Embed Size (px)
Citation preview

Running Head: INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 1
Innovation Diffusion: A Process of Decision-Making
The Case of NAQC
Jonathan E. Beagles, M.S.
Ph.D. Candidate
520-975-1224; [email protected]
School of Government and Public Policy
University of Arizona
Keith G. Provan, Ph.D.
McClelland Professor of Management & Organizations
Eller College of Management and School of Government and Public Policy
University of Arizona
Scott F. Leischow, Ph.D.
Professor, Family and Community Medicine
Arizona Cancer Center
University of Arizona
Work on this paper was funded by a grant from the National Cancer Institute (R01CA128638-
01A11) and an Arizona Cancer Center Support Grant (CCSG - CA 023074)

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 2
Abstract
This research examines the effect of both information sharing ties and internal decision-
making factors to understand the innovation implementation process among organizations within
the North American Quitline Consortium (NAQC). NAQC is a large, publicly funded “whole
network,” spanning both Canada and the U.S., working to get people to quit smoking. Bringing
Simon‟s (1997) decision-making framework together with a framework of innovation diffusion
(Rogers, 2003) we develop and test hypotheses regarding the types of network ties and internal
decision-making factors likely to be influential at various stages in the innovation diffusion
process. Using negative binomial regression to model three distinct stages in the implementation
process (Awareness, Adoption/Rejection, Implementation), the findings provide evidence
supporting the argument that different types of ties are likely to be important at different stages
in the innovation implementation process and the importance of these ties varies depending on
the role an organization plays as well as internal decision-making factors.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 3
Collaboration among networks of public and private organizations has been an especially
important strategy for addressing the public‟s most pressing health and human services needs,
such as mental health, diabetes and obesity, homelessness, child and youth health, and smoking
cessation. In particular, networks have become important mechanisms for building capacity to
recognize complex health and social problems, systematically planning for how such problems
might best be addressed, mobilizing and leveraging scarce resources, facilitating research on the
problem, and delivering needed services (Provan and Milward, 1995; Chaskin et al., 2001;
Lasker, Weiss and Miller, 2001; Bazzoli et al., 2003; Leischow et al., 2010; Luke et al., 2010).
In order to achieve these gains, critical information must flow between and among the
organizations involved in the network. For instance, when addressing complicated health needs,
it has been suggested that information about new practices that appear to be especially effective
needs to be disseminated, not only from those who create knowledge about these practices to
those who utilize them, but also among those who utilize the practices (Ferlie et al., 2005). In
this regard, network ties have been found to be essential for the dissemination of knowledge
leading to adoption of innovative practices (c.f. Greenhalgh et al., 2004; Rogers, 2003; Valente,
2010).
While the association between network ties and the diffusion of innovations has long
been recognized (Coleman, 1966), more recent research suggests networks matter more than
simply as a means of transferring information (Brass et al, 2004). In addition to the literature on
networks and information transfer (Hansen 1999, 2002; Reagans & McEvily, 2003) networks
have been shown to serve as conduits of social influence either through direct influence by social
relations (Galaskiewicz & Wasserman, 1989; Rao, Davis & Ward, 2000) or through similarities
in network positions leading structurally equivalent actors to adopt similar opinions and
INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 4
behaviors (Galaskiewicz & Burt, 1991). This research has contributed significantly to our
understanding of networks. However, additional questions have been left unanswered.
Specifically, while evidence suggests the types of ties, their strength, and who they are with are
important for knowledge transfer and the diffusion of innovations, fewer studies have looked at
how different characteristics of network ties may impact the diffusion process differently or how
the relative importance of these ties may vary across stages in an organization‟s innovation
implementation decision. These questions are especially important with regard to the literature
on „whole networks‟ (Provan, Fish & Sydow, 2007) where the structure of network ties impacts
not only each individual organization but also the network as whole (Provan & Milward, 1995).
In an attempt to address this gap in the literature, this study utilizes an individual
decision-making framework (Simon, 1997) to derive hypotheses regarding the relative
importance of network ties and internal decision-making factors across the distinct stages of the
innovation decision process (Rogers, 2003). We test these hypotheses across organizations
within the North American Quitline Consortium (NAQC); a network of public and private
organizations within the U.S. and Canada involved in the provision of telephone-based
counseling and related services to people trying to quit smoking.
Research Setting
The North American Quitline Consortium (NAQC) is an example of the increasing
number of networks established to help address complex health and social problems (Bazzoli et
al., 2003; Chaskin et al., 2001; Lasker, Weiss and Miller, 2001; Provan and Milward, 1995).
NAQC was established in 2004 in response to a perception, among those in the tobacco control
community, that wide variation existed among emerging quitlines with respect to the practices
being adopted and implemented. In response to this perception, one of the primary purposes of

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 5
NAQC was to increase communication among the quitlines in order to reduce this variation
through the promotion of evidence based practices (Anderson & Zhu, 2007).
In the summer of 2009, when the study began, there were 63 quitlines within the US and
Canada; each quitline consisting of at least one funder and a one service provider. Typically, the
sole or dominant quitline funding organization is the state/provincial public health department,
which then contracts with a vender to provide the actual array of quitline services. In some cases
(n=13), vendors provide services for a single state/province while in other cases (n=7), vendors
serve multiple states/provinces. This leads to a unique network structure within NAQC compared
to the majority of public/private networks previously reported in the literature (Provan, Fish &
Sydow, 2007). Rather than there being a central public funder working with numerous private
service providers (c.f. Provan & Milward, 1995; Provan, Huang & Milward, 2009), within
NAQC, private service providers are often the most central actors spanning numerous political
boundaries to provide services to multiple public funders. At the time of our data collection, the
largest service provider was a for-profit entity contracting with 18 state quitlines. While the
public funders maintain ultimate accountability for the success of the quitlines, the providers
play an important yet varying role in decision-making regarding the services provided within
each quitline.
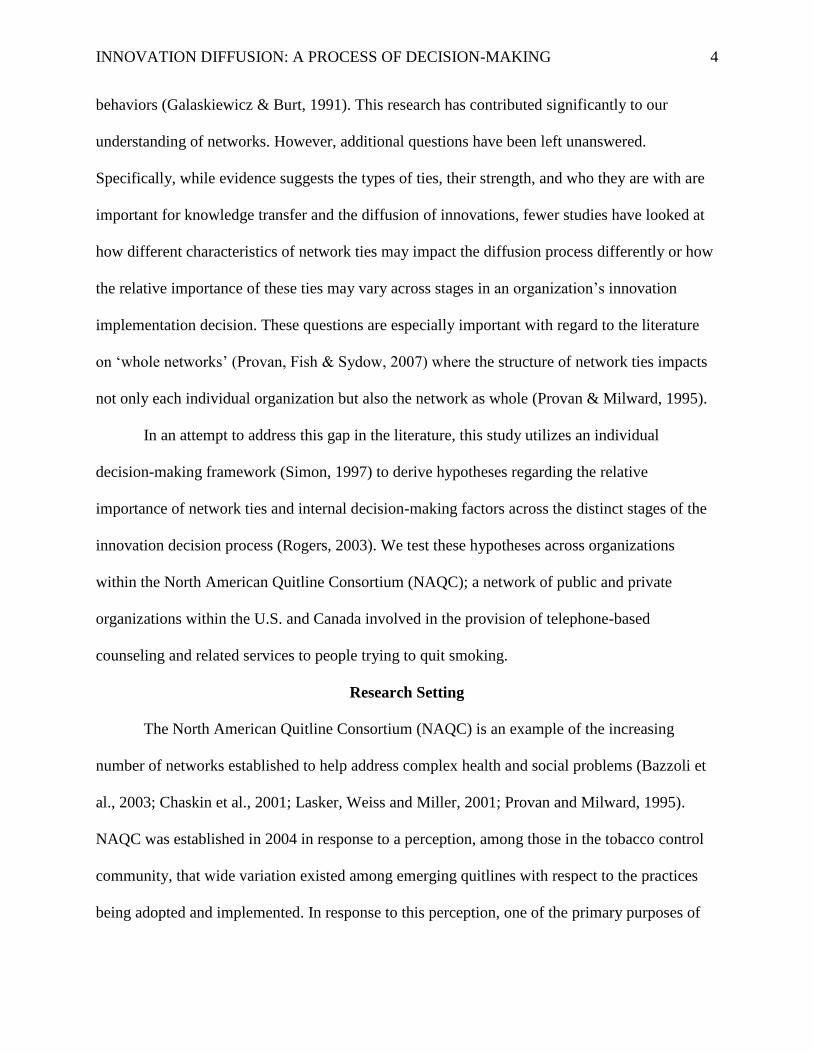
In addition to funders and venders, other organizations and individuals participated in the
network such as national funders and researchers. In 2006, this diversity of roles and interests led
to the creation of an independent network administrative organization (NAO) to serve as the full-
time coordinator and neutral broker for the network (Provan, Beagles & Leischow, 2011). Figure
1 provides a depiction of the network using the NetDraw function in UCINET 6 (Borgatti,
Everett, & Freeman, 2002).

