Embed Size (px)
Citation preview
Chinese Journal of Clinical Oncology Feb, 2007, Vol. 4, No. 1 P42~47 Chunyan Cui et al.42
Magnetic Resonance Imaging of Retropharyngeal Lymphadenopathy in Nasopharyngeal Carcinoma
Chunyan CuiXuewen Liu
State Key Laboratory of Oncology in South-ern China, Imaging Diagnostic and Interven-tional Center, Cancer Center, Sun Yat-sen University, Guangzhou 510060, China.
Correspondence to: Xuewen Liu Tel: 86-20-87343217E-mail: [email protected]
Received December 21, 2006; accepted Feb-ruary 1, 2007.
OBJECTIVE The aim of our study was to document the patterns of RLN spread by using MRI. METHODS The MR images of 294 patients with newly diagnosed NPC were reviewed retrospectively. Criteria for metastatic lymph nodes included: shortest axial diameter, nodal necrosis, extracapsular spread, and a contrast enhancing rim.RESULTS RLN involvement was detected in 190 (64.6%) patients. A significantly higher incidence of metastatic RLNs was observed in patients with involvement of the oropharynx, nasal cavity, pre-styloid parapharyn-geal space, post-styloid parapharyngeal space, levator muscle of the velum palatini, and tensor muscle of the velum palatine. Patients with level II, III, and V node involvement also had a higher incidence of metastatic RLNs. Of the 231 patients who had metastatic RLNs or cervical lymph nodes, 43 (18.6%) had only metastatic RLNs, 41 (17.7%) had only metastatic cervical lymph nodes, and 147 (63.6%) exhibited an involvement of both the RLNs and cervical lymph nodes. The difference between the incidence of RLN involvements (82.3%) and the incidence of cervical lymph node involvement (81.4%) was very small. CONCLUSION Metastatic RLNs are significantly associated with early stage primary tumor involvement and supper cervical lymph node metastasis in NPC.
KEYWORDS: cervical lymph nodes, magnetic resonance imaging, nasopharyngeal carcinoma, retropharyngeal lymph nodes.
INTRODUCTION
Retropharyngeal lymph nodes (RLNs) lie in the retropharyngeal space that is divided into medial and lateral areas. Since the RLNs are deeply located, they are mainly evaluated by imaging exami-nations, such as computed tomography (CT) and magnetic reso-nance imaging (MRI). However, compared to CT, MRI provides a better option for RLN identification because MRI produces a higher soft tissue resolution. According to the study of Sham et al. [1] in 1990, the cervical lymph nodal spreads were orderly down from the upper to lower, but the spread patterns of RLNs in NPC were not addressed well. Three dimensional conformal-radiation therapy and intensity-modulated radiation therapy has recently gained popularity in the treatment of NPC, and an understanding of the patterns of regional lymph node metastasis in NPC can be helpful in delineating the target volumes for radiotherapy. The aim of our study was to evaluate the incidence and distribution of metastatic RLNs, and to examine their relationship to primary
CJCO http://www.cjco.cn E-mail:[email protected](Fax):86-22-2352 2919
[SpringerLink] DOI 10.1007/s11805-007-0042-7

43Chinese Journal of Clinical Oncology Feb, 2007, Vol. 4, No. 1 P42~47 Chunyan Cui et al.
tumor extension and cervical lymph nodes in NPC in order to document the patterns of RLN spread by us-ing MRI.
MATERIALS AND METHODS
Patient characteristicsFrom July 2003 to February 2005, 294 cases with newly diagnosed, untreated NPC that were pathologi-cally proved were enrolled in our study. The 223 men and 71 women were 20~73 years of age (median, 46 years). The male to female ratio was 3.14:1. Patho-logic features (WHO): Type 1, 3 (1.0%); Type 2, 30 (10.2%); Type 3, 261 (88.8%). All patients were staged according to the 2002 International Union against Cancer (UICC)/American Joint Committee on Cancer (AJCC) staging system as follows: T1, 93 (31.6%); T2a, 9 (3.1%); T2b, 34 (11.6%); T3, 117 (39.8%); T4, 41 (13.9%); N0, 108 (36.7%); N1, 107 (36.4%); N2, 62 (21.1%); N3a, 8 (2.7%); N3b, 9 (3.1%); M0, 288 (98.0%); M1, 6 (2.0%). The clinical stagings were as follows: stage I, 40 (13.6%); Stage II, 65 (22.1%); Stage III, 126 (42.9%); Stage IV, 63 (21.4%).
