Embed Size (px)
Citation preview

Q7
1
2
3
4
5
6
7
89
10
11
12
13
14
15
1617
18
19
20
21
22
23
2425
26
27
28
29
30
31
3233
34
35
36
37
38
39
4041
42
43
44
45
46
47
4849
50
51
52
53
54
55
56
CRANIOMAXILLOFACIAL TRAUMA
57
*Consu
Center, U
Helsinki, F
yConsuCenter, U
Helsinki, F
zConsuT€o€ol€o Hos
xRadiolRadiology,
Helsinki U
kConsuUniversity
Finland.
58
59
60
61
62
63
6465
66
67
68
Remember the Vessels! CraniofacialFracture Predicts Risk for Blunt
Cerebrovascular InjuryElina Varjonen, MD,* Frank Bensch, MD, PhD,y Tuomo Pyh€alt€o, MD, PhD,z
Mika Koivikko, MD, PhD,x and Johanna Sn€all, MD, DDS, PhDk
6970
71
7273
74
75
76
77
78
79
8081
82
83
84
85
86
87
8889
90
91
92
Purpose: The risk factors for blunt cerebrovascular injuries (BCVIs) are currently under intensive
research, yet it is still controversial who should be screened. This study aimed to determine whethercraniofacial fractures are associated with BCVI.
Patients andMethods: This retrospective cohort study focused on patients with suspected polytraumaafter whole-body computed tomographic angiography of the cervical arteries. Patients were reviewed for
BCVI and craniofacial fractures. Exclusion criteriawere hanging injury, gunshot injury or other penetrating
injury to the neck, and a cervical fracture on any level. The outcome variable was BCVI, and the main
predictor variable was a craniofacial fracture. A secondary predictor variable was a type of craniofacial
fracture classified as a facial fracture, skull fracture, or a combination of facial and skull fracture. Other
predictor variables were gender, age, and mechanism of injury. In addition, specific craniofacial fractures
were analyzed in more detail. The relevance of associations between BCVI and the predictors underwent
c2 testing. Significance was set at .01.
Results: Four hundred twenty-eight patients 13 to 90 years old during a 12-month period were included
in the analysis. Craniofacial fractures occurred in 75 (17.5%). BCVI occurred significantly more frequentlyin those with than in those without a craniofacial fracture (18.6 vs 7.4%; P = .002). Patients with cranio-
facial fracture had a 4-fold increased risk for BCVI, whereas those 31 to 50 years old had 3.4-fold increased
risk. Type of craniofacial fracture, gender, and mechanism of injury were not associated with BCVI.
Conclusion: Craniofacial fractures are a serious risk factor for BCVI. This research suggests that in
patients with any craniofacial fracture and suspected polytrauma, rigorous imaging of cervical arteries
in search of BCVI is essential.
� 2018 Published by Elsevier Inc. on behalf of the American Association of Oral and Maxillofacial
Surgeons
J Oral Maxillofac Surg -:1.e1-1.e9, 2018
9394
95
9697
Blunt cerebrovascular injury (BCVI) can lead to devas-
tating neurologic sequelae. BCVI occurs in 1 to 2% ofall patients with blunt trauma, and in severely injured
ltant, Department of Radiology, HUS Medical Imaging
niversity of Helsinki and Helsinki University Hospital,
inland.
ltant, Department of Radiology, HUS Medical Imaging
niversity of Helsinki and Helsinki University Hospital,
inland.
ltant, Department of Orthopedics and Traumatology,
pital, Helsinki University Hospital, Helsinki, Finland.
ogist-in-Chief and Adjunct Professor, Department of
HUS Medical Imaging Center, University of Helsinki and
niversity Hospital, Helsinki, Finland.
ltant, Department of Oral and Maxillofacial Diseases,
of Helsinki and Helsinki University Hospital, Helsinki,
1.e1
FLA 5.5.0 DTD � YJOMS58221_proof �
patients, the incidence can be at least twice as high.1-5
Early recognition and prompt initiation of treatment ofthese injuries have resulted in a marked decrease in
Conflict of Interest Disclosures: None of the authors have any
relevant financial relationship(s) with a commercial interest.