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 6
---------------------------------
Figure 1
---------------------------------
Literature Review and Hypotheses
Two frameworks form the basis for developing the hypotheses in this study: Rogers‟
diffusion of innovation framework (2003) and Simon‟s bounded rationality (1997). While the
two frameworks provide important contributions in their respective fields, there has been little
conversation between them. This lack of conversation was noted by Valente (2010) when he
suggested more diffusion studies try to understand how their “postulates influence individual
decision-making” (p. 194).
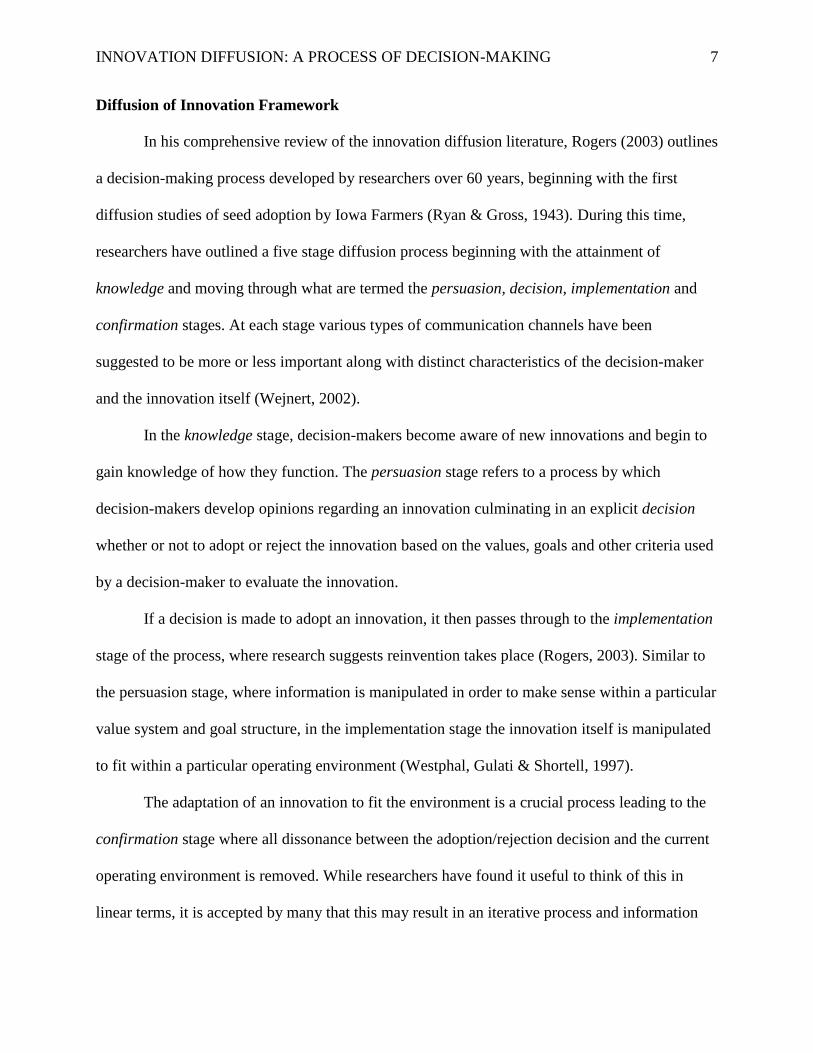
An important distinction between the two frameworks has to do with the perspective
from which they enter the decision-making process. Specifically, research on innovation
diffusion begins with specific innovations of interest and tries to understand how these
innovations move through the stages of the implementation process: knowledge, persuasion,
decision, implementation and confirmation (Figure 2). On the other hand, Simon (1997) and
those developing a decision-making framework study how information, search, evaluation and
capacity (Figure 2) come together in an iterative process around a perceived problem. For those
from a diffusion of innovation perspective a pro-innovation bias assumes the new innovation will
solve a perceived need and make its way through all phases in each organization while those
from a bounded rationality perspective try to understand how a perceived need is solved through
the coming together of these decision-making factors and any particular innovation is one of
many alternatives being evaluated.
-----------------------------
Figure 2
-----------------------------
INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 7
Diffusion of Innovation Framework
In his comprehensive review of the innovation diffusion literature, Rogers (2003) outlines
a decision-making process developed by researchers over 60 years, beginning with the first
diffusion studies of seed adoption by Iowa Farmers (Ryan & Gross, 1943). During this time,
researchers have outlined a five stage diffusion process beginning with the attainment of
knowledge and moving through what are termed the persuasion, decision, implementation and
confirmation stages. At each stage various types of communication channels have been
suggested to be more or less important along with distinct characteristics of the decision-maker
and the innovation itself (Wejnert, 2002).
In the knowledge stage, decision-makers become aware of new innovations and begin to
gain knowledge of how they function. The persuasion stage refers to a process by which
decision-makers develop opinions regarding an innovation culminating in an explicit decision
whether or not to adopt or reject the innovation based on the values, goals and other criteria used
by a decision-maker to evaluate the innovation.
If a decision is made to adopt an innovation, it then passes through to the implementation
stage of the process, where research suggests reinvention takes place (Rogers, 2003). Similar to
the persuasion stage, where information is manipulated in order to make sense within a particular
value system and goal structure, in the implementation stage the innovation itself is manipulated
to fit within a particular operating environment (Westphal, Gulati & Shortell, 1997).
The adaptation of an innovation to fit the environment is a crucial process leading to the
confirmation stage where all dissonance between the adoption/rejection decision and the current
operating environment is removed. While researchers have found it useful to think of this in
linear terms, it is accepted by many that this may result in an iterative process and information

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 8
gathering is necessary at all stages of the process albeit the types of information necessary may
differ.
Bounded Rationality Framework
In his study of Administrative Behavior, Simon (1997) laid out the framework for a study
of organization behavior based on an understanding of individual decision-making. From this
perspective, organization decision-making and action is seen as the result of an interaction
between four key components: information, search, valuation, and capacity. Specifically, it is
argued decision-makers do what is perceived to be in their best interest based on their unique set
of goals and preferences. However, decision-makers are limited in two ways. First, they may be
limited in the amount and quality of information they possess regarding their available
alternatives. Second, they may be limited in their capacity to implement an alternative even if it
is preferred. Thus organizational behavior regarding the adoption and implementation of
innovations is expected to vary based on differences across these components. First, if goals and
values differ across organizations, behavior is expected to differ regardless of whether they
possess the same information and capacities. Second, with the same goals and capacities,
behavior is expected to differ if organizations have access to different information. Finally,
holding information and values/goals constant, differences are expected in organization behavior
due to differences in capacities. For any single organization, decision-making is seen as a
process of adjusting each of these components until an alternative is identified consistent with all
three (Barnard, 1938).
A Synthesis
Despite differences in terminology, the overlap in the frameworks is apparent. It is not
difficult to sense similarities between awareness and information; and the factors that increase
INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 9
the amount of information a decision-maker possesses are also likely to increase its awareness of
any particular innovation. Likewise, the emphasis on goals and values as the criteria used to
evaluate alternatives overlaps neatly with the persuasion and decision stages in the diffusion
literature. Finally, while the diffusion literature highlights the importance of innovation
adaptation and dissonance removal as important aspects of the implementation and confirmation
phases, other research highlights the importance of capacity in an organization‟s ability to utilize
new information (Tsai, 2001). Bringing these two frameworks together allows us to generate
hypotheses regarding which network and decision-making factors are likely to be most important
at each stage in an organization‟s decision whether or not to adopt and implement a new
innovation. Specifically, factors leading to increased information are likely to be most important
for awareness. Factors impacting values, goals and evaluative criteria in general are most likely
to be influential at the decision stage and factors increasing organizational capacity are likely to
be most important for implementation.
Information, Search and Awareness
The importance of networks for gathering information is well documented (Ahuja, 2001;
Burt, 2004; Tsai, Hansen, 1999 & 2002; Owen-Smith & Powell, 2004; Powell, Koput & Smith-
Doerr 1996; Regeans & McEvily, 2003). However, this work shows not all ties are the same.
Early on, Granovetter (1983) suggested weak ties are better for finding jobs because these ties
are more likely to provide an actor with non-redundant information. Burt (1992) modified the
argument suggesting weak ties are important not because they are weak but because they often
span structural holes which leads to nonredundent information. However, Hansen (1999, 2002)
add to the discussion by arguing that complex knowledge, such as information regarding the
costs and benefits of new innovations, is more easily transmitted across strong ties. In their study

