Embed Size (px)
Citation preview

Foot and Ankle Surgery 1999 5: 267–270
Revision lateral ankle ligament reconstructionusing Achilles tendon graft: a case report
B.S. THORNES AND M.M. STEPHENS∗Merlin Park Regional Hospital, Galway and ∗Cappagh Orthopaedic Hospital, Finglas,Dublin, Ireland
SummaryThis report is of a patient with chronic ankle instability, who
underwent revision lateral ligament reconstruction using a graft
from the lateral quarter of the Achilles tendon. The split peroneus
brevis tendon had failed following a previous Evan’s procedure. It
illustrates the use of the lateral quarter of the Achilles tendon as a
graft for reconstruction and illustrates its benefit for revision lateral
ankle ligament reconstruction surgery.
Keywords: ankle instability; revision; stabilization; Achilles tendon;
surgery
Introduction
Operative management of a chronically unstable
ankle is indicated following failure of conservative
functional treatment. Many procedures have been
described to primarily repair or reconstruct the torn
ligament complex. There is little literature regarding
revision surgery following failed primary
reconstruction or re-injury. As many primary
procedures harvest the peroneus brevis tendon as a
graft, a viable substitute must be sought in revision.
We present the case of a patient who required revision
surgery to stabilize his ankle, whose tendon of
peroneus brevis previously had been used. The
patient achieved an excellent result following revision
reconstruction with a graft from the lateral quarter
of the Achilles tendon.
Case historyFigure 1Preoperative stress anteroposterior ankle radiograph showing talarThe patient, a 46-year-old printer and recreationaltilt of 15°.
golfer, presented to the foot and ankle clinic with a
long history of right ankle instability. He had aCorrespondence: Mr M.M. Stephens MSc (Bio Eng) FRCSI,
severe inversion injury to his ankle at age 18, playingConsultant Orthopaedic Surgeon, Cappagh Orthopaedic Hospital,
Finglas, Dublin 11, Ireland (e-mail: [email protected]). football, and 2 years later had a lateral ligament
267 1999 Blackwell Science Ltd
268 B.S. THORNES AND M.M. STEPHENS
reconstruction performed with the Evan’s procedure,
using the split peroneus brevis tendon. He does
not recall a second significant injury to his ankle
following this surgery, but he presented on this
occasion with progressive pain in his ankle and
recurrent giving way.
Clinically, there was a painless laxity on inversion
stress and on anterior drawer testing, confirmed by
stress radiographs (Fig. 1). These revealed a talar tilt
of 15°. There were also Scranton [1] grade II anterior
tibial osteophytes.
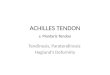
Operative procedureFigure 2Reconstruction using the Achilles tendon.
Through an extended lateral approach, with the sural
nerve being identified and preserved, the ankle joint
was inspected and the anterior tibial osteophytes
excised. A grade III osteochondral flap Postoperative course(3 mm×3 mm) was found on the lateral margin of
The postoperative course was uneventful. The patientthe talar dome and this was debrided and drilled.was discharged home on the fifth postoperative day,Remnants of the old reconstruction were evident,non-weight bearing for 3 weeks, then partial weightincluding a torn split peroneus brevis graft and distalbearing in case for a further 3 weeks. The scotch casefibular tunnel. There was no useful peroneus breviswas removed at 6 weeks and full weight bearing intendon that could be used for reconstruction.an ankle-foot orthosis (AFO) commenced. At 10The lateral 25% of the Achilles tendon wasweeks the AFO was removed and the ankle washarvested, split from its musculo-tendinous junctionpain-free and clinically stable.at the mid-calf level, retaining its distal insertion to
calcaneus intact. This gave a graft length of≈15 cm.
