Embed Size (px)
Citation preview

Dr. Jordan Robertson ND
Sarcopenia and Weight Management
Dr. Jordan Robertson ND
Sarcopenia and Weight ManagementModule 1: Assessment, History Taking and treatment planning

Sarcopenia and Weight ManagementResearch Challenges
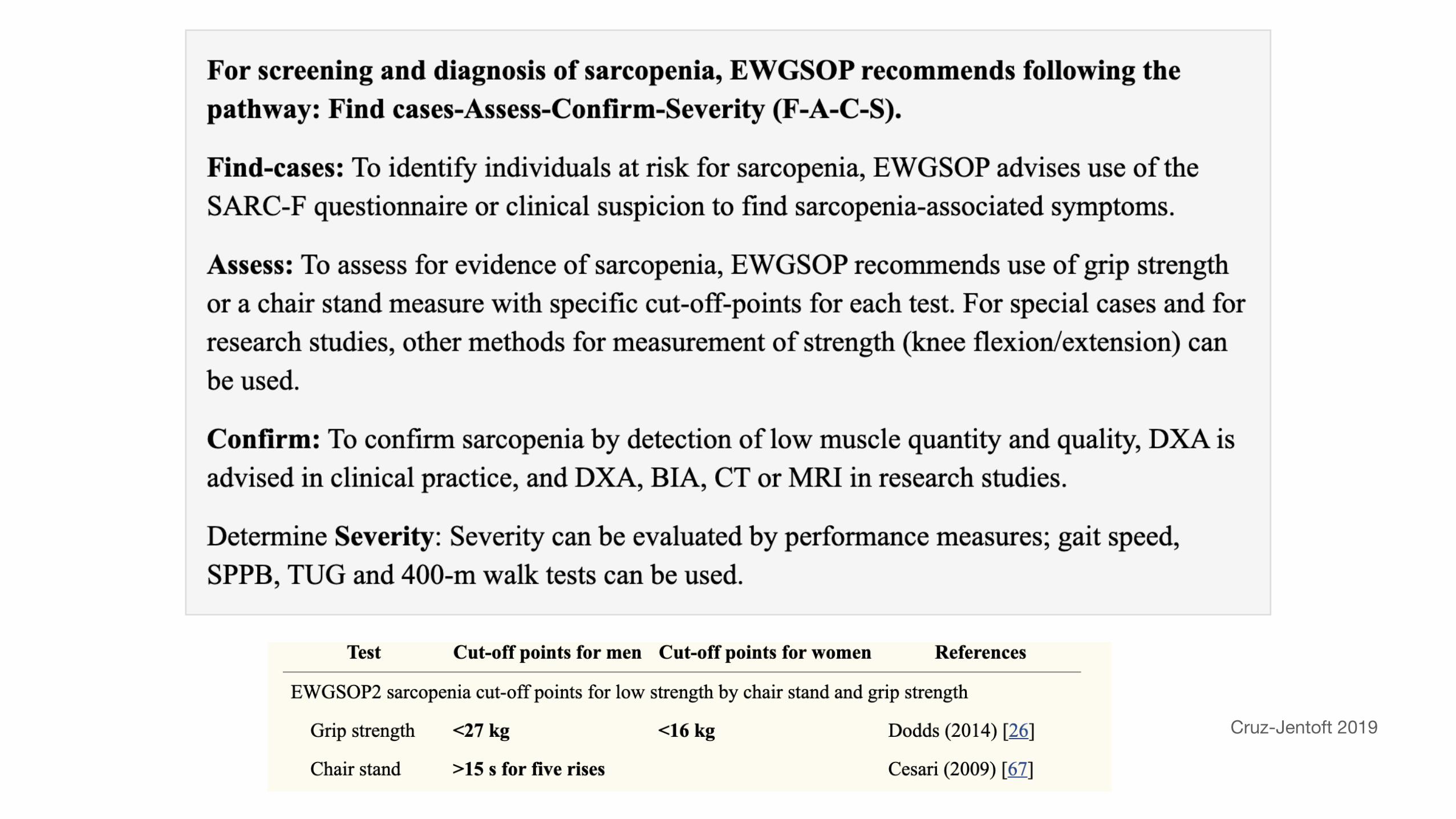
• European Society for Clinical and Economic Aspects of Osteoporosis and Osteoarthritis (ESCEO) has written multiple position papers on what is necessary to understand interventions for sarcopenia:
• The randomized placebo-controlled double-blind parallel-arm drug clinical trials should be the design of choice for both phase II and III trials.
• Treatment and follow-up should run at least 6 months for phase II and 12 months for phase III trials. (Reginster 2021)
• Challenges in recruitment for protein and exercise studies may skew the data collected: For example, in the Amasene (2019) study, 66.6% of eligible participants refused to participate because of health issues, lack of interest in the physical exercise program, or had problems to get to hospital for the intervention sessions.
Sarcopenia and Weight ManagementResearch Challenges
• Weight loss studies are littered with all of the bias seen in nutritional research. (Healthy user bias etc.)
• Chronological aging and menopause have both been implicated in weight gain in women, but both occur simultaneously. (The same may be true for men and testosterone)
• BMI become a poor marker as women age through menopause partly because of loss of height across the same time span as weight loss.
• Menopause causes an approximate ~5% increase in body fat, and almost the same decrease in lean tissue. This has blunted the effect of menopause on weight in studies that do not assess for body composition (Leeners 2017)