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 10
of knowledge transfer within a contract R&D firm, Reagans and McEvily (2003) articulate the
concept of knowledge pools, suggesting specific types of information are located in different
areas of a network based on the roles and functions of those actors. Thus rather than having
relationships spanning structural holes between individuals, they argue tapping into diverse
knowledge pools is what is truly important and having strong ties to these knowledge pools is
beneficial especially when the knowledge is complex.
Within NAQC there are at least five general „knowledge pools‟: state/provincial funders,
service providers, national tobacco policy and funding organizations, and researchers as well as
an independent network administrative organization (NAO) (Provan & Kenis, 2008) which was
established to coordinate activities and information sharing among these other participants. Each
of these groups plays an important role in the network and is perceived by the NAO to contribute
a unique set of resources and perspectives to the network (Provan et al., 2011). While it seems
reasonable each group of organizations can and does contribute unique knowledge to the
network and can be the source of new innovations, the role of researchers stands out as an
exceptionally likely source of information regarding evidence based practices. Also, because the
role of the NAO is to gather and disseminate knowledge we suspect ties to the NAO will
increase the likelihood of an organization being aware of evidence based practices . Based on
this logic, we propose the following hypotheses:
Hypothesis 1a: The greater the number of connections an organization has to others in
the network (especially researchers), the more likely it will be aware of innovative
practices.
Hypothesis 1b: Organizations connected to the network administrative organization will
be more likely to be aware of innovative practices.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 11
In addition to network ties, research in both the innovation diffusion and decision-making
literatures has identified search behavior as an important factor influencing a decision-makers
awareness of information (March & Simon, 1958; Rogers, 2003). Both lines of research have
noted decision-makers with a felt need are likely to be more active in seeking out solutions while
those without a perceived need may be more passive in receiving information from their social
contacts or simply mimic the behavior of others (DiMaggio & Powell, 1983). Being actively
involved in decision-making may be one factor leading to more active search behavior. For
example, if an organization perceives itself to be in a role with significant decision-making
responsibility it may feel a need to be more informed regarding information affecting those
decisions. However, if an organization shares its decision-making responsibilities with others, it
may perceive less of a need to stay informed. Stated in the form of a hypothesis:
Hypothesis 2: The more control in decision-making an organization perceives itself to
have, the greater the number of innovative practices it will be aware of.
Values, Norms and Decision-Making
More than a means of information sharing, research suggests networks are important for
transmitting social norms (Galaskiewicz & Wasserman, 1989; Galaskiewicz & Burt, 1991)
which lead to the adoption of behaviors above and beyond what would be expected by rational
processes. Often these forces come from central or powerful organizations in the environment
such as national policy or funding organizations (Fligstein, 1990) or central network
coordinating organizations (Owen-Smith & Powell, 2004).
If this is indeed the case, we could expect ties to the NAO and to national policy and
funding organizations to serve more than just an information sharing function. In addition to
information sharing, we would suspect ties with these powerful organizations to influence a

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 12
decision-makers valuation criteria. Specifically, in the context of our study, we would suspect
ties to the NAO and these national organizations, more than ties to other organizations, to
increase the likelihood of an organization adopting evidence based practices while controlling for
its level of awareness. Stated in the form of hypotheses:
Hypothesis 3a: Organizations connected to the network administrative organization will
be more likely it will be to adopt innovative practices.
Hypothesis 3b: The greater the number of connections an organization has to National
Organizations, the more likely it will be to adopt innovative practices.
Internal decision-making processes such as values and goals and other evaluative criteria
are likely to have their biggest impact at the decision stage of the innovation diffusion process. It
is at this stage where diffusion researchers suggest we will see the culmination of an
organization‟s process of evaluating an innovation based on the knowledge it has gleaned.
However, to understand this evaluation process, it is important to be familiar with the evaluative
criteria organizations are likely to use. Three criteria are prevalent in the literature: efficiency,
effectiveness and prestige. Underlying the rational decision-making perspective is the idea
decision-makers will choose the alternative they perceive to be in their best interest. This concept
of best interests is commonly understood to be the most efficient (greatest benefit for least cost)
decision. Another criterion used to evaluate alternatives is by their perceived effectiveness. This
criterion differs from efficiency in that it pays less attention to the costs of an alternative. In
practice, effectiveness is often evaluated based on perceptions of consistency with an
organization‟s mission. Finally, in the innovation diffusion literature, research suggests
prestigious organizations are more likely to adopt new innovations; especially when they are
perceived as being consistent with the norms of the community (Rogers, 2003). Depending on

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 13
which criterion an organization utilizes, we can expect differences in its adoption/rejection
decisions. Specifically, organizations placing a greater emphasis on efficiency are likely to
require an innovation to meet more rigorous requirements than those placing an emphasis on
mission fit as an evaluative criterion in deciding whether or not to adopt a particular evidence
based practice. While both may see benefits in implementing a practice those focusing on
efficiency also place a great deal of concern on the cost side of the equation. Prestigious
organizations may also have less rigorous requirements for adopting new practices because of
the additional perceived benefit of maintaining their status within the network. Stated in the form
of hypotheses:
Hypothesis 4a: The greater the importance an organization places on rational
factors(efficiency), the less likely an organization will adopt new evidence based
practices.
Hypothesis 4b: The greater the importance an organization places on mission fit, the
more likely an organization will adopt new evidence based practices.
Hypothesis 4c: The greater an organization’s reputation within the network, the more
likely an organization will adopt new evidence based practices.
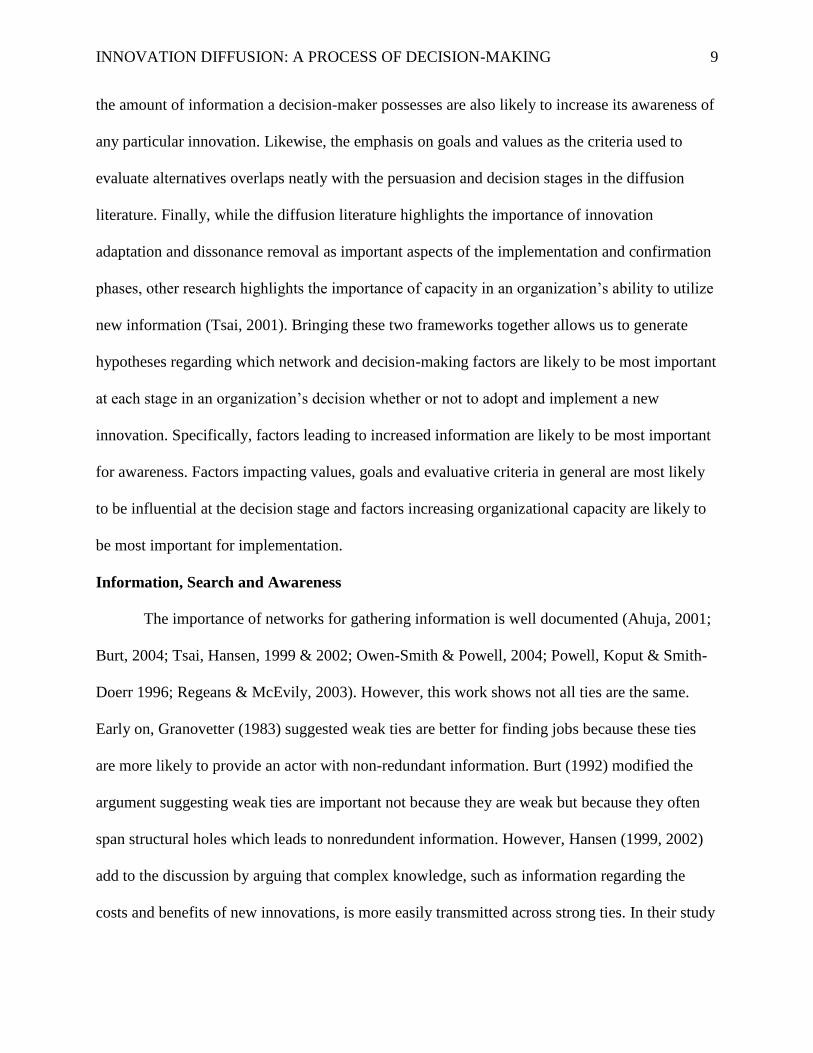
Capacity and Implementation
The final stage of the innovation-decision process with which we are concerned has to do
with implementation. At this stage information about the practice has been gathered and it has
been evaluated in light of the evaluative criteria of the organization. Here we suspect the capacity
of an organization will play a crucial role in determining whether or not an organization is able
to implement a practice it has decided to adopt. Along with internal capacities such as technical
expertise and finances, network and diffusion researchers have pointed to the importance of
INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 14
network relations at the implementation stage. Specifically, these findings suggest the ability of
an organization to implement a new innovation effectively is enhanced when it can communicate
with others who have gone through or are going through the same process (Ducharme, et al.,
2007). A second way in which implementing organizations can gain the information they need is
through connections to the NAO; since this organization often plays a central role in the network
and is charged with network coordination and the dissemination of information. In the case of
quitlines, these connections are likely to be most important for provider organizations because of
their direct involvement in the implementation and reinvention process. Also, because
reinvention is an important part of successful implementation, the involvement of implementing
organizations in the decision-making process should enhance the effectiveness of reinvention
decisions and thus increase the likelihood of successful implementation. Stated in the form of
hypotheses:
Hypothesis 5a: The greater the number of connections a quitline’s provider organization
has with other providers the greater the number of innovative practices successfully
implemented.
Hypothesis 5b: Quitlines with provider organizations connected to the network
administrative organization will successfully implement a greater number of innovative
practices.
Hypothesis 5c: The more a quitline’s provider organization is made part of the decision-
making process, the greater the number of innovative practices it will successfully
implement.
Figure 3 provides a visualization of the hypotheses.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 15
---------------------------
Figure 3
---------------------------
Data
The data for this analysis was collected during the summer of 2009. It is the first of three
rounds of data collection, which will ultimately allow for longitudinal analysis and a better
understanding of the diffusion process. The network consists of numerous individuals and
organizations filling a variety of roles. However, our focus on the adoption and implementation
of innovations guided our decision to limit the collection of data to only the organizations
directly involved in this particular decision-making process along with the network
administrative organization (NAO).
The organizations surveyed (n=95) consisted of 73 funder organizations (some quitlines
had multiple funders), 20 service providers and one organization serving in both capacities as
well as the NAQC NAO. Depending on organization size, data were collected from 1 to 6
respondents (identified beforehand as the top decision-makers regarding quitline issues) at each
organization. Primary data were collected using a web-based survey developed expressly for this
project but based on methods and measures utilized previously by Provan and colleagues
(Provan and Milward, 1995; Provan, et al., 2009). In addition, questions and methods were pre-
tested on a “working group” of key quitline members who agreed to provide initial feedback.
After extensive follow-up efforts using email and telephone, our final results included completed
surveys from 186 of 277 individual respondents (67.1% response rate), representing 85 of 94
quitline component organizations (90.4%) plus the NAQC NAO, and at least partial data (at least
one component organization) from 62 of the 63 quitlines (98.4%).