Starting on the posterosuperior extra-articularDiscussion
portion of the calcaneus and exiting at the peroneal
tubercle, a horizontal tunnel through the calcaneus The lateral ligament complex includes the anteriorwas drilled and smoothed with a burr and the graft talo-fibular ligament, the calcaneo-fibular ligamentthreaded through it. A new tunnel was made through and the stronger posterior talo-fibular ligament.the distal fibula to allow a more accurate anatomic Acute injury to the anterior talo-fibular ligament is by
reconstruction. The graft was threaded through from far the most common, and accounts for a significant
posterior tip of the lateral malleolus to its anterior number of casualty attendances in Ireland [2, 3]. It
aspect. The graft was then brought through a tunnel is estimated that between 10% to 30% of acute injuries
from the anterolateral talus to the sinus tarsi, insertion will develop chronic symptoms of instability [4].
point of anterior talo-fibular ligament and then re- Stress radiographs confirm the diagnosis of ankle
sutured onto itself. In this way the calcaneo-fibular, instability. A talar tilt of ≥10°, as compared to the
anterior talo-fibular and lateral talo-calcaneal other side, or an anterior drawer of ≤6 mm, or
ligaments were reconstructed in an anatomical 3 mm greater than the other side, are diagnostic [5].
position (Fig. 2). Magnetic resonance imaging (MRI) is increasingly
The wound was closed over a closed suction drain. being used in the diagnosis of ankle ligament injuries
A below-knee scotch cast was applied with the ankle [6]. They have the advantage of being useful to grade
an acute injury and to diagnose other causes ofin slight eversion and dorsiflexion.
1999 Blackwell Science Ltd, Foot and Ankle Surgery, 5, 267–270

REVISION LATERAL ANKLE LIGAMENT RECONSTRUCTION 269
chronic lateral ankle instability, such as soft tissue as a primary procedure in nine patients, citing the
advantage of not sacrificing the dynamic effect ofimpingement, tendon pathology or osteochondral
lesions. MRI is most useful in the evaluation of high peroneus brevis in preventing inversion of the foot,
but this tendon is relatively small. Rudert et al. [16]demand patients such as professional athletes.
Many procedures for lateral ligament used regional perisosteal flaps to anatomically
reconstruct the anterior talo-fibular and calcaneo-reconstruction have been described, as a result there
is no agreed gold standard procedure. Surgical fibular ligaments. This spares the peroneus brevis
tendon and gave a good to excellent result in 81% ofprocedures can be subdivided in two main ways:
anatomic versus non-anatomic reconstructions, using 90 patients. Primary anatomical reconstruction using
periosteal flaps yielded a better functional outcomeautogenous or synthetic grafts.
Anatomic repair of torn ligaments has been compared to a non-anatomical peroneus brevis
ligamentoplasty in a recent study [19].described by Brostrom [7] which gives good results in
the short-term and has the advantage of not altering There is little literature regarding revision ligament
reconstructive surgery. Sammarco [20] reported onankle biomechanics and through the extensor
retinaculum the subtalar joint can be stabilized [8]. a series of 10 revision procedures, including three
revision Brostrom-type repairs, seven of which usedIn the acute injury conservative functional treatment
is found to be as effective as early operative repair peroneus brevis or plantaris tendon as a graft. All
had good results. Patients with acute injuries should[9]. However, if symptoms of chronic instability
occur, after rehabilitation and a proprioceptive initially be treated conservatively with functional
rehabilitation. If chronic instability develops, primaryprogramme, primary anatomic repair of the torn
ligaments using the Brostrom procedure is probably suturing using the Brostrom procedure should first be
considered. If this fails or is not possible, ligamentousthe treatment of choice [10].
Non-anatomic reconstructions usually use either reconstruction should be performed such as the
Chrisman–Snook technique. If a second injury occursa complete or split portion of the peroneus brevis
tendon. These include the Evan’s procedure [11], and leads to instability, we suggest harvesting the
lateral portion of Achilles tendon as a graft forthe Watson–Jones procedure [12] and the
Chrisman–Snook procedure [13]. Other techniques revision reconstruction when peroneus brevis has
been previously used, because the results arehave been described using grafts from Achilles
tendon [14], plantaris [15], or from a regional flap of excellent, particularly compared to synthetic
materials.periosteum [16].
Reconstructions using peroneus brevis tendon
should be considered after a failed Brostrom repair, Referencesin a hypermobile foot, or if the time from injury to
1 Scranton PE, McDermott JE. Anterior tibiotalar spurs: arepair is greater than 10 years. There is little to choose
comparison of open versus arthroscopic debridement. Foot Anklebetween the different procedures, all offering good 1992; 13: 125–129.
