Embed Size (px)
Citation preview

Recent Advances in the Management ofUnstable Cardiac Ischemic Syndromes
Elliot Rapaport, MDMonterey, CAMay 1, 2010
STRIVE ®
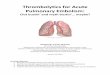
ACUTE CORONARY SYNDROMES
No ST elevation ST elevationUnstable angina NSTEMI STEMI
Spectrum of Acute Ischemic CAD
Figures reprinted with permission from Davies MJ. Heart. 2000;83(3):361-366.
Lloyd-Jones D, et al. Heart Disease and Stroke Statistics—2010 Update: A Report From the American Heart Association Circulation 2009 Dec 17 [Epub ahead of print]
Abbreviations: CAD, coronary artery disease; NSTEMI, non–ST-segment elevation myocardial infarction; STEMI, ST-segment elevation myocardial infarction.
~0.4 MillionDischarges Per Year
~1 MillionDischarges Per Year
Approach to Preventing the Consequences of a Vulnerable Plaque Rupture or Erosion
Manage the culprit lesion either invasively or conservatively based onquantifying the potential immediate and long term risk, with the primary goal of immediate (STEMI) or early (NSTEMI) restorationof maximum epicardial and microvascular coronary blood flow.
Utilize long term dual antiplatelet therapy of at least one year ( whether or not a PCI was done ) to minimize the potential of similar future episodes arising either from the same or other vulnerarble areas.
Insure maximum long term medical management as well as appropriate lifestyle changes to pacify other potential vulnerable plaques and to arrest the generalized progression of atherothrombosis.

Copyright ©2009 American Heart Association
Chan, M. Y. et al. Circulation 2009;119:3110-3117
Kaplan-Meier mortality curves of STEMI vs NSTEMI showing all-cause mortality from the time of cardiac catheterization
Mortality
Time ( years )
NSTEMI
STEMI
Management failuren=2399
n=1957
STRIVE ®
5
Effect of Door-to-Balloon Time on Mortality in Patients With STEMI
McNamara RL, et al. J Am Coll Cardiol. 2006;47(11):2180-2186.
8
7
6
5
4
3
2
1
0≤90 >90 - 120 >120 - 150 >150
Door-to-Balloon Time (min)
In-h
osp
ital
Mo
rtal
ity,
%
NRMI 3 and 4 ( 1999-2002)
STRIVE ®
6
Class I Modified Recommendations
Reperfusion Therapy for STEMI
• STEMI patients presenting to a hospital with PCI capability should be treated with primary PCI within 90 minutes of first medical contact as a systems goal (Level of Evidence: A)
• STEMI patients presenting to a hospital without PCI capability and who cannot be transferred to a PCI center and undergo PCI within90 minutes of first medical contact should be treated with fibrinolytictherapy within 30 minutes of hospital presentation as a systems goal unless fibrinolytic therapy is contraindicated (Level of Evidence: B)
Antman EM, et al. J Am Coll Cardiol. 2008;51(2):210-247.
2007 ACC/AHA STEMI Focused Update

STRIVE ®
7
Reperfusion Times
PrehospitalECG
(n=1941)
In-Hospital ECG
(n=5157)P value
Fibrinolytic agentsDTN time (min)a
DTN time ≤30 min
(n=72)19 (10, 30)
72
(n=167)29 (19, 45)
49.003.05
Primary PCI
DTB time (min)a
DTB time ≤90 min
(n=1501)
61 (46, 79)82
(n=3563)
75 (58, 95)70
<.0001<.0001
Timing of Reperfusion Therapy by Pre- versus In-Hospital ECG Utilization
Diercks DB, et al. J Am Coll Cardiol. 2009;53(2):161-166. (NCDR ACTION Registry)
STRIVE TM
TRANSFER-AMI
• Primary end point (death, MI, heart failure, severe recurrent ischemia, or shock at 30 days): 10.6% in pharmacoinvasive arm vs 16.6% in standard treatment arm (P=.0013)
• Reinfarction: 3.3% vs 6.0% (P=.044)
• Recurrent ischemia: 0.2% vs 2.2% (P=.02)
Preliminary Results
Conclusions
(P=.0013)
Pharmacoinvasivestrategy(n=522)
Standard therapy(n=508)
Primary End Point• Pharmacoinvasive approach safe and
efficacious compared with treatment with thrombolytics and transfer for rescue PCI only. No excess in major bleeding
• Optimal window: 6 hours
0
10
20
% 10.6
16.63.7 3.6
%
0
1
5
2
3
4
Mortality
(P=.94)
Trial design: Patients with high-risk STEMI who presented where timelyPrimary PCI was not feasible were randomized to a pharrmacoinvasive(ASA, TNK, UFH or Enox, clopidogrel strategy with emergent transfer for PCI within 6 hours of fibrinolysis) or to standard treatment after fibrinolysis
Cantor W,. N. Engl. J. Med. 360 (26):2705-18. Cantor W,. N. Engl. J. Med. 360 (26):2705-18.
n=133n=133 n=125n=125
Halvorsen S.ESC 2009 Congress;Barcelona, Spain.