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 16
Our unit of analysis is the quitline, represented by the funder organization. We focused
on the funder for a number of reasons. First, we had complete data on network ties as well as
responses about awareness, adoption, rejection and implantation of evidence-based practices
from 60 of the 63 quitlines, but only partial data from a number of the larger, multi-quitline
provider organizations. In particular, one of these large providers did not complete the practice
questions since its management felt strongly that because the funder organization initiates the
contract and pays the bills, it is the funder who decides what practices to use. We used this logic
as well in our decision to focus on the funder. Second, many of the providers served multiple
states and provinces, making it difficult to disentangle the effects of the role of these providers
relative to one of its quitlines versus another. Each U.S. state (and territory) and each Canadian
province is represented by a quitline funder organization, each with its own separate budget and
network connections, making it possible to compare meaningfully across quitlines and thus, test
our hypotheses. Finally, while providers represent public, nonprofit, and for-profit entities, all
quitlines are predominantly funded by a public entity, allowing us to examine the impact of
public contracting on service awareness. Hence, our analytical focus is the funder organization
as the representative of each quitline.
Measures
Innovation decision stages. To gather information at each stage of implementation, we
asked respondents where they believed their quitline was in the implementation process
regarding 23 practices identified by the network NAO and „project working group‟. These
practices ranged from the provision of proactive counseling to the use of text messaging and the
referral of callers to health plans. However, for this study we excluded six practices from the
analysis: two because they pertained to US quitlines only; two because they were pharmacology
INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 17
related practices; and two due to lack of evidence supporting their effectiveness. The remaining
17 practices related to behavioral therapy and related management practices consistent with the
core mission of quitlines (See Appendix A for a complete list of practices).
In completing this section of the survey, respondents were first asked to indicate „Yes‟ or
„No‟ regarding whether or not they were aware of a practice. If respondents indicated „Yes‟ they
were aware of the practice, they were then presented with a follow-up question asking them to
indicate at what level of the decision-making process their quitline was at. To answer this
question, they were provided four response options: „Have not yet discussed‟, „In discussion‟,
„Decided not to Implement‟ or „Decided to Implement.‟ If the respondent indicated a decision
had been made to implement a particular practice, they were next presented with a 5-point scale
1=No progress has been made yet to 5=Fully implemented (the practice has become part of the
quitline’s policy or standard operating procedures for all eligible callers) and asked to indicate
what level of implementation they felt their quitline had achieved regarding the practice. From
this information we created four binary variables for each practice for each quitline1. A quitline
was considered AWARE2 of a practice and received a score of 1 if at least one respondent from
the quitline marked „Yes‟ to the first question. A quitline was considered to REJECT a practice
and received a score of 1 for the practice if the majority of respondents within the quitline
indicated „Decided not to Implement‟ in the second question. Likewise, a quitline was
considered to ADOPT a practice and received a score of 1 for the practice if a majority of
respondents indicated „Decided to Implement‟ in the second question. Finally, for
1 While providers were asked to respond to these questions separately for each quitline they served, due to the
abstention from these questions by one of the large providers, we chose to analyze the funder‟s responses as the
quitline‟s response except where noted otherwise. 2 While the measure described is a count of the number of practices a quitline is aware of, analysis was done on
UNAWARE (the number of practices a quitline was unaware of) to better suit negative binomial modeling 2 While the measure described is a count of the number of practices a quitline is aware of, analysis was done on
UNAWARE (the number of practices a quitline was unaware of) to better suit negative binomial modeling

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 18
IMPLEMENT, quitlines received a 1 if the majority of respondents indicated a 4 or higher on the
5-point scale in the last question. Once these variables were constructed, a count variable was
calculated to indicate the number of practices in which a quitline received a score of 1 at each
stage. Scores could range from 0 to 17 (See Table 1 for a summary)
--------------------------
Table 1
--------------------------
Information sharing. Data on network relationships were collected based on receipt of
information in four areas: financial, general management, service delivery, and
promotion/outreach. Respondents were presented with a list of all quitline funders, then provider
organizations, and then other national non-quitline member organizations having a major tobacco
control focus and involvement. For each organization listed, respondents were asked to indicate
whether they received information from that organization, which of the four types of information
they received, and the level of intensity of the relationship in terms of frequency and importance
(scored on a 1 to 3 scale). Only responses scored at a high level of intensity (3) were utilized in
the final analysis.
Because some quitlines consist of multiple funders or multiple providers, we found it
necessary to aggregate these multiple responses to obtain a single funder or single provider
response for each quitline. Of the 62 quitlines from which we received at least partial data, we
received multiple funder responses from six and multiple provider responses from one. To obtain
a single funder and single provider response from each quitline, we aggregated individual
responses from the multiple organizations as if the respondents came from the same
organization. These aggregations left us with 60 funder and 17 provider responses.
Because responses were provided by individuals and the analysis for this paper is

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 19
presented at the organization level, a tie was considered to exist at the organization level if at
least one respondent from that organization reported receiving information from that
organization. We apply this rule based on the presumption that the segregation of duties within
an organization often necessitates a single individual be the primary person responsible for
maintaining a relationship with a particular organization (Broshack, 2004; Maurer & Ebers,
2006).
Using these data, a series of network variables were constructed for both the funders and
providers of each quitline. Consistent with the survey data and the hypotheses, the following
five distinct types of network variables were constructed for each funder, all based on indegree
(information received) centrality and all based on the highest level of intensity of involvement:
funder ties to the NAO (fnNAO: coded 0 or 1); the number of funder ties to other funders
(fnFUNDERS); number of funder ties to other providers (fnPROVIDERS); number of funder ties
to the 12 national organizations that were NAQC members, but which were not part of a specific
quitlines, like the RWJ foundation, CDC, American Legacy Foundation, and Health Canada
(fnNATIONAL); and the number of funder ties to the 10 most highly connected tobacco control
researchers (fnRESEARCH) (from a drop-down list of 42 tobacco control researchers previously
identified). For this last measure, each quitline respondent was allowed to list up to five
researchers but responses were weighted so no quitline organization could score more than a
single point for any one researcher and no more than five points total.
Because our hypotheses regarding the effect of providers‟ connections is based on their
ability to observe and discuss implementation related information we constructed the following
two variables: provider ties to the NAO (prNAO: coded 0, 1); provider ties to other providers

