Embed Size (px)
Citation preview

Central Annals of Otolaryngology and Rhinology
Cite this article: Hui LR, Selamat M, Hamid Z, Abu Bakar AZ, Thomas TH (2016) Retropharyngeal Abscess in Child – Dilemma in Airway Management. Ann Otolaryngol Rhinol 3(11): 1141.
*Corresponding author
Lo Ren Hui, Department of Otorhinolaryngology, Hospital Ampang, 68000 Selangor, Malaysia, Tel: 60-123486938; Fax 603-42954666; Email:
Submitted: 13 September 2016
Accepted: 12 October 2016
Published: 14 October 2016
ISSN: 2379-948X
Copyright© 2016 Hui et al.
OPEN ACCESS
Keywords•Retropharyngeal abscess•Airway management•Pediatric
Case Report
Retropharyngeal Abscess in Child – Dilemma in Airway ManagementLo Ren Hui1*, Mazlina Selamat1, Zubaidah Hamid1, Azreen Zaira Abu Bakar1, and Tristan Hilary Thomas2 1Department of Otorhinolaryngology, Hospital Ampang, Malaysia2Department of Radiology, Hospital Ampang, Malaysia
Abstract
Retropharyngeal abscesses in pediatric is becoming increasingly rare with the availability and advancement of broad spectrum antibiotics in recent years. It is a life-threatening emergency condition because it can lead to airway compromise and induce other catastrophic complications. We report a child with supraglotitis which was then complicated with an extensive retropharyngeal abscess.
INTRODUCTIONRetropharyngeal abscess is a deep neck space infection that
usually affects mostly young children [1]. It is an abscess which involves space that extends from base of skull to the mediastinum at the level of first and second thoracic vertebrae, anteriorly bordered by buccopharyngeal fascia, laterally by carotid sheath and posteriorly by deep cervical fascia draining upper aero digestive tract. Retropharyngeal abscess incidence is declining because of the common use of antibiotic and improvement in medical care for which commonly caused by upper respiratory infection, commonly Staphylococcus Aureus and Group A Streptococcus [2,3]. Predominantly male (2:1) with seventy percent of the patients are younger than six years of age [4].
CASE PRESENTATIONA fifteen months old previously healthy girl presented with
one week history of upper respiratory tract infection and later developed supraglottitis. She was electively intubated and responded well with intravenous Ceftriaxone. She was discharged well after completion of seven days of antibiotic. Unfortunately two days later, she developed noisy breathing and reduced oral intake. On examination, there were audible stertor and child was mildly tachypnoeic with stable vital signs. There was no obvious neck swelling seen or palpable on inspection and neck palpation respectively. Fiber optic examination showed right retropharyngeal bulge extending from the level of nasopharynx to the tip of epiglottis. She was breathing with good oxygen saturation even though the laryngeal inlet could not be visualized at all due to the retropharyngeal bulge.
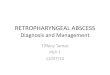
Immediate CT scan was done, showing a large rim enhancing retropharyngeal collection, extending from the base of skull until C7 vertebral body measuring 2x4.6x5.2cm (Figure 1) with multiple enlarged cervical lymph nodes. The airway appears
narrowed at the supraglottic region at the level of hyoid bone (Figure 2).
Patient was planned for immediate incision and drainage in view of impending airway compromised. Intubation was successful with single attempt without rupturing the abscess. Intraoral incision was made at the most bulging part of the posterior pharyngeal wall, and drained about ten milliliters of pus. Post operatively was uneventful.
She was kept intubated for three days to secure the airway while awaiting the supraglottic edema to subside. The culture did not show any growth. Patient was discharged well after completing seven days of intravenous Tazocin and Clindamycin.
Figure 1 This is the contrast enhanced CT scan sagittal view of the patient showing extensive retropharyngeal abscess, occluding the airway.