TNK to 1TNK to 1stst balloon 3.0 d (0,13)balloon 3.0 d (0,13)
TNK to 1TNK to 1stst balloon 163m (137,191)balloon 163m (137,191)
STRIVE ®
2009 STEMI Focused Update ( New Recommendations )
Class IIa
In STEMI patients undergoing PCI who are at high risk of bleeding,Bivalirudin anticoagulation is reasonable.
It is reasonable for high risk patients who receive fibrinolytic therapyas primary reperfusion therapy at a non-PCI capable facility to be transferred as soon as possible to a PCI-capable facility where PCI can be performed either when needed or as a pharmacoinvasivestrategy. Consideration should be given to initiating a preparatory antithrombotic (anticoagulant plus antiplatelet) regimen before andduring patient transfer to the catheterization laboratory.
It is reasonable to use an insulin-based regimen to achieve and Maintain glucose levels less than 180 mg/dL while avoiding hypoglycemia for patients with STEMI with either a complicatedor uncomplicated course.
Kushner FG, et al. J Am Coll Cardiol. 2009;54(23):2205-2241.
STRIVE TM
0.1 0.5 1 2 5
Favors Invasive
Favors Conservative
Odds Ratio Death or MI
OR 0.82, P<.0012.2% abs reduction
Trial (N)
TIMI IIIB (1473)
VANQWISH (920)
MATE (201)
FRISC II (2457)
TACTICS (2220)
RITA 3 (1810)
Total (N = 9212)
Invasive Management of UA/NSTEMI Meta-analysis: Death/MI at End of Follow-up (Mean 17.3 months)
11.6 13.8
32.9 30.3
14.4 12.2
10.4 14.1
7.3 9.5
10.6 12.9
VINO (131) 6.3 22.4
Inv (%) Cons (%)
12.2 14.4
Mehta S, et al. JAMA. 2005;293:2908-2917.

Acute care patterns by early invasive management*
Bhatt et al. JAMA 2004;292:2096
No early invasive care(n=9889)
Early invasive care(n=8037) p value
Aspirin 87.7% 93.8% <0.001
Clopidogrel 26.1% 51.3% <0.001
B blocker 71.9% 77.7% <0.001
Heparin 73.7% 88.8% <0.001
GP IIb/IIIainhibitor 14.2% 50.9% <0.001
Bhatt et al. JAMA 2004;292:2096
STRIVE ®
14
%
4.96.0
TIMACS
No difference in primary outcome (death, MI, stroke) between the two arms (HR, 0.85; 95% CI, 0.68-1.06; P= .15), except in high-risk patients (GRACE risk score >140) (HR, 0.65; 95% CI, 0.48-0.88; P = .005)
Death, MI, refractory ischemia ↓ in early invasive arm (P = .0002), due to ↓ in refractory ischemia (P <.0001); death (P = .19), stroke (P = .74) similar
Major bleeding was similar (P = .53)
Trial design: Patients with NSTEMI were randomized to an early (within 24 hours) or delayed (after 36 hours) invasive strategy. Clinical outcomes were compared at 6 months.
Results
Conclusions An early invasive strategy (within 24 hours) is not
associated with harm compared with a delayed invasive strategy (after 36 hours) in patients with NSTEMI, and may be beneficial in high-risk patients
Significant reduction in refractory ischemia with an early invasive strategy
Mehta SR, et al. : American Heart Association 2008 Scientific Sessions
(P = .15)
Early invasive(n = 1593)
Delayed invasive(n = 1438)
(P = .19)20
15
10
5
0
9.711.4
Primary end point Mortality
%
20
15
10
5
0
Trial design: Patients with NSTEMI were randomized to an early (within 24 hours) or delayed (after 36 hours) invasive strategy. Clinical outcomes were compared at 6 months. Trial design: Patients with NSTEMI were randomized to an early (within 24 hours) or
delayed (after 36 hours) invasive strategy. Clinical outcomes were compared at 6 months.
Preliminary Results
ABOARD study designABOARD study designABOARD study design
NSTENSTE--ACS ( n = 352 )ACS ( n = 352 )2 of 3 Criteria: Ischemic symptom, ST2 of 3 Criteria: Ischemic symptom, ST--T change, troponin riseT change, troponin rise
with TIMI score with TIMI score >> 33
Immediate cathImmediate cath Next day cathNext day cath
All PCIs on abciximabAll PCIs on abciximab
11--month Followmonth Follow--upup
IVRS RANDOMIZATIONIVRS RANDOMIZATION
JAMA 2009;302:947-954