Address correspondence and reprint requests to Dr Varjonen:
Department of Radiology, T€o€ol€o Trauma Center, Topeliuksenkatu
5, 00029 HUS, Finland; e-mail: [email protected]
Received January 1 2018
Accepted March 23 2018
� 2018 Published by Elsevier Inc. on behalf of the American Association of Oral
and Maxillofacial Surgeons
0278-2391/18/30293-3
https://doi.org/10.1016/j.joms.2018.03.035
18 April 2018 � 2:37 pm � CE AH
98
99
100
101
102
103
104105
106
107
108
109
110
111
112

Q2
1.e2 BLUNT CEREBROVASCULAR INJURY Q1
113
114
115
116
117
118
119
120121
122
123
124
125
126
127
128129
130
131
132
133
134
135
136137
138
139
140
141
142
143
144145
146
147
148
149
150
151
152153
154
155
156
157
158
159
160161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176177
178
179
180
181
182
183
184185
186
187
188
189
190
191
192193
194
195
196
197
198
199
200201
202
203
204
205
206
207
208209
210
211
212
213
214
215
216217
218
219
220
221
222
223
224
cerebrovascular ischemic insults from 20 to 31% to 0.5
to 9.6%.3,6-9 If left untreated, mortality associated with
these injuries increases to 9 to 13%.3,4,6
BCVI diagnosis has been facilitated by the wide-
spread adoption of standardized screening protocols
and advances in imaging technology, such as multide-
tector cervical computed tomographic angiography
(CTA). Various screening guidelines are available toidentify patients with risk factors suggestive of a
possible BCVI, such as the evidence-based guidelines
established by the Eastern Association for the Surgery
of Trauma (EAST)10 and the Denver Group guide for
practicing physicians in screening, diagnosing, and
treating BCVI.3,6,8,11
The most common etiology for BCVI is assumed to
be hyperextension of the neck, causing stretching ofthe carotid arteries over the lateral processes of C1
to C3.11,12 Basic screening guidelines, such as the
Denver criteria, include fractures of the upper
cervical spine as an indication for BCVI screening.
Further studies have suggested expanding screening
protocols to include any cervical fracture.13,14
The role of facial fractures in BCVIs is not completely
understood, and BCVIs can be missed when applyinginsufficient screening protocols. Mundinger et al15
investigated 4,398 patients with facial fractures and
found BCVI in 1.2%. They also reported that 20% of
BCVIs would have been missed by the EAST BCVI
screening criteria. Burlew et al11 similarly reported
that one fifth of patients with confirmed BCVI did not
meet the Denver screening criteria, and up to one third
of themhad amandibular fracture. Geddes et al16 imple-mented expanded screening criteria (mandibular frac-
tures, complex skull fractures, traumatic brain injury
with thoracic injuries, scalp degloving, thoracic
vascular injuries, and upper rib fractures) to include
the ‘‘missing’’ 20% of patients with BCVI. They found
that 28% of patients with asymptomatic BCVI were
identified solely by the new screening indications pro-
vided as the expanded criteria. Most current BCVIscreening criteria include only Le Fort pattern fractures
as an indication for imaging, although a systematic
review identified mandibular fractures as the most
commonBCVI-associated craniomaxillofacial pattern.17
A correlation between skull base fractures and BCVI
has been repeatedly reported in previous
studies.1,14,15,18,19 These studies were consistent in
indicating skull base fractures as a risk factor for BCVI,although fracture types varied. Previously, the focus
was on petrous bone fractures and carotid canal
involvement,18-20 whereas more recent investigations
have taken into account other parts of the skull
base13-15 and fronto-orbital area.11 York et al21 reported
BCVI rates for all types of skull fractures.
In bony craniofacial trauma, fracture lines often
continue across facial and cranial bones, so the
FLA 5.5.0 DTD � YJOMS58221_proof �
craniofacial region can be considered a single unit.
Therefore, in contrast to previous studies, the present
analyses included any type of facial and skull fracture,
with the aim of analyzing possible correlations
between BCVI and craniofacial fractures and evalu-
ating BCVI incidence in different types of craniofacial
fractures. The hypothesis was that there would be an
association between craniofacial fractures and BCVI.Specific aims for the study were to analyze whether
some facial fracture subtypes correlate with an
increased risk for BCVI.
Patients and Methods
STUDY DESIGN
For this retrospective study, the cohort consisted of
patients with suspected blunt high-energy polytrauma
who were admitted to a level 1 trauma center (T€o€ol€oTrauma Center, Helsinki University Hospital, Helsinki,
Finland) in accord with a trauma alarm protocol from
May 2015 through May 2016. These included patients
with a mechanism of injury serious enough to requirecomputed tomography (CT) of the whole body. All
patients were subjected to split-bolus whole-body
64-slice CT (Discovery CT 750 HD, GE Healthcare,
Milwaukee,WI) including angiography (aWBCT),which
includes a continuous scan from the skull base to the
ischium in simultaneous arterial and portal venous
phases. Table 1 presents the imaging protocol. Data for
patients imaged by aWBCT, in addition to their demo-graphic data, clinical findings, and initial reports, were
retrospectively retrieved from the Picture Archiving
and Communications System (Impax 6, Agfa HealthCare
NV, Mortsel, Belgium) and electronic patient files.
Exclusion criteria were hanging injury, gunshot
injury or other penetrating injury to the neck region,
and cervical fracture at any level.
All CT studies were reviewed by 2 board-certifiedradiologists with 12 and 6 years of experience in
trauma radiology, respectively, who were blinded to
the initial reports. Any discrepancies were resolved
by consensus.