MR examination and image analysisAll MR imaging was performed with a 1.5-Tesla sys-tem (Signa, General Electric, CV/i) with a head and neck combined coil. The area from the suprasellar cistern to the inferior margin of the sternoclavicular joint was examined. T1-weighted fast spin-echo MR images in the axial, coronal and sagittal planes (rep-etition time of 500~600 ms and echo time of 10~20 ms), and T2-weighted fast spin-echo MR images in the axial plane (repetition time of 4000~6000 ms and echo time of 95~110 ms) were obtained before injection of contrast material. After intravenous Gd-DTPA injection at a dose of 0.1 mmol per kg of body weight, spin-echo T1-weighted axial and sagittal se-quences, and spin-echo T1-weighted fat-suppressed coronal sequences were performed sequentially, with parameters similar to those used before Gd-DTPA injection. Section thickness was 5 mm with a 1 mm interslice gap for the axial plane, and 6 mm with a 1 mm interslice gap for the coronal and sagittal planes. Two experienced radiologists separately evalu-ated the MRI images. The maximal axial diameter of each lymph node was measured on T2-weighted axial planes. The locations of each RLN and cervical node were recorded according to the level of the cervical vertebral body and disk space, and cervical nodes were recorded according to Som nodal classification [2]. Based on the criteria of RLN involvement intro-
duced by Brekel and King et al.[3,4]: (1) The shortest axial diameter of the cervical nodes was ≥10 mm (≥11 mm in the IIA region), or there was a group of three or more nodes that were borderline in size if their shortest axial diameter was 8~9 mm (9~10 mm in the IIA regions); (2) The lateral RLNs were consid-ered metastatic if their shortest axial diameter was ≥5 mm, and any visible node in the median retropharyn-geal group was considered malignant; (3) Nodes were considered to be metastatic in the presence of central necrosis or extracapsular spread or surrounding rim of enhancement.
Statistical analysisAll statistical analyses were performed using the Sta-tistical Package for the Social Sciences (SPSS) 10.0 software. The chi-square test was used to analyze the relationship between metastatic RLNs and the extent of primary tumor and cervical lymph node metasta-ses. A two-tailed P value of <0.05 was considered statistically significant in all cases.
RESULTS
Incidence and distribution of RLNsAmong the 294 patients 190 (64.6%) displayed 273 RLNs. Metastatic RLNs were seen at the follow-ing levels with the number of nodes: skull base, 29 (10.6%); C1, 166 (60.8%); C1/2, 44 (16.1%); C2, 30 (11.0%); C2/3, 2 (0.7%) and C3, 2 (0.7%). The inci-dence of metastatic RLNs showed an orderly decrease from the level of C1 to C3. The metastatic RLNs were distributed among the 190 patients as follows: 1 node, 121 (63.7%) patients; 2 nodes, 57 (30.0%) pa-tients; 3 nodes, 9 (4.7%) patients; 4 nodes, 3 (1.6%) patients. Of the 190 patients with metastatic RLNs, 133 (70.0%) had metastatic unilateral RLNs, 56 (29.5%) had metastatic bilateral RLNs and 1 patient (0.5%) was observed with bilateral side lateral RLN and an enlarged medial RLN. Of the 133 patients with metastatic unilateral RLNs, 55 (41.4%) had nodes on the left side and 78 (58.6%) on the right.