Sarcopenia and Weight ManagementResearch Challenges
• Many studies that conclude that a particular diet is ‘more’ successful than others has failed to record or comment on caloric intake.
• Attrition rates or “non-participatory” rates.
• Tracking EE and EI are challenging (patients do not exist in a vacuum)
• Studies that are shorter, are often using surrogate markers instead of clinical endpoints.
• HOMA-IR, HBA1C, cholesterol and TG, waist circumference, crude weight etc.
• Very tightly controlled studies are often days long, whereas long “RCTs” often dissolve into an observational trial because of how many variables they can’t control for in a 1 year study period.

Sarcopenia and Weight ManagementResearch Challenges
• Age at menopause and delay in HRT initiation may influence body composition and weight
• Generally there is a lack of focus on weight loss trials in women in menopause, with a systematic review that looked at all of the trials between 2003 and 2011 only finding 3 studies (Jull 2014)
• A systematic review of 56 studies found that very few could report successful weight maintenance over a 12 month period of time (Collins 2013)

Sarcopenia and Weight ManagementResearch Challenges
When reading any research study on weight and nutrition, you really only get to ask two questions:
1.Did it change energy expenditure?
2.Did it change energy intake?

Sarcopenia and Weight LossModule 1: Assessment and Treatment Planning
• In this module we will focus on the following:
• History Taking
• Risk Factors
• Relevant personal and family history
• Diagnostic Assessment
• Physical exam and laboratory assessment


Sarcopenia and Weight LossModule 1: Assessment and Treatment Planning
• Sedentary Lifestyle• Hormone and cytokine changes• Protein synthesis and regeneration changes• Motor Unit Remodeling• Evolutionary basis• Early developmental Influences • (Cruz-Jentoft 2019)
Sarcopenia and Weight LossModule 1: Assessment and Treatment Planning
• Muscle mass of the human body decreases by approximately 1.5% yearly after the age of 50 and by 2.5-3.0% yearly after the age of 60 (Xie 2020)
• 10% decrease in muscle mass leads to a decrease in immune function and an increase in the risk of infection.
• 20% reduction in muscle mass results in muscle weakness, a decreased ability to participate in activities of daily living, and an increased risk of falling.
• 30% reduction in muscle mass results in disability, loss of independent living ability, and failure of wound and pressure ulcer healing.
• 40% reduction in muscle mass results in a markedly increased risk of death from pneumonia, respiratory dysfunction
• Muscle is responsible for the consumption of nearly 80% of the body’s glucose content, and its resting metabolic rate accounts for 30% of the entire body’s resting metabolic rate
Sarcopenia and Weight LossModule 1: Assessment and Treatment Planning
History Taking
• History of weight loss and regain
• Medications
• Hormone status (adolescent, PCOS, thyroid, perimenopause, menopause, androgen deficient male)
Cruz-Jentoft 2019

Sarcopenia and Weight LossModule 1: Physical Exam
• Height, weight, WC, BMI calculation
• BMI testing has some inherent challenges (changes to height with age, overestimating adiposity in athletes and shorter patients)
• WC may be the more accurate measure of cardiovascular risk in women (Goh 2014).
Sarcopenia and Weight LossModule 1: Hormones and Gender differences
• Beginning at puberty, positive energy balance leads to female-typical AT distribution, i.e. greater acceleration of gluteofemoral subcutaneous AT and less growth of visceral AT.
• Estrogens and adipocyte genes synergize to produce female-typical AT distribution.
• Glutealfemoral fat deposits actually increase cell number before cell size, which may contribute to the protective effects of GF-AT on metabolic risk.
• Women can gain weight in this region without severe metabolic effects. • Loss of estrogens after menopause partially reverses female-typical regional AT
distribution, and estrogenic HRT prevents this. • Loss of estrogens after menopause increases total adiposity and decreases lean
body mass, and estrogenic HRT prevents this.