STUDY VARIABLES
Themain outcome variable was BCVI. Themain pre-
dictor variable was a craniofacial fracture. A secondary
predictor variable was type of craniofacial fracture
classified as a facial fracture, skull fracture, or a combi-
nation of facial and skull fractures. Other predictor
variables were gender, age, mechanism of injury, andcraniofacial fracture subgroups.
Patients with craniofacial fractures were identified
and their fractures were divided into 4 facial fracture
subgroups and 3 skull fracture subgroups. Facial
fractures consisted of 1) combined facial fractures
18 April 2018 � 2:37 pm � CE AH

Table 1. IMAGING PROTOCOL OF BODY COMPUTEDTOMOGRAPHIC ANGIOGRAPHY OF CERVICALARTERIES
Split-bolus imaging protocol
Scan area
Circle of Willis and ischium (lower extremities on
request)
Contrast enhancement
Cervical spine in arterial phase
Body in simultaneous arterial and venous phases
80 mL+ 50-mL contrast medium bolus (Omnipaque*Q4 350 mg/mL + iohexol) at 22-second interval
Contrast delay
Cervical spine, SmartPrep* with 130-HU threshold
Body, 45-second fixed delay
Image acquisition parameters
Slice thickness, 0.625 mm
Range, 120-700 mA
Pitch, 39.37 mm/rotation
Table feed: neck, 98.4 mm/second; body,
137.5 mm/second
Neck: kV 100, NI 40
Body: kV 120, NI 50
Reformatted series
Axial, coronal, sagittal planes; vascular and bone
windows
Reformatted slice thickness
Cervical spine: axial, 1.25 mm; coronal and sagittal,
1.5 mm
Cervical vessels, 2 mm coronal and sagittal
Body, 3 mm coronal and sagittal
* GE Healthcare Ireland (Cork, Ireland).
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac
Surg 2018.
Table 2. DESCRIPTIVE STATISTICS FOR 428 PATIENTSWITH TRAUMA
n %
Gender
Male 304 71.0
Female 124 29.0
Age (yr)
Mean 41.9
Range 13-90
Age groups (yr)
13-30 133 31.1
31-50 156 36.4
51-70 111 25.9
71-90 28 6.5
Mechanism of trauma
Motor vehicle accident 199 46.5
Fall from height 86 20.1
Bicycle accident 35 8.2
Pedestrian traffic injuries 24 5.6
Fall on stairs 19 4.4
Assault 14 3.3
Other 51 11.9
Craniofacial fracture 75 17.5
Facial fracture 42 9.8
Skull fracture 19 4.4
Facial + skull fracture 14 3.4
BCVI 40 9.3
Abbreviation: BCVI, blunt cerebrovascular injury.
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac
Surg 2018.
VARJONEN ET AL 1.e3
225
226
227
228
229
230
231
232233
234
235
236
237
238
239
240241
242
243
244
245
246
247
248249
250
251
252
253
254
255
256257
258
259
260
261
262
263
264265
266
267
268
269
270
271
272273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288289
290
291
292
293
294
295
296297
298
299
300
301
302
303
304305
306
307
308
309
310
311
312313
314
315
316
317
318
319
320321
322
323
324
325
326
327
328329
330
331
332
333
334
335
336
(mandibular and midfacial fractures, midfacial and
upper third fractures, and panfacial fractures extend-
ing to all facial thirds); 2) upper third fractures
(fractures of the frontal sinus, orbital roof, or anterior
skull base); 3) midfacial fractures (multiple midfacial
fractures, Le Fort I to III, naso-orbito-ethmoidal, zygo-
matic, and orbital fractures other than the roof or nasal
fractures); or 4) lower facial fractures (exclusivelymandibular fractures). Skull fractures consisted of 1)
basilar skull fractures (fractures of the sphenoid,
petrous temporal bone, or basilar portion of the occip-
ital bone); 2) other skull fractures; or 3) complex skull
fractures (combination of basilar skull fractures and
other skull fractures). Specific facial fractures and
fractures involving the carotid canal and foramen
magnum were documented separately.
STATISTICAL ANALYSIS
For statistical analysis, SPSS 24.0 (IBM Corp,
Armonk, NY) was used. The relevance of associations
between BCVI and craniofacial fractures, facial and
skull fracture subtypes, gender, age, and mechanism
FLA 5.5.0 DTD � YJOMS58221_proof �
of traumawas testedwith the c2 test. Significance level
was set at .01. Multivariate logistic regression analysis
was performed to test the relation between BCVI and
the explanatory variables gender, age, mechanism of
injury, and any craniofacial fracture.
ETHICAL APPROVAL
The internal review board of the Division of Muscu-
loskeletal Surgery at the Helsinki University Hospital
approved the study. Patient-informed consent was
waived, because the study was retrospective. The
study followed the principles of the Declaration
of Helsinki.