Relationship between metastatic RLNs and tumor involvementThe relationship between involvement of RLNs and primary tumors is shown in Table 1. A significantly higher incidence of metastatic RLNs was observed with involvement of the oropharynx, nasal cavity, pre-styloid space, post-styloid space, levator muscle of velum palatini and tensor muscle of the velum palatini. On the contrary, there was no significant difference in the incidence of involvement of RLNs when the primary tumor extended into the pterygopal-

Chinese Journal of Clinical Oncology Feb, 2007, Vol. 4, No. 1 P42~47 Chunyan Cui et al.44
atine fossa, clivus, base of the sphenoid bone, floor of the pterygoid bone, foramen ovale, foramen lacerum, paranasal sinus, infratemporal fossa, laryngopharynx, orbit or intracranial extension.
Relationship between metastatic RLNs and cervical lymph nodesOf 294 patients, 231 (78.6%) had metastatic RLNs or cervical lymph nodes. Of these 231 patients, 43 (18.6%) had metastatic RLNs only, 41 (17.7%) had metastatic cervical lymph nodes only, and 147 (63.6%) exhibited an involvement of both the RLNs and cervical lymph nodes. These 231 patients had an equal incidence (82.3% vs. 81.4%) of metastatic RLNs and cervical lymph nodes. A higher incidence of metastatic RLNs was found when cervical lymph node metastasis was present (χ2=40.653, P≤0.001).
The incidence of metastatic RLNs in patients with bilateral cervical lymph node metastasis was higher than in patients with unilateral cervical lymph node metastasis (85.7% vs. 75.0%), with a difference that was very close to statistical significance (χ2=5.054, P=0.081). The relationship between the metastatic RLNs and cervical lymph nodes at different levels is shown in Table 2. There was a statistically significant association between the involvement of RLNs and level II, level III and level V nodes. Conversely, there was no significant association between RLNs involve-ment and level I, level IV and supraclavicular nodes. Of 132 patients with metastatic unilateral RLNs, 55 (41.6%) had metastatic ipsilateral cervical nodes, 31 (23.5%) had metastatic bilateral cervical nodes, and only 11 (8.3%) had metastatic contralateral cervical nodes.
Table 1. Relationship between metastatic RLNs and extent of primary tumor.
No. of patients with RLNs (%)Extent of primary tumor Site not involved Site involved χ2 value P valueLevator muscle of velum palatini 37/82 (45.1) 153/212 (72.2) 18.922 0.000Oropharynx 138/235 (58.7) 42/59 (88.1) 17.846 0.000Nasal cavity 133/217 (61.3) 57/77 (74.0) 4.032 0.045Pre-styloid space 74/147 (50.3) 116/147 (78.9) 26.246 0.000Post-styloid space 128/219 (58.4) 62/75 (82.7) 14.335 0.000Tensor muscle of velum palatini 70/140 (50.0) 120/154 (77.9) 25.009 0.000Base of the sphenoid bone 108/178 (60.7) 82/116 (70.7) 3.082 0.079Floor of the pterygoid bone 112/184 (60.9) 78/110 (70.9) 3.035 0.081Clivus 125/204 (61.3) 65/90 (72.2) 3.274 0.070Foramen lacerum 132/214 (61.7) 58/80 (72.5) 2.981 0.084Foramen ovale 147/236 (62.3) 43/58 (74.1) 2.860 0.091Sinus 161/254 (63.4) 29/40 (72.5) 1.256 0.262Orbit 186/289 (64.4) 4/5 (80.0) 0.659*Intracranial extension 169/262 (64.5) 21/32 (65.6) 0.016 0.900Laryngopharynx 188/291 (64.6) 2/3 (66.7) 1.000*Infratemporal fossa 188/290 (64.8) 2/4 (50.0) 0.616
n Level I Level II Level IIA Level IIB Level III Level IV Level V SLNsRLNs negative 104 0 40 20 33 8 3 2 2RLNs positive 190 7 134 76 132 60 14 17 5χ2 value 36.626 13.184 38.880 21.569P value 0.054* <0.001 <0.001 <0.001 <0.001 0.189* 0.023* 0.500*
* Fisher exact test
Table 2. Relationship between metastatic RLNs and cervical lymphadenopathy.