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 20
(prPROVIDERS). Ties to these two knowledge pools are suspected to be most important for
implementation and reinvention decisions.
Search. To capture an organization‟s involvement in quitline decision-making, we asked
each respondent the following question: “When deciding whether or not to implement a new
treatment practice, please indicate how decisions are usually made between your organization
and your quitline partner organization(s).” Responses were provided using a likert-type 5-point
scale with 1 = ‘Funder Decides’, 5 = ‘Service Provider Decides’, and 3 = ‘Decision is Shared
Equally’. After taking the average individual score within the organization as the organization‟s
response, we created a dummy variable, WHO, with organizations scoring a three or higher
receiving a 0 indicating the provider is heavily involved in decision-making and organizations
scoring less than 3 receiving a 1 indicating the funder dominates decision-making. Twenty-six of
the 60 funders reported the provider was heavily involved in decision-making.
Valuation criteria. In addition to the information sharing data, we asked 12 questions
regarding a quitlines‟ decision-making process (see Appendix B for a copy of the questions). The
12 items (4 items each) were designed to capture the three components of the Theory of Planned
Behavior (Ajzen, 1991): attitude toward behavior, subjective norms, and perceived behavior
control. The first 8 items, anticipated to capture the first two components, were measured using a
likert-type 5-point scale where 1 = Strongly Disagree and 5 = Strongly Agree. The final 4 items
thought to capture the last component again used a likert-type 5-point scale where 1 = Not Very
Important to 5 = Very Important. We then took the average individual response within each
organization to serve as the organization level response. If an organization did not have a
response for a particular item, we substituted the overall average response. Next we reverse
coded the responses to question 7 and ran a confirmatory factor analysis (see Appendix C for the

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 21
results). Using Varimax rotation with stata v.9 we confirmed a three factor solution. However,
the three factors were not the three factors anticipated. Rather, the four questions anticipated to
capture attitudes toward behavior split in to two factors with the first two questions regarding
evidence of effectiveness and cost loading on one factor with a scale reliability alpha of .66
while the last two items regarding the importance of mission and team consensus loading on the
third factor with a scale reliability alpha of .68. Four of the remaining eight items created a third
factor with a scale reliability alpha of .58.
Based on the factor analysis, we constructed two variables. The first variable,
RATIONAL, was constructed by taking the average of an organization‟s responses to the two
items loading on the first factor regarding effectiveness and cost. The second variable, MISSION,
was constructed by taking the average of an organization‟s responses to the two items loading on
the third factor regarding mission and consensus. Being part of the attitudes component, these
two factors correspond well with the two evaluative criteria identified in the literature: efficiency
and mission fit. Because the construct underlying the items in factor two was not apparent and
the scale reliability was low, we exclude these items from the analysis.
Reputation. Respondents were asked to identify up to five quitlines that “other than
[their] own, [they] most admire for doing an especially good job regarding tobacco quitline
activities.” Because organizations could have more than one respondent and thus nominate more
than five quitlines, the responses were first aggregated to the organization level and each
organization was given a total of five votes. Thus, if individuals belonging to the same
organization listed 10 quitlines, each of those 10 quitlines received a score of .5. Likewise, if an
organization only reported admiring a single quitline, that quitline received a score of 53. All the
3 Other methods for creating a REPUTATION variable were explored such as using the total individual responses or
total organization responses. While the results did not vary substantively, we chose this measure as a way of

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 22
organization level scores were aggregated for each quitline giving it an overall REPUTATION
score ranging from 0 to 56.19.
Controls. Finally, because the size of an organization has consistently been shown to
predict innovation and the adoption of innovation (Rogers, 2003), we control for a quitline‟s size
by including a variable, SPEND, indicating the quiltine‟s 2009 spending per smoker as
calculated by the NAQC NAO based on data reported by the quitlines in the network‟s Annual
Survey. The overall average spending per smoker was substituted for any missing data (Table 2
provides correlations and descriptive statistics for all the variables described above).
--------------------------
Table 2
--------------------------
Analysis
As discussed above, we constructed four dependent variables capturing three stages of
the innovation-decision process: awareness, decision, and implementation. Because an
organization could decide either to adopt or reject a practice it was necessary to create a variable
to capture both decisions. In this way, an organization rejecting a practice would not be modeled
as a late adopting organization but rather as a distinct type of organization perhaps more
comparable to those identified as early adopters. Because we are analyzing count variables that
do not meet the distribution requirements of a Poisson distribution we utilize negative binomial
regression for all analysis. Negative binomial regression allows us to test and correct for
oversdispersion in the data (Long & Freese, 2006). Using robust standard errors adds an
additional level of conservatism in the case of high levels of underdispersion (Winkelmann,
Signorino & King, 1995)
controlling for large organizations skewing the results. In addition if an organization admired only a single quitline,
we presumed that this admiration was much more important to the organization than those admiring several
quitlines.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 23
For each dependent variable, we ran three models. In the first models (Table 3 – Models
1 & 4; Table 4 – Model 7 & 10), we included a single variable of the stage immediately prior as
a control for the general level of either awareness (in the case of adoption & rejection) or
decisions to adopt (in the case of implementation). Essentially, we are trying to control for the
possibility that organizations which are aware of more practices adopt or reject more practices
and those that adopt more implement more. This is especially important for the AWARE >
ADOPT > IMPLEMENT path because of the high and significant correlations between the
variables ranging from .64 to .71 (See Table 2).
In the second set of models (Table 3 – Models 2 & 5; Table 4 – Models 8 & 11) we add
all of our independent variables to each equation. These equations help us begin to ascertain the
effect of each variable at each stage of the innovation diffusion process while controlling for its
effect on previous stages. Second, because, we are faced with a modest number of observations
on which to conduct our analysis (a common problem for studies of whole-networks), we found
ourselves in the position of utilizing more degrees of freedom (df = 14 - 15) than is recommend
for a data set with only 60 observations. This makes us susceptible to overfitting the model
(Babyak, 2004). To determine whether or not our estimates were a result of overfitting, we ran a
third set of models (Table 3 –Models 3 & 6; Table 4 – Model 9 & 12) including only the
variables we found to be significant in the full models at the α = .10. Except for the effect of
funders ties to the NAO (fnNAO) on the likelihood of rejection, in each case the reduced model
confirmed the results found in the full models increasing our confidence in the findings. In
addition, the substantially smaller BIC statistics for these trimmed models indicate the trimmed
models are a better fit of the data.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 24
---------------------------
Table 3 & 4
---------------------------
Our hypotheses were derived from our expectation that specific information sharing
relationships and internal evaluation criteria will impact the innovation-decision at different
stages in the process. Specifically, we expected a funder‟s connections to all different types of
organizations, but most specifically the NAO (fnNAO) and top researchers (fnRESEARCH), to
play an important role in a quitline‟s awareness of the 17 evidence based practices (hypotheses
1a & 1b). We also expected a funder‟s connection to the NAO (fnNAO) and to national policy
and funding organizations (fnNATIONAL) to have an impact on the decision stage independent
of their effect on awareness because of the influence they are suspected to have on the norms
and values within the network (hypothesis 3a & 3b). In only one case, were our hypotheses
supported. Specifically, only ties to researchers (fnRESEARCH, Table 3 – Model 3) increased
the likelihood of an organization being aware of more evidence based practices and neither ties
to the NAO or to national organizations significantly impacted the likelihood of a quitline
organization adopting or rejecting an additional practice. One type of network tie that appears to
increase the likelihood of an organization rejecting evidence-based practices was connections to
more provider organizations (fnPROVIDERS). However, it is unclear why this is the case. One
explanation consistent with our understanding of power and competition (Burt, 1992) could be
that funders who communicate with multiple competing providers are better able to select the
bundle of services they feel is right for them
In addition to network connections, we expected funders actively involved in quitline
decision-making (WHODECIDES = 1) to be more active in searching out innovations thus
increasing their overall awareness (hypothesis 2). However, at the implementation stage, we
expected quitlines in which providers take an active role in decision-making (dmWHODECIDES