Sarcopenia and Weight LossModule 1: Hormones and Gender differences
• The decision to eat is primary driven by processes involving complicated signals from the GI tract, AT, metabolic processes, and reward/learning signals.
• There are many secondary mechanisms that drive food intake such as circadian rhythm, emotions, psychological state and stress.
• Sex hormone exert their influence on these secondary mechanisms.
• Mood and cognition both impact EI, which becomes exacerbated with menopausal changes in mood and cognition (Leener 2017)
• Many of the other effects of hormones on eating: taste, insulin, leptin etc have been examined in animal models, but are not clinically relevant at this time.
Sarcopenia and Weight LossModule 1: Hormones and Gender differences
• The best relationship between ovarian hormones and EI can be seen in cycling women, with decreases in appetite in the follicular phase, and increases in the luteal phase.
• In healthy-weight cycling women, food intake decreases ~200–300 kcal/d from the luteal maximum to the peri-ovulatory minimum, an amount relevant to body-weight regulation (Leener 2017)
• The decrease in calories consumed in the follicular phase is related to meal size, not meal frequency.
• There is a reduction in the intake of sweet foods in the follicular phase.
• Eating does not decrease during anovulatory cycles
• Estrogen decreases emotional binge eating and progestins oppose the effect of estrogens.

Sarcopenia and Weight LossModule 1: Hormones and Gender differences
• Exercise is the only voluntary ways to increase EE.
• Women spontaneously walk more (1600 steps per day) in the follicular phase (Day 2015).
• Around menopausal age (hormone independent) Exercise EE decreases.
• The decrease in Exercise EE at the age of menopause may be upwards of 40% reduction from earlier in a woman’s life. This is clinically relevant.
• Women can likely increase exercise EE without a substantial increase in food intake, or even a slight reduction (Reviewed in Leener 2017)

Sarcopenia and Weight LossModule 1: Hormones and Gender differences
• Greendale 2019 examined the difference between pre-menopause, the MT and post menopause and the anthropometric changes that occur during those years.
• Steady increase in weight, fat mass and BMI begins in the 8 years prior to the MT.
• Accelerated changes in fat mass (increase) and lean tissue (decrease) occurs in the 4 years straddling the FMP.
• Weight and BMI had steady increases over the years, without a MT accelerated change.
• Changes to body composition slowed in post menopause.

Sarcopenia and Weight LossModule 1: Testing
Testing Summary• Fasting Glucose, Insulin and HbA1C• Lipid panel (TG/HDL ratio)• Liver Enzymes (and/or US) for NAFLD• Thyroid Panel (TSH, T4, T3 rT3?)• Serum hormones to assess ovulation, and menopause status. • PCOS Screening: LH/FSH ratio, AMH• Serum androgens (total T, free T, calculated FAI)• SHBG• Vitamin D • Ferritin (Skalnaya 2017, Beard 1997) • CBC with platelet count (Park 2018)

Sarcopenia and Weight LossModule 1: The impact of Hormones
• Thyroid lab work is challenging to interpret in the context of weight management.
• “Thus far, evidence is scarce from weight-loss trials where the cause of weight change is known and homogeneous among individuals.” (Liu 2017)
• Most human data on the relationship between TH parameters and nutritional status are derived from drastic interventions such as bariatric surgery, very low calorie diets, or manipulation of macronutrient composition
• Declines in T3 are mostly driven by CR and not by exercise induced weight loss (Weiss 2008)
• Weight loss restores TSH and elevated fT3 levels, which reduces RMR. This is likely part of the challenge of weight maintenance after loss (Longhi 2013)
• Of note, patients medicated for their thyroid, even with normal TSH, have lower scores of overall wellbeing when compared to controls (Saravanan 2002)
Sarcopenia and Weight LossModule 1: The impact of Hormones
• We may observe higher T3 “than expected” in obese patients at baseline.
• Obese patients with high-normal T3 may have a greater than expected reduction in RMR with weight loss.
• T3 will decline with caloric restriction. It’s not clear if this is important clinically.
• Testing thyroid function before and after weight loss (6 months) may be helpful to track implications on thyroid function.

Sarcopenia and Weight LossModule 1: Medication Options
• There are currently no FDA approved medications for sarcopenia (Dhillion 2017)

Sarcopenia and Weight LossModule 1: Medication History
• A review of 49 trials on OCP and weight did not find a significant association between combined OCP use and weight gain (Gallo 2014)
• Progestin only contraceptives may have a relationship with weight gain, with some studies showing an average increase of 2 kg per year (Lopez 2013)
• Research on GNRh inhibitors is mixed (for precocious puberty) and women treated for endometriosis are rarely on the drug longer than 6 months.

Dr. Jordan Robertson ND
Sarcopenia and Weight ManagementModule 2: Nutrition

Sarcopenia and Weight LossModule 2: Nutrition - Motivational Interviewing
• Patients have mixed feelings about change, and keeping things the same (ambivalence).
• Patients who are exposed to MI are more likely to enter, stay in and complete their treatments.
• Armstrong (2011) systematic review on MI (n=12)
• Greater reduction in body weight (-1.4 kg) in the MI group versus control.
• The review by Barnes (2015) examined 24 RCTs using MI for weight loss in adults.
• 1/3 of MI studies showed benefit over control
• 50% of MI studies lost more than 5% of initial starting weight.