* Fisher exact test
45Chinese Journal of Clinical Oncology Feb, 2007, Vol. 4, No. 1 P42~47 Chunyan Cui et al.
DISCUSSION
The incidence of metastatic lymph nodes in NPC is higher than in other head and neck cancers, with a RLN involvement of 29.1%~89% based on previous literature[4-7].The difference in the incidence of RLNs which has been higher in various reports may result from different radiological size criteria or different methods of examination. Lam et al.[5] and King et al. [4] found that normal RLNs were smaller than 4 mm or 4.5 mm in their maximum diameter of the shortest axis according to observation respectively in normal groups of 20 and 100 people. Therefore, our study used a maximal axial diameter of ≥5 mm as the size
criteria for metastatic RLNs based on the recommen-dation of published reports. The vast majority of RLN involvement in NPC patients was among the lateral group. Since the medial retropharyngeal nodes are usually not visible, any MRI finding of a medial ret-ropharyngeal node is regarded as abnormal. The incidence of involvement of RLNs was 64.6% in our study, whereas in a study by Chua et al. [7] , metastatic rates were 29.1% in NPC patients with metastatic RLNs. However, that study was based on CT imaging, and a dimension of ≥10 mm was used to assign RLN involvement, possibly leading to a higher difference in the incidence of RLN involvement. It is difficult to discriminate RLNs from front muscle
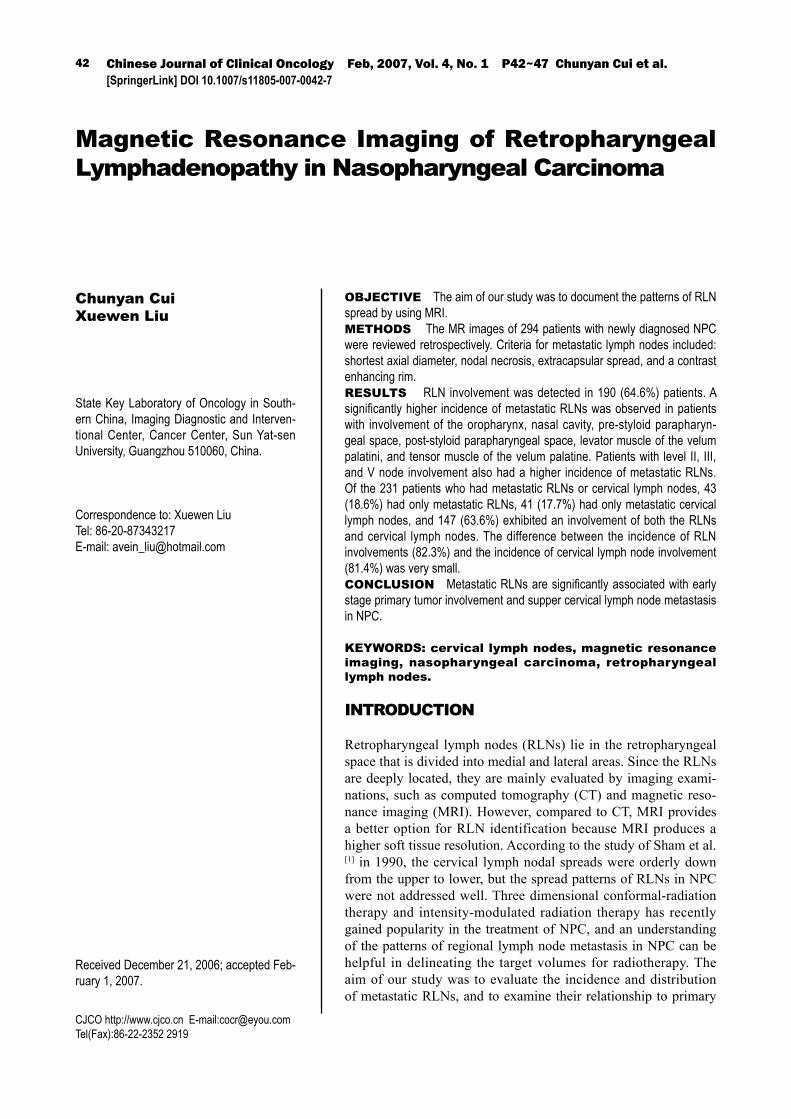
Fig.1. MR imaging in a 41-year-old man with nasopharyngeal carcinoma showing enlarged lateral retropharyngeal lymph nodes bi-laterally (white arrowheads). (a) Transverse T2-weighted fast spin-echo MR image. (b) Transverse T1-weighted fast spin-echo MR image. (c) Transverse T1-weighted spin-echo contrast-enhanced MR image. (d) Coronal T1-weighted spin-echo contrast-enhanced MR image obtained with fat suppression.
