Embed Size (px)
Citation preview

Pakistan Journal of Otolaryngology 2014; 30 : 29-31
Candida Albicans Retropharyngeal Abscess
INTRODUCTION: Retropharyngeal abscess is apotentially sinister deep neck infection especially amongimmunosuppressed individuals such as in diabetesmellitus patients. It is because of the suppressedimmunity status, which makes them prone to developserious complications such as mediastinitis and jugularvein thrombosis. Bacteria are by far the commonestorganism involved in the pathogenesis. Anaerobes,aerobes and Gram negative organisms were usuallyidentified on culture of the drained pus. The commonlyisolated organisms include Group A Beta-hemolyticstreptococci and Staphylococcus aerius1,2. Fungal agentswere rarely reported as a cause of retropharyngealabscess.CASE REPORT: A 67 year old Malay male withunderlying diabetes mellitus on medication presentedwith complaint of difficulty in swallowing for two weeks.He had odynophagia and was unable to tolerate solidfood and even fluids. It was associated with the presenceof left neck swelling which was noticed one week priorto admission. He claimed that the swelling was increasingin size. A day prior to admission, he had coughed outyellowish pus mixed with saliva. He denied hoarsenessof voice and breathing difficulty. There was no loss ofappetite and no loss of weight. Clinical examination
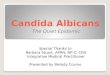
showed a medium built man who appeared to becomfortable in supine position. He had no drooling ofsaliva and no respiratory distress. Blood pressurerecording was 110/80 mmHg, pulse rate was 80 beatsper minutes and he was afebrile. There was a diffuseleft lateral neck swelling which extended to the anteriorpart of neck (Figure 1a and 1b). It was tender, warmand fluctuant. There was no trismus. Oropharyngealexamination revealed an erythematous and bulgedposterior pharyngeal wall with uvula deviation to theright side. The patient was edentulous and oral hygienewas fair. Laryngoscopic examination revealed a bulgedarea over the right pyriform fossa with pooling of salivaand pus. Epiglottis was normal while vocal cords werenot visualized. Blood investigation showed total whiteblood cell count of 8.3 x 109 /L and hemoglobin level of12.9 g/dl. Blood sugar level was 7.2 mmol/ L. Tuberculintest was negative. Lateral soft tissue neck x-ray revealedwidening of prevertebral soft tissue at level C1 to C7with presence of air pockets (Figure 2). A computedtomography (CT) scan showed presence of an ill definedthin rim-enhancing hypodense collection (Figure 3a and3b). The lesion involved retropharyngeal region extendinginto prevertebra space from level C1 to T4/T5 causingbulging into oropharynx, which consequently resulted
Department of Otolaryngology, Head and Neck Surgery, School of Medical Sciences, Universiti Sains Malaysia,
ABSTRACT: Retropharyngeal abscess is a potentially lethal deep neck infection, which is usually causedby anaerobes, Gram positive and Gram negative organisms. It is a disease of children in whom over 95%occur in children aged less than 6 years old. It is rare in adult but the frequency is increasing nowadays.However the mortality incidence is less due to advent of antibiotics. Fungal agents are rarely associatedwith such infections. We report a rare case of retropharyngeal abscess in a 60-year old adult with diabetesmellitus in whom Candida Albicans was the implicated pathogen.Key Words: Retropharyngeal abscess, Adult, Candida albicans.
Zalilah Musa, Irfan Mohamad, Khairul Bariah Johan, Azian Harun
Case Report
Fig.-1a & 1b: Fullness at left lateral part of neck which extends anteriorly. Fig.-2: Lateral soft tissue neck x-ray showing widening of soft tissue ofprevertebral area with area of lucency indicating air content.