Sarcopenia and Weight LossModule 2: Nutrition - Motivational Interviewing
• The 40-Something Randomized Controlled Trial (Williams 2013) was an RCT focused on preventing weight gain in normal weight 45–50 year-old women who were on the brink of the menopause transition.
• The intervention aimed to intrinsically motivate the women to permanently change their diet and physical activity behaviors to achieve weight control.
• At the end of the 12 month intervention, women who had received the MI based intervention had a significantly lower mean body weight and diastolic blood pressure
• The diets of the MI group were more nutrient dense with respect to food sources of iron and potassium, and they consumed more fruit

Sarcopenia and Weight LossModule 2: Nutrition - Motivational Interviewing
• The follow up to the 40 something weight loss trial (Williams 2019) followed up with the participants from the original data set 12 months after discontinuing their support. They had goals of an average 2.5 kg reduction in the MI group after 12 months of “no treatment”.
• In the monitoring phase they attended the lab at 12, 18 and 24 months and was mailed one newsletter about the study.
• Both the 10,000 steps per day and increased vegetable servings suggestion at the exit interview were positively corelated to successful weight maintenance at 24 months.


Sarcopenia and Weight LossModule 2: Nutrition - Motivational Interviewing
1. Open-ended questions. Avoid asking questions that can be answered with a “yes” or “no.” Broad questions allow patients maximum freedom to respond without fear of a right or wrong answer. It can be as simple as, “What's been going on with you since we last met?” Another question, appropriate for almost anyone, would be, “If you had one habit that you wanted to change in order to improve your health, what would that be?”
2. Affirmations. Never underestimate the power of expressing empathy during tough spots or in celebrating patients' accomplishments. When you review patients' goals, take joy in their success and show your joy. One of the authors (CF) even gives patients gold stars – the same ones distributed in elementary school. Patients love getting them and wear them proudly.

Sarcopenia and Weight LossModule 2: Nutrition - Motivational Interviewing
3. Reflective listening. Patients often have the answers; the physician's role is to help guide them. Reflective listening involves letting patients express their thoughts and then, instead of telling them what to do, capturing the essence of what they have said, with the purpose of eliciting conversation and helping them arrive at an idea for change. Here's an example: It is also appropriate to acknowledge the patient's mood about what he or she is telling you. For example, “You mentioned that you won't go in public in a bathing suit because of your weight. That seems to make summertime very stressful for you.” Reflecting patients' statements and feelings back to them reinforces self-efficacy, and it allows the conversation to keep moving forward.
4. Summaries. Summarizing involves recapping what the patient has said, calling attention to the salient elements of the discussion and allowing the patient to correct any misunderstandings and add anything that was missed. Summaries can occur throughout the visit but are particularly helpful in bringing the visit to a close. It is often effective to end a summary with an open-ended statement such as “I am wondering what you're feeling at this point” or “I am wondering what you think your next step should be.”
Sarcopenia and Weight LossModule 2: Nutrition - Motivational Interviewing
• Ask you patient what their greatest barriers are and what possible solutions look like.
• Ask what are the “low hanging fruit” and how exactly they would change it. (Time, day, how to prepare, etc – create specificity)
• Ask about barriers to continuing their positive changes.
• Advanced MI uses statements to position yourself as the one “against” the changes.

Sarcopenia and Weight LossModule 2: Nutrition – Other strategies
• Free weekly community meetings improve diet (fibre, protein, etc) and weight loss over standard care. (Ambrosini 2018)
• Studies on PCOS that have used Facebook groups do show greater compliance than control (Turner-McGrievy 2014)
• Text messaging once every two weeks had a small but significant increase in weight loss (Silina 2017)
• Appointment attendance at 2 months is significantly correlated to success and attrition in PCOS women (Moran 2019)
• Person to person care appears better than computer delivered care (Beleigoli2020)
Sarcopenia and Weight LossModule 2: The patient Interview
• 24 hour diet recall, week pattern and monthly pattern discussion.
• Ask patients what they do well and where they struggle.
• Meal timing
• Fasting window, front or back loading, hunger between meals
• Macronutrient profile
• Caloric intake
• Dietary pattern
• Day, week, month

Sarcopenia and Weight LossModule 2: The patient Interview
• Ask your patient about previous “successes” and why they were successful?
• Structure, accountability, affordability, community, support etc.
• Ask your patient what was difficult about maintaining these successes.
• Time, cost, lack of knowledge in maintenance phase, hunger etc.
• Ask your patient how they want their current solution to look.
• What is their best-case scenario?
• Connect their ideas about a solution with expectations and results.