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 25
= 0) to have a higher rate of implementation (hypothesis 5c). Both these hypotheses were
supported (Table 3 – Model 3; Table 4 – Model 12). While funders who are more engaged in
decision-making are more likely to be aware of evidence based practices, the evidence in this
data suggests that allowing service providers to take a more active role in decision-making may
result in more complete implementation of the practices. An alternative conclusion could be that
funders who are less active in decision-making don‟t have a good sense of how well practices are
being implemented by their service providers and thus are more likely to perceive
implementation is more complete than may be accurate.
We expected the three evaluative criteria to (RATIONAL, MISSION & REPUTATION)
to have their greatest influence on the decision stage of the implementation process Specifically,
we expected concerns with efficiency (RATIONAL) to reduce the likelihood of adopting
innovations because of the use of more stringent evaluative criteria compared to those concerned
with mission fit (MISSION) or prestige (REPUTATION) (hypotheses 4a, 4b & 4c). We found
none of the variables in our analysis to influence an organization‟s decision to adopt an
innovation beyond their impact on awareness (Table 4 – Model 9). However, a number of these
factors do seem to impact a quitline‟s decision to reject a practice (Table 3 – Model 6).
Specifically, the more an organization is concerned with either MISSION or REPUTATION the
less likely they are to reject an evidence based practice which they are aware of. These findings
support or general hypotheses (4b & 4c). While concern with efficiency (RATIONAL) does not
appear to significantly impact the likelihood of either adoption or rejection, we do find that it
does significantly increase the likelihood of an organization being aware of evidence-based
practices (Table 3 – Model 3). A possible explanation for this finding consistent with our search
hypothesis could be that organizations highly concerned with obtaining evidence about

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 26
innovations perform more search activity and as a result are aware of more evidence based
practices.
Our final set of hypotheses focused on the implementation stage and the impact a
providers‟ information sharing ties might have on the process (hypotheses 5a & 5b). Specifically,
we expected providers‟ connections to other providers (prPROVIDER) and the NAO (prNAO) to
play an important role in enabling them to more successfully implement new practices. Neither
of these hypotheses was supported. However, it is not to say these connections are not important.
Rather, the analysis in model 6 (Table 3) suggests these variables are important in reducing the
likelihood of a quitline organization rejecting an evidence based practice once it becomes aware
of it. There are a number of plausible explanations for these findings. However one explanation
consistent with our arguments regarding the iterative nature of the diffusion process could be that
quitlines may only reject evidence based practices once attempts to implement the practice have
proven unsuccessful. Alternatively, providers may take information regarding capacity in to
account during the decision stage thus reducing the chance adopted innovations cannot be fully
implemented. However, these hypotheses require further investigation.
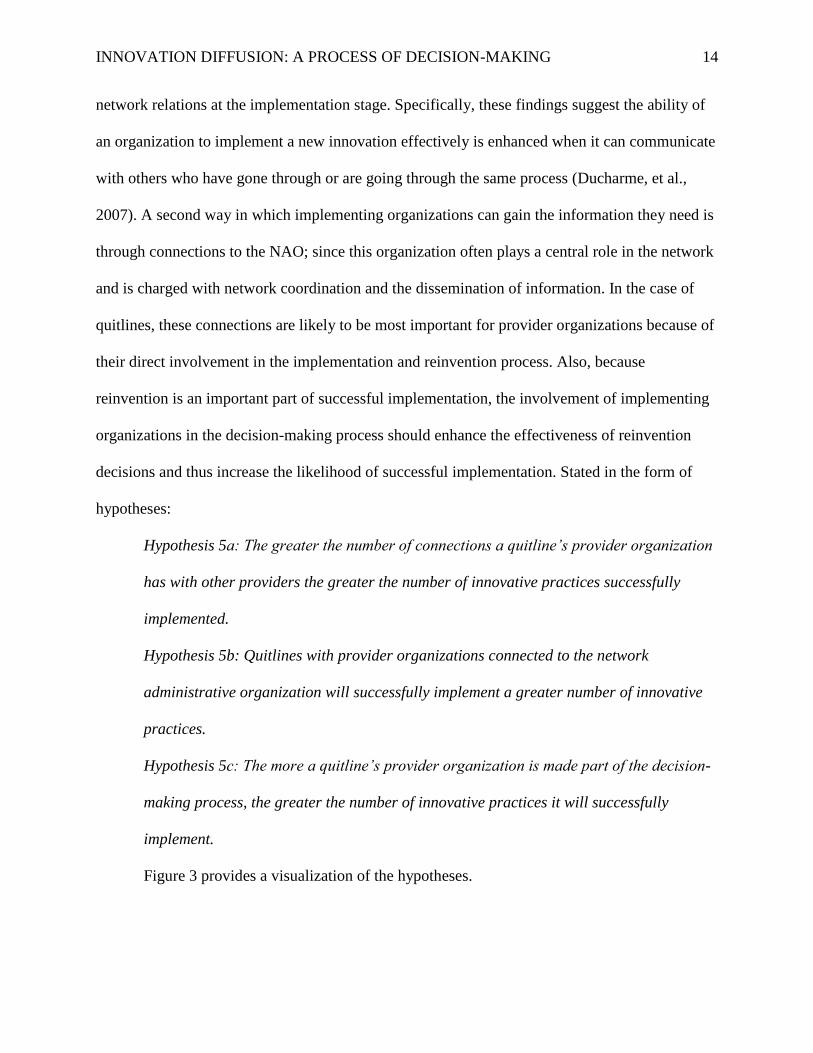
Discussion and Conclusions
Overall, 5 of our 11 hypotheses were supported. While, a number of our hypotheses were
not supported, the analysis suggests it is not because these variables are unimportant, rather the
impact of these variables manifested themselves at different stages than the ones expected (See
Figure 4 for a summary of significant relationships). Specifically, while we expected concerns
with efficiency to impact an organization‟s decision to adopt or reject an innovation our analysis
suggests a concern with efficiency is likely to impact the amount of energy invested in searching
out information and alternatives to solve problems. Additionally, we expected the providers‟

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 27
information sharing ties to enhance their „how to knowledge‟ which in turn would impact their
ability to fully implement new practices. While this may be the case, we found the significance
of these ties was manifested in an increased likelihood of adopting new practices. This leads to
multiple possible interpretations. First, consistent with our initial arguments, providers not
having adequate capacity to successfully implement a practice may be more likely to reject the
practice without attempting to implement it. Alternatively, a mimetic argument could also
explain this relationship. Specifically, providers that are more embedded within the network may
feel more pressure to adopt new practices while those on the periphery do not feel as much
pressure and may be more able to reject practices inconsistent with their goals or values.
Interestingly, funders with an increased number of ties to other providers had the opposite effect.
One possible explanation for this could be that having ties with multiple potential contracting
partners could allow funders to be more selective in the practices they decided to provide to their
constituents. The complexity of these findings, especially with regard to network ties, suggests
further work is necessary to fully understand the complexity of the innovation diffusion process.
Overall, this study has implications for both theory and practice. First, this analysis
provides support for the argument that taking a decision-making approach may be a useful way
of disentangling this complexity of innovation diffusion (Valente, 2010). Specifically, network
ties appear to impact the diffusion process in multiple ways. Ties to some organizations provide
opportunities for gaining information about the existence of new practices. Other ties may
influence the adoption decision through the transmission of normative pressures or „how to
knowledge‟. Alternatively, these same ties may provide opportunities for reducing dependency
or constraint (Burt, 1992) on a particular contracting partner. What determines the effect of these

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 28
ties is likely due in some part to the role different actors play in a network and the internal goals,
values and decision-making structure of these organizations.
For public managers, NAQC provides an important example of a public/private
collaboration where public organizations are not the central actors in the network. Rather, we see
a private network coordinator (NAO) and a cluster of private service providers filling key central
roles due to the pattern of contracting across political boundaries. This analysis also suggests that
while a funder‟s ties to researchers can help them stay informed about the innovative practices
emerging in the field of tobacco control, ties to service providers and their ties to others in the
network have a significant influence on quitline decisions to either adopt or reject these
practices. For public managers operating in the „hollow state‟ (Milward & Provan, 2000),
understanding the network dynamics within their particular policy domain and taking the
initiative to maintain relationships within this domain may help improve their ability to contract
with and monitor the service providers representing the government on the ground.
Limitations & Future Steps
This study is not without its limitations. First, the cross sectional nature of the data does
not allow us to make causal inference. Second, because we are essentially performing a case
study of one network any attempts to generalize to other networks must be done with extreme
caution. Finally, with the modest number of cases and limited qualitative data, thoughts
regarding the mechanisms underlying our observations must be corroborated with further study.
Because this is the first slice of a three year study, the findings in this study will be able
to focus our attention as we test our hypotheses over two more waves of data. In addition, the
dedication and interest of a working group of managers within the network provide us with a
forum for scrutinizing our findings for face validity. Finally, although this is a single goal-direct