Results
Of the 465 patients, 7 were excluded for poor image
quality or lack of intravenous contrast media and 30
were excluded for cervical spine fractures. None of
the patients had sustained a hanging, gunshot, or other
penetrating injury to the neck region. Thus, 428patients were accepted for the final analyses.
Table 2 presents descriptive statistics for the 428
patients. Most patients (71%) were male, and mean
18 April 2018 � 2:37 pm � CE AH

Q5
1.e4 BLUNT CEREBROVASCULAR INJURY
337
338
339
340
341
342
343
344345
346
347
348
349
350
351
352353
354
355
356
357
358
359
360361
362
363
364
365
366
367
368369
370
371
372
373
374
375
376377
378
379
380
381
382
383
384385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400401
402
403
404
405
406
407
408409
410
411
412
413
414
415
416417
418
age was 41.9 years. The most common mechanism of
injury was motor vehicle accident (46.5%), followed
by fall from a height (20.1%) and bicycle accident
(8.2%). Other injury mechanisms were pedestrian
traffic injuries (5.6%), a fall on the stairs (4.4%), and
assault (3.3%). The remaining 11.9% fell under other
injury mechanisms, in which the mechanism was un-
known or the trauma was considered of relativelylow energy. Such mechanisms include falls from low
heights or on even on the ground, sports injuries,
and being struck by or crushed between blunt objects.
Craniofacial fractures had occurred in 75 patients
(17.5%), of whom 42 (58.3%) had a facial fracture,
19 (25.3%) had a skull fracture, and 14 (18.7%) had
facial and skull fractures, and 40 (9.3%) had BCVI.
Table 3 presents the association between BCVI andits predictors. BCVI was evident in 18.6% of patients
with craniofacial fracture, reaching significance
(P = .002). BCVI occurred most frequently with skull
fractures (21.1%), followed by facial fractures
(19.0%) and combinations of facial and skull fractures
(14.3%), although the differences among these 3
patient groups were nonsignificant (P = .882). No
meaningful associations emerged between BCVI andgender or mechanism of trauma. Table 4 presents a
logistic regression analysis between BCVI and gender,
Table 3. ASSOCIATION BETWEEN BCVI AND PREDICTORS IN
n BCVI Present
Gender
Male 304 24
Female 124 16
Age groups (yr)
13-30 133 7
31-50 156 21
51-70 111 9
71-90 28 3
Mechanism of trauma
Motor vehicle accident 199 23
Fall from height 86 9
Bicycle accident 35 1
Pedestrian traffic injuries 24 1
Fall on stairs 19 2
Assault 14 0
Other 51 4
Craniofacial fracture
Yes 75 14
No 353 26
Facial fracture 42 8
Skull fracture 19 4
Facial + skull fracture 14 2
Note: Significance level was set at .01.Abbreviation: BCVI, blunt cerebrovascular injury.
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac Surg 20
FLA 5.5.0 DTD � YJOMS58221_proof �
age group, mechanism of injury, and craniofacial frac-
tures. Analysis showed a 4-fold higher risk of BCVI in
patients with craniofacial fracture than in those with
other trauma (odds ratio [OR] = 4.096; 95% confi-
dence interval [CI], 1.866-8.993; P < .001). Patients
31 to 50 years old had a 3.4-fold higher risk than their
reference group (13 to 30 yr; OR = 3.426; 95% CI,
1.356-8.656; P = .009).Table 5 presents associations between craniofacial
fracture subgroups and BCVI. In the 56 patients with
facial fractures, BCVI most commonly occurred in
combined facial (20.0%) and midfacial (20.0%)
fractures. None with exclusively upper or lower facial
fractures showed BCVI. No statistically relevant differ-
ences appeared between BCVI and facial fracture
subgroups. Of the 33 patients with skull fractures,BCVI occurred most frequently in those with complex
skull fractures (37.5%), followed by basilar skull
fractures (14.3%), but in no other types of skull
fracture. The correlation between BCVI and complex
skull fractures was almost significant (P = .033).
Table 6 presents specific facial fractures and
fractures extending into the carotid canal and foramen
magnum. Further analysis showed that all BCVIs infacial fractures occurred in isolated zygomatico-
orbital fractures (35.7%), combined facial fractures
428 PATIENTS WITH TRAUMA
% BCVI in 40 Patients, % P Value
.110
7.9 60.0
12.9 40.0
.110
5.3 17.5
13.5 52.5
8.1 22.5
10.7 7.5
.500
11.6 57.5
10.5 22.5
2.9 2.5
4.2 2.5
10.5 5
0 0
7.8 10
18.6 35.0 .002
7.4 65.0
19.0 20 .882
21.1 10
14.3 5
18.