Sarcopenia and Weight LossModule 2: The patient Interview
• In my opinion, most weight loss programs don’t have enough learning about the factors that influence weight, hunger, body water fluctuation, caloric intake or realistic goals on body composition.
• This is a set-up for when patient’s finish the program.
• For example, patients on WW don’t know what to do about nuts when the program is over.
• Long term success HAS to include LEARNING on your patient’s part in order to have long term success.

Sarcopenia and Weight LossModule 2: The patient Interview
• The “Audit”
• Have your patient’s audit their diet for 14 days.
• Track what they eat, amounts, time of day.
• Track how they feel, hunger cues, energy patterns.
• I prefer them to use an app that gives feedback on caloric intake.
• Then they return ask them what they “notice”.
• Look at each meal, day, week, week/weekend pattern.
• Let patient help you create solutions.
• Give feedback that gets them closer to their goals/macro needs.

Sarcopenia and Weight LossModule 2: Diet Tracking
• There are numerous concerns regarding nutrition tracking and the potential for triggering harm or disordered eating.
• Overall the research is positive for self-monitoring behaviours (weight and nutrition tracking) on successful weight loss and maintenance (Simpson 2017)
• Studies on disordered eating and negative thoughts and the use of tracking devices shows that the disordered eating patterns were present before the trial, not caused by the trial.
• That said, there is evidence that tracking before the visit may be a clue for disordered eating (tracking exercise and nutrition). (Plateau 2018)

Sarcopenia and Weight LossModule 2: Caloric Intake
• What about sarcopenia and caloric restriction?
• Paradoxically CR without malnutrition may ameliorate some of the cellular dysfunction seen in sarcopenia (Marzetti 2009)
• Xie (2020) has a great review on the molecular mechanisms behind CR impacting sarcopenia.
• Not enough clinical data to prescribe CR for sarcopenia, but the current evidence doesn’t show harm in CR without malnutrition.
• Kawano (2021) saw some negative impacts of undernutrition on T2D older subjects on muscle mass over 18 months.

Sarcopenia and Weight LossModule 2: Macronutrient Breakdown
• Macronutrient manipulation in a eucaloic diet may change markers of disease but will not change weight.
• For example, women with PCOS prescribed a 40% eucaloric diet will see improvements in HOMA-IR scores but no change in weight (or other clinical outcomes)
• Macronutrient ratios should consider a patient’s goals, satiety, CR, culture and symptoms
• C (25-55%), P (15-30%), F (20-40%) will fit the majority of your patients.