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 29
„whole network‟, a number of its fundamental characteristics can be found in numerous other
examples allowing us to find future forums for us to more fully develop our understanding.
References
Anderson, C. M., & Zhu, S.H. 2007. Tobacco quitlines: Looking back and looking ahead.
Tobacco Control, 16(Suppl I), i81-i86.
Ajzen, I. (1991). The theory of planned behavior. Organization Behavior and Human Decision
Processes 50, 179-211
Babyak, M. (2004). What you see may not be what you get: A brief, nontechnical introduction to
overfitting in regression-type models. Psychosomatic Medicine, 66, 411-421.
Barnard, C.I. (1938). The Functions of the Executive. Cambridge, MA: Harvard University
Press.
Bazzoli, G.J., Casey, E., Alexander, J.A., et al. 2003. Collaborative initiatives: Where the rubber
meets the road in community partnerships. Medical Care Research and Review, 60, 63S-
94S.
Borgatti, S. P., Everett, M. & Freeman, L. 2002. Ucinet for Windows: Software for Social
Network Analysis. Harvard, MA: Analytic Technologies.
Brass, D. J., Galaskiewicz, J., Greve, H. R., & Wenpin, T. (2004). Taking stock of networks &
organizations: A multilevel perspective. Academy of Management Journal, 47, 581-629.
Broschak, Joseph P. (2004). Managers’ mobility and market interface: The effect of managers’
career mobility on the dissolution of market ties. Administrative Science Quarterly, 49,
608-640.
Burt, R. S. (1992). Structural holes: The social structure of competition. Cambridge, MA:
Harvard University Press.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 30
Burt, R.S. (2004). Structural holes and good ideas. The American Journal of Sociology, 110,
349-399.
Chaskin, R.J., Brown, P., Venkatesh, S., & Vidal, A. (2001). Building Community Capacity.
New York: Aldine de Gruyter.
Coleman, J.S., Katz, E. & Menzel, H. (1966). Medical Innovations: A Diffusion Study. New
York: Bobbs-Merrill.
DiMaggio, P. J. & Powell, W.W. (1983) The iron cage revisited: Istitutional isomorphism and
collective rationality in organizational fields. American Sociological Review, 48, 147-
160.
Ducharme, L.J., Knudsen, H.K., Roman, P.M. & Johnson, J.A. (2007). Innovation adoption in
substance abuse treatment: Exposure, trialability, and the clinical trials network. Journal
of Substance Abuse Treatment, 32, 321-329.
Ferlie, E., Fitzgerald, L., Wood, M. & Hawkins, C. (2005). The (non) spread of innovations: The
mediating role of professionals. Academy of Management Journal, 48, 117-134.
Fligstein, N. (1990). The Transformation of Corporate Control. Cambridge, MA: Harvard
University Press.
Galaskiewicz, J. & Burt, R. (1991). Interorganizational contagion in corporate philanthropy.
Administrative Science Quarterly, 36, 88-105.
Galaskiewicz, J. & Wasserman, S. (1989). Mimetic processes within an interorganizational field:
Am empirical test. Administrative Science Quarterly, 34, 454-479.Granovetter, M. 1983.
The Strength of weak ties. American Journal of Sociology, 78:1360-1380.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 31
Greenhalgh, T., Robert, G., MacFarlane, F., Bate, P. & Kyriakidou, O. (2004). Diffusion of
innovations in service organizations: Systematic review and recommendations. The
Milbank Quarterly, 82, 581-629.
Hansen, M.T. (1999). The search-transfer problem: The role of weak ties in sharing knowledge
across organization subunits. Administrative Science Quarterly, 44, 82-111.
Hansen, M. T. (2002) Knowledge networks: Explaining effective knowledge sharing in multiunit
companies. Organization Science, 13, 232-248.
Lasker, R., Weiss, E. S., & Miller, R. (2001). Partnership synergy: A practical framework for
studying and strengthening the collaborative advantage. The Milbank Quarterly, 79, 179-
205.
Leischow, S.J., Luke, D.A., Mueller, N., Harris, J.K., Ponder, P., Marcus, S., & Clark, P.I. 2010.
Mapping U.S. government tobacco control leadership: Networked for success? Nicotine
and Tobacco Research. 12(9): 888–894.
Long, J.S. and Freese, J., 2006. Regression Models for Categorical Dependent Variables using
Stata. 3rd
ed. College Station, TX: Stata Press.
Luke D.A., Harris J.K., Shelton S., Allen P., Carothers B.J., & Mueller N.B. 2010. Systems
analysis of collaboration in 5 national tobacco control networks. American Journal of
Public Health; 100(7): 1290-7.
March, J.G., & Simon, H. (1958) Organizations. New York: John Wiley and Sons, Inc.
Maurer, I. & Ebers, M. (2006). Dynamics of social capital and their performance implications:
Lessons from biotechnology startups. Administrative Science Quarterly, 51, 262-292.
Milward, H.B. & Provan, K.G. (2000). Governing the hollow state. Journal of Public
Administration Research and Theory, 10, 359-379.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 32
Owen-Smith, J. & Powell, W.W. (2004). Knowledge networks as channels and conduits: The
effects of spillovers in the Boston biotechnology community. Organization Science, 15,
5-21.
Powell, W.W., Koput, K.W., & Smith-Doerr, L. (1996). Interorganizational collaboration and the
locus of innovation: Networks of learning in biotechnology. Administrative Science
Quarterly, 41, 116-145.
Provan, K.G., Beagles, J.E. & Leischow, S.F. (2011). Network formation, governance, and
evolution in public health: The North American Quitline Consortium case. Health Care
Management Review, 36(3).
Provan, K.G., Huang, K., & Milward, H.B. (2009). The evolution of structural embeddedness
and organizational social outcomes in a centrally governed health and human services
network. Journal of Public Administration Research and Theory, 19, 873-893.
Provan, K.G. & Kenis, P. (2008). Modes of network governance: Structure, management, and
effectiveness. Journal of Public Administration Research and Theory, 18, 229-252.
Provan, K.G. & Milward, H. B. (1995). A preliminary theory of interorganizational network
effectiveness: A comparative study of four community mental health systems.
Administrative Science Quarterly, 40, 1-33.
Provan, K.G., Fish, A., & Sydow, J. (2007). Interorganizational networks at the network level: A
review of the empirical literature on whole networks. Journal of Management , 33, 479-
516.
Rao H., Davis, G. F., & Ward, A. (2000) Embeddedness, social identity and mobility: Why firms
leave the NASDAQ and join the New York Stock Exchange. 45, 268-292.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 33
Reagans, R., & McEvily, B. (2003). Network structure and knowledge transfer: The effects of
cohesion and range. Administrative Science Quarterly, 48, 240-267.
Rogers, E.M. (2003). Diffusion of Innovations. New York: Free Press.
Ryan, B. & Gross, N. (1943). The diffusion of hybrid corn seed in two Iowa communities. Rural
Sociology, 8:15-24.
Simon, H. (1997). Administrative behavior (4th
ed.). New York: The Free Press (Original work
published 1945).
Tsai, W. (2001). Knowledge transfer in intraorganizational networks: Effects of network position
and absorptive capacity on business unit innovation and performance. Academy of
Management Journal, 44, 996-1004.
Wejnert, B., (2002) Integrating models of diffusion of innovations: A conceptual framework.
Annual Review of Sociology, 28, 297-326.
Westphal, J.D. Gulati, R & Shortell, S. M. (1997) Customization or conformity? An institutional
and network perspective on the content and consequences of TQM adoption.
Administrative Science Quarterly, 42, 366-394.
Winkelmann, R., Signorino, C. S. & King, G. (1995). A correction for an underdispersed event
count probability distribution. Political Analysis, 5, 215-228
Valente, T., (2010) Social networks and health: Models, methods, and applications. Oxford:
Oxford University Press.