Preliminary Results
Composite Ischemic Endpoints at 1 monthComposite Ischemic Endpoints at 1 month
%%
0
5
10
15
20
25
Death / MI / UR Death / MI / UR / RI
ImmediateDelayed
Key secondary EP
P=0.31
P=0.94
JAMA 2009;302:947-954
STRIVE TM
Optimal Timing for Pretreatment With Clopidogrel 300 mg Before PCI: CREDO Study
Steinhubl SR, et al. J Am Coll Cardiol. 2006;47(5):939-943.
For pretreatment ≥15 h vs placebo, P=.018; for pretreatment ≥15 h vs <15 h, P=.033; for placebo vs pretreatment <15 h, P=.72.
10
8
6
4
2
00 5 10 15 20 25
Dea
th, M
I, U
TV
R, %
Days
Placebo Pretreatment (n=915)
Clopidogrel Pretreatment <15 hours (n=645)
Clopidogrel Pretreatment ≥15 hours (n=202)
3.5%
7.8%8.3%
Pts randomize to receive study drug or placebo between 3 and 24 hours before PCI
STRIVE ®
1818
ARMYDA-ACS: Design and Primary End PointPrimary end point: death, MI,
or unplanned revasc. at 30 days
P=.01
5%
0%
5%
10%
15%
Atorvastatin Placebo
17%
Atorvastatin80 mg 12hbefore PCI;
additional 40 mg2h before PCI
(N=86)
Placebo 12h before PCI;
additional dose 2h before PCI
(N=85)
Patients with NSTE-ACSsent to early PCI
(<48 hours). Statin naïve patients
Randomization(N=171)
Patti G, et al. J Am Coll Cardiol. 2007;49(12):1272-1278.
All patients given clopidogrel 600 mg loading dose; long-term atorvastatin
(40 mg/d)
20%

UA/NSTEMI Strategy OverviewUA/NSTEMI Strategy OverviewUA/NSTEMI Strategy Overview
ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, Circulation.ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, 6, 2007, Circulation.Circulation.
2007 ACC/AHA UA/NSTEMI Guideline Revision
EARLY INVASIVE VS. INITIAL CONSERVATIVE THERAPY
“In initially stabilized patients, an initially conservative (i.e., a selectively invasive) strategy may be considered as a treatment strategy for UA/NSTEMI patients (without serious comorbidities or contraindications to such procedures) who have an elevated risk for clinical events, including those who are troponin positive.” (Class IIb) “The decision to implement an initial conservative (vs. initial invasive) strategy in these patients may be made by considering physician and patient preference.” (Class IIb)
2007 ACC/AHA UA/NSTEMI Guideline Revision
EARLY INVASIVE VS. INITIAL CONSERVATIVE THERAPYEARLY INVASIVE VS. INITIAL CONSERVATIVE THERAPY
““In initially stabilized patients, an In initially stabilized patients, an initially conservative (i.e., a initially conservative (i.e., a selectively invasive) strategy may be consideredselectively invasive) strategy may be considered as a treatment as a treatment strategy for UA/NSTEMI patients (without serious strategy for UA/NSTEMI patients (without serious comorbiditiescomorbidities or or contraindications to such procedures) who have an elevated risk contraindications to such procedures) who have an elevated risk for for clinical events, clinical events, including those who are including those who are troponintroponin positivepositive..”” (Class (Class IIbIIb) ) ““The decision to implement an initial conservative (vs. initial The decision to implement an initial conservative (vs. initial invasive) strategy in these patients may be made by invasive) strategy in these patients may be made by considering considering physician and patient preferencephysician and patient preference..”” (Class (Class IIbIIb))
Cumulative risk of CV death or MI by risk groupCumulative risk of CV death or MI by risk group
High
Intermediate
Low
11.1% abs. risk reduction
3.8% abs RR
2% abs RR
““A A conservative strategyconservative strategy is recommended in is recommended in women with lowwomen with low--risk features (I, B)risk features (I, B)””
2007 ACC/AHA UA/NSTEMI Guideline Revision
EARLY INVASIVE VS. INITIAL CONSERVATIVE THERAPYEARLY INVASIVE VS. INITIAL CONSERVATIVE THERAPY