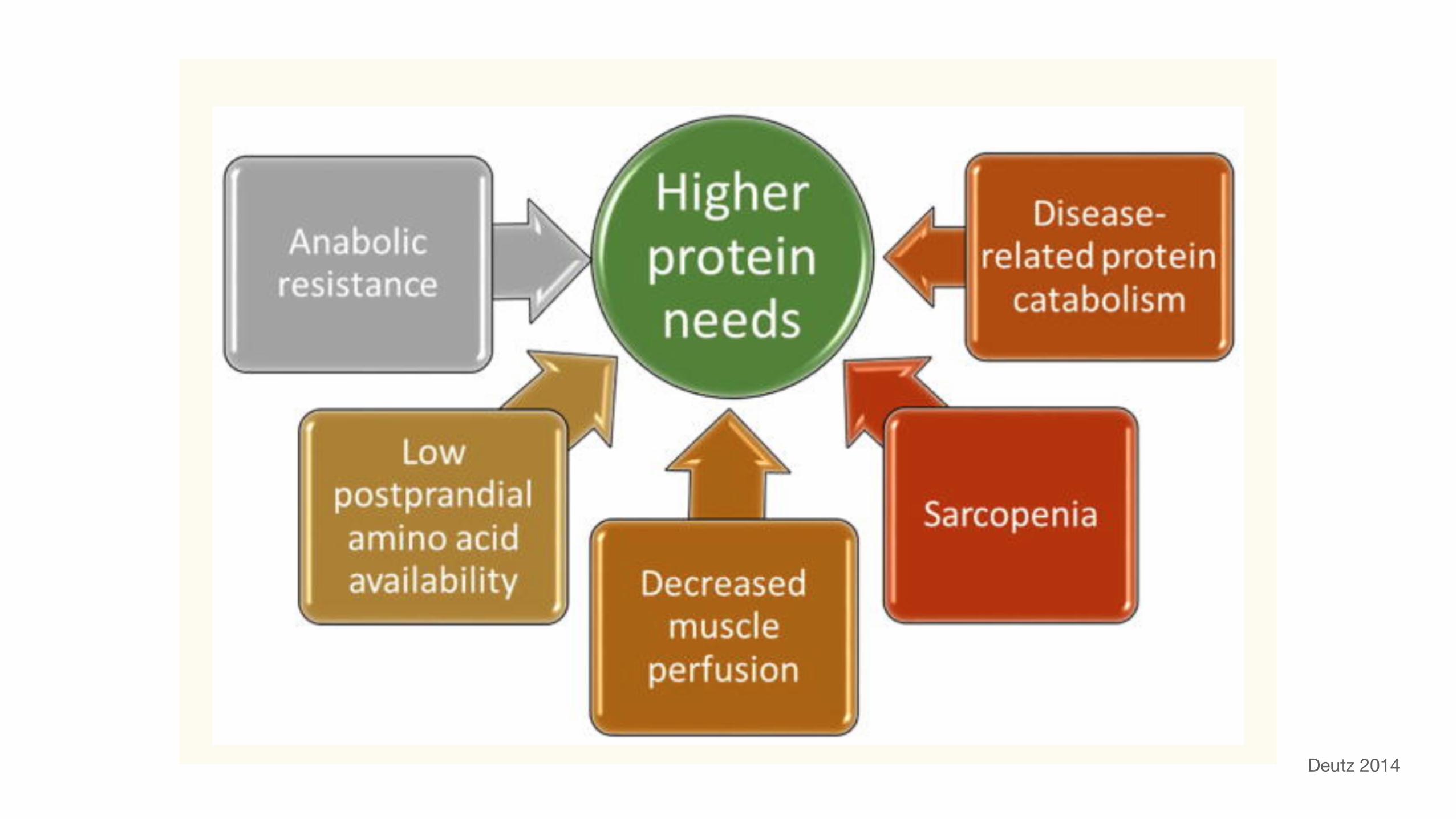
Sarcopenia and Weight LossModule 2: Nutrition – Protein
• General guidelines recommend 1.2-1.5 grams per kilo per day.
• Studies show safety up to 4.0 grams but likely no benefit beyond 2.0 g/kg/d
• Some of the challenges of studying the elderly and protein is the rampant malnutrition in this population.
• Cramer (2016) is a great example:
• Malnourished adults benefit from both a low dose (14 gram) and “high dose” (20 gram) oral protein supplement.
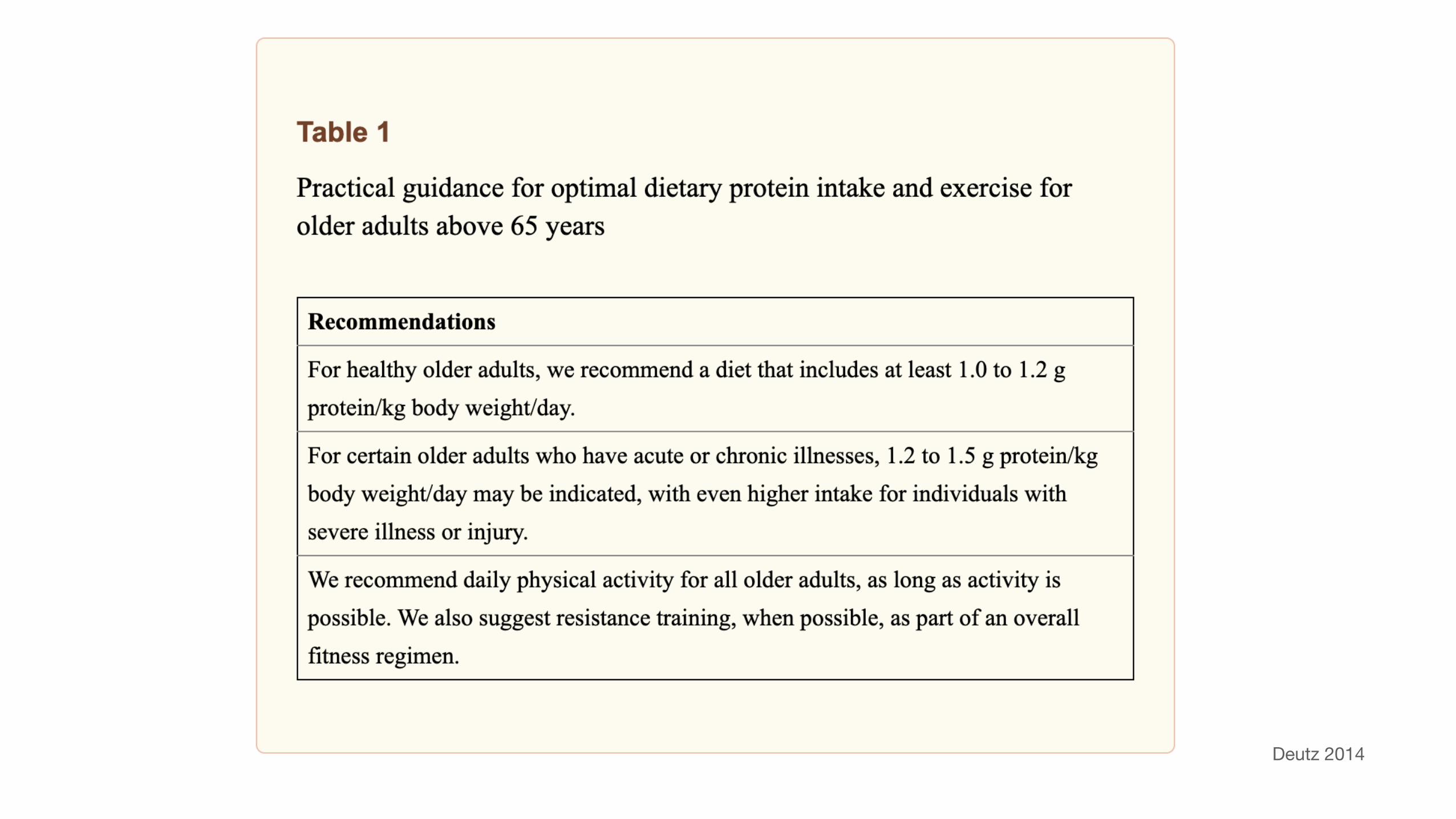
Deutz 2014
Deutz 2014

