CorrelationofthehypoxicfractionandthetumortomusclemedianSUVvaluemeasuredbyF-FAZAPETinprimarytumors,excludingnonhypoxictumors.ThePearsoncorrelationcoefficient,r,isalsoshown.We have also compiled data from various F-FAZA studies in order to verify the correlationbetweentheHFandthegrosstumorvolumeovertwoordersofmagnitude,asshowninFigure4,butnocorrelationcouldbeobserved.Thus,largetumorstendtohaveahypoxicfractionthatissimilartothatinsmalltumors.
Figure 4. Correlation of hypoxic fraction and gross tumor volume asmeasuredby F-FAZAPET andCT for allhypoxic tumors. The Pearson correlation coefficient, r, is also shown. The equivalent F-FMISO plot leads tosimilarconclusions,butthedatahaslowerdynamicrangeandstatistics.

Scientificreport2013-2015
19
Summary:Weperformedameta-analysisofallavailabledataonPEThypoxia-imagingofHNtumors, and extractedpatientdata relevant to the statistical distributionof hypoxic voxels,their behavior during regular radiochemotherapy and their correlation to final outcome. Alarge fraction(seeTable1)ofHNtumorsarehypoxic,andalthoughtheyshowasignificantresponsetotherapy(seeTable2),thefinalfailureprobabilityis4.6timeshigherthaninthecaseofnonhypoxic tumors.Wehaveanalyzedthedistributionof theHF forvarious tracersandtumortypes(primaryversusnodal)andconcludedthatisolatingthemetabolicallyactivevolumeiseffectiveinexcludingnonhypoxicvoxelsfromtheimagedtumors.HFiscorrelatedwiththemedianratioofthetumortomuscleSUVratiowhenafixedT/Mthresholdisused.Nevertheless,HFisuncorrelatedwiththegrosstumorvolume,suggestingthatthesizeofthetumor,asdelineatedbyCT,doesnotinfluencethepercentageofhypoxicvoxels.TheoptimisedhypoxicheadandneckcancermodelGiven the above results, themodelwas further developedwith different levels of hypoxia,ranging fromseverelyhypoxic tumours(3mmHg)towelloxygenatedtumours(10mmHg),withanoxygenenhancementratioof3(OER). Hypoxiccellresistance,bymeansofhypoxicsurvivingfraction(SFhypoxic)hasbeenmodelledasafunctionoftheoxygenenhancementratioand the surviving fraction of oxic cells in their corresponding cell cycle phase (resultspresentedatThe39thARACongress,Frascati,July2015).Therefore:
SF!"#$%&' = 1−1− SF!"#$"%&'
OER
Next to hypoxia, the tumourmodel also considers the cancer stem cell population (Marcu2004,2010,2014b,2015)(resultsalsopresentedattheWorldCongressonMedicalPhysics&BiomedicalEngineering,Toronto,June2015).ThefirstidentificationofCSCinHNCislinkedtothe work of Prince et al (2007) who has isolated a cellular subgroup exhibiting stem-likeproperties.Todate,thereareveryfewquantitativereportsintheliteratureonthepercentageofCSC inheadandneckcancer.The findings illustrate that therearesignificantdifferencesamongthestudiedheadandneckcell lines.Consequently, in theexperimentsconductedbyTang et al. (2013) the CSC proportion in various head and neck cell lines ranged between1.7%and13.5%.AnotherexperimentundertakenonHNCcell linesbyHarperetal. (2007)hasindicatedthattheproportionofCSCinCaLH3cell lineis12.3%.ThislimitednumberofquantitativestudiesonCSCinHNCcan,nevertheless,assisttheinsilico implementationandanalysisoftheeffectsofCSCsontumourbehaviourduringtreatment.Tostudyinter-patientvariabilityintreatmentresponse,threegroupsoftumours(withslow,average and rapid proliferation) have been simulated (figure 5 and table 3) (somepreliminaryresultspresentedatThe15thInternationalCongressofRadiationResearch,Kyoto,May2015).Thehierarchicalcelllineageiscomprisedof(1)cancerstemcellsthatdividebothsymmetrically and asymmetrically, (2) differentiated cells, which are short-lived non-stemcancercellsand(3)quiescentorrestingcells.Asaresultofmultipleiterationsthevalueof1.9hasbeendeterminedastheprobabilityoftheoriginalstemcellstodividesymmetrically,suchthatthebiologicallyvalidtumourkineticsaremaintainedthroughoutthesimulation.Naturalcelllossis85%,alsoinaccordancewiththeliterature.Ateverynewcellgeneration,boththeoriginalaswellasthenewcellareassignedanewcell-cycletime.Thevaluesofcell-cycletimeare created according to an asymmetrical Gaussian distribution truncated at one standarddeviationtowardslowervaluesand2standarddeviationstowardshighervalues(figure6).