Meta analysis – Death in women
Study name Dead / Total Statistics for each study Odds ratio and 95% CI
Routine Selective Odds Lower Upper Invasive Invasive ratio limit limit p-Value
FRISC II 14 / 348 13 / 401 1.25 0.58 2.70 0.57
RITA 3 18 / 350 8 / 332 2.20 0.94 5.12 0.07
TACTICS 15 / 395 13 / 362 1.06 0.50 2.26 0.88
OASIS 5 8 / 92 1 / 92 8.67 1.06 70.77 0.04
55 /1185 35 /1187 1.50 0.96 2.35 0.07
0.01 0.1 1 10 100
Favours Early Invasive Favours Selective Invasive
STRIVE ®
23
Adjunctive Thrombectomy and Embolic Protection Devices in AMI: Meta-analysisa
P=.018
P=.050
Mo
rtal
ity,
%
P=.69
Bavry AA, et al. Eur Heart J. 2008;29(24):2989-3001.
2.7
5.3
4.4
2.8 3.1
0
3
6
Catheter thrombusaspiration
Mechanical thrombectomy
Embolic protection
Adjunctive device prior to PCI
PCI alone
3.4
a Meta-analysis of 30 randomized clinical trials with 6415 patients.
Sites of Anticoagulant and Sites of Anticoagulant and AntiplateletAntiplatelet Drug ActionDrug Action
Tissue factorTissue factor
Plasma clottingcascade
Plasma clottingcascade
ProthrombinProthrombin
ThrombinThrombin
FibrinogenFibrinogen FibrinFibrin
ThrombusThrombus
Platelet aggregationPlatelet aggregation
Platelet activationPlatelet activation
CollagenCollagen
Thromboxane A2Thromboxane A2
ADPADP
ATAT
ATAT
Aspirin
ClopidogrelPrasugrelCangrelorTicagrelor
EptifibatideAbciximabTirofiban
Bivalirudin
FactorXa
FactorXa
Heparin Enoxaparin
Fibrinolytics
Fondaparinux
ATAT
SCH 530348