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 34
Figure 1. Network of Information Receipt within the North American Quitline Consortium
Funders Providers NAO Researchers Non-Quitline Members
Information Receipt Intensity Level High

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 35
Figure 2. Comparison of Frameworks
Figure 3. Hypotheses & Variables

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 36
Figure 4. Significant Relationships

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 37
Table 1
Coding of Dependent Variable
Q1
„No‟ „Yes‟
AWARE 0 1
Q2
Not Yet
Discussed
In
Discussion
Decided
NOT to
Implement
Decided
to
Implement
REJECT 0 0 1 0
ADOPT 0 0 0 1
Q3
No
Progress Low Medium High
Fully
Implemented
IMPLEMENT 0 0 0 1 1
Table 2
Correlations and Descriptive Statistics
Mean SD 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
1 UNAWRE 2.40 2.34 -
2 REJECT .92 1.55 -.32 -
3 ADOPT 12 1.89 -.64 -.24 -
4 IMPLEMENT 10.56 1.99 -.50 -.12 .71 -
5 SPEND 2.73 2.26 -.23 .09 .16 .20 -
6 fnNAO .55 .50 -.25 -.14 .18 .06 .01 -
7 fnFUNDERS 1.93 3.07 -.06 .03 .11 .05 -.21 -10 -
8 fnPROVIDERS 1.30 .93 -.13 .08 .08 -.06 .06 .08 .25 -
9 fnNATIONAL 1.02 1.02 -.15 .14 .16 .11 -.03 -.15 .26 .34
10 fnRESEARCH 2.62 1.89 -.37 .17 .31 .28 -.02 .12 .27 .29 .47 -
11 WHO DECIDES .57 .50 -.33 -.03 .32 .00 .03 .02 .21 .21 .21 .11 -
12 RATIONAL 4.63 .43 -.07 .18 -.03 .07 -.13 -.03 -.11 -.06 -.15 -.16 -.16 -
13 MISSION 3.96 .77 -.07 -.18 .24 .11 .13 -.24 -.02 .14 .15 .09 .02 .08 -
14 REPUTATION 5.23 8.18 -.17 -.18 .16 .04 -.03 .33 .11 .36 .03 .26 .30 -.24 -.08 -
15 prNAO .78 .42 -.17 -.13 .19 .20 .18 .01 -.08 .13 .21 .07 .11 .01 .20 -.16 -
16 prPROVIDER 2.63 1.77 -.12 -.20 .33 .20 .03 .19 -.08 .01 .08 .25 .12 -.04 .23 .01 .31
BOLD p < .05, ITALIC p < .10

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 38
Table 3
Negative Binomial Estimation of Unawareness and Rejection
UNAWARE REJECT
Base Full Trimmed Base Full Trimmed
Model1 Model 2 Model 3 Model 4 Model 5 Model 6
coef. s.e. coef. s.e. coef. s.e. coef. s.e. coef. s.e. coef. s.e.
UNAWRE -.30 .17 -.58 .15 -.51 .09
SPEND -.09 .03 -.10 .03 .03 .04
fnNAQC -.40 .26 -.68 .37 -.58 .37
fnFUNDERS -.02 .03 -.01 .04
fnPROVIDERS .10 .16 .55 .18 .54 .23
fnNATIONAL .10 .17 .30 .19
fnRESEARCH -.28 .11 -.23 .08 -.03 .14
WHODECIDE -.74 .24 -.67 .23 -.67 .59
RATIONAL -.51 .30 -.55 .27 .23 .50
MISSION -.04 .17 -.78 .20 -.60 .20
REPUTATION .01 .02 -.13 .04 -.15 .05
prNAQC -.34 .27 -.78 .29 -.84 .42
prPROVIDER .06 .07 -.19 .08 -.18 .08
Constant 4.65 1.38 4.51 1.29 .43 .24 3.87 2.80 4.19 .75
alpha .26 .16 .32 .17 1.28 .73 .00 .00 .11 .40
Wald chi2 37.50 34.64 3.38 100.88 81.05
BIC 277.47 249.50 160.76 174.40 156.44
-2LL -123.84 -110.08 -112.47 -74.24 -56.49 -59.79
df 0 14 6 3 15 9
BOLD = p ≤ .05, Italics p ≤ .10; robust (s.e.)

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 39
Table 4
Negative Binomial Estimation of Adoption and Implementation
ADOPT IMPLEMENT
Base Full Trimmed Base Full Trimmed
Model 7 Model 8 Model 9 Model 10 Model 11 Model 12
coef. s.e. coef. s.e. coef. s.e. coef. s.e. coef. s.e. coef. s.e.
UNAWRE -.04 .00 -.04 .01 -.04 .01 .07 .01 .08 .01 .08 .01
SPEND .00 .00 .01 .01
fnNAQC .01 .03 -.04 .04
fnFUNDERS .01 .00 .00 .01
fnPROVIDERS -.02 .02 -.02 .02
fnNATIONAL .00 .02 .01 .02
fnRESEARCH .00 .01 .01 .01
dmWHO .03 .04 -.11 .04 -.10 .04
dmRATIONAL -.01 .04 .05 .05
dmMISSION .04 .03 -.03 .02
REPUTATION .00 .00 .00 .00
prNAQC -.00 .04 .06 .04
prPROVIDER .02 .01 .02 .01 -.00 .01
Constant 2.59 .02 2.41 .54 2.52 .03 1.48 .12 1.30 0.24 1.43 .13
alpha .00 .00 .00 .00 .00 .00 .00 .00 .00 .00 .00 .00
Wald chi2 45.62 176.84 59.13 50.84 82.99 53.67
BIC 278.27 325.30 281.25 271.35 317.74 274.05
-2LL -135.04 -133.99 -134.48 -131.58 -130.21 -130.88
df 2 14 3 2 14 3
BOLD = p ≤ .05, Italics, p ≤ .10; robust (s.e.)

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 40
Appendix
Appendix A. List of Practices
Innovative Practices Identified by NAQC NAO and ‘Project Working Group’
Practices Used in Analysis
Proactive (outbound) counseling
Reactive (inbound) counseling
Multiple call protocol
Conduct mass media promotions for the mainstream population
Conduct mass media promotions for targeted populations
Provide self-help materials to proxy callers
Provide self-help materials for tobacco users regardless of reason for calling
Provide self-help materials for tobacco users who receive counseling
Provide counseling immediately to all callers who request it
Conduct an evaluation of the effectiveness of the quitline
Refer callers with insurance to health plans that provide telephone counseling
Use text messaging
Integrate phone counseling with web-based programs
Fax referral programs
Re-contact relapsed smokers for re-enrollment in quitline services
Supplement quitlines services with IVR services
Train provider groups on 2A's or 3A's and refer
US Specific Practices
Serve callers without insurance coverage
Obtain Medicaid or other insurance reimbursement
Pharmacological Practices
Provide NRT without requiring counseling
Provide NRT but require counseling
Practices lacking Evidence of Effectiveness
Staff the quitline with counselors who meet or exceed Masters-level training
Integrate phone counseling with face-to-face cessation services

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 41
Appendix B. Decision-making Questions
Strongly
Disagree
Strongly
Agree
Don‟t
Know
1. Strong evidence of effectiveness was an important
consideration. 1 2 3 4 5 6
2. The overall financial cost of the quitline practices
was extremely important. 1 2 3 4 5 6
3. A critical consideration was whether or not these
quitline practices were consistent with <auto-fill
organization‟s name>‟s mission.
1 2 3 4 5 6
4. Opinions of others in <auto-fill organization‟s
name>, such as staff or other decision makers,
strongly influenced the decision to adopt or not
adopt these quitline practices.
1 2 3 4 5 6
5. Dealing with and overcoming bureaucratic
procedures (e.g., rules, red-tape, etc.) was a
significant barrier to the adoption of these quitline
practices.
1 2 3 4 5 6
6. The decision was based on the expertise of current
staff to implement the quitline practices effectively. 1 2 3 4 5 6
7. <Auto-fill organization‟s name> tries not to pay
much attention to cost when considering adopting a
new quitline practice.
1 2 3 4 5 6
8. The practices used by well-respected quitlines in
other states and provinces were important
considerations in our decision process.
1 2 3 4 5 6
Not Very
Important
Very
Important
Don‟t
Know
9. When considering the adoption of these quitline
practices, pressure or mandates from major outside
organizations, like other levels of government,
agencies such as CDC, Health Canada, national
advocacy groups, etc. were
1 2 3 4 5 6
10. Being among the first to adopt a new quitline
practice was 1 2 3 4 5 6
11. When considering the adoption of these quitline
practices, <auto-fill vendor if respondent‟s
organization is the funder; funder if respondent‟s
organization is the vendor>‟s opinion was
1 2 3 4 5 6
12. Whether most other quitlines had adopted or not
adopted these quitline practices was 1 2 3 4 5 6

INNOVATION DIFFUSION: A PROCESS OF DECISION-MAKING 42
Appendix C. Decision-making Factor Analysis
dmRational
dmMISSION
Variable Factor1 Factor2 Factor3 Uniqueness
q1 effective 0.6029 -0.0280 -0.0703 0.6307
q2 cost 0.7358 0.1164 0.0801 0.4387
q3 mission -0.0611 0.1969 0.6510 0.5337
q4 opinion 0.1603 -0.0413 0.6432 0.5589
q5 redtape 0.3739 -0.3129 0.1983 0.7229
q6 expertise 0.0815 0.4107 0.2480 0.7631
q7rv nocost 0.3324 -0.0831 0.0076 0.8826
q8 otherlrspct 0.1258 0.6180 0.2169 0.5552
q9 mandates -0.1236 0.3059 0.2425 0.8324
q10 first -0.3987 0.1524 -0.0848 0.8106
q11 opinion 0.0012 0.4903 -0.1220 0.7448
q12 othermny -0.0543 0.5131 0.0268 0.7331
alpha 0.6624 0.5809 0.6762 Bold – Factor loading ≤ .40





