Central
Hui et al. (2016)Email:
Ann Otolaryngol Rhinol 3(11): 1141 (2016) B/1
DISCUSSION Retropharyngeal abscess is a potentially life threatening
deep neck abscess disease. The initial presenting symptoms, especially in children are usually nonspecific. It includes neck pain (38%), fever (17%), sore throat (17%) and poor oral intake [5]. Only five percent retropharyngeal abscess patient presented with stridor [5]. The number of reported cases is increasing in various centres [6]. This rise is probably due to early detection of the disease because of improved access to investigation tools [7]. Most of the cases can easily being unnoticed and worsened due to high variation of presentation of the disease. Therefore, high suspicious of the possible retropharyngeal abscess should always be ruled out in any of the patients with the above presenting symptoms.
The most likely cause of the abscess in this patient is probably supraglotitis complicated with retropharygeal suppurative lymphadenitis. It has been postulated that younger children are more likely to develop infections in this area because of the presence of lymph nodes that run in a paramedian chain in the retropharyngeal space and will spontaneously regress after five years [7].
CT scan is considered to be the imaging of choice in diagnosing retropharyngeal abscess. It is highly sensitive in diagnosing an abscess (92%) even though it is not specific [8]. Surgical intervention is recommended in patients who has positive CT scan finding. In this patient, surgical drainage was indicated in view of the abscess collection has already worsened as shown in the CT scan and might soon compromise the upper airway completely due to inability to see a normal laryngeal inlet during an awake fibreoptic nasopharyngolaryngo scope.
Treating a retropharyngeal abscess, especially in children is challenging. Mortality was reported as high as 6.7 to 15 percent in younger age group before the wide usage of broad spectrum antibiotic [9]. In early abscess, some patient may respond well with intravenous antibiotic alone [10]. However, sole intravenous
antibiotic treatment for retropharyngeal abscess might slow down patient’s recovery compare to surgical intervention [4]. Apart from having a greater risk of compromised airway, the abscess might even ruptured spontaneously causing potentially fatal event [4].
In this patient, securing an airway before surgery was in the dilemma. Oral intubation may either fail or it may rupture the abscess causing aspiration to the lung as the airway is likely to be distorted with edema and laryngeal displacement [11]. Tracheostomy in pediatric under gas inhalation or local anesthesia is not a worthy option to be considered, furthermore with the probable associate complication and post operative care. Hence, a good communication with an anesthetist is important for the patient’s best outcome which varies from patient to patient.
The child was able to lie down supine without any sign of airway obstruction or respiratory depression overnight. Therefore, a trial of oral intubation by the anesthetic team in operation theatre was decided with otorhinolaryngology team stand by as anticipating difficult airway and potential emergency tracheostomy for acute airway obstruction. The patient was induced with inhalational gas without muscle relaxant and allowed for spontaneous breathing. Good tidal volume and chest expansion was observed. Lower head down position was ordered to prevent any pus aspiration into the larynx in case the abscess is ruptured during manipulation of intubation [11]. Finally, the child was successfully intubated with a single attempt without any difficulty and morbidity. Intraoral incision and drainage of the abscess was uneventful.
CONCLUSIONSManagement of retropharyngeal abscess in children is
challenging, especially when planning to secure the airway preoperatively. Thus, early detection of the disease with a good collaboration from a multidiscipline department is essential in preventing any morbidity or mortality from a life threatening acute upper airway disease.
ACKNOWLEDGEMENTSThe manuscript was accepted as a poster presentation
at: 36th Annual General Meeting of The Malaysian Society of Otorhinolaryngologists, Head and Neck Surgeons in conjuction with two international ENT meetings, the 8th Malaysian International Congress on Otorhinolaryngology and 18th Asian Research Symptosium in Rhinology in Kuala Lumpur, Malaysia on 26th to 28th May 2016.
REFERENCES1. Jain S, Kumar S, Kumar N, Puttewar MP, Nagpure PS. Deep-neck space
infections – a diagnostic dilemma. Indian J Otolaryngol Head Neck Surg. 2008; 60: 349-352.
2. Al-Sabah B, Bin Salleen H, Hagr A, Choi-Rosen J, Manoukian JJ, Tewfik TL. Retropharyngeal Abscess in Children:10-year study . J Otolaryngol. 2004; 33: 352-355.
3. Singh R, Guptha R, Jain A, Vajifdar H. Anaesthesia management of paediatric retropharyngeal abscess our experience. Journal of Anaesthesia and Clinical Pharmacology. 2008; 24: 57-60.
4. Kirse DJ, Robserson DW. Surgical management of retropharyngeal
Figure 2 CT scan axial view of the neck at the hyoid level showing the abscess with rim enhancement.

Central
Hui et al. (2016)Email:
Ann Otolaryngol Rhinol 3(11): 1141 (2016) 3/3
Hui LR, Selamat M, Hamid Z, Abu Bakar AZ, Thomas TH (2016) Retropharyngeal Abscess in Child – Dilemma in Airway Management. Ann Otolaryngol Rhinol 3(11): 1141.
Cite this article
space infections in children. Laryngoscope. 2001; 111: 1413-1422.
5. Craig FW, Schunk JE. Retropharyngeal Abscess in Children: Clinical Presentation, utility of Imaging, and Current Management. Pediatrics 2003; 111: 1394-1398.
6. Wong DK, Brown C, Mills N, Spielmann P, Neeff M. To drain or not to drain - Management of pediatric deep neck abscesses: A case-control study. Int J Pediatr Otorhinolaryngol. 2012; 76: 1810-1813.
7. Grisaru-Soen G, Komisar O, Aizenstein O, Soudack M, Schwartz D, Paret G. Retropharyngeal and parapharyngeal abscess in children – Epidermiology, clinical features and treatment. Int J Pediatr Otorhinolaryngol. 2010; 74: 1016-1020.
8. 8. Page NC, Bauer EM, Lieu JE. Clinical features and treatment of retropharyngeal abscess in children. Otolaryngology-Head and Neck Surg. 2008; 138: 300-306.
9. 9. Richards L. Retropharyngeal absces. N Engl J Med. 1936; 215: 1120-1130.
10. Plaza Mayor G, Martínez-San Millán J, Martínez-Vidal A. Is Conservative treatment of deep neck space infections appropriate. Head Neck. 2001; 23: 126-133.
11. Manjula Sudhakar Rao, YK Linga Raju, PN Vishwanathan. Anesthetic management of difficult airway due to retropharyngeal abscess. Indian J Anaesth. 2010; 54: 246-248.