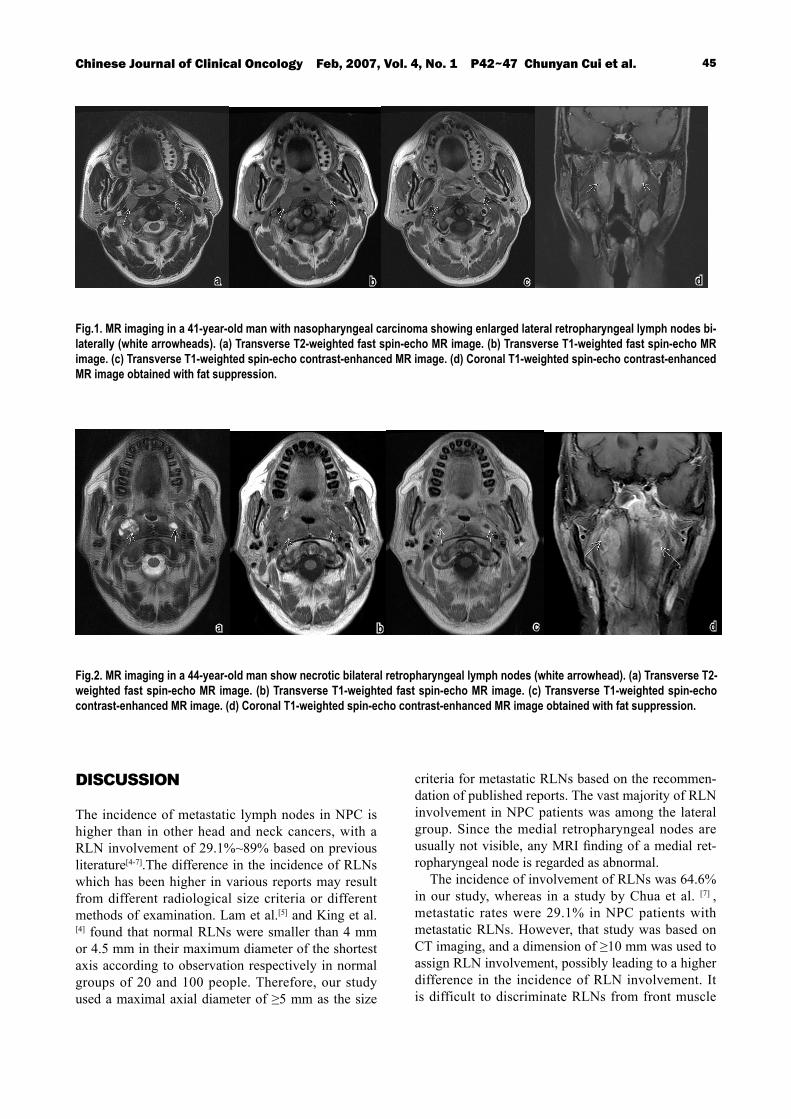
Fig.2. MR imaging in a 44-year-old man show necrotic bilateral retropharyngeal lymph nodes (white arrowhead). (a) Transverse T2-weighted fast spin-echo MR image. (b) Transverse T1-weighted fast spin-echo MR image. (c) Transverse T1-weighted spin-echo contrast-enhanced MR image. (d) Coronal T1-weighted spin-echo contrast-enhanced MR image obtained with fat suppression.