STRIVE ®
25
ARMYDA-2 Study: Design and Primary End Point
Primary composite of death, MI, or target vessel revasc. at 30 days
P=.041
4%
0%
2%
4%
6%
8%
10%
12%
14%
600 mg 300 mg
12%
High Loading Dose of
Clopidogrel600 mgPre-PCI
Standard Loading Dose
of Clopidogrel
300 mgPre-PCI
255 patients with stable CAD or NSTEMI prior to PCI
13% received GP IIb/IIIa inhibitors20% received drug-eluting stents
Randomized 4-8 Hours Pre-PCI
ARMYDA-2, Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty.
Patti G, et al. Circulation. 2005;111(16):2099-2106.
STRIVE TM
26
Clopidogrel High-Dose GroupClopidogrel 600 mg loading dose day 1 followed by 150 mg from days 2 to 7; 75 mg from days 8 to 30
Clopidogrel Standard-Dose GroupClopidogrel 300 mg (+ placebo) day 1 followed
by 75 mg (+ placebo) from days 2 to 7;75 mg from days 8 to 30
Patients with UA or MI planned for early invasiveStrategy (PCI intended as early as possible within 24 h)
RANDOMIZE
Clopidogrel Optimal Loading Dose Usage to Reduce Recurrent EveNTs/Optimal Antiplatelet Strategy for InterventionS-7
CURRENT/OASIS-7
RANDOMIZERANDOMIZE
ASA low-dose groupAt least 300 mg day 1;
75–100 mgfrom days 2 to 30
ASA high-dose groupAt least 300 mg day 1;
300–325 mgfrom days 2 to 30
ASA high-dose groupAt least 300 mg day 1;
300–325 mgfrom days 2 to 30
ASA low-dose groupAt least 300 mg day 1;
75–100 mgfrom days 2 to 30
.
Mehta SR. Eur Heart J Suppl. 2006;8:G25-G30.
Primary Outcome: 30-day CV Death, MI, or Recurrent Ischemia
Days
Cu
mu
lati
ve H
aza
rd
0.0
0.01
0.02
0.03
0.04
0 3 6 9 12 15 18 21 24 27 30
Clopidogrel: Double vs Standard Dose Primary Outcome: PCI Patients
Clopidogrel Standard
Clopidogrel Double
HR 0.8595% CI 0.74-0.99
P=0.036
15% RRR15% RRR
CV Death, MI or StrokeCV Death, MI or Stroke
ECC Aug 30, 2009

Clopidogrel HR 95% CI P P int’n
Standard Double
CV Death/MI/Stroke (Overall)
ASA High 4.6 3.8 0.83 0.70-0.99 0.0360.043ASA Low 4.2 4.5 1.07 0.91-1.27 0.42
MI/Stent Thrombosis (PCI pts)
ASA High 3.8 2.7 0.71 0.56-0.90 0.005 0.19
ASA Low 3.6 3.2 0.89 0.71-1.12 0.32
Major Bleed (Overall)
ASA High 2.2 2.4 1.08 0.86-1.37 0.510.099
ASA Low 1.9 2.7 1.43 1.13-1.81 0.003
Clopidogrel: Double vs Standard Dose byASA Factorial
ECC Aug 30, 2009
Active Metabolite Formation:Prasugrel and Clopidogrel
Active Metabolite Formation:Prasugrel and Clopidogrel
Main trial design
Double-blind
ACS (STEMI or UA/NSTEMI) and planned PCI
ASA
PRASUGREL60 mg LD/ 10 mg MD
CLOPIDOGREL300 mg LD/ 75 mg MD
1o end point: CV death, MI, stroke2o end point: Stent thrombosis Safety end points: TIMI major bleeds, life-threatening bleeds
Duration of therapy: 6-15 months
N = 13,608
TRITON TIMI-38

0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81(0.73-0.90)P = 0.0004Prasugrel
Clopidogrel
Days
En
d P
oin
t (%
)
12.1
9.9
HR 1.32(1.03-1.68)
P = 0.03
Prasugrel
Clopidogrel1.82.4
TRITON TIMITRITON TIMI--38: Primary results38: Primary results
CV death/MI/stroke
TIMI major NonCABG bleeds
Bleeding Events: Safety CohortClop, % Pras, % P
TIMI major 1.8 2.4 .03Life threatening 0.9 1.4 .01Nonfatal 0.9 1.1 .23Fatal 0.1 0.4 .002ICH 0.3 0.3 .74
Efficacy
Safety
TRITON TIMI-38 STEMI cohort
Montalescot et al. ESC 2008
Efficacy endpoints at 15 months
Clopidogrel
Prasugrel
0
2
4
6
8
10
12
14
p= 0.11
p= 0.02
p= 0.09p= 0.02
p= 0.007 p= 0.03 p= 0.02
Pro
po
rtio
n o
f p
op
ula
tio
n (
%)
All Death MI UTVR StentThrombosis*
CV Death/MI
CV Death/MI/UTVR
CV Death/MI/Stroke
* ARC def/probable
No increase in TIMI major or minor non-CABG bleeding was observed
I IIa IIb III
STRIVE ®
33
C
Kushner FG, et al. J Am Coll Cardiol. 2009;54(23):2205-2241.
Thienopyridines
2009 ACC/AHA STEMI/PCI Guidelines Focused Updates
New RecommendationClass 3
2009 ACC/AHA STEMI and PCI Guidelines Focused Updates
In STEMI patients with a prior history of stroke and transient ischemic attack for whom primary PCI is planned, prasugrel is not recommended as part of a dual- antiplatelettherapy regimen