Candida Albicans Retropharyngeal Abscess30
in mild narrowing of lumen. The diagnosis ofretropharyngeal abscess was made and the patient wasstarted on intravenous (IV) Ceftriaxone 1 g bd, IVMetronidazole 500 mg tds and IV Cloxacillin 1 g qid.Incision and drainage was performed via both externaland internal approach. From external incision 2 cmbelow angle of mandible, there was collection of yellowishthick pus posterior to strap muscle at left side of neckwhich continues up to left pyriform sinus and posteriorpharyngeal wall (Figure 4). Thirty milliliter (mL) of thickpus was drained out. Intraorally another vertical incisionwas given at the most bulging area at posteriorpharyngeal wall from which 3 mL of thick yellowish puswas drained. The pus specimens were sent formicrobiological investigation. Patient was put onnasogastric tube for feeding. After two days, thepharyngeal wall bulge subsided. Culture results revealedpure growth of yeast which was later identified asCandida Albicans (Figure 5). No other bacteria includinganaerobes, was isolated from the specimens. Examinationfor acid fast bacilli was also negative. He was startedon oral Fluconazole 200mg daily. A repeat CT scan wasdone which showed no recollection of pus. The nasogastrictube was removed as the patient was able to tolerateorally well. He was discharged with oral fluconazole200mg once daily for a complete course of two weeks.DISCUSSION: Retropharyngeal abscess is a deep tissueneck infection which can be life threatening. Theanatomical location of the space increases the likelihoodof developing upper airway obstruction, descendingmediastinitis and jugulo venous thrombosis.Retropharyngeal abscess among adults is more commonin males then in females with percentage of males beingaffected is around 60%2. Retropharyngeal abscess occursmainly during infancy and childhood in whom 90% ofcases occur before the age of 6 months,2. In children itis frequently associated with viral upper respiratoryinfections, pharyngitis and otitis media. All theseinfections cause adenopathy of retropharyngeal lymph
nodes and suppuration which gives rise toretropharyngeal abscess formation1,2,3. The facts thatthese lymph nodes regress in childhood may account forlow incidence of disease in adults2,4. Majority of patientspresent with symptoms of sore throat, dysphagia or neckpain as seen in this patient1,2. Only a minority of patientpresented with airway obstruction. Compared to children,majority of adult retropharyngeal abscess also havehistory of intraoral procedures, trauma, hypopharyngealforeign body or odontogenic infection2,5. In our patient,the predisposing factors were old age and diabetesmellitus, which is associated with immunocompromisedstatus. The predominant organisms grown from theseabscesses are Group A Beta-hemolytic streptococci,Staphylococcus aureus , Hemophilus influenza andanaerobic cultures commonly are Bacteroides,Peptostreptococcus and Fusobacterium species1,2. In thepresent case, a rare occurrence Candida Albicans wasnoted. This patient is an elderly diabetic patient whoalso faced with senescence of immune system that canalter his host defence mechanism which predisposes himto any type of infection, including invasive Candidiasis.Candida spp. have been reported to cause fungalinfections in humans, ranging from non life threateningmucocutaneous diseases to invasive diseases that caninvolve any organ6. Candida Albicans occur naturallyas a commensal of mucous membranes and the digestivetract. Candida Albicans are present in oral cavities of15 to 75% of population7. The fungus, which is normallya harmless, is associated with root caries and has beenobserved in patients with infected gingival crevices8. Inour patient, Candida Albicans might have invaded theoral mucosa and persist within the epithelium causingsuperficial lesions. These infections reach theretropharyngeal region through the loose connectivetissue planes between muscles of neck. One major rootis via lateral pharyngeal space to retrovisceral space9.Life threatening complications following retropharyngealinfections due to Candida. Albicans such as descending
Fig.-3a & 3b: An extensive neck space abscess involving retropharyngealand prevertebral region.
Fig.-4: Pus coming out from underneath strap muscle originated fromretropharyngeal region intraoperatively.