18 April 2018 � 2:37 pm � CE AH
419
420
421
422
423
424425
426
427
428
429
430
431
432433
434
435
436
437
438
439
440441
442
443
444
445
446
447
448

Table 4. MULTIVARIATE REGRESSION ANALYSIS FORBLUNT CEREBROVASCULAR INJURIES IN 428PATIENTS WITH TRAUMA
OR
95% CI for OR
P ValueLower Upper
Gender (ref, female) 0.460 0.223 0.946 .035
Age groups
(ref, 13-30 yr)
31-50 yr 3.426 1.356 8.656 .009
51-70 yr 2.179 0.746 6.370 .155
71-90 yr 2.432 0.531 11.145 .253
Mechanism of injury
(ref, MVA)
Fall from height 0.701 0.293 1.675 .424
Bicycle accident 0.110 0.013 0.908 .040
Pedestrian traffic
injuries
0.170 0.020 1.449 .105
Fall on stairs 0.491 0.092 2.622 .405
Assault 0.000 0.000 .998
Other 0.452 0.143 1.433 .178
Craniofacial fracture
(ref, yes)
4.096 1.866 8.993 <.001
Note: Significance level was set at .01.Abbreviations: CI, confidence interval; MVA, motor
vehicle accident; OR, odds ratio; ref, reference.
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac
Surg 2018.
VARJONEN ET AL 1.e5
449
450
451
452
453
454
455
456457
458
459
460
461
462
463
464465
466
467
468
469
470
471
472473
474
475
476
477
478
479
480481
482
483
484
485
486
487
488489
490
491
492
493
494
495
496497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512513
514
515
516
517
518
519
520521
522
523
524
525
526
527
528529
530
531
532
533
534
535
536537
(20.0%), and isolated orbital fractures (12.5%). The
number of specific facial fractures was insufficient
for statistical analysis. Only 1 patient with a skull
base fracture extending to the foramen magnum
Table 5. ASSOCIATION BETWEEN BCVI AND SUBGROUPS OFCRANIOFACIAL FRACTURE
n BCVI Present
Facial fracture
Any (n = 56) 56 10
Combined facial 20 4
Upper 1 0
Midfacial 30 6
Lower 5 0
Skull fracture
Any (n = 33) 33 6
Basilar skull fracture* 21 3
Other 4 0
Complex skull fracturey 8 3
Note: Significance level was set at .01.Abbreviation: BCVI, blunt cerebrovascular injury.* Fracture of the sphenoid, petrous, temporal, clivus, or occipity Basilar skull fracture plus other skull fracture.
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac Surg 20
FLA 5.5.0 DTD � YJOMS58221_proof �
(12.5%) had BCVI, and none of the 5 patients with a
fracture extending to the carotid canal had BCVI.
Discussion
The purpose of this study was to analyze possible
correlations between BCVI and craniofacial fractures
and to evaluate the incidence of BCVI in different
types of craniofacial fractures, with the hypothesis of
there being an association between craniofacial frac-
tures and BCVI. Furthermore, the authors investigated
a possible correlation of facial fracture subtypes
to BCVI.The present study of craniofacial fractures and BCVI
showed a strong correlation, with BCVI occurring 2.5
times more frequently in patients with craniofacial
fracture than in those with all other types of severe
trauma. Nearly 1 in 5 patients with craniofacial
fracture (18.6%) was diagnosed with BCVI. There
was no difference between facial fractures and skull
fractures with regard to BCVI. Logistic regressionshowed a 4-fold higher risk of BCVI for craniofacial
fractures compared with all other trauma.
Thus, the present results are in line with those of
Buch et al14 who stated that BCVI can occur in up to
11% of patients with blunt trauma injuries. However,
overall BCVI incidence was considerably higher
(9.3%) in the present study than in previous
studies.1-5 One possible explanation for the higherincidence of BCVI could be the authors’ institution
serving as a level 1 trauma center and a tertiary
hospital and therefore having a higher incidence of
severe trauma. Furthermore, the authors’ guidelines
CRANIOFACIAL FRACTURES IN 75 PATIENTS WITH
% BCVI in 14 Patients, % P Value
17.9 71.4 .757
20.0 28.6 .090
20.0 42.9
18.2 42.9 .924
14.3 21.4 .033
37.5 21.4
al condyle.
18.
18 April 2018 � 2:37 pm � CE AH
538
539
540
541
542
543
544545
546
547
548
549
550
551
552553
554
555
556
557
558
559
560

Table 6. SPECIFIC FACIAL FRACTURES ANDFRACTURES EXTENDING TO THE CAROTID CANALANDFORAMEN MAGNUM AND BCVI IN 75 PATIENTS
n
BCVI
Present %
P
Value
Facial fractures (n = 56) NA
Combined facial 20 4 20.0
Upper third 1 0
Multiple midfacial 4 0
Exclusively orbital 8 1 12.5
Exclusively
zygomatico-orbital
14 5 35.7
Exclusively maxillary 1 0
Exclusively nasal 3 0
Exclusively condylar 2 0
Exclusively
non-condylar
3 0
Skull fractures (n = 33) .084
Carotid canal 5 0
Foramen magnum 8 1 12.5
Fracture not involving
foramen
20 5 25.0
Note: Significance level was set at .01.Abbreviations: BCVI, blunt cerebrovascular injury; NA,
---.Q6
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac
Surg 2018.