Hazard Ratio 1.53
(95% CI 1.07-2.19)
P=0.014
8.0
12.1
1064 1009 999 980 870 755 542
Number at Risk:
Days After Randomization
Non-Carrier
395 364 360 348 306 270 181Carrier
CV
Death
, M
I, o
r S
troke (
%)
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 30 90 180 270 360 450
Non-carriers
Carriers
CYP2C19 and CVD, MI, or StrokeCLOPIDOGREL
* Carriers ~30% of the population
CYP2C19 Reduced-Function Allele Carriers
N=1,477
Hazard Ratio 0.89
(95% CI 0.60-1.31)
P=0.27
9.8
8.5
1048 991 982 951 849 750 541
407 383 376 364 320 276 188
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
0 30 90 180 270 360 450
Number at Risk:
Days After Randomization
Non-Carrier
Carrier
CV
Deat
h, M
I, or
Str
oke
(%
) Non-carriers
CarriersCYP2C19Reduced-Function
Allele Carriers
PRASUGREL
N=1,466
Pharmacogenetics of antiplatelet therapy
Mega et al. NEJM 2009
InvasivePLATO study design
6–12 months treatment
PCI = percutaneous coronary intervention; CV = cardiovascular; PI = principal investigator
NSTEMI ACS (moderate-to-high risk) STEMI (if primary PCI) (N=18,624)Clopidogrel-treated or -naive; randomized <24 hours of index event
At randomization, 13,408 (72%) of patients were specified by the Investigator: intent for invasive strategy
Primary endpoint: CV death + MI + Stroke Primary safety endpoint: Total major bleeding
Clopidogrel (n=6,676)If pre-treated, no additional loading dose;if naive, standard 300 mg loading dose,
then 75 mg qd maintenance;(additional 300 mg allowed pre-PCI)
Ticagrelor (n=6,732)180 mg loading dose, then
90 mg bid maintenance;(additional 90 mg pre-PCI)
InvasivePrimary endpoint: CV death, MI or stroke
0
0
5
10
15
60 120 180 240 300 360
Days after randomization
K-M
es
tim
ate
d r
ate
(%
pe
r ye
ar)
HR: 0.84 (95% CI = 0.75–0.94), p=0.0025
9.02
10.65Clopidogrel
Ticagrelor
No. at risk
Clopidogrel
Ticagrelor
6,676
6,732
6,129
6,236
6,034
6,134
5,881 4,815
4,889
3,680
3,735
2,965
3,0485,972
HR 0.99 (95% CI = 0.89–1.10), p=0.88 for major bleeding

No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,560
8,678
8,405
8,520
8,177
Days after randomisation
6,703
6,796
5,136
5,210
4,109
4,191
0 60 120 180 240 300 360
6
5
4
3
2
1
0
7
Cu
mu
lati
ve i
nc
ide
nc
e (
%)
Clopidogrel
Ticagrelor
5.8
6.9
8,279
HR 0.84 (95% CI 0.75–0.95), p=0.005
0 60 120 180 240 300 360
6
4
3
2
1
0
Clopidogrel
Ticagrelor
4.0
5.1
HR 0.79 (95% CI 0.69–0.91), p=0.001
7
5
9,291
9,333
8,865
8,294
8,780
8,822
8,589
Days after randomisation
7079
7119
5,441
5,482
4,364
4,4198,626
Myocardial infarction Cardiovascular death
Cu
mu
lati
ve i
nc
ide
nc
e (
%)
Secondary efficacy endpoints over time
MortalityMortality
Major BleedingMajor Bleeding
TransfusionTransfusionHypotensionHypotension Cessation of Cessation of ASA/ASA/ClopidogrelClopidogrel
IschemiaIschemia Stent ThrombosisStent Thrombosis InflammationInflammation
Bhatt DL et al. In Braunwald: Harrison’s Online 2005.
Possible Relationship BetweenPossible Relationship BetweenBleeding and Mortality in ACSBleeding and Mortality in ACS
I IIa IIb III
STRIVE ®
39
The usefulness of glycoprotein IIb/IIIa receptor antagonists (as part of a preparatory pharmacologic strategy for patients with STEMI prior to arrival in the cardiac catheterization laboratory for angiography) is uncertain
Kushner FG, et al. J Am Coll Cardiol. 2009;54(23):2205-2241.
Use of GP IIb/IIIa Inhibitors in STEMI
2009 ACC/AHA STEMI/PCI Guidelines Focused Updates
Modified RecommendationClass 2b
2009 ACC/AHA STEMI and PCI Guidelines Focused Updates