a b c d
a b c d

Chinese Journal of Clinical Oncology Feb, 2007, Vol. 4, No. 1 P42~47 Chunyan Cui et al.46
of the vertebra from the primary tumor on CT imag-ing, for they are very similar in density and location. Compared to CT, MRI provides a better option for identification of RLNs and the primary extent into the parapharyngeal space and surrounding normal tissue identification, because MRI shows a higher resolu-tion than CT of soft tissue[8]. Therefore, MR imaging is superior to CT imaging for delineating the target volume for three dimensional conformal radiotherapy and intensity modulated radiation therapy in NPC cases. Our study showed that the majority of metastatic RLNs were located superior to the oropharynx level (from the base of skull to the C1/2 disk level), and the multiple metastatic RLNs were common in NPC. Metastatic RLNs at the oropharyngeal level might re-quire special consideration in radiation planning. The definition of RLNs proposed by Som et al.[2] states that RLNs must lie medial to the internal carotid ar-teries within 2 cm of the skull base. This definition may be not suitable for NPC, because there are so many RLNs located beyond that region. Based on our observations, from the skull base to tongue bone level may be suitable for NPC. The lymphatic drainage of carcinoma of the head and neck was associated with the primary tumor loca-tion and adjacent subsites to which the tumor spread [9]. Drainage regions of the retropharyngeal nodes are the nasal cavities, eustachian tubes, nasopharynx, oropharynx, hypopharynx, pharyngeal wall, and pal-ate[10]. Tumor invasion into the levator muscle of the velum palatini was associated with a higher risk of RLN metastasis, possibly due to submucosal inva-sion. The risk of RLN metastasis markedly increased when the primary tumor invaded beyond the confine-ment of the pharyngobasilar fascia[7]. Furthermore, a higher incidence of metastatic RLNs was associated with primary tumor invasions into the oropharynx, nasal cavity, pre-styloid space, post-styloid space and tensor muscle of the velum palatini. Drainage regions of the retropharyngeal nodes are located mostly of these subsites, and involvement of these sites is clas-sified as T2 according to the 2002 UICC/AJCC Stag-ing System. Also there was no apparent relationship between RLN metastasis and the laryngopharynx, pterygopalatine fossa, infratemporal fossa, skull base, paranasal sinus or intracranial extension. The struc-tures are not drainage regions of the retropharyngeal nodes except for the laryngopharynx, and involve-ment of these sites has not markedly increased in the incidence of RLNs spread. The findings of our study suggest that metastatic RLNs were not associated with involvement of the laryngopharynx in this se-ries. The lymphatic drainage of laryngopharynx may
primarily drain to the retropharyngeal lymph nodes in NPC cases. The incidence of laryngopharyngeal invasion was very low, so we could not evaluate the association between the laryngopharynx and RLNs. The regional lymph node spread in NPC includes cervical lymph nodes and retropharyngeal lymph nodes, which have an apparent relationship. A higher incidence of metastatic RLNs was found in patients with cervical lymph node metastases. This finding is in agreement with the report of Chua et al.[7] We also found that the incidence of metastatic RLNs in pa-tients with bilateral cervical lymph node metastases was lower than in patients with unilateral cervical lymph node metastases. Therefore, the incidence of metastatic RLNs in N2 patients is higher than in N1 patients. A statistically significant association was found between the involvement of RLNs and level II, level III and level V nodes. This was in agreement with the observation that the efferent vessels of RLNs drain to the upper jugular chain and to the posterior triangle [10]. This is the reason for the relationship of retropharyngeal lymph nodes and cervical lymph nodes. The lymphatic vessels drain in two general