1.e6 BLUNT CEREBROVASCULAR INJURY
561
562
563
564
565
566
567
568569
570
571
572
573
574
575
576577
578
579
580
581
582
583
584585
586
587
588
589
590
591
592593
594
595
596
597
598
599
600601
602
603
604
605
606
607
608609
610
611
612
613
614
615
616
617
618
619
620
621
622
623
624625
626
627
628
629
630
631
632633
634
635
636
637
638
639
640641
642
643
644
645
646
647
648649
650
651
652
653
654
655
656657
658
659
660
661
662
663
664665
666
667
668
669
670
671
672
for BCVI screening in patients with high-energy
trauma seem liberal; in addition to the Denver criteria,
the authors included thoracic and lower cervical spine
trauma. In the authors’ unit, even if the trauma alarm
protocol has not been triggered, the attending trauma
surgeon can order an aWBCT when clinical signs ormechanism of trauma indicate possible severe trauma.
Thus, the liberal screening protocol could have
increased the number of imaged patients and diag-
nosed BCVIs, especially among facial fracture cases.
Buch et al14 reported that 87% of their patients with
BCVI also had cervical or skull base fractures or a com-
bination of the 2, but concluded that isolated midface
fractures in the absence of cervical spine or skull basefractures were not associated with underlying BCVI.
However, the only facial injuries observed in their study
were complex facial fractures with midface instability.
The authors excluded cervical fractures to focus on
the effect of craniofacial fractures alone. Occurrence
was almost evenly divided among isolated facial frac-
tures, isolated cranial fractures, and combinations of
the 2 groups. Further analysis showed a high occur-rence of BCVI in combined facial fractures andmidfacial
fractures, especially in zygomatico-orbital fractures
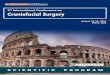
(Figs 1, 2). Based on these results, facial fractures
should be considered an independent risk factor for
BCVI. For more accurate conclusions about different
FLA 5.5.0 DTD � YJOMS58221_proof �
types of craniofacial fractures, a larger number of
patients with specific fracture types is required.
Recent studies have emphasized the relevance of
facial fractures in BCVIs, such as mandibular and
especially extracapsular condylar fractures15,22 and
maxillary fractures involving pterygoid plates.15
Kang et al23 described the injury mechanism of the in-
ternal carotid artery (ICA) in conjunction with Le FortI osteotomy. Owing to the anatomic proximity of the
ICA to the foramen lacerum and the pterygoid plate,
the artery can be directly damaged if a sharp bony
edge causes shearing near the skull base. This is in
line with the findings of Mundinger et al15 who
concluded that in patients with facial fracture, risk
for BCVI without applying screening criteria was
higher in patients with Le Fort I fractures. The samestudy reported corresponding findings in patients
with mandibular subcondylar fractures. Vranis et al22
studied condyle fractures in more detail and found
that direct injury caused by bony fragments, especially
displaced extracapsular condyle fractures, increased
the risk for BCVI. According to these studies, Le Fort
I fractures and extracapsular mandibular condylar frac-
tures, in particular, can lead to localized ICA damage.The authors found no associations between BCVI
and these fracture subtypes. The present study
showed a high occurrence of BCVI, especially in
zygomatico-orbital fractures, indicating that a facial
fracture is a marker of substantial trauma energy,
which in turn increases the likelihood of BCVI, even
when the fracture does not cause direct mechanical
damage to a vessel.Others have reported an association between skull
base fractures and BCVI.1,14,15,18,19 In the present
study, the authors analyzed all types of cranial
fractures. BCVI occurred most frequently in complex
skull fractures (combination of basilar skull fractures
and other skull fractures; 37.5%) and basilar skull
fractures (14.2%), but none of the patients with
exclusively other skull fracture types showed BCVI.This differs from the findings of York et al21 who re-
ported a high BCVI rate in fractures in other parts of
the skull, with 29% of patients with non-basilar skull
fractures having ICA injury. Carotid canal fractures
also have been implicated as a risk factor for BCVI.