Sarcopenia and Weight LossModule 2: Nutrition – Protein
• Atherton (2020) fed elderly subjects 20 or 40 grams of protein following resistance training.
• Participants had improvement in all 1RM lifts (chest press, leg press, squat) after the study period with the 40 g of protein dose following resistance exercise.
• Metabolic studies have shown that subjects ≥65 years of age require about 2% more protein per meal in order to maximize muscle protein synthesis, and leucine supplementation has been shown to be potentially useful for this purpose (Rondanelli 2021)

Sacopenia and WeightModule 2: Nutrition - Protein
• Protein intake and kidney function? (Quoted from Deutz 2014)
• In older adults with healthy kidneys or with only mild dysfunction, standard protein intake is safe.
• In older patients with moderately impaired GFR or another form of CKD, physicians customarily assess the balance between risks and benefits, and use clinical judgment to make recommendations.
• In patients with severe CKD, it is usual to recommend a lower protein intake of 0.6 to 0.8 g/kg/day with sufficient energy intake. However, multi-morbid patients on palliative care are an exception to this rule. These individuals may benefit from unrestricted intake of dietary protein because the short-term risks associated with protein energy wasting are greater than the long-term risks of worsening renal function due to diet with standard protein content.

Sarcopenia and WeightModule 2: Nutrition - Protein
• Elswyk (2018) reviews kidney function in the healthy Americans who exceed the RDA for protein and find no additional kidney disease, improvement in blood pressure and no increase in kidney stones.
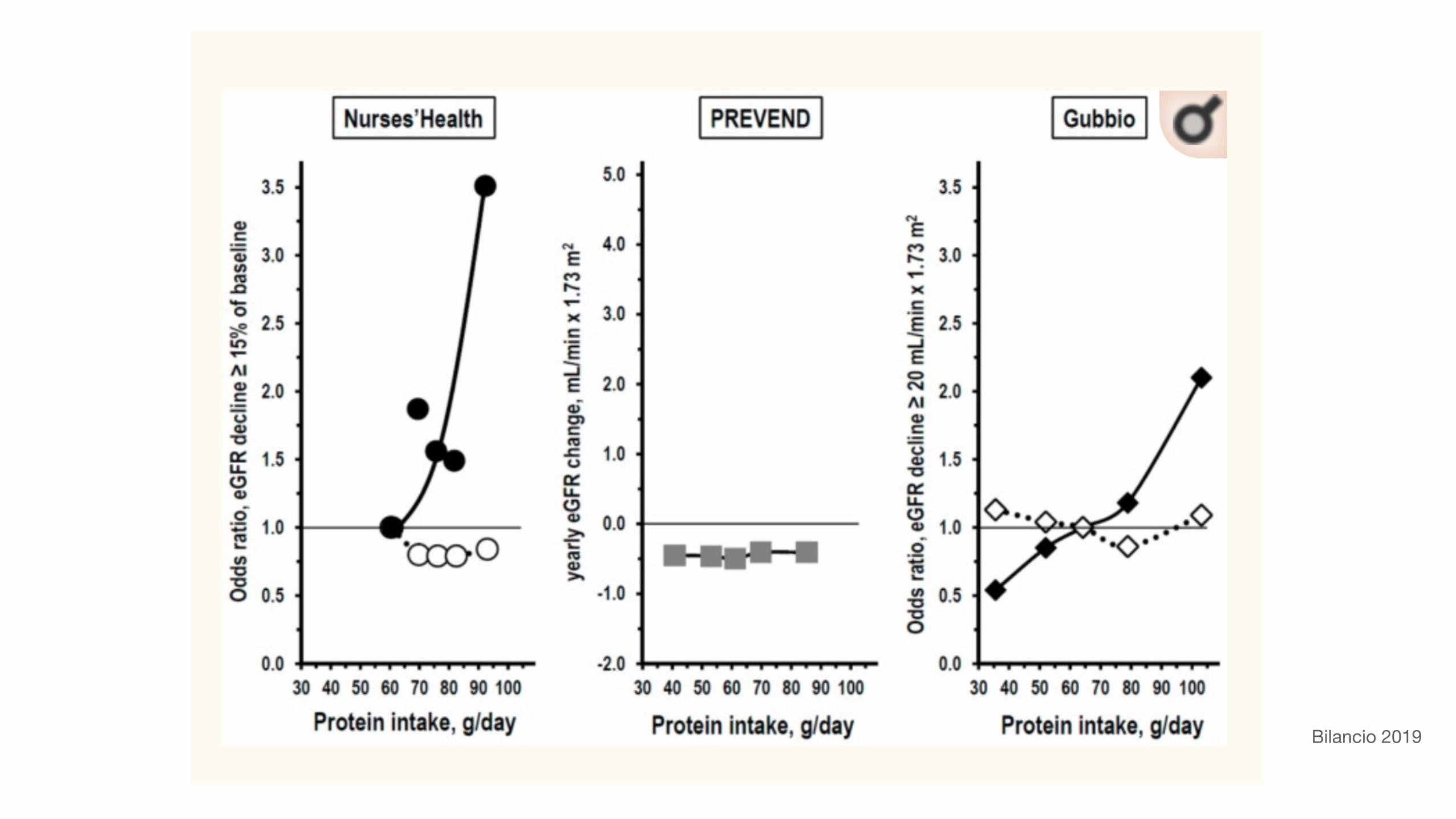
Bilancio 2019