Candida Albicans Retropharyngeal Abscess31
mediastinitis have been reported10. Other complicationsthat can occur are airway obstruction, septicemia andaspiration pneumonia. Diagnosis of retropharyngealabscess is mainly on clinical grounds along withsupportive imaging study. Lateral soft tissue X-ray ofneck appeared to be the single most valuableinvestigations in evaluation of retropharyngeal space asevidenced by study conducted over 23 patients inSingapore General Hospital11. Plain radiograph showedwidened prevertebral soft tissue on lateral view of neck.Wholey et al. in his study among adults and children in1954 concluded that measurement greater than 7mm atC2 and 22mm at C6 are abnormal and strongly supportretropharyngeal abscess12. CT-scan and MRI of neck candifferentiate abscess from simple cellulitis and othercause of retropharyngeal swelling2. It does not onlyconfirm the diagnosis but more importantly it is able tolocalize the involved area and facilitate the intra-operativeapproach. For the management of candidiasis, ClinicalPractice Guidelines by the Infectious Diseases Societyof America 2009 stated that the typical intravenousdosage of Amphotericin B deoxycholate at 0.5-0.7 mg/kgdaily is used for invasive candidiasis but dosage as highas 1mg/kg daily should be considered for invasive Candidainfections caused by less susceptible species like Candida.Glabrata and Candida Krusei. For patients with invasivecandidiasis, fluconazole should be administered with aloading dose of 800 mg (12mg/kg) followed by a dailydose of 400 mg (6 mg/kg); a lower dosage is required inpatients with creatinine clearance < 50 mL/min13. Theintroduction of triazoles like fluconazole has been animportant contribution for treatment of this disease14.As in this patient he was initially started on IVmetronidazole 500 mg tds, IV ceftriaxone1 g bd and IVcloxacillin 1 g qid. Once the culture revealed growth of
Candida Albicans, oral Fluconazole 800 mg loading dosewas given followed by 400 mg once daily was commencedand continued for two weeks. Urgent surgical drainageis mandatory to eradicate the abscess. Access to theretropharyngeal space can be through an externaltranscutaneous incision anterior to sternocleidomastoidmuscle or transoral approach by making a longitudinalincision on the pharyngeal walll5. On rare occasion bothapproaches are used as seen in this patient. Choice ofdrainage is actually depend on location of the abscess.External transcutaneous approach can also allowdrainage of lateral pharyngeal space and to some extentthe submandibular and sublingual region. Thus it isused when retropharyngeal abscess spread to theseregions. The external incision also enables inspection ofcarotid sheath and contents for possible erosion.Sometimes external approach is used if early recurrenceoccurs or if abscess does not resolve rapidly with transoraldrainage. In this patient as the abscess was extensive,both approaches were used for drainage.CONCLUSION: Retropharygeal abscess is one of theserious deep tissue neck infections. It can be caused byvarious types of organisms depending on source ofinfection. A rare case of an immunocompromised adultwith underlying diabetes mellitus having CandidaAlbicans retropharyngeal abscess is reported.REFERENCES:1. Sharma HS, Kurl DN, Hamzah M. Retropharyngeal Abscess:
Recent trends. Auris Nasus Larynx 1998;25:403-6.2. Tannebaum RD. Adult retropharyngeal abscess: A case report and
review of Literature. J Emerg Med 1996;14(2):147-58.3. Maran AGD. Neck space infections. Logan Turner’s Diseases of
the Nose, Throat and ear. London: Wright 1988: 104-8.4. Echevarria J. Deep neck infections. In: Schlossberg D, editor.
Infections of head and neck. New York; Springer 1987:172-4.5. Haug RH, Picard U, Indresano AT. Diagnosis and treatment of
retropharyngeal abscess in adults. Br J Oral and Maxilllofac Surg1990;28:34-8.
6. Fridkin SK. The changing face of fungal infection in health caresettings. Clin Infect Dis 2005; 41:1455-60.
7. Ten Cate JM, Klis FM, Pereira-centi T et al. Molecular and cellularmechanism that lead to candida biofilm formation . J Dent Res2009; 88 : 105-15.
8. Shen S, Samaranayake LP, Yip HK, Dysen JE. Bacteria and yeastflora of root surface carries in elderly ethnic Chinese. Oral Dis2002; 8:207-17.
9. Moncada R, Warpeha R, Pikleman J, et al. Mediastinitis fromodontogenic and deep cervical infection. Chest 1978;73(4):497-500.
10. Parisa B, Abdolvahab A, Farimah F. A case of Candida mediastinitisafter dental extraction. J Infect Dev Ctries 2011;5(1):75-8.
11. Fogeltanz KA, Pursel KJ. Retropharyngeal abscess presentingas benign neck pain; J Manipulative Physiol Ther 2006; 29:174-8.
12. Wholey MH, Bruwer AJ, Baker HY. The lateral roentomogram ofneck. Radiol 1958;71:350-6.
13. Pappas PG, Kauffman CA, Andes D et al. Infectious DiseasesSociety of America Clinical Practice guidelines for managementof candidiasis ; 2009 update by the Infectious Diseases Society ofAmerica. Clin Infect Dis 48:503-35.
14. Bodey GP. Azole antifungal agent. Clin Infect Dis 1992; 14 (1):161-9.
Fig.-5: Candida Albicans grown on corn meal agar slide culture (X400magnification).