1-Year Mortality (All-Cause)
Number at riskBivalirudin aloneHeparin+GPIIb/IIIa
1800 1705 1684 1669 15201802 1679 1664 1647 1487
Mo
rtal
ity
(%)
0
1
2
3
4
5
Time in Months
0 1 2 3 4 5 6 7 8 9 10 11 12
Bivalirudin alone (n=1800)
Heparin + GPIIb/IIIa (n=1802) 4.8%
3.4%
Diff [95%CI] =
-1.4% [-2.7,-0.1]
HR [95%CI] =
0.70 [0.51, 0.98]
P=0.036P=0.036
3.1%
2.1%
Δ = 1.0%
P=0.049
Δ = 1.4%
STRIVE TM
Immediate Pharmacotherapy for STEMI Patient
Managed by Primary PCI
Aspirin
Start anticoagulant in ED
IV Morphine as needed for analgesia
Sublingual NTG followed by IV Drip
If enoxaparin or UFH started, switch to IV Bolus
of bivalarudin once PCI begun. If procedure lasting
longer than 30 minutes start bivalarudin infusion
If bivalarudin not used, consider adding a GP 2b/3a inhibitor,
clopid. 600 mg or Prasugrel 60 mg after angio confirms PCI need
STRIVE TM
Initial Invasive Strategy: Antiplatelet, Anticoagulant Therapy
Aspirin Initiate anticoagulant therapy as soon as possible after
presentation (I, A). Regimens with established efficacy:– Enoxaparin or UFH (I, A)– Bivalirudin or fondaparinux (I, B)
Prior to angiography, initiate one (I, A) or both (IIa, B)– Clopidogrel– IV GP IIb/IIIa inhibitor
Use both if: Delay to angiography High-risk features Early recurrent ischemic syndromes
2007 ACC/AHA UA/NSTEMI Guideline Revision
Anderson JL, et al. J Am Coll Cardiol. 2007;50(7):e1-e157.

STRIVE TM
Secondary Prevention: Additional Recommendations
β-blockers
ACE inhibitors/ARBs
Aldosterone blockade
Lipid management– Statin regardless of
baseline LDL-C initiated prior to discharge
– Goal LDL-C <100 mg/dL
– LDL <70 mg/dLreasonable
Treatment of triglycerides and non–HDL-C useful
– If TG 200-499 mg/dL, non–HDL-C should be <130 mg/dL
– TG 500 mg/dL, fibrate or niacin before LDL-C lowering to prevent pancreatitis
Encouraging consumption of omega-3 fatty acids for risk reduction reasonable
– For treatment of elevated triglycerides, higher doses may be used for risk reduction
2007 ACC/AHA UA/NSTEMI Guideline Revision
Anderson JL, et al. J Am Coll Cardiol. 2007;50(7):e1-e157.
STRIVE TM
Secondary Prevention: Additional Recommendations (cont)
BP control
– <140/90 mm Hg
– <130/80 mm Hg with diabetes or CKD
Diabetes management: HbA1c<7%
Smoking cessation/no environmental smoke exposure
– Education, referral programs, drug therapy
Physical activity (30-60 min, 7 d/wk; min 5 d/wk)
Weight management
– BMI 18.5-24.9 kg/m2
– Waist circumference: men, <40 in; women, <35 in
Discharge education/referral
Stepped-care approach to musculoskeletal pain management
Annual influenza immunization
HRT, antioxidant vitamin supplements (C, E, beta carotene) and folic acid not recommended
2007 ACC/AHA UA/NSTEMI Guideline Revision
Anderson JL, et al. J Am Coll Cardiol. 2007;50(7):e1-e157.