Scientificreport2013-2015
20
Figure 5. Exponential tumour growth curves for three groups of head and neck cancerwith different growthkineticparameters.
Figure6.Gaussiandistributionof cell cycle times (cct)around themeanvaluewhen themeancct is20h.Cellcycletimesarerepresentedontheabscissaandthenumberoftumourcellsontheordinate.Table1.Tumourgrowthparametersaccordingtothemodel
Parameters Tumourgroup1
Tumourgroup2
Tumourgroup3
Literaturedata(range)[reference]
LengthofSphase6.67h 11h 20h
11h13.7h(7.3-37.5)(Tannock1998)
Meancellcycletime(range) 20h
(12–36)33h
(20–60)60h
(36-108)
33h(20-60)(Forster1992)
Volumedoublingtime 31d 52d 96d 45d(33-150)
(Tannock1998)
1.E+00
1.E+02
1.E+04
1.E+06
0 500 1000 1500
Num
bero
ftum
ourcells
Growth1me(days)
Cells20cct Cells33cct Cells60cct

Scientificreport2013-2015
21
Labellingindex 4.71% 4.69% 4.67% 8%(1.2-30)(Forster1992)
Celldivisionrate(24h) 2.3% 1.3% 0.74% -(derivedfromthemodel)
Pre-treatmentpercentageofcancerstemcells
5.37% 5.42% 5.36%-
(derivedfromthemodel)
Celllossfactor 85% 85%(Wigg2001)Hyperfractionatedtreatmenthasbeensimulatedonthevirtualtumour(i.e.1.2Gytwiceaday,5daysaweek,over7weeks,thusatotalof84Gy)growninvarioushypoxicconditionsandhavingdifferentcancerstemcellfractions.The in silicomodel showed that there is a strong synergistic effect beween radiobiologicalhypoxia and the fraction of cancer stem cells (some preliminary results presented at theACPESMWABranchMeeting,Perth,Australia,May2015asaninvitedtalk).Furthermore, the model showed that tumour growth kinetics also influences tumourresponse to treatment. Thus slowly growing tumours show a linear dependence withhypoxia/cancer stem population, while rapidly growing tumours present an exponentialincreasewithhypoxia/cancerstempopulation(figures7&8).
Figure7.Theinterplaybetweengrowthkineticsandcancerstemcelldivisionpatternformildlyhypoxictumours(9mmHg).40
45
50
55
60
65
0% 2% 4% 6% 8% 10% 12%Num
berof1.2Gyfractions
fortumourkill
ProbabilityofCSCsymmetricaldivision
60cct 33cct 20cct

Scientificreport2013-2015
22
Figure 8. Theinterplay betweengrowth kineticsand cancer stemcell divisionpattern forseverelyhypoxictumours(3mmHg).Legend:CSC = cancer stemcell;cct=cellcycletime
This behaviour would require pre-treatment predictive assays for head and neck cancerpatientsinordertodesignpersonalisedtherapies.
IV. Conclusions
Todate,thecurrentprojecthasreacheditssetobjectives:
• An in silico head and neck tumour has been grown using Monte Carlotechniqueswithbiologicallyvalidinputparameters.
• Tumour repopulation mechanisms for the avascular tumour that can betriggeredbyradio-orchemotherapyhavebeenstudiedandimplemented.
• Using the linear quadratic formalism of cell survival, various radiotherapyschedules have been simulated based either on clinical trials or other alteredfractionationprotocols inordertostudythesensitivityofdifferenttreatment-relatedparameterstotumourresponse.
• Theresponseofstemcellsaswellasdifferentiatedcellshavebeenanalysedandtheirinterplayevaluated.
• Thetumourgrowthmodelhasincludedthepartialoxygentensiontoillustratetheextentofspatialoxygenationanddistribution.
• A clinical studyhas beenundertaken encompassing 40head andneck cancerpatients that underwent PET examination, aiming to correlate the SUVparameterwiththeaggressivenatureofthetumour,whichisfurtherlinkedtothehypoxicstatus.
• The high SUV values among patientswith radioresistant tumours explain theeffectoftumourhypoxiaonglucosemetabolism.
• F-FGDbasedPET/CTdoesnotofferaquantitativeanalysisofhypoxicstatusanddistribution, therefore there is need for further investigations using morespecifictracers,suchasF-FAZA,F-MISO,F-FETNIM,F-EF5,F-HX4andCu-ATSM.
• Weperformedameta-analysisofallavailabledataonPEThypoxia-imagingandextractedpatientdatarelevanttothestatisticaldistributionofhypoxicvoxels,theirbehaviorduringregularradiochemotherapyandtheircorrelationtofinaloutcome.
0
100
200
300
400
500
0% 2% 4% 6% 8% 10% 12%Num
berof1.2Gyfractions
fortumourkill
ProbabilityofCSCsymmetricaldivision
60cct 33cct 20cct