2 Flood HD, Mira AG. A review of sports injuries seen in theresults [17]. The Chrisman–Snook procedure did givecasualty department. Ir J Med Sci 1985; 154: 270–273.a slightly more stable ankle on biomechanical testing
3 Burke P, Buckley N, McShane D et al. Sports injuries and thebut may result in decreased inversion and sub-talar casualty department. Ir Med J 1983; 76: 127–129.
4 Trevino SG, Davis P, Hecht PJ. Management of acute andmotion [18].chronic lateral ligament injuries in the ankle. Ortho Clin N AmSolheim et al. [14] described a method of1994; 25: 1–16.
reconstruction using the Achilles tendon. He used5 Stephens MM. Hindfoot laxity: ankle or subtalar joint or both?
the medial third of Achilles tendon to reconstruct Foot Dis 1994; 1: 111–115.
6 O’Farrell DA, McCabe JP, Curtin B et al. Use of magneticthe lateral ligament in 30 patients, with satisfactoryresonance imaging and scintigraphy for diagnosis of
results in 29. The procedure also stabilizes theosteochondral fractures in acutely sprained unstable ankles. J
subtalar joint and corrects recurrent subluxation Foot Ankle Surg 1996; 2: 209–214.
7 Brostrom L. Sprained ankles. VI: Surgical treatment of chronicof the peroneal tendons. However, for a primaryligament ruptures. Acta Chir Scand 1966; 132: 551–565.procedure it requires greater dissection particularly
8 Stephens MM, Sammarco GJ. The stabilizing role of the lateralbecause it harvests the medial portion of the Achilles ligament complex around the ankle and subtalar joints. Foot
Ankle 1992; 13: 130–136.tendon. Anderson [15] used the plantaris tendon
1999 Blackwell Science Ltd, Foot and Ankle Surgery, 5, 267–270

270 B.S. THORNES AND M.M. STEPHENS
9 Moller-Larsen F, Wethelund JO, Jurik AG et al. Comparison of 15 Anderson ME. Reconstruction of the lateral ligaments of the
ankle using the plantaris tendon. J Bone Joint Surg 1985; 67A:three different treatments for ruptured lateral ankle ligaments.
Acta Ortho Scand 1988; 59: 564–566. 930–934.
16 Rudert M, Wulker N, Wirth CJ. Reconstruction of the lateral10 Evans GA, Hardcastle P, Frenyo AD. Acute rupture of the
lateral ligament of the ankle: to suture or not to suture? J Bone ligament of the ankle using a regional periosteal flap. J BoneJoint Surg 1997; 79B: 446–451.Joint Surg 1984; 66B: 209–212.
11 Karlsson J, Bergsten T, Lansinger O et al. Lateral instability of 17 Liu SH, Baker CL. Comparison of lateral ligamentous
reconstruction procedures. Am J Sports Med 1994; 22: 313–317.the ankle treated by the Evan’s procedure: a long-term clinical
and radiological follow-up. J Bone Joint Surg 1988; 70B: 476–480. 18 Hollis JM, Blasier RD, Flahiff CM et al. Biomechanical
comparison of reconstruction techniques in simulated lateral12 Watson-Jones R. Recurrent forward dislocation of the ankle
joint. J Bone Joint Surg 1952; 34B: 519–000. ligament injury. Am J Sports Med 1996; 23: 678–682.
19 Mabit C, Chaudruc JM, Fiorenza F et al. Lateral ligament13 Snook GA, Chrisman OD, Wilson TC. Long-term results of the
Chrisman–Snook operation for reconstruction of the lateral reconstruction of the ankle: comparative study of peroneus
brevis tenodesis versus periosteal ligamentoplasty. J Foot Ankleligaments of the ankle. J Bone Joint Surg 1985; 67A: 1–7.
14 Solheim LF, Denstad TF, Roaas A. Chronic lateral instability Surg 1998; 4: 71–76.
20 Sammarco GJ, Carrasquillo HA. Surgical revision after failedof the ankle: a method of reconstruction using the Achilles
tendon. Acta Ortho Scand 1980; 51: 193–196. ankle reconstruction. Foot Ankle Int 1995; 16: 748–753.
1999 Blackwell Science Ltd, Foot and Ankle Surgery, 5, 267–270