direc-tions, lateral and medial. The primary drainage is the lateral pathway, which drains the lateral nasopharynx (pharyngeal recess), and flows into the lateral RLNs or into the lateral half of the upper internal jugular chain (group II lymph nodes) by them or directly into group II lymph nodes. The medial drainage pathway drains the roof and posterior wall of the nasophar-ynx, and flows into the median RLNs penetrating the pharyngobasilar fascia[9]. Our study revealed that the incidence of metastatic RLNs was almost equal to the incidence of cervical lymph nodes metastases, and was also nearly equivalent to the incidence of cervical level II node metastases. In 41 (17.7%) of the 231 pa-tients with nodal metastases, the metastasis bypassed the RLNs and spread directly to the level II nodes. Of 132 patients with unilateral RLNs involvement, 23.5% had bilateral cervical lymphadenopathy and 8.3% had contralateral cervical lymphadenopathy. These results support the view that another lymphatic pathway exists in NPC, which allows direct lymphat-ic spread to level II nodes without RLN involvement [6,11]. Consequently, these results indicate that both RLNs and cervical level II nodes might be the first-echelon nodes in nasopharyngeal carcinoma. In conclusion, a high incidence of RLN involve-ment is present in patients with nasopharyngeal carci-noma. The majority of metastatic RLNs were located superior to the oropharynx level, and the incidence of RLNs showed an orderly decrease from the level of C1 to C3. Both RLNs and cervical level II nodes

47Chinese Journal of Clinical Oncology Feb, 2007, Vol. 4, No. 1 P42~47 Chunyan Cui et al.
appear to be the first-echelon nodes in NPC. The pat-terns of RLN spread, which have been demonstrated in our research, are helpful for the delineation the target area in radiotherapy in three dimensional con-formal radiotherapy and intensity modulated radia-tion therapy. A higher incidence of metastatic RLNs was associated with early stage primary involvement beyond the pharyngobasilar fascia and the upper cer-vical lymph node metastasis. The implication is that RLN involvement might affect treatment outcome in NPC. The prognostic significance of RLNs in NPC must be reevaluated with a larger follow-up study.
REFERENCES1 Sham JST, Choy D, Wei WI. Nasopharyngeal carcinoma:
Orderly neck node spread. Int J Radiat Oncol Biol Phys 1990;19:929–933.
2 Som PM, Curtin HD, Mancuso AA. Imaging-based nodal classification for evaluation of neck metastatic adenopathy. AJR 2000;174:837–844.
3 Van den Brekel MWM, Stel HV, Castelijns JA, et al. Cer-vical lymph node metastasis: assessment of radiologic criteria. Radiology 1990;177:379–384.
4 King AD, Ahuja AT, Leung SF, et al. Neck node metas-tases from nasopharyngeal carcinoma: MR imaging of patterns of disease. Head Neck 2000;22:275-281.
5 Lam WWM, Chan YL, Leung SF, et al. Retropharyngeal lymphadenopathy in nasopharyngeal carcinoma. Head Neck 1997;19:176-181.
6 Shu-Hang Ng, Joseph Tung-Chieh Chang, Sheng-Chieh Chan, et al. Nodal metastases of nasopharyngeal car-cinoma: patterns of disease on MRI and FDG PET. Eur J Nucl Med Mol Imaging, 2004;31:1073-1080.
7 Chua DT, Sham JS, Kwong DL, et al. Retrophayrngeal lymphadenopathy in patients with nasopharyngeal carcinoma. Cancer 1997;79:869–877.
8 Olmi P, Fallai C, Colagrande S, et al. Staging and follow up of nasopharyngeal carcinoma: magnetic resonance imaging versus computerized tomography. Int J Radiat Oncol Biol Phys 1995;32:795–800.
9 Mukherji S, Armao D, Joshi V. Cervical nodal metasta-ses in squamous cell carcinoma of the head and neck: What to expect. Head Neck 2001;23:995-1005.
10 Rufener JB, Cohen JI. Metachronous spread of parathy-roid carcinoma to a retropharyngeal lymph node. Head Neck 2003;25:968-971.
11 Wakisaka M, Mori H, Fuwa N, et al. MR analysis of na-sopharyngeal carcinoma: correlation of the pattern of tumor extent at the primary site with the distribution of metastasized cervical lymph nodes. Preliminary re-sults. Eur Radiol 2000;10:970-977.