Petrous bone fractures and carotid canal involvement
can lacerate a blood vessel, especially in the intraosteal
segment.20 York et al21 also evaluated the incidence ofICA injury and skull fractures, establishing that in skull
fractures with carotid canal involvement (35%), injury
to the ICA was twice as frequent as without canal
involvement (15%). Interestingly, in the present study,
none of the 5 patients with carotid canal involvement
and only 1 of 8 patients with a fracture extending to
the foramen magnum had BCVI. The number of these
patients was small, and further investigation with a
18 April 2018 � 2:37 pm � CE AH

print&web4C=FPO
FIGURE1. A 25-year-old unconscious woman was admitted with an unclear injury mechanism. Radiologic imaging depicted a left zygomaticarch fracture (broad arrow), right mandibular parasymphyseal fracture (thin arrow), and dental injuries to the upper incisors (arrowhead).
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac Surg 2018.
VARJONEN ET AL 1.e7
673
674
675
676
677
678
679
680681
682
683
684
685
686
687
688689
690
691
692
693
694
695
696697
698
699
700
701
702
703
704705
706
707
708
709
710
711
712713
714
715
716
717
718
719
720721
722
723
724
725
726
727
728
729
730
731
732
733
734
735
736737
738
739
740
741
742
743
744745
746
747
748
749
750
751
752753
754
755
756
757
758
759
760761
762
763
764
765
766
767
768769
770
771
772
773
774
775
776777
778
779
780
781
782
783
784
larger cohort of patients might clarify any associations
between skull fracture subtypes and BCVI.
The question arises as to whether BCVI correlates
with a certain type of injury or requires a certainamount of trauma energy. Even minor craniofacial
trauma has coincided with serious carotid injury.
One case study described a healthy young man with
a non-dislocated mandibular double fracture as a result
of a single punch, who was diagnosed with carotid
dissection and acute secondary embolic infarcts.24
Considering that report and the variation in craniofa-
cial fractures with BCVI in the present and previousstudies, the energy required to cause any craniofacial
fracture seems sufficient to cause an associated
BCVI. Interestingly, a previous study found that a
long styloid process of the temporal bone can
contribute to the pathogenesis of cervical carotid
FLA 5.5.0 DTD � YJOMS58221_proof �
dissection.25 Thus, taking into consideration that
hyperextension, rotation, and lateral flexion of the
neck predispose to BCVI, more detailed evaluation
of a local anatomic association is required. Furtherinvestigation of the level of BCVI and possible vectors
for trauma energy would probably shed some light on
these associations.
Controversy still exists concerning which patients
with trauma are at risk for BCVI and for whom
screening is thus indicated. Current BCVI screening
guidelines allow for BCVI being missed and risk for
stroke. Thus, more liberalized screening for BCVIduring initial CT in patients with trauma and signs of
typical mechanisms or high-energy trauma is war-
ranted.2 The overall incidence of BCVI has increased
during the past decade, in part because of the
increased availability and accuracy of cervical CTA in
18 April 2018 � 2:37 pm � CE AH

Q3
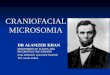
FIGURE 2. Cervical computed tomographic angiography displayed blunt cerebrovascular injury (Biffl grade 2) in the 2 internal carotidarteries (arrows).
Varjonen et al. Blunt Cerebrovascular Injury. J Oral Maxillofac Surg 2018.
1.e8 BLUNT CEREBROVASCULAR INJURY
785
786
787
788
789
790
791
792793
794
795
796
797
798
799
800801
802
803
804
805
806
807
808809
810
811
812
813
814
815
816817
818
819
820
821
822
823
824825
826
827
828
829
830
831
832833
834
835
836
837
838
839
840
841
842
843
844
845
846
847
848849
850
851
852
853
854
855
856857
858
859
860
861
862
863
864865
866
867
868
869
870
871
872873
874
875
876
877
878
879
880881
882
883
884
885
886
887
888889
890
891
892
893
894
895
896
combinationwith an increasing index of suspicion and
increased experience among trauma surgeons treatingthese injuries.1,26
Despite greater academic interest in this topic,
unambiguous evidence of associations between
craniofacial injuries and BCVIs is lacking. The present
study found that craniofacial fractures are a notable
risk factor for BCVI, without relevant differences in
risk between fracture subtypes. Therefore, in all
patients with polytrauma and craniofacial fractures,BCVI should be excluded.