Scientificreport2013-2015
23
• Hypoxia-specificPETimaginghasthepotentialtostratifypatients’responsetoradiochemotherapy.
• WehaveshowedthathypoxicfractiongreatlycorrelateswithmedianSUVbutnot with gross tumor volume, suggesting that the size of the tumor, asdelineatedbyCT,doesnotinfluencethepercentageofhypoxicvoxels.
• The in silicomodel has been optimised for various hypoxia levels and cancerstem cell fractions, showing that there is a strong synergistic effect beweenthesetwofactors.
• Furthermore, the model showed that tumour growth kinetics also influencestumour response to treatment. Thus slowly growing tumours show a lineardependence with hypoxia/cancer stem population, while rapidly growingtumourspresentanexponentialincreasewithhypoxia/cancerstempopulation.
Based on the aforementioned results, in the final phase of the project the hypoxic tumourmodel will be treated with various radiotherapy schedules, mainly unconventional (non-standard) in order to find the optimal protocol for head and neck cancer as a function ofhypoxialevelandfractionofcancerstemcells.
References:
1. ChirlaR,MarcuL,PET-basedquantificationofstatisticalpropertiesofhypoxictumorsubvolumesinheadandneckcancer,PhysicaMedica(2015)(submitted)
2. Dörr W, ThreeA'sofrepopulationduring fractionated irradiation of squamous epithelia: Asymmetryloss,Accelerationofstem-celldivisionsandAbortivedivisions,IntJRadiatBiol.1997;72(6):635-43.
3. Dörr W, Modulationofrepopulationprocesses in oral mucosa: experimental results, Int J RadiatBiol.2003,79(7):531-7.
4. DörrW,Timefactorsinnormaltissueresponsestoirradiation,In:JoinerM,vanderKogelA,Basicclinicalradiobiology,4thed,CRCPress,2009.
5. ForsterG,CookeTG,CookeLD,etal.Tumourgrowthratesinsquamouscarcinomaoftheheadandneckmeasuredbyinvivobromodeoxyuridineincorporationandflowcytometry,BrJCancer1992;65(5):698-702.
6. HarperL,PiperK,CommonJ,etal.Stemcellpatternsincelllinesderivedfromheadandnecksquamouscellcarcinoma,JOralPatholMed2007;36(10):594-603.
7. Harriss-Phillips WM,Bezak E, Yeoh EK, Monte Carlo radiotherapy simulations of acceleratedrepopulationandreoxygenationforhypoxicheadandneckcancer,BrJRadiol.2011;84(1006):903-18.
8. Jennings M, Marcu L, Bezak E, PET-specific parameters and radiotracers in theoretical tumourmodelling,ComputationalandMathematicalMethodsinMedicine2015;ArticleID415923.
9. MarcuL,vanDoornT,Olver I,Modellingofpost-irradiationacceleratedrepopulationinsquamouscellcarcinomas,PhysMedBiol.2004;49(16):3767-79.
10. Marcu L, Bezak E, Modellingoftumourrepopulationafter chemotherapy, Australas Phys Eng SciMed.2010;33(3):265-70.
11. MarcuL,Harriss-PhillipsW,FilipS,Hypoxiainheadandneckcancerintheoryandpractice:aPET-basedimagingapproach,ComputationalandMathematicalMethodsinMedicine2014a,ArticleID624642.
12. Marcu L, Tumour repopulation and the role of abortive division in squamous cell carcinomas duringchemotherapy,CellProliferation2014b;47(4):318-325.
13. MarcuL,ThefirstRsofradiotherapy-orstandingontheshouldersofgiants,AustralasianPhysEngSciMed2015,38(4).
14. PrinceME, Sivanandan R, Kaczorowski A, et al. Identification of a subpopulation of cellswith cancerstemcellpropertiesinheadandnecksquamouscellcarcinoma.ProcNatlAcadSciUSA2007;104:973–978.
15. TangAL,Owen JH,Hauff SJ, et al.Headandneck cancer stemcells: theeffectofHPV--an invitroandmousestudy,OtolaryngolHeadNeckSurg2013;49(2):252-60.
16. Trott K (1999) The mechanisms of acceleration of repopulation in squamous epithelia during dailyirradiation.ActaOncol.38,153–157.

Scientificreport2013-2015
24
17. TubianaM(1988)Repopulationinhumantumours,ActaOncol.27,83–88.18. TannockIF,HillRP.Thebasicscienceofoncology,3rded.,McGraw-Hill,pp.135-165,1998.19. WiggD.Applied radiobiologyandbioeffectplanning,Madison,Wisconsin,MedicalPhysicsPublishing,
2001.20. WithersHR(1993)Treatment-InducedAcceleratedHumanTumorGrowth,SeminRadiatOncol.3,135-
143.21. Zimny M, Gagel B, DiMartino E, Hamacher K, et al (2006) FDG--a marker of tumour hypoxia? A
comparisonwith [18F]fluoromisonidazole andpO2-polarography inmetastaticheadandneck cancer.EurJNuclMedMolImaging33(12):1426-31.
Projectdirector,
prof.univ.dr.LoredanaGabrielaMARCU