Bilancio 2019

Sarcopenia and Weight LossModule 2: Nutrition – Weight Regain? The LOOK AHEAD
• The Look AHEAD trial, a diabetes prevention lifestyle program which encompassed a multi-disciplinary behavioural-focused intervention.
• In the intensive intervention group, mean weight loss was 8.5% initial bodyweight at 1yr, and 4.7% at 4yrs
• By year 8 of the program there had been a stabilising effect on weight loss in the intensive intervention group, with average weight loss remaining on average 4-4.7% between 4yrs and 8yrs
• Participants that lost >10% of bodyweight during the initial 1yr intervention were significantly more likely to maintain between 5-10% weight loss at 4yrs follow-up.
• 42% had maintained 10% of weight loss, while 70% had maintained >5% loss
• After 8yrs of follow-up, those numbers remained 39% and 65%.

Sarcopenia and Weight LossModule 2: Nutrition – Long Term Maintenance
• The general advice group received:
• 3 x 1hr meetings per year from 1yr to 4yrs with general advice on diet, lifestyle, and physical activity education
• 1 meeting per year for 5yrs to 8yrs
• The results in this group were underwhelming.

Sarcopenia and Weight LossModule 2: Nutrition – Long Term Maintenance
• The Intensive support group in the Look AHEAD Study, participants received:
• Small groups of 10-20
• 3 meetings per month for the first 6-months
• 2 meetings per month between 6-months to 1yr
• 1 meeting per month up to 8yrs
• In addition to these monthly group sessions, subjects had individual sessions with an ‘interventionist’ (which included registered dietitians, psychologists, and exercise specialists) every month in person, with a second contact by phone or email 2-weeks thereafter.


Sarcopenia and Weight LossModule 2: Nutrition – Long Term Maintenance
• The Look Ahead Trial
• The energy goal for persons < 114 kg (250 lb) is 1200−1500 kcal/d and is 1500−1800 kcal/d for individuals ≥ 114 kg.
• Participants counted calories and fat grams with the aid of a booklet provided. They are prescribed < 30% of calories from fat, with < 10% from saturated fat.
• During weeks 3−19 individuals were encouraged to replace two meals with a liquid shake and one snack with a bar and to eat conventional foods for dinner.
• From weeks 20−22, participants decreased their use of meal replacements and increased the consumption of conventional foods.

Hall 2018

Hall 2018

Sarcopenia and Weight LossModule 2: Nutrition – Long Term Maintenance
• Greater physical activity levels [including less screen time] (Look Ahead, Wing 2008, Ayyad 2000)
• Fewer intentional weight loss episodes (Mcguire 1999,Wadden)
• Greater time spent in maintenance (Wing 2005, Weiss 1999)
• Less dietary restraint (Wing 2005, Westenhoefer 2004)
• Frequency of self-weighing (Wing 2005, Look Ahead, Wing 2008)
• Higher self-motivation, self-efficacy, and locus of control (Lazzeretti 2005)
Sarcopenia and Weight LossModule 2: Nutrition – Weight Regain
• In the Lean Habits Study, Westenhoefer (2004) quantified 8 behavioural characteristics at baseline:
• Flexible vs. rigid dietary control
• Meal regularity
• Eating Behaviours
• Food choices
• Restriction of food quantity
• Physical activity
• Stress coping



