References
1. Berne JD, Cook A, Rowe SA, et al: A multivariate logistic regres-sion analysis of risk factors for blunt cerebrovascular injury.J Vasc Surg 51:57, 2010
FLA 5.5.0 DTD � YJOMS58221_proof �
2. Bruns BR, Tesoriero R, Kufera J, et al: Blunt cerebrovascularinjury screening guidelines: What are we willing to miss? JTrauma Acute Care Surg 76:691, 2014
3. Miller PR, Fabian TC, Croce MA, et al: Prospective screening forblunt cerebrovascular injuries: Analysis of diagnostic modalitiesand outcomes. Ann Surg 236:386, 2002
4. Biffl WL, Ray CE Jr, Moore EE, et al: Treatment-related outcomesfrom blunt cerebrovascular injuries: Importance of routinefollow-up arteriography. Ann Surg 235:699, 2002
5. Fleck SK, Langner S, Baldauf J, et al: Incidence of blunt craniocer-vical artery injuries: Use of whole-body computed tomographytrauma imaging with adapted computed tomography angiog-raphy. Neurosurgery 69:615, 2011
6. Stein DM, Boswell S, Sliker CW, et al: Blunt cerebrovascu-lar injuries: Does treatment always matter? J Trauma 66:132, 2009
7. Miller PR, Fabian TC, Bee TK, et al: Blunt cerebrovascular in-juries: Diagnosis and treatment. J Trauma 51:279, 2001
8. Eastman AL, Muraliraj V, Sperry JL, et al: CTA-based screening re-duces time to diagnosis and stroke rate in blunt cervical vascularinjury. J Trauma 67:551, 2009
18 April 2018 � 2:37 pm � CE AH

VARJONEN ET AL 1.e9
897
898
899
900
901
902
903
904905
906
907
908
909
910
911
912913
914
915
916
917
918
919
920921
922
923
924
925
926
927
928
929
930931
932
933
934
935
936
937
938939
940
941
942
943
944
9. Fabian TC, Patton JH Jr, Croce MA, et al: Blunt carotid injury.Importance of early diagnosis and anticoagulant therapy. AnnSurg 223:513, 1996
10. Bromberg WJ, Collier BC, Diebel LN, et al: Blunt cerebro-vascular injury practice management guidelines: TheEastern Association for the Surgery of Trauma. J Trauma68:471, 2010
11. Burlew CC, Biffl WL, Moore EE, et al: Blunt cerebrovascular in-juries: Redefining screening criteria in the era of noninvasivediagnosis. J Trauma Acute Care Surg 72:330, 2012
12. Burlew CC, Biffl WL: Imaging for blunt carotid and vertebralartery injuries. Surg Clin North Am 91:217, 2011
13. Nakajima H, Nemoto M, Torio T, et al: Factors associated withblunt cerebrovascular injury in patients with cervical spineinjury. Neurol Med Chir (Tokyo) 54:379, 2014
14. Buch K, Nguyen T, Mahoney E, et al: Association between cervi-cal spine and skull-base fractures and blunt cerebrovascularinjury. Eur Radiol 26:524, 2016
15. MundingerGS,Dorafshar AH,GilsonMM, et al: Blunt-mechanismfacial fracture patterns associated with internal carotid arteryinjuries: Recommendations for additional screening criteriabased on analysis of 4,398 patients. J Oral Maxillofac Surg 71:2092, 2013
16. Geddes AE, Burlew CC, Wagenaar AE, et al: Expanded screeningcriteria for blunt cerebrovascular injury: A bigger impact thananticipated. Am J Surg 212:1167, 2016
17. Kelts G, Maturo S, Couch ME, et al: Blunt cerebrovascular injuryfollowing craniomaxillofacial fractures: A systematic review.Laryngoscope 127:79, 2017
FLA 5.5.0 DTD � YJOMS58221_proof �
18. BifflWL, Moore EE, Ryu RK, et al: The unrecognized epidemic ofblunt carotid arterial injuries: Early diagnosis improves neuro-logic outcome. Ann Surg 228:462, 1998
19. Cothren CC, Biffl WL, Moore EE, et al: Treatment for blunt cere-brovascular injuries: Equivalence of anticoagulation and anti-platelet agents. Arch Surg 144:685, 2009
20. Carter DA, Mehelas TJ, Savolaine ER, et al: Basal skull fracturewith traumatic polycranial neuropathy and occluded left carotidartery: Significance of fractures along the course of the carotidartery. J Trauma 44:230, 1998
21. York G, Barboriak D, Petrella J, et al: Association of internalcarotid artery injury with carotid canal fractures in patientswith head trauma. AJR Am J Roentgenol 184:1672, 2005
22. Vranis NM, Mundinger GS, Bellamy JL, et al: Extracapsularmandibular condyle fractures are associated with severe bluntinternal carotid artery injury: Analysis of 605 patients. PlastReconstr Surg 136:811, 2015
23. Kang SY, Lin EM, Marentette LJ: Importance of complete ptery-gomaxillary separation in the Le Fort I osteotomy: An anatomicreport. Skull Base 19:273, 2009
24. Murabit A, Tredget EE: Blunt carotid artery injury after minorfacial trauma. Can J Plast Surg 20:194, 2012
25. Raser JM, Mullen MT, Kasner SE, et al: Cervical carotid arterydissection is associated with styloid process length. Neurology77:2061, 2011
26. Berne JD, Reuland KS, Villarreal DH, et al: Sixteen-slice multi-detector computed tomographic angiography improves theaccuracy of screening for blunt cerebrovascular injury. J Trauma60:1204, 2006
18 April 2018 � 2:37 pm � CE AH
945
946947
948